

Association of Alpha-1 Antitrypsin Pi*Z Allele Frequency and Progressive Liver Fibrosis in Two Chronic Hepatitis C Cohorts

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patients’ Characteristics
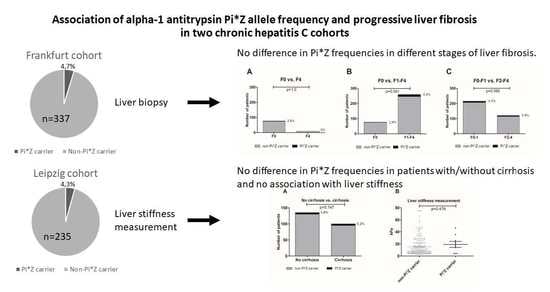
3.2. Frankfurt Cohort—No Difference in Pi*Z Frequencies in Patients with Different Stages of Liver Fibrosis
3.3. Leipzig Cohort—No Difference in Pi*Z Frequencies in Patients with/without Cirrhosis and No Association with Liver Stiffness or Serologic Fibrosis Parameters
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choo, Q.-L.; Kuo, G.; Weiner, A.J.; Overby, L.R.; Bradley, D.W.; Houghton, M. Isolation of a cDNA cLone Derived from a Blood-Borne Non-A, Non-B Viral Hepatitis Genome. Science 1989, 244, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Vermehren, J.; Park, J.S.; Jacobson, I.M.; Zeuzem, S. Challenges and perspectives of direct antivirals for the treatment of hepatitis C virus infection. J. Hepatol. 2018, 69, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.P.; El-Serag, H.B.; Kanwal, F. Global epidemiology and burden of HCV infection and HCV-related disease. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.J.; Liang, T.J. Hepatitis C—identifying patients with progressive liver injury. Hepatology 2006, 43, S194–S206. [Google Scholar] [CrossRef]
- Missiha, S.B.; Ostrowski, M.; Heathcote, E.J. Disease Progression in Chronic Hepatitis C: Modifiable and Nonmodifiable Factors. Gastroenterology 2008, 134, 1699–1714. [Google Scholar] [CrossRef]
- Strnad, P.; McElvaney, N.G.; Lomas, D.A. Alpha1-Antitrypsin Deficiency. N. Engl. J. Med. 2020, 382, 1443–1455. [Google Scholar] [CrossRef]
- Katzer, D.; Ganschow, R.; Strnad, P.; Hamesch, K. Pi∗ZZ-related liver disease in children and adults—Narrative review of the typical presentation and management of alpha-1 antitrypsin deficiency. Dig. Med. Res. 2021, 4, 31. [Google Scholar] [CrossRef]
- Greene, C.M.; Marciniak, S.J.; Teckman, J.; Ferrarotti, I.; Brantly, M.L.; Lomas, D.A.; Stoller, J.K.; McElvaney, N.G. Alpha1-Antitrypsin deficiency. Nat. Rev. Dis. Prim. 2016, 2, 16051. [Google Scholar] [CrossRef]
- Luisetti, M.; Seersholm, N. Alpha1-antitrypsin deficiency. 1: Epidemiology of alpha1-antitrypsin deficiency. Thorax 2004, 59, 164–169. [Google Scholar] [CrossRef]
- Segeritz, C.P.; Rashid, S.T.; de Brito, M.C.; Serra, M.P.; Ordonez, A.; Morell, C.M.; Kaserman, J.E.; Madrigal, P.; Hannan, N.R.; Gatto, L.; et al. hiPSC hepatocyte model demonstrates the role of unfolded protein response and inflammatory networks in alpha1-antitrypsin deficiency. J. Hepatol. 2018, 69, 851–860. [Google Scholar] [CrossRef]
- Hamesch, K.; Mandorfer, M.; Pereira, V.M.; Moeller, L.S.; Pons, M.; Dolman, G.E.; Reichert, M.C.; Schneider, C.V.; Woditsch, V.; Voss, J.; et al. Liver Fibrosis and Metabolic Alterations in Adults With alpha-1-antitrypsin Deficiency Caused by the Pi∗ZZ Mutation. Gastroenterology 2019, 157, 705–719.e18. [Google Scholar] [CrossRef]
- Clark, V.C.; Marek, G.; Liu, C.; Collinsworth, A.; Shuster, J.; Kurtz, T.; Nolte, J.; Brantly, M. Clinical and histologic features of adults with alpha-1 antitrypsin deficiency in a non-cirrhotic cohort. J. Hepatol. 2018, 69, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Fromme, M.; Schneider, C.V.; Pereira, V.; Hamesch, K.; Pons, M.; Reichert, M.C.; Benini, F.; Ellis, P.; Thorhauge, K.H.; Mandorfer, M.; et al. Hepatobiliary phenotypes of adults with alpha-1 antitrypsin deficiency. Gut 2021, 71, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Kümpers, J.; Fromme, M.; Schneider, C.V.; Trautwein, C.; Denk, H.; Hamesch, K.; Strnad, P. Assessment of liver phenotype in adults with severe alpha-1 antitrypsin deficiency (Pi∗ZZ genotype). J. Hepatol. 2019, 71, 1272–1274. [Google Scholar] [CrossRef] [PubMed]
- Tanash, H.A.; Piitulainen, E. Liver disease in adults with severe alpha-1-antitrypsin deficiency. J. Gastroenterol. 2019, 54, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Strnad, P.; Buch, S.; Hamesch, K.; Fischer, J.; Rosendahl, J.; Schmelz, R.; Brueckner, S.; Brosch, M.; Heimes, C.V.; Woditsch, V.; et al. Heterozygous carriage of the alpha1-antitrypsin Pi∗Z variant increases the risk to develop liver cirrhosis. Gut 2019, 68, 1099–1107. [Google Scholar] [CrossRef]
- Schneider, C.V.; Hamesch, K.; Gross, A.; Mandorfer, M.; Moeller, L.S.; Pereira, V.; Pons, M.; Kuca, P.; Reichert, M.C.; Benini, F.; et al. Liver Phenotypes of European Adults Heterozygous or Homozygous for Pi∗Z Variant of AAT (Pi∗MZ vs. Pi∗ZZ genotype) and Non-carriers. Gastroenterology 2020, 159, 534–548.e11. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.V.; Hamesch, K.; Strnad, P. Response to: The Pi∗MZ Allele in Alpha-1 Antitrypsin Increases Liver-Related Outcomes in a Population-Based Study. Gastroenterology 2021, 160, 1874–1875. [Google Scholar]
- Guldiken, N.; Hamesch, K.; Schuller, S.M.; Aly, M.; Lindhauer, C.; Schneider, C.V.; Fromme, M.; Trautwein, C.; Strnad, P. Mild Iron Overload as Seen in Individuals Homozygous for the Alpha-1 Antitrypsin Pi∗Z Variant Does Not Promote Liver Fibrogenesis in HFE Knockout Mice. Cells 2019, 8, 1415. [Google Scholar] [CrossRef]
- Hakim, A.; Moll, M.; Qiao, D.; Liu, J.; Lasky-Su, J.A.; Silverman, E.K.; Vilarinho, S.; Jiang, Z.G.; Hobbs, B.D.; Cho, M.H. Heterozygosity of the Alpha 1-Antitrypsin Pi∗Z Allele and Risk of Liver Disease. Hepatol. Commun. 2021, 5, 1348–1361. [Google Scholar] [CrossRef]
- Motawi, T.; Shaker, O.; Hussein, R.; Houssen, M. Polymorphisms of α1-antitrypsin and Interleukin-6 genes and the progression of hepatic cirrhosis in patients with a hepatitis C virus infection. Balk. J. Med. Genet. 2016, 19, 35–44. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Propst, T.; Propst, A.; Dietze, O.; Judmaier, G.; Braunsteiner, H.; Vogel, W. Prevalence of hepatocellular carcinoma in alpha-1-antitrypsin deficiency. J. Hepatol. 1994, 21, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Regev, A.; Guaqueta, C.; Molina, E.G.; Conrad, A.; Mishra, V.; Brantly, M.L.; Torres, M.; De Medina, M.; Tzakis, A.G.; Schiff, E.R. Does the Heterozygous State of Alpha-1 Antitrypsin Deficiency Have a Role in Chronic Liver Diseases? Interim Results of a Large Case-Control Study. J. Craniofacial. Surg. 2006, 43, S30–S35. [Google Scholar] [CrossRef]
- Scott, B.B.; Egner, W. Does alpha1-antitrypsin phenotype PiMZ increase the risk of fibrosis in liver disease due to hepatitis C virus infection? Eur. J. Gastroenterol. Hepatol. 2006, 18, 521–523. [Google Scholar] [CrossRef] [PubMed]
- Serfaty, L.; Chazouilleres, O.; Poujol-Robert, A.; Morand-Joubert, L.; Dubois, C.; Chretien, Y.; Poupon, R.E.; Petit, J.C.; Poupon, R.A. Risk factors for cirrhosis in patients with chronic hepatitis C virus infection: Results of a case-control study. Hepatology 1997, 26, 776–779. [Google Scholar] [CrossRef]
- Sarrazin, C.; Schwendy, S.; Möller, B.; Dikopoulos, N.; Buggisch, P.; Encke, J.; Teuber, G.; Goeser, T.; Thimme, R.; Klinker, H.; et al. Improved Responses to Pegylated Interferon Alfa-2b and Ribavirin by Individualizing Treatment for 24–72 Weeks. Gastroenterology 2011, 141, 1656–1664. [Google Scholar] [CrossRef]
- Fischer, J.; Böhm, S.; Müller, T.; Witt, H.; Sarrazin, C.; Susser, S.; Migaud, P.; Schott, E.; Stewart, G.; Brodzinski, A.; et al. Association of IFNL3 rs12979860 and rs8099917 with Biochemical Predictors of Interferon Responsiveness in Chronic Hepatitis C Virus Infection. PLoS ONE 2013, 8, e77530. [Google Scholar] [CrossRef]
- Fischer, J.; Weber, A.; Böhm, S.; Dickhöfer, S.; El Maadidi, S.; Deichsel, D.; Knop, V.; Klinker, H.; Möller, B.; Rasenack, J.; et al. Sex-specific effects of TLR9 promoter variants on spontaneous clearance of HCV infection. Gut 2017, 66, 1829–1837. [Google Scholar] [CrossRef]
- Thabet, K.; Asimakopoulos, A.; Shojaei, M.; Romero-Gomez, M.; Mangia, A.; Irving, W.L.; Berg, T.; Dore, G.J.; Grønbæk, H.; Sheridan, D.; et al. MBOAT7 rs641738 increases risk of liver inflammation and transition to fibrosis in chronic hepatitis C. Nat. Commun. 2016, 7, 12757. [Google Scholar] [CrossRef]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef]
- Lin, Z.-H.; Xin, Y.-N.; Dong, Q.-J.; Wang, Q.; Jiang, X.-J.; Zhan, S.-H.; Sun, Y.; Xuan, S.-Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Castéra, L.; Vergniol, J.; Foucher, J.; Le Bail, B.; Chanteloup, E.; Haaser, M.; Darriet, M.; Couzigou, P.; de Lédinghen, V. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology 2005, 128, 343–350. [Google Scholar] [CrossRef]
- Hamesch, K.; Strnad, P. Non-Invasive Assessment and Management of Liver Involvement in Adults with Alpha-1 Antitrypsin Deficiency. Chronic Obstr. Pulm. Dis. J. COPD Found. 2020, 7, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Graziadei, I.W.; Joseph, J.J.; Wiesner, R.H.; Therneau, T.M.; Batts, K.P.; MD., M.K.P. Increased risk of chronic liver failure in adults with heterozygous α-antitrypsin deficiency. Hepatology 1998, 28, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Hodges, J.R.; Millward-Sadler, G.H.; Barbatis, C.; Wright, R.; Heterozygous, M.Z. Alpha 1-antitrypsin deficiency in adults with chronic active hepatitis and cryptogenic cirrhosis. N. Engl. J. Med. 1981, 304, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.L.; Taylor, L.; Sherlock, S. Alpha-1-antitrypsin deficiency in liver disease: The extent of the problem. Gastroenterology 1976, 71, 646–651. [Google Scholar] [CrossRef]
- Vecchio, F.; Fabiano, A.; Orsini, G.; Ragusa, D.; Massi, G. Alpha-1-Antitrypsin MZ Phenotype and Cryptogenic Chronic Liver Disease in Adults. Digestion 1983, 27, 100–104. [Google Scholar] [CrossRef]
- Abul-Husn, N.S.; Cheng, X.; Li, A.H.; Xin, Y.; Schurmann, C.; Stevis, P.; Liu, Y.; Kozlitina, J.; Stender, S.; Wood, G.C.; et al. A Protein-Truncating HSD17B13 Variant and Protection from Chronic Liver Disease. N. Engl. J. Med. 2018, 378, 1096–1106. [Google Scholar] [CrossRef]
- Eigenbrodt, M.L.; McCashland, T.M.; Dy, R.M.; Clark, J.; Galati, J. Heterozygous alpha 1-antitrypsin phenotypes in patients with end stage liver disease. Am. J. Gastroenterol. 1997, 92, 602–607. [Google Scholar]
- Bochud, P.-Y.; Cai, T.; Overbeck, K.; Bochud, M.; Dufour, J.-F.; Müllhaupt, B.; Borovicka, J.; Heim, M.; Moradpour, D.; Cerny, A.; et al. Genotype 3 is associated with accelerated fibrosis progression in chronic hepatitis C. J. Hepatol. 2009, 51, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Martinez-González, C.; Blanco, I.; Diego, I.; Bueno, P.; Miravitlles, M. Estimated Prevalence and Number of PiMZ Genotypes of Alpha-1 Antitrypsin in Seventy-Four Countries Worldwide. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 2617–2630. [Google Scholar] [CrossRef] [PubMed]
- Blanco, I.; Bueno, P.; Diego, I.; Pérez-Holanda, S.; Casas, F.; Esquinas, C.; Miravitlles, M. Alpha-1 antitrypsin Pi∗Z gene frequency and Pi∗ZZ genotype numbers worldwide: An update. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 561–569. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address eee, Clinical Practice Guidelines Panel C, representative EGB, Panel m. EASL recommendations on treatment of hepatitis C: Final update of the series(☆). J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Friedrich-Rust, M.; Poynard, T.; Castera, L. Critical comparison of elastography methods to assess chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 402–411. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Total, n = 337 | Pi*Z Non-Carriers, n = 321 | Pi*Z Carriers, n = 16 | Significance (p Value) |
|---|---|---|---|---|
| Age (years) | 42.7 ± 11.1 | 42.6 ± 11.2 | 45.6 ± 8.2 | 0.228 |
| Men (n) | 156 (46.2) | 146 (45.5) | 10 (62.5) | 0.207 |
| BMI (kg/m²) | 25.7 ± 4.5 | 25.6 ± 4.5 | 26.9 ± 3.6 | 0.087 |
| HCV genotype | 0.756 | |||
| 1 (n) | 60 (17.8) | 56 (17.4) | 4 (25) | |
| 2 (n) | 86 (25.5) | 83 (25.9) | 3 (18.8) | |
| 3 (n) | 185 (54.9) | 176 (54.8) | 9 (56.3) | |
| 5 (n) | 6 (1.8) | 6 (1.9) | 0 (0) | |
| ALT (U/L) | 81.6 ± 58.7 | 81.5 ± 58.5 | 86.2 ± 64.2 | 0.879 |
| AST (U/L) | 56.0 ± 39.1 | 55.9 ± 39.1 | 56.9 ± 40.5 | 0.864 |
| GGT (U/L) | 68.5 ± 70.9 | 67.3 ± 70.6 | 91.4 ± 75.2 | 0.046 * |
| Bilirubin (mg/dL) | 0.7 ± 0.3 | 0.7 ± 0.3 | 0.6 ± 0.3 | 0.117 |
| Albumin (g/dL) | 4.5 ± 0.4 | 4.4 ± 0.3 | 4.5 ± 0.3 | 0.248 |
| Creatinine (mg/dL) | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.8 ± 0.1 | 0.388 |
| Hemoglobin (g/dL) | 14.8 ± 1.4 | 14.8 ± 1.4 | 14.7 ± 1.4 | 0.607 |
| Leucocytes (/nL) | 6.9 ± 2.1 | 6.9 ± 2.1 | 7.2 ± 1.9 | 0.338 |
| Platelets (/nL) | 240 ± 63 | 240 ± 63 | 244 ± 71 | 0.959 |
| HbA1c (%) | 5.4 ± 0.4 | 5.4 ± 0.4 | 5.3 ± 0.3 | 0.378 |
| HOMA-IR score | 3.2 ± 3.4 | 3.2 ± 3.5 | 2.4 ± 2.0 | 0.528 |
| Parameters | Total, n = 337 | Pi*Z Non-Carriers, n = 321 | Pi*Z Carriers, n = 16 | Significance (p Value) |
|---|---|---|---|---|
| Biopsy-determined stage of fibrosis | ||||
| F0 (n) | 77 (22.8) | 75 (23.4) | 2 (12.5) | 0.541 |
| F1 (n) | 139 (41.2) | 132 (41.1) | 7 (43.6) | 1.0 |
| F2 (n) | 73 (21.7) | 69 (21.5) | 4 (25) | 0.753 |
| F3 (n) | 38 (11.2) | 35 (10.9) | 3 (18.6) | 0.405 |
| F4 (n) | 10 (3.0) | 10 (3.1) | 0 (0) | 1.0 |
| Serologic scores | ||||
| APRI score | 0.56 ± 0.21 | 0.56 ± 0.21 | 0.52 ± 0.21 | 0.444 |
| APRI score < 0.5 (n) | 152 (45.1) | 143 (44.5) | 9 (56.2) | 0.443 |
| APRI score > 1 (n) | 8 (2.3) | 8 (2.5) | 0 (0) | 1.0 |
| FIB-4 score | 1.27 ± 1.01 | 1.28 ± 1.03 | 1.21 ± 0.55 | 0.516 |
| FIB-4 score < 1.45 (n) | 248 (73.6) | 235 (73.2) | 13 (81.3) | 0.575 |
| FIB-4 Score > 3.25 (n) | 15 (4.5) | 15 (4.7) | 0 (0) | 1.0 |
| Variables (n = 216) | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age | 1.080 (1.041–1.121) | <0.001 | 1.079 (1.038–1.122) | <0.001 |
| Female sex | 1.532 (0.725–3.324) | 0.264 | ||
| Body mass index | 1.113 (1.033–1.198) | 0.005 | 1.107 (1.021–1.200) | 0.014 |
| Genotype 3 | 1.061 (0.506–2.228) | 0.875 | ||
| Hemoglobin A1c | 1.831 (0.864–3.879) | 0.114 | ||
| Pi*Z heterozygosity | 2.330 (0.569–9.550) | 0.240 | ||
| Parameters | Total, n = 235 | Pi*Z Non-Carriers, n = 225 | Pi*Z Carriers, n = 10 | Significance (p Value) |
|---|---|---|---|---|
| LSM (kPa) | 15.5 ± 14.9 | 15.3 ± 15.0 | 19.2 ± 14.8 | 0.479 |
| LSM cut-offs HCV, (n) | ||||
| <7.1 kPa | 80 (34.0) | 77 (34.2) | 3 (30) | 1.0 |
| 7.1–<9.5 kPa | 24 (10.2) | 24 (10.7) | 0 (0) | 0.604 |
| 9.5–<12.5 kPa | 13 (5.5) | 13 (5.8) | 0 (0) | 1.0 |
| ≥12.5kPa | 76 (32.3) | 70 (31.1) | 6 (60) | 0.081 |
| LSM cut-offs A1ATD, (n) | ||||
| <7.1 kPa | 80 (34.0) | 77 (34.2) | 3 (30) | 1.0 |
| 7.1–<10.0 kPa | 25 (10.6) | 25 (11.1) | 0 (0) | 0.605 |
| 10.0–<13.0 kPa | 14 (6.0) | 14 (6.2) | 0 (0) | 1.0 |
| ≥13.0 kPa | 74 (14.8) | 68 (30.2) | 6 (60) | 0.076 |
| Serologic scores | ||||
| APRI score | 1.85 ± 2.05 | 1.86 ± 2.09 | 1.63 ± 1.12 | 0.705 |
| APRI score < 0.5 (n) | 44 (18.7) | 43 (19.1) | 1 (10) | 0.693 |
| APRI score > 1 (n) | 118 (50.2) | 112 (49.8) | 6 (60) | 0.749 |
| FIB-4 score | 4.24 ± 4.01 | 4.20 ± 4.03 | 5.01 ± 3.63 | 0.355 |
| FIB-4 score < 1.45 (n) | 59 (25.1) | 57 (25.3) | 2 (20) | 1.0 |
| FIB-4 Score > 3.25 (n) | 92 (39.1) | 86 (38.2) | 6 (60) | 0.195 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mücke, V.T.; Fischer, J.; Mücke, M.M.; Teumer, A.; Koch, A.; Vermehren, J.; Fromme, M.; Zeuzem, S.; Trautwein, C.; Sarrazin, C.; et al. Association of Alpha-1 Antitrypsin Pi*Z Allele Frequency and Progressive Liver Fibrosis in Two Chronic Hepatitis C Cohorts. J. Clin. Med. 2023, 12, 253. https://doi.org/10.3390/jcm12010253
Mücke VT, Fischer J, Mücke MM, Teumer A, Koch A, Vermehren J, Fromme M, Zeuzem S, Trautwein C, Sarrazin C, et al. Association of Alpha-1 Antitrypsin Pi*Z Allele Frequency and Progressive Liver Fibrosis in Two Chronic Hepatitis C Cohorts. Journal of Clinical Medicine. 2023; 12(1):253. https://doi.org/10.3390/jcm12010253
Chicago/Turabian StyleMücke, Victoria Therese, Janett Fischer, Marcus Maximilian Mücke, Alexander Teumer, Alexander Koch, Johannes Vermehren, Malin Fromme, Stefan Zeuzem, Christian Trautwein, Christoph Sarrazin, and et al. 2023. "Association of Alpha-1 Antitrypsin Pi*Z Allele Frequency and Progressive Liver Fibrosis in Two Chronic Hepatitis C Cohorts" Journal of Clinical Medicine 12, no. 1: 253. https://doi.org/10.3390/jcm12010253
APA StyleMücke, V. T., Fischer, J., Mücke, M. M., Teumer, A., Koch, A., Vermehren, J., Fromme, M., Zeuzem, S., Trautwein, C., Sarrazin, C., Berg, T., Zhou, B., & Hamesch, K. (2023). Association of Alpha-1 Antitrypsin Pi*Z Allele Frequency and Progressive Liver Fibrosis in Two Chronic Hepatitis C Cohorts. Journal of Clinical Medicine, 12(1), 253. https://doi.org/10.3390/jcm12010253