
Effect of Ultrasound-Guided Percutaneous Neuromodulation of Sciatic Nerve on Hip Muscle Strength in Chronic Low Back Pain Sufferers: A Pilot Study
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Institutional Review Board
2.3. Participants
2.4. Outcome Measures
- -
- Hip passive internal rotation range of motion (IR-ROM). The authors only recorded the hip IR-ROM because it is the only one that is related to low back pain [6]. The hip passive IR-ROM was measured bilaterally. Each test was carried out three times and the average chosen as the final score. All measurements were performed by two testers, using a hand-held universal goniometer [28]. Tester 1 controlled the patient’s correct position and performed the passive hip movements and tester 2 measured and noted the hip ROM scores. To analyze hip IR, all individuals were positioned prone on a treatment table with the hip in neutral, the knee flexed to 90° and the pelvis stabilized with a belt, and the contralateral limb was placed in approximately 20° of abduction. The tester measured the ROM by bringing the limb to a firm end point of IR. Each test was carried out three times and the average calculated as the final score. Intra-rater reliability was established in the first 15 volunteers as sufficient for clinical measurement. The intraclass correlation coefficient (ICC) and the standard error of measurements (SEM) were 0.91 and 2.72, respectively, for the hip IR-ROM variable, indicating high reliability.
- -
- Hip muscle strength. The hip muscle strength assessments of the hip abduction, external rotation, internal rotation, flexion and extension, were analyzed using a hand-held dynamometer (HHD) (Power Track II Commander/JTECH Medical, Salt Lake City, Ut, USA) [29]. Each measurement was taken bilaterally. The hip flexion and abduction strength were measured in the supine position, the hip extension strength was measured in the prone position, and the hip internal rotation-external rotation strength was measured in the prone position, and in the sitting position. The test positions were chosen based on clinical practice [30], and all strength tests were isometric strength tests, according to previous studies [31]. All patients were instructed in the procedures, and that they should achieve one isometric sub-maximal contraction into the tester’s hand. Each test was carried out three times and the average calculated as the final score. Intra-rater reliability was established in the first 15 volunteers as sufficient for clinical measurement. The ICC and SEM were 0.88 and 4.1, respectively, for the abduction variable, indicating good reliability; 0.91 and 3.5, respectively, for the external rotation variable, indicating high reliability; 0.93 and 4.0, respectively, for the internal rotation variable, indicating high reliability; 0.85 and 2.2, respectively, for the flexion variable, indicating good reliability; and 0.89 and 1.5, respectively, for the extension variable, indicating good reliability.
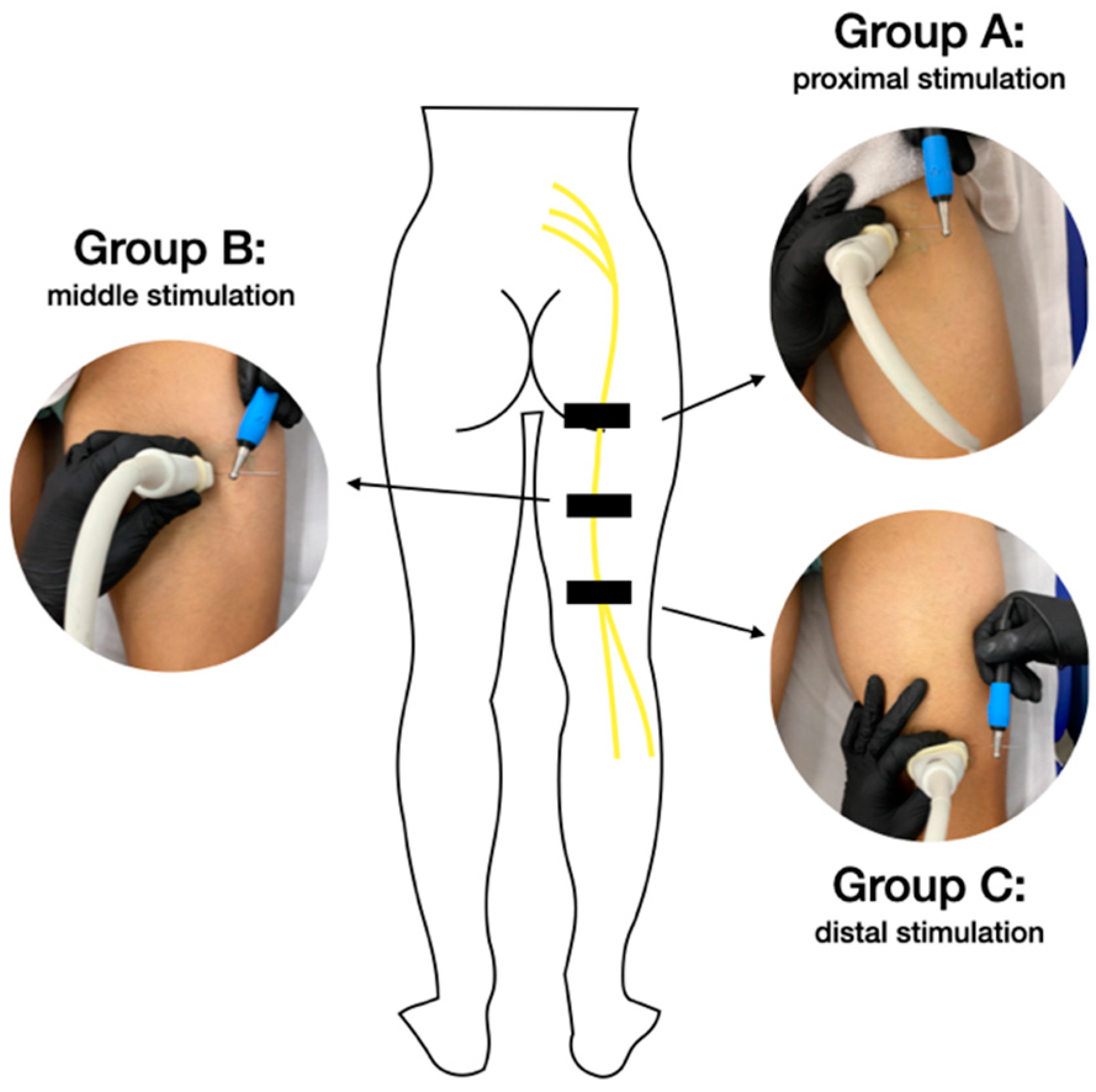
2.5. Ultrasound-Guided PNM Procedure
2.6. Data Analysis
3. Results
4. Discussion
Clinical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bell, J.A.; Burnett, A. Exercise for the primary, secondary and tertiary prevention of low back pain in the workplace: A systematic review. J. Occup. Rehabil. 2009, 19, 8–24. [Google Scholar] [CrossRef] [Green Version]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, D.G. Epidemiology, etiology, diagnostic evaluation, and treatment of low back pain. Curr. Opin. Rheumatol. 2001, 13, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Qaseem, A.; Snow, V. Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann. Intern. Med. 2007, 147, 478–491. [Google Scholar] [CrossRef]
- Kendall, K.D.; Schmidt, C.; Ferber, R. The relationship between hip-abductor strength and the magnitude of pelvic drop in patients with low back pain. J. Sport Rehabil. 2010, 19, 422–435. [Google Scholar] [CrossRef]
- Sadeghisani, M.; Manshadi, F.D.; Kalantari, K.K.; Rahimi, A.; Namnik, N.; Karimi, M.T.; Oskouei, A.E. Correlation between Hip Rotation Range-of-Motion Impairment and Low Back Pain. A Literature Review. Ortop. Traumatol. Rehabil. 2015, 17, 455–462. [Google Scholar] [CrossRef]
- Cooper, N.A.; Scavo, K.M.; Strickland, K.J.; Tipayamongkol, N.; Nicholson, J.D.; Bewyer, D.C.; Sluka, K.A. Prevalence of gluteus medius weakness in people with chronic low back pain compared to healthy controls. Eur. Spine J. 2016, 25, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Reiman, M.P.; Bolgla, L.A.; Loudon, J.K. A literature review of studies evaluating gluteus maximus and gluteus medius activation during rehabilitation exercises. Physiother. Theory Pract. 2012, 28, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Gilmore, C.A.; Kapural, L.; McGee, M.J.; Boggs, J.W. Percutaneous Peripheral Nerve Stimulation (PNS) for the Treatment of Chronic Low Back Pain Provides Sustained Relief. Neuromodulation 2019, 22, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Gilmore, C.; Kapural, L.; Hanling, S.; Plunkett, A.; McGee, M.; Boggs, J. Percutaneous Peripheral Nerve Stimulation for Pain Reduction and Improvements in Functional Outcomes in Chronic Low Back Pain. Mil. Med. 2009, 184 (Suppl. S1), 537–541. [Google Scholar] [CrossRef] [PubMed]
- Valera-Garrido, F.; Minaya-Muñoz, F. Fisioterapia Invasiva; Elsevier España SL: Barcelona, Spain, 2016. [Google Scholar]
- De-la-Cruz-Torres, B.; Abuín-Porras, V.; Navarro-Flores, E.; Calvo-Lobo, C.; Romero-Morales, C. Ultrasound-Guided Percutaneous Neuromodulation in Patients with Chronic Lateral Epicondylalgia: A Pilot Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 4877. [Google Scholar] [CrossRef] [PubMed]
- García-Bermejo, P.; De-la-Cruz-Torres, B.; Romer-Morales, C. Ultrasound-guided percutaneous neuromodulation in patients with unilateral anterior knee pain: A randomised clinical trial. Appl. Sci. 2020, 10, 4647. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Arias-Buría, J.L.; El Bachiri, Y.R.; Plaza-Manzano, G.; Cleland, J.A. Ultrasound-guided percutaneous electrical stimulation for a patient with cubital tunnel syndrome: A case report with a one-year follow-up. Physiother. Theory Pract. 2020, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- San-Emeterio-Iglesias, R.; Minaya-Muñoz, F.; Romero-Morales, C.; De-la-Cruz-Torres, B. Correct Sciatic Nerve Management to Apply Ultrasound-Guided Percutaneous Neuromodulation in Patients with Chronic Low Back Pain: A Pilot Study. Neuromodulation 2021, 24, 1067–1074. [Google Scholar] [CrossRef]
- De-la-Cruz-Torres, B.; Barrera-García-Martín, I.; Albornoz-Cabello, M. Immediate effects of ultrasound-guided percutaneous neuromodulation versus physical exercise on performance of the flexor hallucis longus muscle in professional dancers: A randomised clinical trial. Acupunct. Med. 2019, 37, 91–97. [Google Scholar] [CrossRef]
- De-la-Cruz-Torres, B.; Barrera-García-Martín, I.; Romero-Morales, C. Comparative Effects of One-Shot Electrical Stimulation on Performance of the Flexor Hallucis Longus Muscle in Professional Dancers: Percutaneous Versus Transcutaneous? Neuromodulation 2020, 23, 865–870. [Google Scholar] [CrossRef]
- De-la-Cruz-Torres, B.; Carrasco-Iglesias, C.; Minaya-Muñoz, F.; Romero-Morales, C. Crossover effects of ultrasound-guided percutaneous neuromodulation on contralateral hamstring flexibility. Acupunct. Med. 2020, 39, 512–521. [Google Scholar] [CrossRef]
- Álvarez-Plats, D.; Carvajal-Fernández, O.; Pérez-Mellada, N.; Minaya-Muñoz, F. Changes in Maximal Isometric Quadriceps Strength after the Application of Ultrasound-Guided Percutaneous Neuromodulation of the Femoral Nerve: A Case Series. Rev. Fisioter Invasiva 2019, 2, 39–45. [Google Scholar]
- Gallego-Sendarrubias, G.M.; Arias-Buría, J.L.; Úbeda-D’Ocasar, E.; Hervás-Pérez, J.P.; Rubio-Palomino, M.A.; Fernández-de-Las-Peñas, C.; Valera-Calero, J.A. Effects of Percutaneous Electrical Nerve Stimulation on Countermovement Jump and Squat Performance Speed in Male Soccer Players: A Pilot Randomized Clinical Trial. J. Clin. Med. 2021, 10, 690. [Google Scholar] [CrossRef]
- Plaza-Manzano, G.; Gómez-Chiguano, G.F.; Cleland, J.A.; Arías-Buría, J.L.; Fernández-de-Las-Peñas, C.; Navarro-Santana, M.J. Effectiveness of percutaneous electrical nerve stimulation for musculoskeletal pain: A systematic review and meta-analysis. Eur. J. Pain 2020, 24, 1023–1044. [Google Scholar] [CrossRef]
- Deyo, R.; Dworkin, S.F.; Amtmann, D.; Andersson, G.; Borenstein, D.; Carragee, E.; Carrino, J.; Chou, R.; Cook, K.; DeLitto, A.; et al. Report of the NIH Task Force on research standards for chronic low back pain. Spine J. 2014, 14, 1375–1391. [Google Scholar] [CrossRef] [PubMed]
- Carmona, L.; Ballina, J.; Gabriel, R.; Laffon, A. The burden of musculoskeletal diseases in the general population of Spain: Results from a national survey. Ann. Rheum. Dis. 2001, 60, 1040–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grande-Alonso, M.; Suso-Martí, L.; Cuenca-Martínez, F.; Pardo-Montero, J.; Gil-Martínez, A.; La Touche, R. Physiotherapy Based on a Biobehavioral Approach with or without Orthopedic Manual Physical Therapy in the Treatment of Nonspecific Chronic Low Back Pain: A Randomized Controlled Trial. Pain Med. 2019, 20, 2571–2587. [Google Scholar] [CrossRef] [PubMed]
- Avman, M.A.; Osmotherly, P.G.; Snodgrass, S.; Rivett, D.A. Is there an association between hip range of motion and nonspecific low back pain? A systematic review. Musculoskelet. Sci. Pract. 2019, 42, 38–51. [Google Scholar] [CrossRef]
- Grande-Alonso, M.; Muñoz-García, D.; Cuenca-Martínez, F.; Delgado-Sanz, L.; Prieto-Aldana, M.; La Touche, R.; Gil-Martínez, A. Relationship between healthcare seeking and pain expansion in patients with nonspecific chronic low back pain. Peer J. 2020, 8, e8756. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry disability index. Spine 2000, 25, 2940–2952. [Google Scholar] [CrossRef]
- Lea, R.D.; Gerhardt, J.J. Range-of-motion measurements. J. Bone Joint Surg. Am. 1995, 77, 784–798. [Google Scholar] [CrossRef]
- Thorborg, K.; Petersen, J.; Magnusson, S.P.; Hölmich, P. Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand. J. Med. Sci. Sports 2010, 20, 493–501. [Google Scholar] [CrossRef]
- Pua, Y.H.; Wrigley, T.W.; Cowan, S.M.; Bennell, K.L. Intrarater test–retest reliability of hip range of motion and hip muscle strength measurements in persons with hip osteoarthritis. Arch Phys. Med. Rehabil. 2008, 89, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Sisto, S.A.; Dyson-Hudson, T. Dynamometry testing in spinal cord injury. J. Rehabil. Res. Dev. 2007, 44, 123–136. [Google Scholar] [CrossRef]
- Maughan, E.F.; Lewis, J.S. Outcome measures in chronic low back pain. Eur. Spine J. 2010, 19, 1484–1494. [Google Scholar] [CrossRef] [PubMed]
- Nourbakhsh, M.; Arab, A. Relationship between mechanical factors and incidence of low back pain. J. Orthop. Sports Phys. Ther. 2002, 32, 447–460. [Google Scholar] [CrossRef]
- Nelson-Wong, E.; Poupore, K.; Ingvalson, S.; Dehmer, K.; Piatte, A.; Alexander, S.; Gallant, P.; McClenahan, B.; Davis, A.M. Neuromuscular strategies for lumbopelvic control during frontal and sagittal plane movement challenges differ between people with and without low back pain. J. Electr. Kinesiol. 2013, 23, 1317–1324. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Malmivaara, A.; van Tulder, M.W. Exercise therapy for chronic low back pain. Cochrane Database Syst. Rev. 2021, 9, CD009790. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Data | Total (n = 60) | Group A (n = 20) | Group B (n = 20) | Group C (n = 20) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 41.98 (12.9) | 42.40 (12.1) | 43.9 (15.3) | 39.65 (11.3) | 0.583 |
| Weight (kilograms) | 71.31 (12.2) | 73.3 (13.2) | 70.15 (13.1) | 70.5 (10.4) | 0.678 |
| Height (meters) | 1.71 (0.07) | 1.71 (0.09) | 1.69 (0.07) | 1.71 (0.06) | 0.728 |
| BMI (kg/m2) | 24.23 (3.26) | 24.56 (3.23) | 24.22 (3.84) | 23.9 (2.76) | 0.823 |
| Gender (F/M) | 30/30 | 10/10 | 10/10 | 10/10 | N/A |
| Dominant side (R/L) | 47/13 | 17/3 | 15/5 | 15/5 | N/A |
| Intervention side (R/L) | 26/34 | 9/11 | 7/13 | 10/10 | N/A |
| Intrasubject Treatment Effects | |||||
|---|---|---|---|---|---|
| Measure | Group A | Group B | Group C | Time Value F (Df); p (Eta2) | Treatment × Time F (Df); p (Eta2) |
| Pain (NRS) | F (1, 57) = 237.12; p = 0.001 (0.81) | F (1, 57) = 1.29; p = 0.28 (0.05) | |||
| Baseline | 4.85 ± 1.3 | 5.50 ± 0.9 | 5.30 ± 1.3 | ||
| 1 week | 1.90 ± 1.2 | 2.20 ± 1.3 | 2.75 ± 1.7 | ||
| ODI (%) | F (1, 57) = 151.47; p = 0.001(0.73) | F (1, 57) = 4.13; p = 0.02 (0.13) | |||
| Baseline | 16.3 ± 5.2 | 19.3 ± 9.9 | 17.4 ± 7.7 | ||
| 1 week | 8.1 ± 4.8 | 6.7 ± 5.7 | 9.8 ± 7.4 | ||
| IR prone Non-Intervention limb (°) | F (1,57) = 12.45; p = 0.001(0.18) | F (1,57) = 1.18; p = 0.31 (0.04) | |||
| Baseline | 36.7 ± 5.4 | 40.1 ± 7.3 | 40.9 ± 5.2 | ||
| 1-week | 38.1 ± 5.2 | 40.7 ± 6.2 | 41.5 ± 5.1 | ||
| IR prone Intervention limb (°) | F (1,57) = 252.20; p = 0.001(0.82) | F (1,57) = 1.18; p = 0.31 (0.04) | |||
| Baseline | 29.6 ± 5.4 | 31.3 ± 6.5 | 33.4 ± 5.5 | ||
| 1-week | 38.3 ± 5.5 | 39.2 ± 5.4 | 40.2 ± 4.8 | ||
| Intrasubject Effects | |||||
|---|---|---|---|---|---|
| Measure (Kgf) | Group A | Group B | Group C | Time Value F (Df); p (Eta2) | Treatment × Time F (Df); p (Eta2) |
| Flexion Non-Intervention limb | F (1,57) = 111.95; p = 0.001 (0.66) | F (1,57) = 3.77; p = 0.03 (0.12) | |||
| Baseline | 15.2 ± 3.0 | 13.0 ± 3.7 | 14.0 ± 2.8 | ||
| 1-week | 17.7 ± 3.7 | 15.6 ± 3.2 | 15.4 ± 2.3 | ||
| Flexion Intervention limb | F (1,57) = 129.48; p = 0.001 (0.70) | F (1,57) = 0.25; p = 0.78 (0.01) | |||
| Baseline | 14.3 ± 3.3 | 12.1 ± 3.8 | 12.8 ± 3.1 | ||
| 1-week | 17.8 ± 5.1 | 15.5 ± 3.3 | 15.8 ± 3.7 | ||
| ER sitting Non-Intervention limb | F (1,57) = 83.99; p = 0.001 (0.60) | F (1,57) = 0.50; p = 0.61 (0.02) | |||
| Baseline | 11.8 ± 3.1 | 9.8 ± 2.7 | 10.9 ± 2.7 | ||
| 1-week | 13.8 ± 3.6 | 11.6 ± 2.5 | 12.4 ± 2.8 | ||
| ER sitting Intervention limb | F (1,57) = 101.48; p = 0.001 (0.64) | F (1,57) = 0.51; p = 0.601(0.018) | |||
| Baseline | 10.8 ± 2.7 | 9.5 ± 2.7 | 10.1 ± 2.6 | ||
| 1-week | 13.7 ± 3.6 | 12.0 ± 2.8 | 12.4 ± 2.6 | ||
| IR sitting Non-Intervention limb | F (1,57) = 57.39; p = 0.001 (0.50) | F (1,57) = 0.57; p = 0.57 (0.02) | |||
| Baseline | 12.3 ± 2.2 | 10.7 ± 2.5 | 11.0 ± 2.5 | ||
| 1-week | 14.9 ± 3.9 | 13.3 ± 3.3 | 12.9 ± 2.7 | ||
| IR sitting Intervention limb | F (1,57) = 71.49; p = 0.001 (0.56) | F (1,57) = 0.84; p = 0.43 (0.03) | |||
| Baseline | 11.5 ± 2.1 | 9.4 ± 2.0 | 10.4 ± 2.7 | ||
| 1-week | 14.7 ± 3.1 | 13.0 ± 3.5 | 12.8 ± 3.4 | ||
| ER prone Non-Intervention limb | F (1,57) = 24.64; p = 0.001 (0.30) | F (1,57) = 0.53; p = 0.59 (0.02) | |||
| Baseline | 12.2 ± 2.9 | 10.4 ± 2.2 | 11.5 ± 3.3 | ||
| 1-week | 13.4 ± 3.5 | 11.7 ± 2.1 | 12.3 ± 2.6 | ||
| ER prone Intervention limb | F (1,57) = 89.63; p = 0.001 (0.61) | F (1,57) = 0.13; p = 0.88 (0.004) | |||
| Baseline | 11.5 ± 2.2 | 10.1 ± 2.6 | 10.3 ± 2.4 | ||
| 1-week | 13.6 ± 3.3 | 12.4 ± 2.5 | 12.4 ± 2.8 | ||
| IR prone Non-Intervention limb | F (1,57) = 53.84; p = 0.001 (0.49) | F (1,57) = 0.85; p = 0.43 (0.03) | |||
| Baseline | 10.5 ± 2.4 | 9.7 ± 2.7 | 9.5 ± 2.2 | ||
| 1-week | 12.7 ± 3.2 | 11.1 ± 2.4 | 11.2 ± 2.3 | ||
| IR prone Intervention limb | F (1,57) = 166.47; p = 0.001 (0.75) | F (1,57) = 2.06; p = 0.14 (0.07) | |||
| Baseline | 9.1 ± 2.3 | 8.5 ± 2.4 | 8.8 ± 2.3 | ||
| 1-week | 12.8 ± 3.7 | 11.5 ± 2.6 | 11.4 ± 2.4 | ||
| Abduction Non-Intervention limb | F (1,57) = 71.03; p = 0.001 (0.55) | F (1,57) = 1.36; p = 0.27 (0.04) | |||
| Baseline | 12.5 ± 2.1 | 11.5 ± 3.0 | 12.1 ± 2.3 | ||
| 1-week | 14.8 ± 3.5 | 13.8 ± 2.6 | 13.6 ± 2.6 | ||
| Abduction Intervention limb | F (1,57) = 111.79; p = 0.001 (0.66) | F (1,57) = 1.07; p = 0.35 (0.04) | |||
| Baseline | 11.3 ± 1.9 | 10.6 ± 2.9 | 10.7 ± 2.3 | ||
| 1-week | 15.3 ± 3.6 | 14.2 ± 2.9 | 13.6 ± 3.0 | ||
| Extension Non-Intervention limb | F (1,57) = 61.86; p = 0.001 (0.52) | F (1,57) = 2.29; p = 0.11 (0.07) | |||
| Baseline | 19.4 ± 4.3 | 16.1 ± 3.5 | 17.5 ± 4.3 | ||
| 1-week | 24.9 ± 9.5 | 19.9 ± 4.0 | 20.3 ± 4.6 | ||
| Extension Intervention limb | F (1,57) = 109.80; p = 0.001 (0.66) | F (1,57) = 1.11; p = 0.34 (0.0) | |||
| Baseline | 17.4 ± 4.6 | 15.0 ± 3.2 | 15.9 ± 4.2 | ||
| 1-week | 24.6 ± 9.5 | 20.9 ± 4.3 | 21.0 ± 4.5 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
San-Emeterio-Iglesias, R.; De-la-Cruz-Torres, B.; Romero-Morales, C.; Minaya-Muñoz, F. Effect of Ultrasound-Guided Percutaneous Neuromodulation of Sciatic Nerve on Hip Muscle Strength in Chronic Low Back Pain Sufferers: A Pilot Study. J. Clin. Med. 2022, 11, 6672. https://doi.org/10.3390/jcm11226672
San-Emeterio-Iglesias R, De-la-Cruz-Torres B, Romero-Morales C, Minaya-Muñoz F. Effect of Ultrasound-Guided Percutaneous Neuromodulation of Sciatic Nerve on Hip Muscle Strength in Chronic Low Back Pain Sufferers: A Pilot Study. Journal of Clinical Medicine. 2022; 11(22):6672. https://doi.org/10.3390/jcm11226672
Chicago/Turabian StyleSan-Emeterio-Iglesias, Roberto, Blanca De-la-Cruz-Torres, Carlos Romero-Morales, and Francisco Minaya-Muñoz. 2022. "Effect of Ultrasound-Guided Percutaneous Neuromodulation of Sciatic Nerve on Hip Muscle Strength in Chronic Low Back Pain Sufferers: A Pilot Study" Journal of Clinical Medicine 11, no. 22: 6672. https://doi.org/10.3390/jcm11226672