
Physical Activity and the Risk of COVID-19 Infection and Mortality: A Nationwide Population-Based Case-Control Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
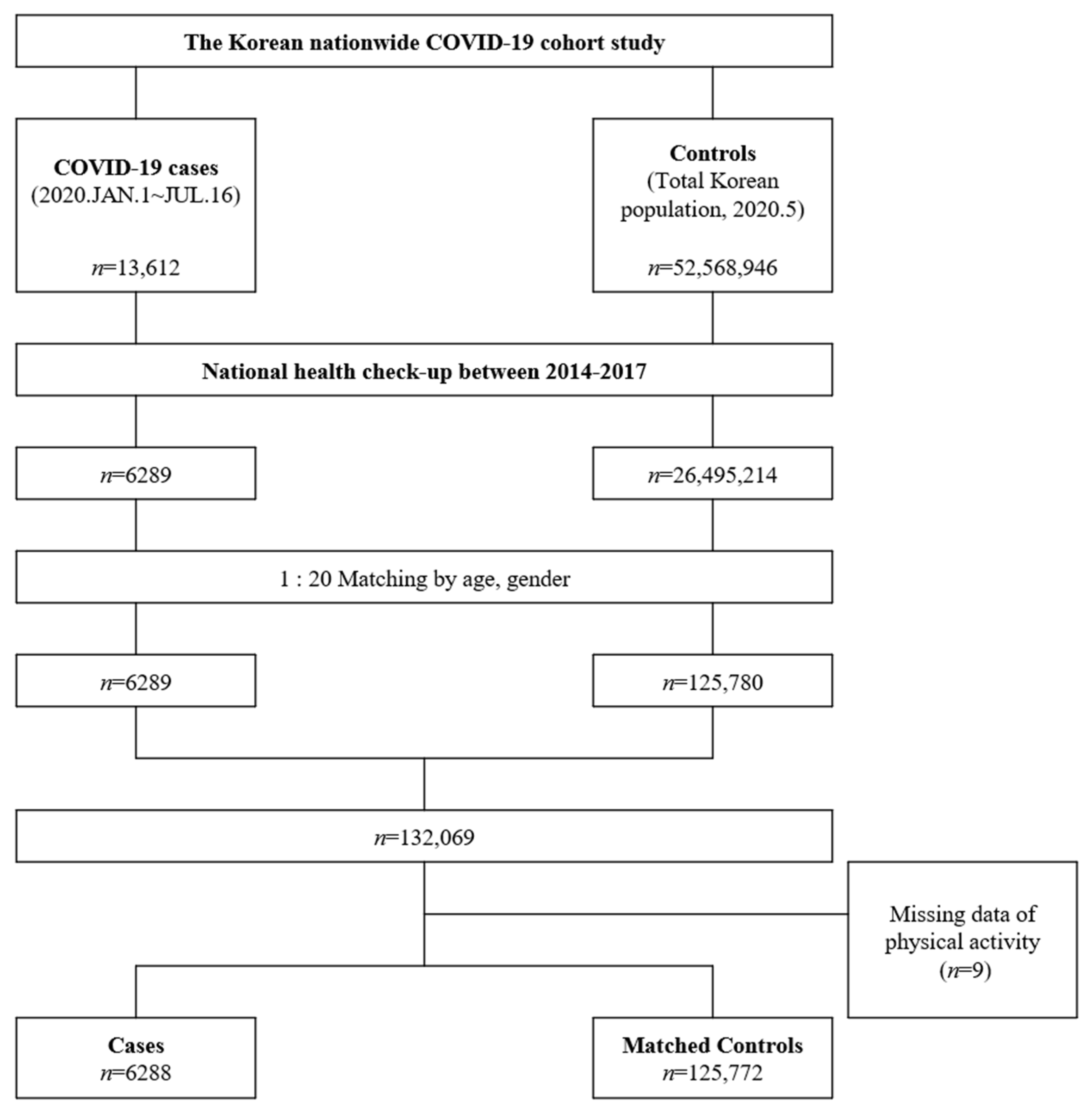
2.1. Data Sources and Target Population
2.2. Case Patients and Controls
2.3. Physical Activity and Other Variables
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
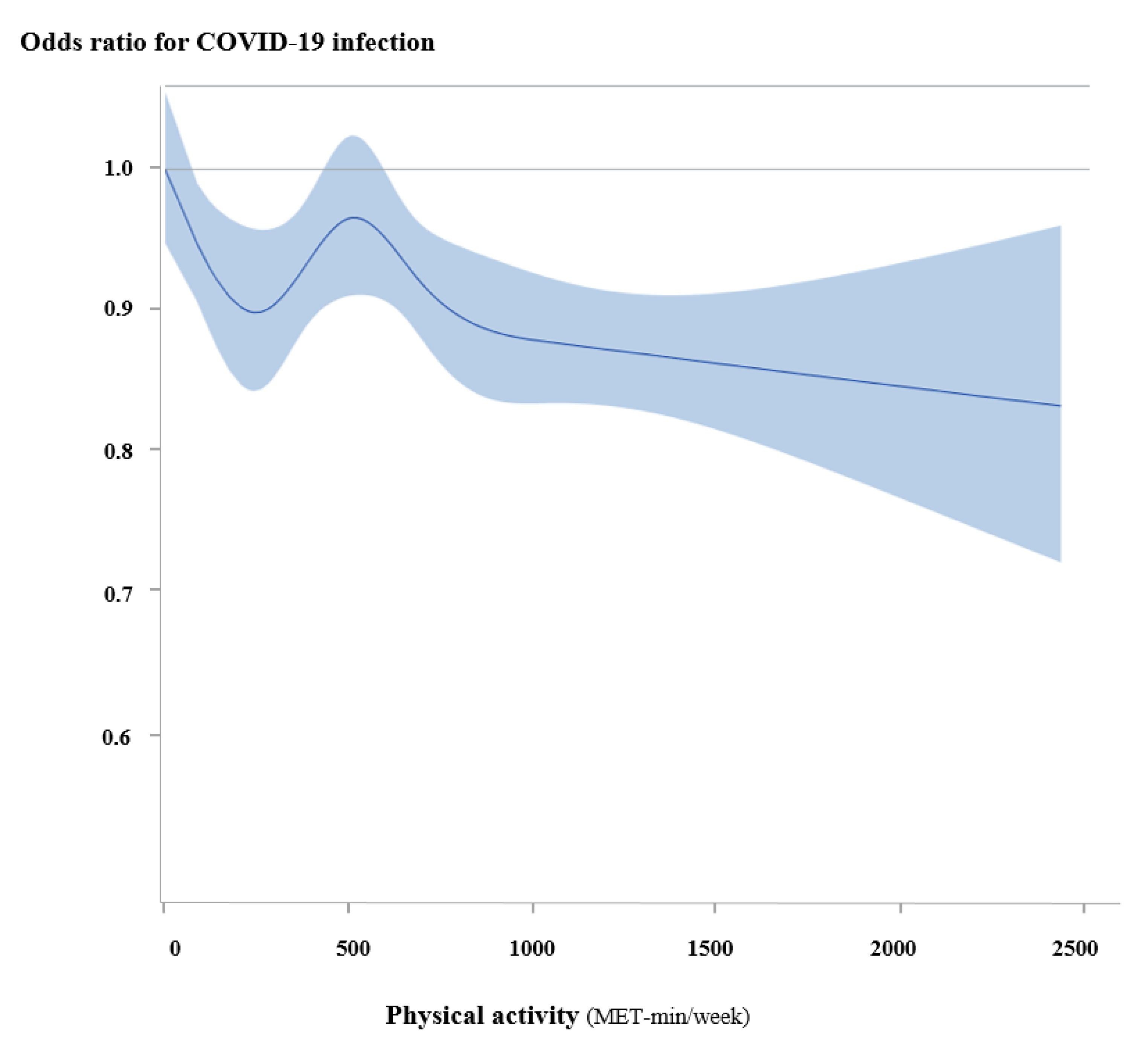
3.2. Physical Activity and the Risk of COVID-19
3.3. Physical Activity and the Risk of Mortality
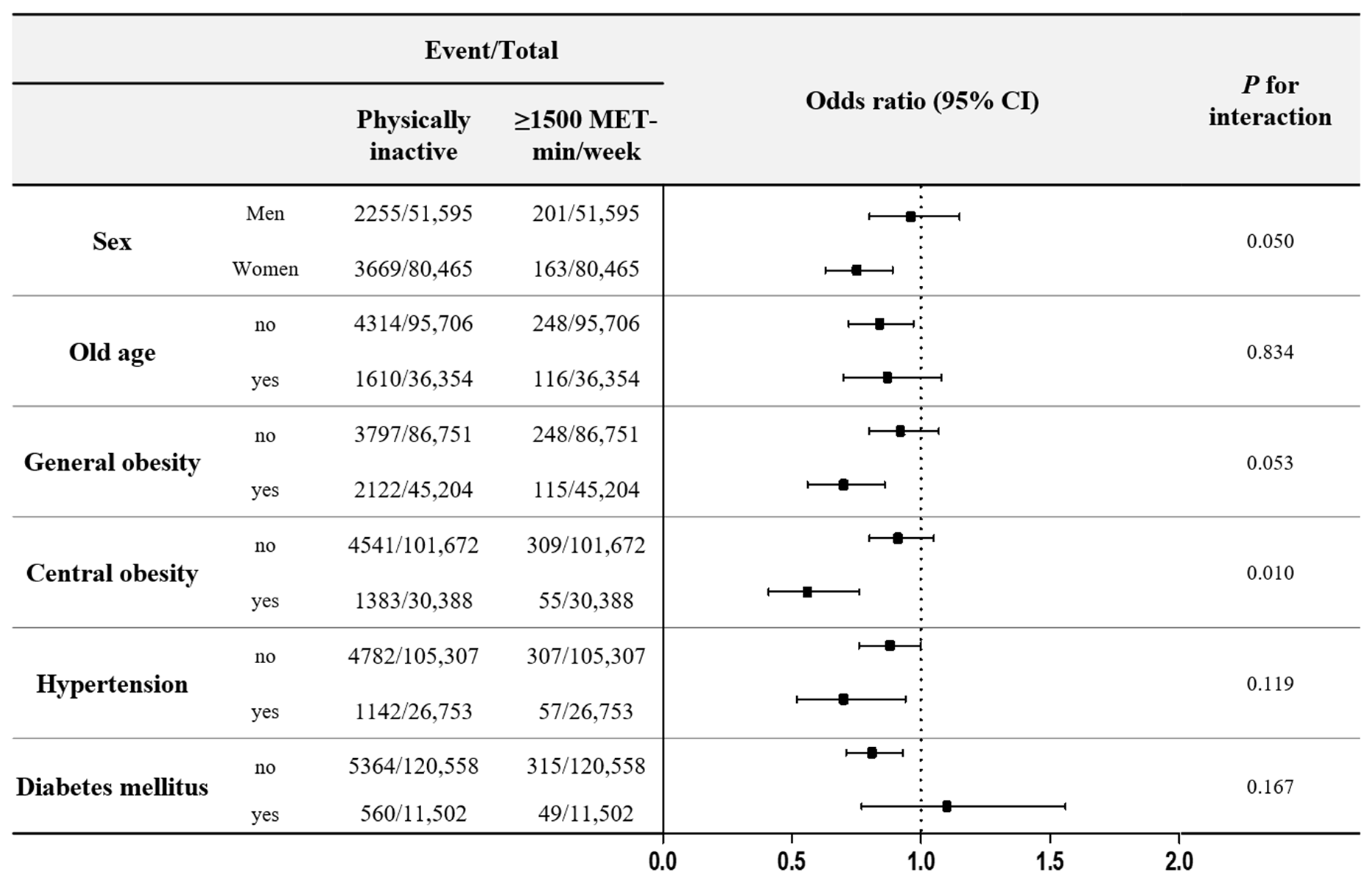
3.4. Subgroup Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phelan, A.L.; Katz, R.; Gostin, L.O. The novel coronavirus originating in wuhan, china: Challenges for global health governance. JAMA 2020, 323, 709–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cucinotta, D.; Vanelli, M. Who declares covid-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Pavon, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of covid-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with obesity and covid-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. 2020, 21, e13128. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide effect of covid-19 on physical activity: A descriptive study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Group, L.P.A.S.W. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Nieman, D.C.; Henson, D.A.; Austin, M.D.; Sha, W. Upper respiratory tract infection is reduced in physically fit and active adults. Br. J. Sports Med. 2011, 45, 987–992. [Google Scholar] [CrossRef]
- Wong, C.M.; Lai, H.K.; Ou, C.Q.; Ho, S.Y.; Chan, K.P.; Thach, T.Q.; Yang, L.; Chau, Y.K.; Lam, T.H.; Hedley, A.J.; et al. Is exercise protective against influenza-associated mortality? PLoS ONE 2008, 3, e2108. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Kivimaki, M.; Gale, C.R.; Batty, G.D. Lifestyle risk factors, inflammatory mechanisms, and covid-19 hospitalization: A community-based cohort study of 387,109 adults in UK. Brain Behav. Immun. 2020, 87, 184–187. [Google Scholar] [CrossRef]
- Brawner, C.A.; Ehrman, J.K.; Bole, S.; Kerrigan, D.J.; Parikh, S.S.; Lewis, B.K.; Gindi, R.M.; Keteyian, C.; Abdul-Nour, K.; Keteyian, S.J. Maximal exercise capacity is inversely related to hospitalization secondary to coronavirus disease 2019. Mayo Clin. Proc. 2020, 96, 32–39. [Google Scholar] [CrossRef]
- Boukelia, B.; Alataibi, A.S. The effect of bmi and physical activity levels on the duration of symptomatic days with covid-19 infection. medRxiv 2020. [Google Scholar] [CrossRef]
- Cho, D.H.; Yoo, B.S.; Son, J.W.; Kim, I.C.; Park, S.M.; Choi, D.J. Covid-19—implications for patients with heart failure: The korean society of heart failure’s clinical recommendations. Int. J. Heart Fail. 2020, 2, 111–114. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.W.; Ha, E.K.; Yeniova, A.O.; Moon, S.Y.; Kim, S.Y.; Koh, H.Y.; Yang, J.M.; Jeong, S.J.; Moon, S.J.; Cho, J.Y.; et al. Severe clinical outcomes of covid-19 associated with proton pump inhibitors: A nationwide cohort study with propensity score matching. Gut 2021, 70, 76–84. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Adhikari, S.; Pulgarin, C.; Troxel, A.B.; Iturrate, E.; Johnson, S.B.; Hausvater, A.; Newman, J.D.; Berger, J.S.; Bangalore, S.; et al. Renin-angiotensin-aldosterone system inhibitors and risk of covid-19. N. Engl. J. Med. 2020, 382, 2441–2448. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The national health insurance service-national health screening cohort (nhis-heals) in korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, S.; Lee, H.J.; Han, K.D.; Kim, D.H.; Lee, S.P.; Hwang, I.C.; Yoon, Y.; Park, J.B.; Lee, H.; Kwak, S. Association of physical activity with all-cause and cardiovascular mortality in 7666 adults with hypertrophic cardiomyopathy (hcm): More physical activity is better. Br. J. Sports Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.W.; Kim, S.H.; Kang, S.H.; Kim, H.J.; Yoon, C.H.; Youn, T.J.; Chae, I.H. Mortality reduction with physical activity in patients with and without cardiovascular disease. Eur. Heart J. 2019, 40, 3547–3555. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.; Abaraogu, U.; Bourgois, J.; Dall, P.; Darnborough, J.; Duncan, E.; Dumortier, J.; Jiménez Pavón, D.; McParland, J.; Roberts, N. Physical activity, immune function and risk of community acquired infectious disease in the general population: Systematic review and meta-analysis. SSRN 2020. [Google Scholar] [CrossRef]
- Baik, I.; Curhan, G.C.; Rimm, E.B.; Bendich, A.; Willett, W.C.; Fawzi, W.W. A prospective study of age and lifestyle factors in relation to community-acquired pneumonia in us men and women. Arch. Intern. Med. 2000, 160, 3082–3088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuman, M.I.; Willett, W.C.; Curhan, G.C. Physical activity and the risk of community-acquired pneumonia in us women. Am. J. Med. 2010, 123, 281.e7–281.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, Y.; Koizumi, A.; Wada, Y.; Iso, H.; Watanabe, Y.; Date, C.; Yamamoto, A.; Kikuchi, S.; Inaba, Y.; Toyoshima, H. Risk and protective factors related to mortality from pneumonia among middleaged and elderly community residents: The jacc study. J. Epidemiol. 2007, 17, 194–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grande, A.J.; Keogh, J.; Silva, V.; Scott, A.M. Exercise versus no exercise for the occurrence, severity, and duration of acute respiratory infections. Cochrane Database Syst. Rev. 2020, 4, CD010596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, J.P.; Turner, J.E. Debunking the myth of exercise-induced immune suppression: Redefining the impact of exercise on immunological health across the lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef]
- Nieman, D.C. Is infection risk linked to exercise workload? Med. Sci. Sports Exerc. 2000, 32 (Suppl. S7), S406–S411. [Google Scholar] [CrossRef]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- Nieman, D.C.; Johanssen, L.M.; Lee, J.W.; Arabatzis, K. Infectious episodes in runners before and after the los angeles marathon. J. Sports Med. Phys. Fit. 1990, 30, 316–328. [Google Scholar]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corra, U.; Cosyns, B.; Deaton, C. 2016 european guidelines on cardiovascular disease prevention in clinical practice: The sixth joint task force of the european society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the european association for cardiovascular prevention & rehabilitation (eacpr). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Murphy, E.A.; Davis, J.M.; Brown, A.S.; Carmichael, M.D.; Van Rooijen, N.; Ghaffar, A.; Mayer, E.P. Role of lung macrophages on susceptibility to respiratory infection following short-term moderate exercise training. Am. J. Physiol. Regul Integr. Comp. Physiol. 2004, 287, R1354–R1358. [Google Scholar] [CrossRef]
- McFarlin, B.K.; Flynn, M.G.; Phillips, M.D.; Stewart, L.K.; Timmerman, K.L. Chronic resistance exercise training improves natural killer cell activity in older women. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1315–1318. [Google Scholar] [CrossRef] [Green Version]
- Kohut, M.L.; Senchina, D.S. Reversing age-associated immunosenescence via exercise. Exerc. Immunol. Rev. 2004, 10, 41. [Google Scholar]
- Tracey, K.J. Reflex control of immunity. Nat. Rev. Immunol. 2009, 9, 418–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| COVID-19 (n = 6288) | Controls (n = 125,772) | p Value | |
|---|---|---|---|
| Age, years | 50.7 ± 14.3 | 50.7 ± 14.3 | 0.968 |
| Women, n (%) | 3832 (60.9%) | 76,633 (60.9%) | 0.996 |
| BMI, kg/m2 | 24.1 ± 3.4 | 23.9 ± 3.5 | 0.003 |
| General obesity, n (%) | 2237 (35.6%) | 42,967 (34.2%) | 0.021 |
| WC, cm | 80.5 ± 9.6 | 80.3 ± 14.0 | 0.079 |
| SBP, mmHg | 121.1 ± 15.1 | 122.0 ± 14.9 | <0.001 |
| DBP, mmHg | 75.0 ± 10.1 | 75.6 ± 10.0 | <0.001 |
| Medical history, n (%) | |||
| Hypertension | 1199 (19.1%) | 25,554 (20.3%) | 0.017 |
| Diabetes mellitus | 609 (9.7%) | 10,893 (8.7%) | 0.005 |
| Dyslipidaemia | 571 (9.1%) | 10,855 (8.6%) | 0.224 |
| Ischaemic heart disease | 20 (0.3%) | 331 (0.3%) | 0.484 |
| Stroke | 103 (1.6%) | 1692 (1.4%) | 0.057 |
| Current smoking | 566 (9.0%) | 21,507 (17.1%) | <0.001 |
| Alcohol consumption | 2511 (39.9%) | 62,392 (49.6%) | <0.001 |
| Physical activity, by intensity | |||
| Physically inactive, n (%) | 1313 (20.9%) | 23,978 (19.1%) | <0.001 |
| Light intensity, n (%) | 1752 (27.9%) | 33,185 (26.4%) | |
| Moderate intensity, n (%) | 861 (13.7%) | 17,557 (14.0%) | |
| Vigorous intensity, n (%) | 2362 (37.6%) | 51,052 (40.6%) | |
| Moderate to vigorous intensity, n (%) | 3223 (51.3%) | 68,609 (54.6%) | <0.001 |
| Physical activity, by level of MET-min/week | |||
| MET-min/week | 558.2 ± 516.3 | 580.2 ± 525.7 | 0.001 |
| <500 MET-min/week | 1889 (30.0%) | 38,540 (30.6%) | 0.001 |
| 500–1000 MET-min/week | 1973 (31.4%) | 38,970 (31.0%) | |
| 1000–1500 MET-min/week | 752 (12.0%) | 16,340 (13.0%) | |
| ≥1500 MET-min/week | 364 (5.8%) | 7944 (6.3%) |
| (A) | Case n (%) | Control n (%) | Multivariate OR (95% CI) | |
| Model 1 | Model 2 | |||
| By intensity | ||||
| Physically inactive | 1313 (20.9%) | 23,978 (19.1%) | 1 | 1 |
| Light | 1752 (27.9%) | 33,185 (26.4%) | 0.96 (0.93–1.04) | 0.98 (0.91–1.06) |
| Moderate | 861 (13.7%) | 17,557 (14.0%) | 0.89 (0.82–0.98) * | 0.93 (0.85–1.02) |
| Vigorous | 2362 (37.6%) | 51,052 (40.6%) | 0.84 (0.78–0.90) * | 0.88 (0.82–0.94) * |
| Moderate to vigorous | 3223 (51.3%) | 68,609 (54.6%) | 0.87 (0.83–0.92) * | 0.90 (0.86–0.95) * |
| By level of MET-min/week | ||||
| Physically inactive | 1313 (20.9%) | 23,978 (19.1%) | 1 | |
| <500 MET-min/week | 1889 (30.0%) | 38,540 (30.6%) | 0.89 (0.83–0.96) * | 0.93 (0.87–1.00) |
| 500–1000 MET-min/week | 1973 (31.4%) | 38,970 (31.0%) | 0.92 (0.86–0.99) * | 0.96 (0.89–1.03) |
| 1000–1500 MET-min/week | 752 (12.0%) | 16,340 (13.0%) | 0.84 (0.77–0.92) * | 0.86 (0.78–0.94) * |
| ≥1500 MET-min/week | 364 (5.8%) | 7944 (6.3%) | 0.84 (0.74–0.94) * | 0.85 (0.75–0.96) * |
| 1 SD of MET-min/week | 0.96 (0.93–0.98) * | 0.96 (0.93–0.99) * | ||
| (B) | Mortality n (%) | Survivor n (%) | Multivariate OR (95% CI) | |
| Model 1 | Model 2 | |||
| By intensity | ||||
| Physically inactive | 31 (33.7%) | 1313 (21.2%) | 1 | 1 |
| Light | 27 (29.3%) | 1752 (28.3%) | 0.67 (0.38–1.18) | 0.57 (0.31–1.04) |
| Moderate | 4 (4.3%) | 861 (13.9%) | 0.27 (0.09–0.81) * | 0.26 (0.08–0.81) * |
| Vigorous | 13 (14.1%) | 2362 (38.1%) | 0.40 (0.20–0.81) * | 0.38 (0.18–0.81) * |
| Moderate to vigorous | 17 (18.5%) | 3223 (52.0%) | 0.45 (0.25–0.80) * | 0.47 (0.26–0.87) * |
| By level of MET-min/week | ||||
| Physically inactive | 31 (33.7%) | 1313 (21.2%) | 1 | 1 |
| <500 MET-min/week | 19 (20.7%) | 1886 (30.4%) | 0.65 (0.35–1.21) | 0.54 (0.28–1.08) |
| 500–1000 MET-min/week | 16 (17.4%) | 1973 (31.8%) | 0.44 (0.23–0.85) * | 0.42 (0.21–0.83) * |
| 1000–1500 MET-min/week | 6 (6.5%) | 752 (12.1%) | 0.53 (0.21–1.35) | 0.56 (0.21–1.49) |
| ≥1500 MET-min/week | 3 (3.3%) | 364 (5.9%) | 0.30 (0.09–1.03) | 0.23 (0.06–0.85) * |
| 1 SD of MET-min/week | 0.66 (0.49–0.88) * | 0.65 (0.48–0.88) * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, D.-H.; Lee, S.J.; Jae, S.Y.; Kim, W.J.; Ha, S.J.; Gwon, J.G.; Choi, J.; Kim, D.W.; Kim, J.Y. Physical Activity and the Risk of COVID-19 Infection and Mortality: A Nationwide Population-Based Case-Control Study. J. Clin. Med. 2021, 10, 1539. https://doi.org/10.3390/jcm10071539
Cho D-H, Lee SJ, Jae SY, Kim WJ, Ha SJ, Gwon JG, Choi J, Kim DW, Kim JY. Physical Activity and the Risk of COVID-19 Infection and Mortality: A Nationwide Population-Based Case-Control Study. Journal of Clinical Medicine. 2021; 10(7):1539. https://doi.org/10.3390/jcm10071539
Chicago/Turabian StyleCho, Dong-Hyuk, Sun Ju Lee, Sae Young Jae, Woo Joo Kim, Seong Jun Ha, Jun Gyo Gwon, Jimi Choi, Dong Wook Kim, and Jang Young Kim. 2021. "Physical Activity and the Risk of COVID-19 Infection and Mortality: A Nationwide Population-Based Case-Control Study" Journal of Clinical Medicine 10, no. 7: 1539. https://doi.org/10.3390/jcm10071539