
Measures Derived from Panoramic Ultrasonography and Animal-Based Protein Intake Are Related to Muscular Performance in Middle-Aged Adults


 ,
, 
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Heath Screening and Anthropometric Measures
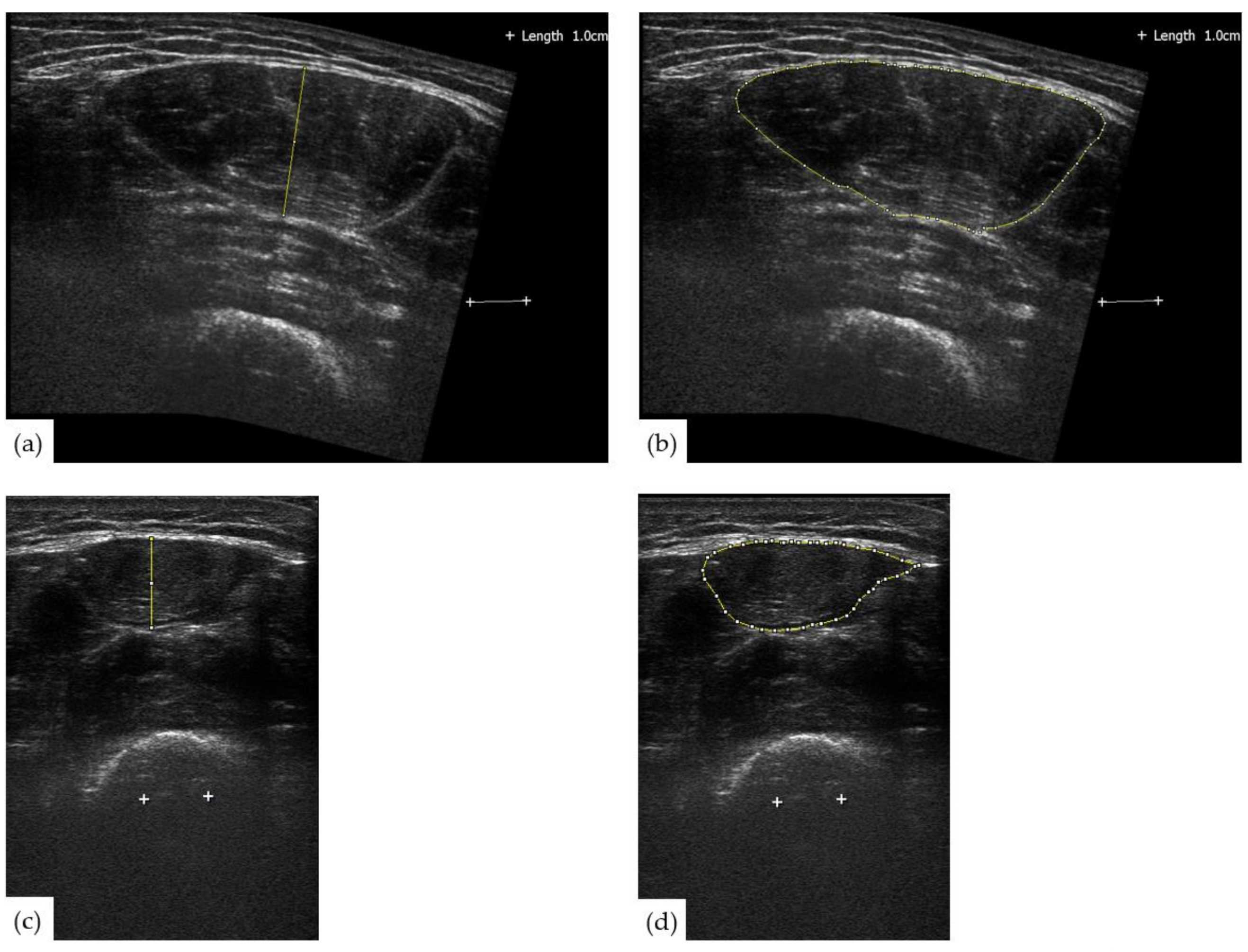
2.2. Ultrasonography
2.3. Performance Measures
2.4. Physical Activity Assessment
2.5. Nutrition Analysis
2.6. Statistical Analyses
2.6.1. Primary Analyses: Measures from Ultrasonography and Their Relationships with Muscular Performance and the Association between Rectus Femoris Echogenicity and Specific Force
2.6.2. Secondary Analyses: Animal-Based Protein Intake and Muscular Performance
2.6.3. Descriptive Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stokes, T.; Tripp, T.R.; Murphy, K.; Morton, R.W.; Oikawa, S.Y.; Lam Choi, H.; McGrath, J.; McGlory, C.; MacDonald, M.J.; Phillips, S.M. Methodological considerations for and validation of the ultrasonographic determination of human skeletal muscle hypertrophy and atrophy. Physiol. Rep. 2021, 9, 1–12. [Google Scholar] [CrossRef]
- Ponti, F.; de Cinque, A.; Fazio, N.; Napoli, A.; Guglielmi, G.; Bazzocchi, A. Ultrasound imaging, a stethoscope for body composition assessment. Quant. Imaging Med. Surg. 2020, 10, 1699–1722. [Google Scholar] [CrossRef] [PubMed]
- Stringer, H.J.; Wilson, D. The Role of Ultrasound as a Diagnostic Tool for Sarcopenia. J. Frailty Aging 2018, 7, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, Y.; Ikezoe, T.; Yamada, Y.; Tsukagoshi, R.; Nakamura, M.; Mori, N.; Kimura, M.; Ichihashi, N. Skeletal muscle quality assessed from echo intensity is associated with muscle strength of middle-aged and elderly persons. Eur. J. Appl. Physiol. 2012, 112, 1519–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshiko, A.; Kaji, T.; Sugiyama, H.; Koike, T.; Oshida, Y.; Akima, H. Muscle quality characteristics of muscles in the thigh, upper arm and lower back in elderly men and women. Eur. J. Appl. Physiol. 2018, 118, 1385–1395. [Google Scholar] [CrossRef] [PubMed]
- Ismail, C.; Zabal, J.; Hernandez, H.J.; Woletz, P.; Manning, H.; Teixeira, C.; DiPietro, L.; Blackman, M.R.; Harris-Love, M.O. Diagnostic ultrasound estimates of muscle mass and muscle quality discriminate between women with and without sarcopenia. Front. Physiol. 2015, 6, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salim, S.Y.; Al-Khathiri, O.; Tandon, P.; Baracos, V.E.; Churchill, T.A.; Warkentin, L.M.; Khadaroo, R.G. Thigh ultrasound used to identify frail elderly patients with sarcopenia undergoing surgery: A pilot study. J. Surg. Res. 2020, 256, 422–432. [Google Scholar] [CrossRef]
- Wilkinson, T.J.; Gore, E.F.; Vadaszy, N.; Nixon, D.G.D.; Watson, E.L.; Smith, A.C. Utility of ultrasound as a valid and accurate diagnostic tool for sarcopenia. J. Ultrasound Med. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Perkisas, S.; Baudry, S.; Bauer, J.; Beckwée, D.; De Cock, A.M.; Hobbelen, H.; Jager-Wittenaar, H.; Kasiukiewicz, A.; Landi, F.; Marco, E.; et al. Application of ultrasound for muscle assessment in sarcopenia: Towards standardized measurements. Eur. Geriatr. Med. 2018, 9, 739–757. [Google Scholar] [CrossRef]
- Scott, J.M.; Martin, D.S.; Ploutz-Snyder, R.; Matz, T.; Caine, T.; Downs, M.; Hackney, K.; Buxton, R.; Ryder, J.W.; Ploutz-Snyder, L. Panoramic ultrasound: A novel and valid tool for monitoring change in muscle mass. J. Cachexia. Sarcopenia Muscle 2017, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Barbat-Artigas, S.; Rolland, Y.; Vellas, B.; Aubertin-Leheudre, M. Muscle quantity is not synonymous with muscle quality. J. Am. Med. Dir. Assoc. 2013, 14, 852.e1–852.e7. [Google Scholar] [CrossRef] [PubMed]
- Strasser, E.M.; Draskovits, T.; Praschak, M.; Quittan, M.; Graf, A. Association between ultrasound measurements of muscle thickness, pennation angle, echogenicity and skeletal muscle strength in the elderly. Age (Omaha) 2013, 35, 2377–2388. [Google Scholar] [CrossRef] [Green Version]
- Abiri, B.; Vafa, M. Nutrition and sarcopenia: A review of the evidence of nutritional influences. Crit. Rev. Food Sci. Nutr. 2019, 59, 1456–1466. [Google Scholar] [CrossRef] [PubMed]
- Deer, R.R.; Volpi, E. Protein intake and muscle function in older adults. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 248–253. [Google Scholar] [CrossRef] [Green Version]
- Højfeldt, G.; Nishimura, Y.; Mertz, K.; Schacht, S.R.; Lindberg, J.; Jensen, M.; Hjulmand, M.; Lind, M.V.; Jensen, T.; Jespersen, A.P.; et al. Daily protein and energy intake are not associated with muscle mass and physical function in healthy older individuals—a cross-sectional study. Nutrients 2020, 12, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, J.-A.; Bendsen, N.T.; Tremblay, A.; Astrup, A. Effect of proteins from different sources on body composition. Nutr. Metab. Cardiovasc. Dis. 2011, 21 (Suppl. 2), B16–B31. [Google Scholar] [CrossRef]
- Berrazaga, I.; Micard, V.; Gueugneau, M.; Walrand, S. The role of the anabolic properties of plant-versus animal-based protein sources in supporting muscle mass maintenance: A critical review. Nutrients 2019, 11, 1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godin, G. International launch of the PAR-Q+ and ePARmed-X+ The Physical Activity Readiness Questionnaire for Everyone (PAR-Q+) and Electronic Physical Activity Readiness Medical Examination (ePARmed-X+). Health Fit. J. Canada 2011, 4, 18–22. [Google Scholar]
- Abe, T.; Kondo, M.; Kawakami, Y.; Fukunaga, T. Prediction equations for body composition of Japanese adults by B-mode ultrasound. Am. J. Hum. Biol. 1994, 6, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Reimers, C.D.; Harder, T.; Saxe, H. Age-related muscle atrophy does not affect all muscles and can partly be compensated by physical activity: An ultrasound study. J. Neurol. Sci. 1998, 159, 60–66. [Google Scholar] [CrossRef]
- Thoirs, K.; English, C. Ultrasound measures of muscle thickness: Intra-examiner reliability and influence of body position. Clin. Physiol. Funct. Imaging 2009, 29, 440–446. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- English, K.L.; Lee, S.M.C.; Loehr, J.A.; Ploutz–Snyder, R.J.; Ploutz–Snyder, L.L. Isokinetic strength changes following long-duration spaceflight on the ISS. Aerosp. Med. Hum. Perform. 2015, 86, 68–77. [Google Scholar] [CrossRef]
- Migueles, J.H.; Rowlands, A.V.; Huber, F.; Sabia, S.; van Hees, V.T. GGIR: A research community–driven open source R package for generating physical activity and sleep outcomes from multi-day raw accelerometer data. J. Meas. Phys. Behav. 2019, 2, 188–196. [Google Scholar] [CrossRef] [Green Version]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Chalé-Rush, A.; Guralnik, J.M.; Walkup, M.P.; Miller, M.E.; Rejeski, W.J.; Katula, J.A.; King, A.C.; Glynn, N.W.; Manini, T.M.; Blair, S.N.; et al. Relationship between physical functioning and physical activity in the lifestyle interventions and independence for elders pilot. J. Am. Geriatr. Soc. 2010, 58, 1918–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spartano, N.L.; Lyass, A.; Larson, M.G.; Tran, T.; Andersson, C.; Blease, S.J.; Esliger, D.W.; Vasan, R.S.; Murabito, J.M. Objective physical activity and physical performance in middle-aged and older adults. Exp. Gerontol. 2019, 119, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Aslam, M. Using heteroscedasticity-consistent standard errors for the linear regression model with correlated regressors. Commun. Stat. Simul. Comput. 2014, 43, 2353–2373. [Google Scholar] [CrossRef]
- Akima, H.; Yoshiko, A.; Tomita, A.; Ando, R.; Saito, A.; Ogawa, M.; Kondo, S.; Tanaka, N.I. Relationship between quadriceps echo intensity and functional and morphological characteristics in older men and women. Arch. Gerontol. Geriatr. 2017, 70, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Young, H.J.; Jenkins, N.T.; Zhao, Q.; Mccully, K.K. Measurement of intramuscular fat by muscle echo intensity. Muscle Nerve 2015, 52, 963–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pillen, S.; Tak, R.O.; Zwarts, M.J.; Lammens, M.M.Y.; Verrijp, K.N.; Arts, I.M.P.; van der Laak, J.A.; Hoogerbrugge, P.M.; van Engelen, B.G.M.; Verrips, A. Skeletal muscle ultrasound: Correlation between fibrous tissue and echo intensity. Ultrasound Med. Biol. 2009, 35, 443–446. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, F.; Zambon, S.; Giacometti, L.; Sergi, G.; Corti, M.C.; Manzato, E.; Busetto, L. Obesity, muscular strength, muscle composition and physical performance in an elderly population. J. Nutr. Health Aging 2015, 19, 785–791. [Google Scholar] [CrossRef]
- Hurt, R.T.; McClave, S.A.; Martindale, R.G.; Ochoa Gautier, J.B.; Coss-Bu, J.A.; Dickerson, R.N.; Heyland, D.K.; Hoffer, L.J.; Moore, F.A.; Morris, C.R.; et al. Summary points and consensus recommendations from the International Protein Summit. Nutr. Clin. Pract. 2017, 32, 142S–151S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paddon-Jones, D.; Short, K.R.; Campbell, W.W.; Volpi, E.; Wolfe, R.R. Role of dietary protein in the sarcopenia of aging. Am. J. Clin. Nutr. 2008, 87, 1562–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Wonsuk, Y.; Robert, M.; Sejong, B.; Karan, S.; He, Q.; James, W.L.J. A study of effects of multicollinearity in the multivariable analysis. Int. J. Appl. Sci. Technol. 2013, 6, 9–19. [Google Scholar]



{kind=link}
{kind=link}
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Total (n = 50) | Below Median ABPI (n = 25) | Above Median ABPI (n =25) | Total (n = 41) | Below Median ABPI (n = 21) | Above Median ABPI (n =20) | |
| Age (years) | 54.00 | 55.00 | 54.00 | 51.00 | 55.00 | 50.00 |
| Height (cm) | 165.20 | 164.00 | 165.50 | 181.00 | 176.70 | 181.05 |
| Weight (kg) | 68.30 | 67.33 | 69.12 | 87.7 | 85.20 | 92.36 |
| BMI | 25.11 | 24.43 | 25.54 | 26.57 | 26.57 | 26.32 |
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Total (n = 50) | Below Median ABPI (n = 25) | Above Median ABPI (n =25) | Total (n = 38) | Below Median ABPI (n = 21) | Above Median ABPI (n =17) | |
| Muscle Thickness at 50% (cm) | 2.109 | 2.038 | 2.178 | 2.339 | 2.275 | 2.345 |
| Muscle Thickness at 75% (cm) | 0.707 | 0.710 | 0.706 | 0.994 | 0.918 | 1.070 |
| Echogenicity at 50% (A.U.) | 96.70 | 97.86 | 96.64 | 35.90 | 34.85 | 41.73 |
| Echogenicity at 75% (A.U.) | 91.99 | 93.34 | 90.63 | 81.99 | 74.56 | 84.54 |
| Muscle CSA at 50% (cm2) | 7.384 | 6.569 | 7.861 | 10.593 | 10.470 | 10.963 |
| Muscle CSA at 75% (cm2) | 0.957 | 0.790 | 1.055 | 1.934 | 1.660 | 2.088 |
| Variable Entered | Dependent Variable | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Knee Extensor Peak Torque (Nm) | Summed Peak Torque (Nm) | Knee Extensor Total Work (J) | Summed Total Work (J) | 30-s Chair Stand Test (Repetitions) | Handgrip Strength (kg) | |||||||
| R | B ± S.E. | R | B ± S.E. | R | B ± S.E. | R | B ± S.E. | R | B ± S.E. | R | B ± S.E. | |
| Muscle Thickness at 50% (cm) | 0.816 p < 0.001 | 11.098 ± 10.286 p = 0.302 | 0.861 p < 0.001 | 42.622 ± 20.024 p = 0.036 | 0.707 p < 0.001 | 174.654 ± 134.410 p = 0.197 | 0.850 p < 0.001 | 595.980 ± 200.221 p = 0.004 | 0.353 p = 0.025 | 1.348 ± 1.415 p = 0.334 | 0.900 p < 0.001 | 6.966 ± 3.328 p = 0.001 |
| Muscle Thickness at 75% (cm) | 0.826 p < 0.001 | 23.166 ± 9.955 p = 0.022 | 0.862 p < 0.001 | 42.533 ± 19.076 p = 0.025 | 0.719 p < 0.001 | 269.252 ± 126.430 p = 0.036 | 0.849 p < 0.001 | 555.550 ± 191.981 p = 0.005 | 0.347 p = 0.029 | 0.963 ± 1.357 p = 0.480 | 0.885 p < 0.001 | 0.307 ± 2.131 p = 0.886 |
| Echogenicity at 50% (A.U.) | 0.822 p < 0.001 | −0.271 ± 0.141 p = 0.059 | 0.854 p < 0.001 | −0.237 ± 0.275 p = 0.389 | 0.854 p < 0.001 | −5.809 ± 1.710 p = 0.001 | 0.836 p < 0.001 | −3.622 ± 2.804 p = 0.200 | 0.349 p = 0.027 | −0.016 ± 0.019 p = 0.412 | 0.895 p < 0.001 | −0.078 ± 0.029 p = 0.008 |
| Echogenicity at 75% (A.U.) | 0.817 p < 0.001 | −0.142 ± 0.129 p = 0.274 | 0.853 p < 0.001 | −0.058 ± 0.248 p = 0.815 | 0.853 p < 0.001 | −4.763 ± 1.550 p = 0.003 | 0.834 p < 0.001 | −4.763 ± 1.550 p = 0.370 | 0.376 p = 0.012 | −0.027 ± 0.017 p = 0.113 | 0.895 p < 0.001 | −0.071 ± 0.026 p = 0.007 |
| Muscle CSA at 50% (cm2) | 0.823 p < 0.001 | 3.406 ± 1.754 p = 0.056 | 0.867 p < 0.001 | 9.915 ± 3.271 p = 0.005 | 0.717 p < 0.001 | 44.281 ± 22.142 p = 0.049 | 0.860 p < 0.001 | 126.648 ± 32.205 p < 0.001 | 0.349 p = 0.028 | 0.193 ± 0.237 p = 0.418 | 0.897 p < 0.001 | 1.050 ± 0.354 p = 0.004 |
| Muscle CSA at 75% (cm2) | 0.828 p < 0.001 | 8.120 ± 3.245 p = 0.014 | 0.860 p < 0.001 | 12.464 ± 6.294 p = 0.051 | 0.726 p < 0.001 | 104.435 ± 40.951 p = 0.013 | 0.844 p < 0.001 | 153.621 ± 63.783 p = 0.018 | 0.341 p = 0.034 | 0.165 ± 0.445 p = 0.713 | 0.885 p < 0.001 | −0.154 ± 0.698 p = 0.826 |
| Variable Entered | Specific Force Variable | R | F4,83 | Age (Beta ± S.E.) | Gender (Beta ± S.E.) | BMI (Beta ± S.E.) | Entered Variable (Beta ± S.E.) |
|---|---|---|---|---|---|---|---|
| Echogenicity at 50% (A.U.) | Peak KE Torque by Muscle Thickness at 50% (Nm/cm) | 0.299 | 2.030 p = 0.098 | −0.799 ± 3.154 p = 0.801 | −106.185 ± 54.253 p = 0.054 | 10.527±4.306 p = 0.017 | −1.381 ± 0.770 p = 0.077 |
| Peak KE Torque by Muscle CSA at 50% (Nm/cm2) | 0.311 | 2.226 p = 0.073 | −0.625 ± 2.187 p = 0.776 | −5.110 ± 37.627 p = 0.892 | 6.163±2.986 p = 0.042 | −0.831 ± 0.534 p = 0.123 | |
| Echogenicity at 75% (A.U.) | Peak KE Torque by Muscle Thickness at 75% (Nm/cm) | 0.239 | 1.253 p = 0.295 | −0.074 ± 3.181 p = 0.982 | −45.255 ± 41.943 p = 0.284 | 9.403±4.341 p = 0.033 | −0.370 ± 0.702 p = 0.600 |
| Peak KE Torque by Muscle CSA at 75% (Nm/cm2) | 0.267 | 1.594 p = 0.184 | −0.161 ± 2.199 p = 0.535 | 32.388 ± 28.991 p = 0.267 | 5.416±3.001 p = 0.075 | −0.131 ± 0.485 p = 0.788 |
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Total (n = 50) | Below Median ABPI (n = 25) | Above Median ABPI (n = 25) | Total (n = 41) | Below Median ABPI (n = 21) | Above Median ABPI (n = 20) | |
| Relative Energy (kcal/kg/day) | 24.46 | 30.51 | 22.51 | 28.41 | 31.08 * | 26.73 |
| Relative Fat (g/kg/day) | 1.04 | 1.14 * | 0.90 | 1.15 | 1.20 | 0.99 |
| Fat Percent Energy (%) | 35.66 | 37.03 | 34.88 | 34.85 | 34.02 | 35.63 |
| Relative Carbohydrate (g/kg/day) | 2.85 | 3.22 ** | 2.30 | 3.56 | 4.12 ** | 2.81 |
| Carbohydrate Percent Energy (%) | 46.20 | 48.56 * | 44.36 | 46.86 | 48.82 *** | 41.16 |
| Relative Protein (g/kg/day) | 1.19 | 1.15 * | 1.25 | 1.28 | 1.28 | 1.24 |
| Protein Percent Energy (%) | 17.99 | 14.40 ** | 21.27 | 17.35 | 14.54 *** | 18.65 |
| Relative Animal Protein (g/kg/day) | 0.77 | 0.61 *** | 1.00 | 0.87 | 0.82 * | 0.96 |
| Animal Protein Percent Energy (%) | 11.99 | 8.59 *** | 16.08 | 11.74 | 10.39 *** | 15.16 |
| Relative Plant Protein (g/kg/day) | 0.31 | 0.37* | 0.27 | 0.34 | 0.39 ** | 0.29 |
| Plant Protein Percent Energy (%) | 4.92 | 5.23 | 4.81 | 4.56 | 4.77 | 4.26 |
| Vitamin D (IU/day) | 155.28 | 105.58 | 236.41 | 149.70 | 206.52 | 135.49 |
| Calcium (mg/day) | 849.06 | 743.91 ** | 951.94 | 1166.69 | 1103.57 | 1212.28 |
| Mg (mg/day) | 202.96 | 196.17 | 210.15 | 315.96 | 254.04 | 332.94 |
| Mn (mg/day) | 1.67 | 1.50 | 1.98 | 2.03 | 2.31 | 1.89 |
| Vitamin K (mcg/day) | 72.01 | 88.31 | 59.97 | 70.72 | 52.02 | 77.98 |
| Fe (mg/day) | 12.49 | 12.51 | 12.03 | 16.10 | 18.43 | 14.80 |
| Vitamin C (mg/day) | 107.42 | 84.78 | 115.31 | 79.03 | 86.42 | 54.11 |
| Vitamin E (mg/day) | 7.716 | 7.00 | 13.06 | 7.71 | 5.37 | 8.10 |
| P (mg/day) | 772.54 | 809.96 | 765.45 | 1314.39 | 1265.21 | 1349.81 |
| K (mg/day) | 1693.39 | 1692.27 | 1754.97 | 2577.01 | 2577.01 | 2576.71 |
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Total (n = 50) | Below Median ABPI (n = 25) | Above Median ABPI (n = 25) | Total (n = 41) | Below Median ABPI (n = 21) | Above Median ABPI (n = 20) | |
| Wear Days (days) | 7.00 | 6.00 | 7.007 | 7.00 | 7.00 * | 6.00 |
| Wear Time (min/day) | 867.04 | 869.50 | 864.57 | 895.33 | 895.71 | 891.87 |
| Sedentary Time (min/day) | 559.58 | 556.00 | 563.001 | 613.14 | 606.00 | 620.91 |
| Light Physical Activity (min/day) | 265.13 | 285.83 | 260.33 | 242.38 | 269.43 | 210.11 |
| Moderate Physical Activity (min/day) | 27.46 | 30.67 | 22.00 | 27.86 | 31.83 | 25.85 |
| Vigorous Physical Activity (min/day) | 0.15 | 0.14 | 0.29 | 0.33 | 2.00 | 0.00 |
| Moderate to Vigorous Physical Activity (min/day) | 31.05 | 31.20 | 27.14 | 33.25 | 33.83 | 27.00 |
| Variable | Variable | |||||||
|---|---|---|---|---|---|---|---|---|
| Relative Energy Intake | Relative Fat (g/kg/day) | Fat Percent Energy (%) | Relative Carbohydrate (g/kg/day) | Carbohydrate Percent Energy (%) | Relative Protein (g/kg/day) | Protein Percent Energy (%) | Relative Animal Protein (g/kg/day) | |
| Relative Fat (g/kg/day) | 0.819 p < 0.001 | - | - | - | - | - | - | - |
| Fat Percent Energy (%) | −0.120 p = 0.258 | 0.435 p < 0.001 | - | - | - | - | - | - |
| Relative Carbohydrate (g/kg/day) | 0.911 p < 0.001 | 0.534 p < 0.001 | -0.440 p < 0.001 | - | - | - | - | - |
| Carbohydrate Percent Energy (%) | 0.315 p = 0.002 | −0.188 p = 0.074 | −0.845 p < 0.001 | 0.648 p < 0.001 | - | - | - | - |
| Relative Protein (g/kg/day) | 0.755 p < 0.001 | 0.617 p < 0.001 | −0.144 p = 0.174 | 0.570 p < 0.001 | −0.019 p = 0.858 | - | - | - |
| Protein Percent Energy (%) | −0.353 p = 0.001 | −0.351 p = 0.001 | −0.114 p = 0.281 | −0.438 p < 0.001 | −0.438 p < 0.001 | 0.297 p = 0.004 | - | - |
| Relative Animal Protein (g/kg/day) | 0.548 p < 0.001 | 0.452 p < 0.001 | −0.122 p = 0.248 | 0.357 p = 0.001 | −0.138 p = 0.191 | 0.922 p < 0.001 | 0.473 p < 0.001 | - |
| Animal Protein Percent Energy (%) | −0.350 p < 0.001 | −0.332 p = 0.001 | −0.082 p = 0.439 | −0.440 p < 0.001 | −0.431 p < 0.001 | 0.277 p = 0.008 | 0.916 p < 0.001 | 0.550 p < 0.001 |
| Performance Variable | R | F9,81 | Age (Beta ± S.E.) | Gender (Beta ± S.E.) | BMI (Beta ± S.E.) | MVPA (Beta ± S.E.) | Relative Energy (Beta ± S.E.) | Fat Percent Energy (Beta ± S.E.) | Carbohydrate Percent Energy (Beta ± S.E.) | Protein Percent Energy (Beta ± S.E.) | Animal-Based Protein Intake Median Split (Beta ± S.E.) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Summed Isokinetic Peak Torque (Nm) | 0.887 | 33.111 p < 0.001 | −3.767 ± 1.138 p = 0.001 | 190.543 ± 13.850 p < 0.001 | 1.694 ± 1.874 p = 0.369 | 0.287 ± 0.395 p = 0.469 | −0.829 ± 0.862 p = 0.339 | −3.754 ± 8.467 p = 0.659 | −3.889 ± 8.351 p = 0.643 | −5.769 ± 8.007 p = 0.473 | 65.874 ± 19.855 p = 0.001 |
| Summed Isokinetic Work (J) | 0.870 | 28.032 p < 0.001 | −46.224 ± 11.546 p < 0.001 | 1671.298 ± 126.695 p < 0.001 | 29.436 ± 19.814 p = 0.141 | 2.842 ± 4.617 p = 0.540 | 16.825 ± 9.500 p = 0.080 | −100.977 ± 76.033 p = 0.188 | −95.794 ± 76.033 p = 0.204 | −92.620 ± 71.011 p = 0.196 | 549.944 ± 232.478 p = 0.020 |
| Transformed 30-Second Chair Stand (repetitions #) | 0.437 | 2.128 p = 0.036 | 0.004 ± 0.010 p = 0.700 | 0.316 ± 0.128 p = 0.016 | −0.024 ± 0.013 p = 0.081 | 0.000 ± 0.003 p = 0.940 | 0.008 ± 0.009 p = 0.859 | −0.092 ± 0.077 p = 0.237 | −0.103 ± 0.076 p = 0.182 | −0.095 ± 0.076 p = 0.214 | 0.086 ± 0.156 p = 0.584 |
| Transformed Handgrip Strength (kg) | 0.913 | 45.026 p < 0.001 | −0.029 ± 0.008 p = 0.001 | 1.898 ± 0.105 p < 0.001 | 0.001 ± 0.018 p = 0.956 | 0.003 ± 0.003 p = 0.295 | −0.008 ± 0.008 p = 0.323 | −0.083 ± 0.042 p = 0.052 | −0.091 ± 0.041 p = 0.027 | −0.111 ± 0.040 p = 0.007 | 0.349 ± 0.171 p = 0.045 |
| Performance Variable | R | F9,81 | Age (Beta ± S.E.) | Gender (Beta ± S.E.) | BMI (Beta ± S.E.) | MVPA (Beta ± S.E.) | Relative Energy (Beta ± S.E.) | Fat Percent Energy (Beta ± S.E.) | Carbohydrate Percent Energy (Beta ± S.E.) | ABPI Energy (Beta ± S.E.) | Total Protein Intake Median Split (Beta ± S.E.) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Summed Isokinetic Peak Torque (Nm) | 0.871 | 28.366 p < 0.001 | −4.013 ± 1.171 p = 0.001 | 189.571 ± 14.575 p < 0.001 | 2.003 ± 2.029 p = 0.326 | 0.194 ± 0.427 p = 0.651 | −0.792 ± 0.962 p = 0.413 | −0.049 ± 4.836 p = 0.992 | −0.681 ± 4.576 p = 0.882 | 1.754 ± 3.637 p = 0.631 | 19.397 ± 23.176 p = 0.405 |
| Summed Isokinetic Work (J) | 0.856 | 24.638 p < 0.001 | −47.751 ± 12.387 p < 0.001 | 1654.781 ± 134.463 p < 0.001 | 32.111 ± 22.256 p = 0.153 | 2.090 ± 5.296 p = 0.694 | 16.687 ± 10.609 p = 0.120 | −24.735 ± 61.303 p = 0.688 | −24.971 ± 58.990 p = 0.673 | 29.836 ± 43.397 p = 0.494 | −2.405± 258.849 p = 0.993 |
| Transformed 30-Second Chair Stand (repetitions #) | 0.409 | 1.806 p = 0.080 | 0.004 ± 0.011 p = 0.728 | 0.313 ± 0.130 p = 0.018 | −0.024 ± 0.013 p = 0.084 | 0.000 ± 0.003 p = 0.958 | 0.007 ± 0.009 p = 0.466 | −0.011 ± 0.043 p = 0.803 | −0.024 ± 0.040 p = 0.549 | 0.003 ± 0.043 p = 0.939 | −0.112 ± 0.172 p = 0.519 |
| Transformed Handgrip Strength (kg) | 0.904 | 40.523 p < 0.001 | −0.030 ± 0.009 p = 0.001 | 1.901 ± 0.121 p < 0.001 | 0.004 ± 0.0.019 p = 0.834 | 0.002 ± 0.003 p = 0.680 | −0.008 ± 0.008 p = 0.360 | −0.018 ± 0.043 p = 0.683 | −0.031 ± 0.042 p = 0.459 | 0.000 ± 0.032 p = 0.997 | 0.187 ± 0.197 p = 0.953 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, N.R.; Kotarsky, C.J.; Hackney, K.J.; Trautman, K.A.; Dicks, N.D.; Byun, W.; Keith, J.F.; David, S.L.; Stastny, S.N. Measures Derived from Panoramic Ultrasonography and Animal-Based Protein Intake Are Related to Muscular Performance in Middle-Aged Adults. J. Clin. Med. 2021, 10, 988. https://doi.org/10.3390/jcm10050988
Johnson NR, Kotarsky CJ, Hackney KJ, Trautman KA, Dicks ND, Byun W, Keith JF, David SL, Stastny SN. Measures Derived from Panoramic Ultrasonography and Animal-Based Protein Intake Are Related to Muscular Performance in Middle-Aged Adults. Journal of Clinical Medicine. 2021; 10(5):988. https://doi.org/10.3390/jcm10050988
Chicago/Turabian StyleJohnson, Nathaniel R., Christopher J. Kotarsky, Kyle J. Hackney, Kara A. Trautman, Nathan D. Dicks, Wonwoo Byun, Jill F. Keith, Shannon L. David, and Sherri N. Stastny. 2021. "Measures Derived from Panoramic Ultrasonography and Animal-Based Protein Intake Are Related to Muscular Performance in Middle-Aged Adults" Journal of Clinical Medicine 10, no. 5: 988. https://doi.org/10.3390/jcm10050988