
A Human Model of the Effects of an Instant Sheer Weight Loss on Cardiopulmonary Parameters during a Treadmill Run
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Evaluation and Echocardiography
2.3. Resting Spirometry and Cardiopulmonary Exercise Testing
2.3.1. General Settings and Resting Spirometry
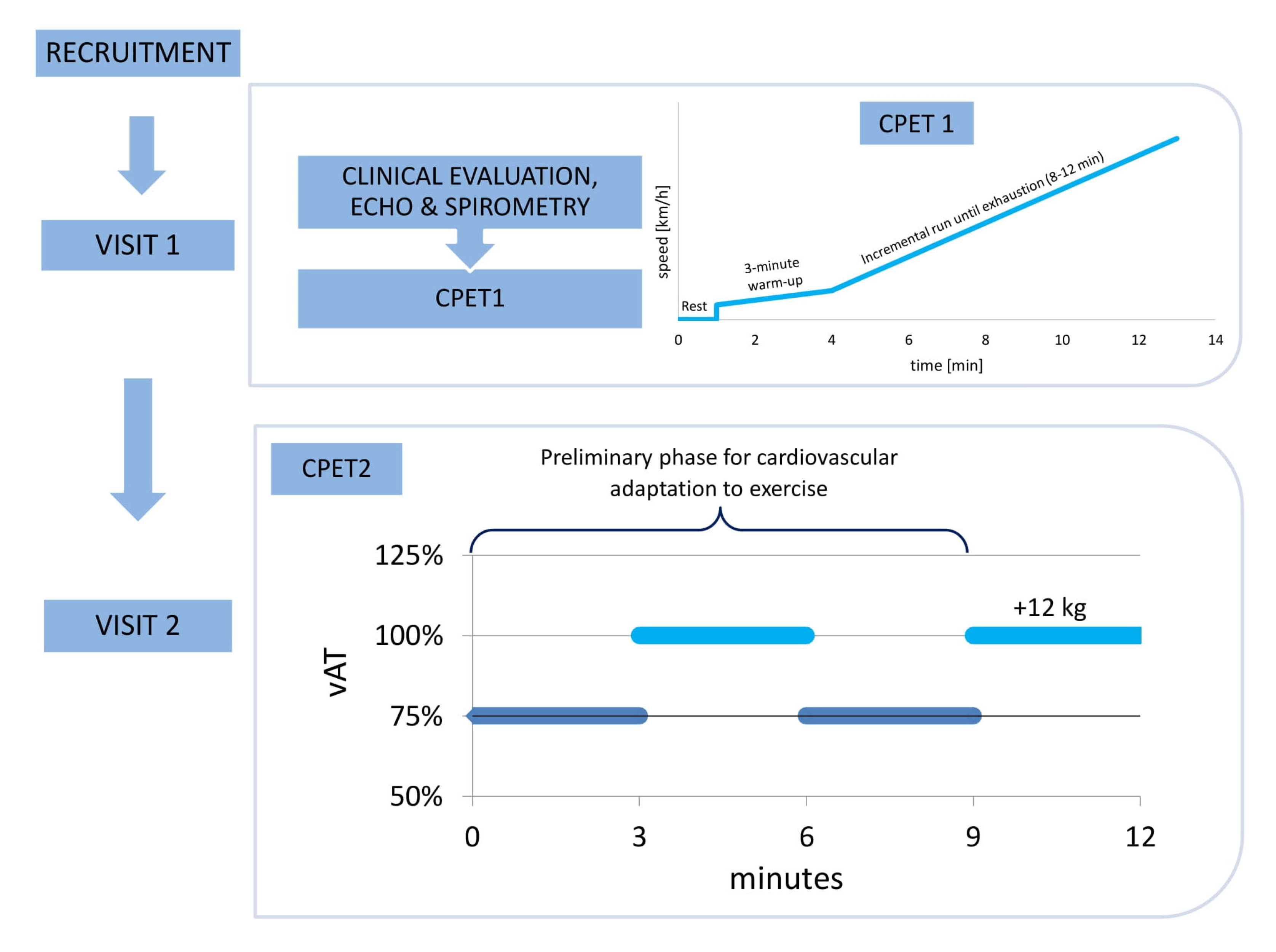
2.3.2. CPET1
2.3.3. CPET2
- HR—heart rate.
- VO2—the volume of consumed O2.
- O2 pulse as a ratio of VO2 to HR.
- VCO2—the volume of produced CO2.
- VE—minute ventilation.
- TV—the tidal volume.
- BF—breathing frequency.
- BR%—breathing reserve as a fraction of VE to MVV.
- VE/VO2—the ventilatory equivalent for oxygen.
- VE/VCO2—the ventilatory equivalent for carbon dioxide.
- RER—respiratory exchange ratio.
- PetO2—the end-tidal oxygen tension.
- PetCO2—the end-tidal carbon dioxide tension.
2.4. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics, Echocardiography, and Resting CPET

{kind=link}
{kind=link}
| CPET2 | CPET1 AT | vs. AT | CPET1 RCP | vs. RCP | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | 25th p | 75th p | Median | 25th p | 75th p | p | Median | 25th p | 75th p | p | |
| BF (breaths/min) | 47.0 | 44.0 | 50.5 | 35.8 | 31.0 | 39.1 | <0.0001 | 43.0 | 41.0 | 46.5 | 0.6681 |
| VCO2 (L/min) | 3.41 | 2.97 | 3.67 | 2.72 | 2.52 | 3.02 | 0.0423 | 3.84 | 3.41 | 4.17 | 0.3003 |
| VE/VCO2 | 29.15 | 27.83 | 30.53 | 26.41 | 24.87 | 27.70 | <0.0001 | 28.50 | 27.48 | 29.55 | 1 |
| VE/VO2 | 30.05 | 28.30 | 32.55 | 27.15 | 24.78 | 28.38 | 0.0023 | 30.95 | 29.33 | 33.13 | 1 |
| VO2 (L/min) | 3.27 | 2.86 | 3.48 | 2.81 | 2.58 | 3.11 | 0.0132 | 3.50 | 3.15 | 3.80 | 1 |
| VE (L/min) | 104.40 | 92.83 | 117.84 | 80.52 | 73.94 | 87.30 | 0.0197 | 114.02 | 104.78 | 128.45 | 0.6681 |
| TV (L) | 2.24 | 1.98 | 2.38 | 2.43 | 2.24 | 2.62 | 0.3972 | 2.60 | 2.45 | 2.77 | 0.0005 |
| RER | 1.04 | 1.01 | 1.09 | 0.96 | 0.93 | 0.99 | 0.0132 | 1.09 | 1.05 | 1.13 | 0.8499 |
| HR (beats/min) | 169 | 167 | 178 | 163 | 156 | 166 | 0.0291 | 178 | 174 | 185 | 0.3459 |
| O2pulse (mL/beat) | 18.86 | 16.91 | 20.50 | 17.58 | 16.27 | 19.06 | 0.0132 | 19.59 | 17.57 | 22.64 | 1 |
| PetO2 (mmHg) | 111.0 | 108.0 | 112.3 | 107.0 | 100.4 | 108.0 | 0.0107 | 111.5 | 109.8 | 113.3 | 1 |
| PetCO2 (mmHg) | 41.0 | 40.4 | 43.0 | 39.1 | 38.2 | 40.0 | 0.0001 | 40.0 | 38.8 | 42.0 | 0.224 |
| % | AT | RCP | ||||
|---|---|---|---|---|---|---|
| Median | 25th p | 75th p | Median | 25th p | 75th p | |
| BF | −28.13 | −32.94 | −20.00 | −4.36 | −12.15 | 0.00 |
| VCO2 | −16.64 | −23.21 | −12.55 | 12.06 | 5.52 | 20.98 |
| VE/VCO2 | −9.18 | −11.99 | −6.03 | −3.09 | −6.83 | 0.35 |
| VE/VO2 | −13.34 | −17.89 | −6.71 | 4.02 | −2.95 | 7.97 |
| VO2 | −11.69 | −17.16 | −8.23 | 8.40 | 0.72 | 15.35 |
| VE | −19.84 | −28.50 | −13.16 | 11.18 | 2.40 | 19.17 |
| TV | 11.35 | 2.82 | 20.67 | 21.55 | 4.89 | 27.65 |
| RER | −4.96 | −11.80 | −4.23 | 4.62 | 1.22 | 9.56 |
| HR | −6.21 | −8.44 | −3.57 | 4.73 | 2.89 | 6.84 |
| O2 pulse | −7.18 | −11.94 | −1.97 | 1.59 | −2.83 | 10.09 |
| PetO2 | −5.69 | −7.66 | −2.82 | 0.92 | −0.90 | 2.08 |
| PetCO2 | −4.88 | −5.53 | −2.88 | −3.36 | −4.88 | 0.00 |
| p-Value | BF | VCO2 | VE/VCO2 | VE/VO2 | VO2 | VE | TV | RER | HR | O2pulse | PetO2 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| VCO2 | 1 | - | - | - | - | - | - | - | - | - | - |
| VE/VCO2 | 0.0347 | 1 | - | - | - | - | - | - | - | - | - |
| VE/VO2 | 0.2909 | 1 | 1 | - | - | - | - | - | - | - | - |
| VO2 | 0.6629 | 1 | 1 | 1 | - | - | - | - | - | - | - |
| VE | 1 | 1 | 0.7417 | 1 | 1 | - | - | - | - | - | - |
| TV | <0.0001 | <0.0001 | 0.0004 | <0.0001 | <0.0001 | <0.0001 | - | - | - | - | - |
| RER | 0.0003 | 0.0917 | 1 | 1 | 1 | 0.0166 | 0.0400 | - | - | - | - |
| HR | 0.0001 | 0.0300 | 1 | 1 | 1 | 0.0048 | 0.1197 | 1 | - | - | - |
| O2pulse | <0.0001 | 0.0224 | 1 | 1 | 1 | 0.0035 | 0.1553 | 1 | 1 | - | - |
| PetO2 | <0.0001 | 0.0011 | 1 | 0.4695 | 0.2004 | 0.0001 | 1 | 1 | 1 | 1 | - |
| PetCO2 | <0.0001 | 0.0013 | 1 | 0.5274 | 0.2272 | 0.0001 | 1 | 1 | 1 | 1 | 1 |

3.2. Comparison with the CPET1 Run at AT
3.3. Comparison with the CPET1 Run at RCP
3.4. Relative Changes of CPET Parameters between CPET2 and CPET1 at AT
3.5. Comparison of Relative Changes of CPET Parameters between CPET2 and CPET1 at AT
3.6. Correlation of Relative Changes of CPET Parameters (between CPET2 and CPET1 at AT) and Change in Weight
4. Discussion
4.1. Breathing Mechanics
4.2. O2 Consumption and CO2 Production
4.3. Energy Metabolism in Aerobic and Aerobic-Anaerobic Zones
4.4. Effects of Body Weight Reduction on PetO2
4.5. Effects of Body Weight Reduction on CPET Parameters
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guzik, A.; Bushnell, C. Stroke Epidemiology and Risk Factor Management. Contin Lifelong Learn. Neurol 2017, 23, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Mandviwala, T.; Khalid, U.; Deswal, A. Obesity and Cardiovascular Disease: A Risk Factor or a Risk Marker? Curr. Atheroscler. Rep. 2016, 18, 21. [Google Scholar] [CrossRef] [PubMed]
- De Pergola, G.; Silvestris, F. Obesity as a Major Risk Factor for Cancer. J. Obes. 2013, 2013, 291546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aras, M.; Tchang, B.G.; Pape, J. Obesity and Diabetes. Nurs. Clin. N. Am. 2021, 56, 527–541. [Google Scholar] [CrossRef] [PubMed]
- Kachur, S.; Lavie, C.J.; de Schutter, A.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular diseases. Minerva Med 2017, 108, 212–228. [Google Scholar] [CrossRef]
- Panahi, S.; Tremblay, A. Sedentariness and Health: Is Sedentary Behavior More Than Just Physical Inactivity? Front. Public Health 2018, 6, 258. [Google Scholar] [CrossRef] [Green Version]
- Wadden, T.A.; Butryn, M.L.; Wilson, C. Lifestyle Modification for the Management of Obesity. Gastroenterology 2007, 132, 2226–2238. [Google Scholar] [CrossRef]
- Newsome, P.N.; Buchholtz, K.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.J.; Sejling, A.S.; Harrison, S.A. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2021, 384, 1113–1124. [Google Scholar] [CrossRef]
- Ojeniran, M.; Dube, B.; Paige, A.; Ton, J.; Lindblad, A.J. Semaglutide for weight loss. Can. Fam. Physician 2021, 67, 842. [Google Scholar] [CrossRef]
- Lundgren, J.R.; Janus, C.; Jensen, S.B.K.; Juhl, C.R.; Olsen, L.M.; Christensen, R.M.; Svane, M.S.; Bandholm, T.; Bojsen-Møller, K.N.; Blond, M.B.; et al. Healthy Weight Loss Maintenance with Exercise, Liraglutide, or Both Combined. N. Engl. J. Med. 2021, 384, 1719–1730. [Google Scholar] [CrossRef]
- Grunvald, E.; Shah, R.; Hernaez, R.; Chandar, A.K.; Pickett-Blakely, O.; Teigen, L.M.; Harindhanavudhi, T.; Sultan, S.; Singh, S.; Davitkov, P.; et al. AGA Clinical Practice Guideline on Pharmacological Interventions for Adults With Obesity. Gastroenterology 2022, 163, 1198–1225. [Google Scholar] [CrossRef]
- Grover, B.T.; Morell, M.C.; Kothari, S.N.; Borgert, A.J.; Kallies, K.J.; Baker, M.T. Defining Weight Loss After Bariatric Surgery: A Call for Standardization. Obes. Surg. 2019, 29, 3493–3499. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery: A Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, K.F.; Shulman, G.I. Etiology of Insulin Resistance. Am. J. Med. 2006, 119, S10–S16. [Google Scholar] [CrossRef] [Green Version]
- Tchernof, A.; Després, J.-P. Pathophysiology of Human Visceral Obesity: An Update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Leiva, A. What are the benefits of moderate weight loss? Exp. Clin. Endocrinol. Diabetes 2009, 106, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Vidal, J. Updated review on the benefits of weight loss. Int. J. Obes. 2002, 26, S25–S28. [Google Scholar] [CrossRef] [Green Version]
- Rueda-Clausen, C.F.; Ogunleye, A.A.; Sharma, A.M. Health Benefits of Long-Term Weight-Loss Maintenance. Annu. Rev. Nutr. 2015, 35, 475–516. [Google Scholar] [CrossRef]
- Glaab, T.; Taube, C. Practical guide to cardiopulmonary exercise testing in adults. Respir. Res. 2022, 23, 9. [Google Scholar] [CrossRef]
- Sietsema, K.E.; Sue, D.Y.; Stringer, W.W.; Ward, S.A. Wasserman & Whipp’s Principles of Exercise Testing and Interpretation; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2021. [Google Scholar]
- Gruchała-Niedoszytko, M.; Niedoszytko, P.; Kaczkan, M.; Pieszko, M.; Gierat-Haponiuk, K.; Śliwińska, A.; Skotnicka, M.; Szalewska, D.; Małgorzewicz, S. Cardiopulmonary Excercise Test and Bioimpedance as prediction tools used to predict the outcomes of obesity treatment. Pol. Arch. Intern. Med. 2019, 129, 225–233. [Google Scholar] [CrossRef]
- Sawicka-Gutaj, N.; Gruszczyński, D.; Guzik, P.; Mostowska, A.; Walkowiak, J. Publication ethics of human studies in the light of the Declaration of Helsinki–A mini-review. J. Med. Sci. 2022, 91, e700. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Stephens, P.; McBride, M.G.; Paridon, S.M. CHAPTER 20-Cardiopulmonary Stress Testing. In Paediatric Cardiology, 3rd ed.; Anderson, R.H., Baker, E.J., Penny, D.J., Redington, A.N., Rigby, M.L., Wernovsky, G., Eds.; Churchill Livingstone: Philadelphia, PA, USA, 2010; pp. 415–436. [Google Scholar] [CrossRef]
- Myers, J.; Froelicher, V.F. Exercise Testing. Cardiol. Clin. 1993, 11, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Kozlov, S.; Caprnda, M.; Chernova, O.; Matveeva, M.; Alekseeva, I.; Gazdikova, K.; Gaspar, L.; Kruzliak, P.; Filipova, S.; Gabbasov, Z. Peak Responses during Exercise Treadmill Testing using Individualized Ramp Protocol and Modified Bruce Protocol in Elderly Patients. Folia Med. (Plovdiv) 2020, 62, 76–81. [Google Scholar] [CrossRef]
- Wasserman, K.; Whipp, B.J.; Koyl, S.N.; Beaver, W.L. Anaerobic threshold and respiratory gas exchange during exercise. J. Appl. Physiol. 1973, 35, 236–243. [Google Scholar] [CrossRef]
- Kinnear, W.J.M.; Blakey, J. A Practical Guide to the Interpretation of Cardiopulmonary Exercise Tests; Oxford Respiratory Medicine Library: Oxford, UK, 2014. [Google Scholar]
- Balmain, B.N.; Halverson, Q.M.; Tomlinson, A.R.; Edwards, T.; Ganio, M.S.; Babb, T.G. Obesity Blunts the Ventilatory Response to Exercise in Men and Women. Ann. Am. Thorac. Soc. 2021, 18, 1167–1174. [Google Scholar] [CrossRef]
- McMurray, R.G.; Ondrak, K.S. Effects of being overweight on ventilatory dynamics of youth at rest and during exercise. Eur. J. Appl. Physiol. 2011, 111, 285–292. [Google Scholar] [CrossRef]
- Bernhardt, V.; Babb, T.G. Exertional dyspnoea in obesity. Eur. Respir. Rev. 2016, 25, 487–495. [Google Scholar] [CrossRef] [Green Version]
- Borasio, N.; Neunhaeuserer, D.; Gasperetti, A.; Favero, C.; Baioccato, V.; Bergamin, M.; Busetto, L.; Foletto, M.; Vettor, R.; Ermolao, A. Ventilatory Response at Rest and During Maximal Exercise Testing in Patients with Severe Obesity Before and After Sleeve Gastrectomy. Obes. Surg. 2021, 31, 694–701. [Google Scholar] [CrossRef]
- Richman, P.S.; Yeung, P.; Bilfinger, T.V.; Yang, J.; Stringer, W.W. Exercise Capacity in Unilateral Diaphragm Paralysis: The Effect of Obesity. Pulm. Med. 2019, 2019, 1090982. [Google Scholar] [CrossRef] [Green Version]
- Bhammar, D.M.; Stickford, J.L.; Bernhardt, V.; Babb, T.G. Effect of weight loss on operational lung volumes and oxygen cost of breathing in obese women. Int. J. Obes. 2016, 40, 998–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanak, R.; Fahey, P.J.; Vanderwarf, C. Oxygen Cost of Breathing. Chest 1985, 87, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Hakala, K.; Mustajoki, P.; Aittomäki, J.; Sovijärvi, A. Improved gas exchange during exercise after weight loss in morbid obesity. Clin. Physiol. 1996, 16, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Hulens, M.; Vansant, G.; Lysens, R.; Claessens, A.L.; Muls, E. Exercise capacity in lean versus obese women. Scand. J. Med. Sci. Sports 2001, 11, 305–309. [Google Scholar] [CrossRef]
- Wolfe, R.R. Fat Metabolism in Exercise. In Skeletal Muscle Metabolism in Exercise and Diabetes; Richter, E.A., Kiens, B., Galbo, H., Saltin, B., Eds.; Springer: Boston, MA, USA, 1998; Volume 441, pp. 147–156. [Google Scholar] [CrossRef]
- Hargreaves, M.; Spriet, L.L. Skeletal muscle energy metabolism during exercise. Nat. Metab. 2020, 2, 817–828. [Google Scholar] [CrossRef]
- Harris, M.B.; Kuo, C.-H. Scientific Challenges on Theory of Fat Burning by Exercise. Front. Physiol. 2021, 12, 685166. [Google Scholar] [CrossRef]
- Achten, J.; Jeukendrup, A.E. Optimizing fat oxidation through exercise and diet. Nutrition 2004, 20, 716–727. [Google Scholar] [CrossRef]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H.; Schmid, J.P. Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 726–734. [Google Scholar] [CrossRef]
- Nedeljkovic-Arsenovic, O.; Banovic, M.; Radenkovic, D.; Rancic, N.; Polovina, S.; Micic, D.; Nedeljkovic, I. The Amount of Weight Loss Six Months after Bariatric Surgery: It Makes a Difference. Obes. Facts 2019, 12, 281–290. [Google Scholar] [CrossRef]
- Herdy, A.H.; Uhlendorf, D. Valores de referência para o teste cardiopulmonar para homens e mulheres sedentários e ativos. Arq. Bras. Cardiol. 2011, 96, 54–59. [Google Scholar] [CrossRef]
- Ingle, L.; Rigby, A.; Brodie, D.; Sandercock, G. Normative reference values for estimated cardiorespiratory fitness in apparently healthy British men and women. PLoS ONE 2020, 15, e0240099. [Google Scholar] [CrossRef] [PubMed]
- Wilms, B.; Ernst, B.; Thurnheer, M.; Weisser, B.; Schultes, B. Differential Changes in Exercise Performance After Massive Weight Loss Induced by Bariatric Surgery. Obes. Surg. 2013, 23, 365–371. [Google Scholar] [CrossRef] [PubMed]
| Median | LQ | UQ | |
|---|---|---|---|
| Age (years) | 26 | 23 | 42 |
| Training days a week (days) | 5 | 4 | 7 |
| Training hours a week (hours) | 8 | 5 | 16 |
| Height (cm) | 182 | 175 | 184 |
| Body mass (kg) | 73.5 | 67.0 | 78.5 |
| Delta mass (%) | 14.04 | 13.26 | 15.19 |
| BMI (kg/m2) | 22.20 | 21.18 | 25.86 |
| BMI +12 kg (kg/m2) | 25.81 | 25.03 | 29.82 |
| Treadmill velocity at AT (km/h) | 12.4 | 11.7 | 13.0 |
| Treadmill velocity at RCP (km/h) | 15.50 | 14.48 | 16.15 |
| Maximal treadmill velocity (km/h) | 17.15 | 16.25 | 17.93 |
| RVIDd (mm) | 34.0 | 31.0 | 37.5 |
| IVSd (mm) | 9 | 8 | 9 |
| LVIDd (mm) | 50.0 | 47.5 | 54.5 |
| LVPWd (mm) | 9.0 | 9.0 | 10.5 |
| LVIDs (mm) | 40.5 | 34.0 | 42.0 |
| LVEF (%) | 63.2 | 61.4 | 64.4 |
| LADs (mm) | 38 | 34 | 41 |
| MV E (m/s) | 0.75 | 0.65 | 0.84 |
| MV A (m/s) | 0.44 | 0.41 | 0.53 |
| E/E’ mean | 4.83 | 4.70 | 5.47 |
| AV Vmax (m/s) | 1.19 | 1.10 | 1.31 |
| LAI (mL/m2) | 41.99 | 30.79 | 49.62 |
| Rest | Peak Exercise | |||||
|---|---|---|---|---|---|---|
| Median | LQ | UQ | Median | LQ | UQ | |
| BF (breaths/min) | 17.0 | 13.3 | 21.0 | 50.5 | 47.5 | 59.5 |
| VCO2 (L/min) | 0.38 | 0.29 | 0.48 | 4.54 | 3.98 | 4.78 |
| VE/VCO2 | 32.4 | 29.9 | 34.0 | 30.9 | 29.1 | 32.0 |
| VE/VO2 | 27.0 | 23.9 | 29.6 | 36.8 | 32.9 | 38.2 |
| VO2 (L/min) | 0.46 | 0.37 | 0.54 | 3.83 | 3.46 | 4.12 |
| VO2kg (L/min × kg) | 5.92 | 5.23 | 7.21 | 50.16 | 47.49 | 52.69 |
| VE (L/min) | 14.33 | 9.97 | 16.42 | 146.41 | 126.48 | 160.39 |
| TV (L) | 0.84 | 0.68 | 1.15 | 2.72 | 2.51 | 3.01 |
| RER | 0.85 | 0.78 | 0.92 | 1.17 | 1.12 | 1.21 |
| HR (beats/min) | 79 | 70 | 88 | 184 | 181 | 195 |
| O2pulse (mL/beat) | 5.78 | 5.04 | 6.64 | 20.26 | 18.18 | 22.79 |
| PetO2 (mmHg) | 110.0 | 104.0 | 111.3 | 116.5 | 112.8 | 118.0 |
| PetCO2 (mmHg) | 35.5 | 34.5 | 37.0 | 37.5 | 36.8 | 40.0 |
| Correlation between the Relative Body Weight Reduction and CPET Parameters between Running with a +12 kg Vest at vAT and | ||||
|---|---|---|---|---|
| Without the Vest at vAT | Without the Vest at vRCP | |||
| rho | p-Value | rho | p-Value | |
| BF | −0.07 | 0.7821 | 0.00 | 0.9849 |
| VCO2 | −0.18 | 0.4410 | 0.09 | 0.7113 |
| VE/VCO2 | −0.24 | 0.3052 | −0.12 | 0.6212 |
| VE/VO2 | 0.04 | 0.8696 | 0.01 | 0.9824 |
| VO2 | −0.24 | 0.3067 | −0.14 | 0.5573 |
| VE | −0.16 | 0.4884 | −0.09 | 0.6995 |
| VT | −0.13 | 0.5900 | −0.06 | 0.7931 |
| RER | 0.03 | 0.9095 | 0.24 | 0.3146 |
| HR | 0.02 | 0.9245 | 0.39 | 0.0871 |
| O2 pulse | −0.31 | 0.1834 | −0.22 | 0.3575 |
| PetO2 | −0.10 | 0.6646 | −0.31 | 0.1767 |
| PetCO2 | −0.02 | 0.9332 | 0.06 | 0.8109 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pytka, M.J.; Domin, R.A.; Tarchalski, J.L.; Lubarska, M.I.; Żołyński, M.S.; Niziński, J.; Piskorski, J.; Wykrętowicz, A.; Guzik, P. A Human Model of the Effects of an Instant Sheer Weight Loss on Cardiopulmonary Parameters during a Treadmill Run. J. Clin. Med. 2023, 12, 98. https://doi.org/10.3390/jcm12010098
Pytka MJ, Domin RA, Tarchalski JL, Lubarska MI, Żołyński MS, Niziński J, Piskorski J, Wykrętowicz A, Guzik P. A Human Model of the Effects of an Instant Sheer Weight Loss on Cardiopulmonary Parameters during a Treadmill Run. Journal of Clinical Medicine. 2023; 12(1):98. https://doi.org/10.3390/jcm12010098
Chicago/Turabian StylePytka, Michał J., Remigiusz A. Domin, Jacek L. Tarchalski, Marta I. Lubarska, Mikołaj S. Żołyński, Jan Niziński, Jarosław Piskorski, Andrzej Wykrętowicz, and Przemysław Guzik. 2023. "A Human Model of the Effects of an Instant Sheer Weight Loss on Cardiopulmonary Parameters during a Treadmill Run" Journal of Clinical Medicine 12, no. 1: 98. https://doi.org/10.3390/jcm12010098