
Reduction of Phantom Limb Pain and Improved Proprioception through a TSR-Based Surgical Technique: A Case Series of Four Patients with Lower Limb Amputation

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Procedures
2.3. Assessments
2.4. Analysis
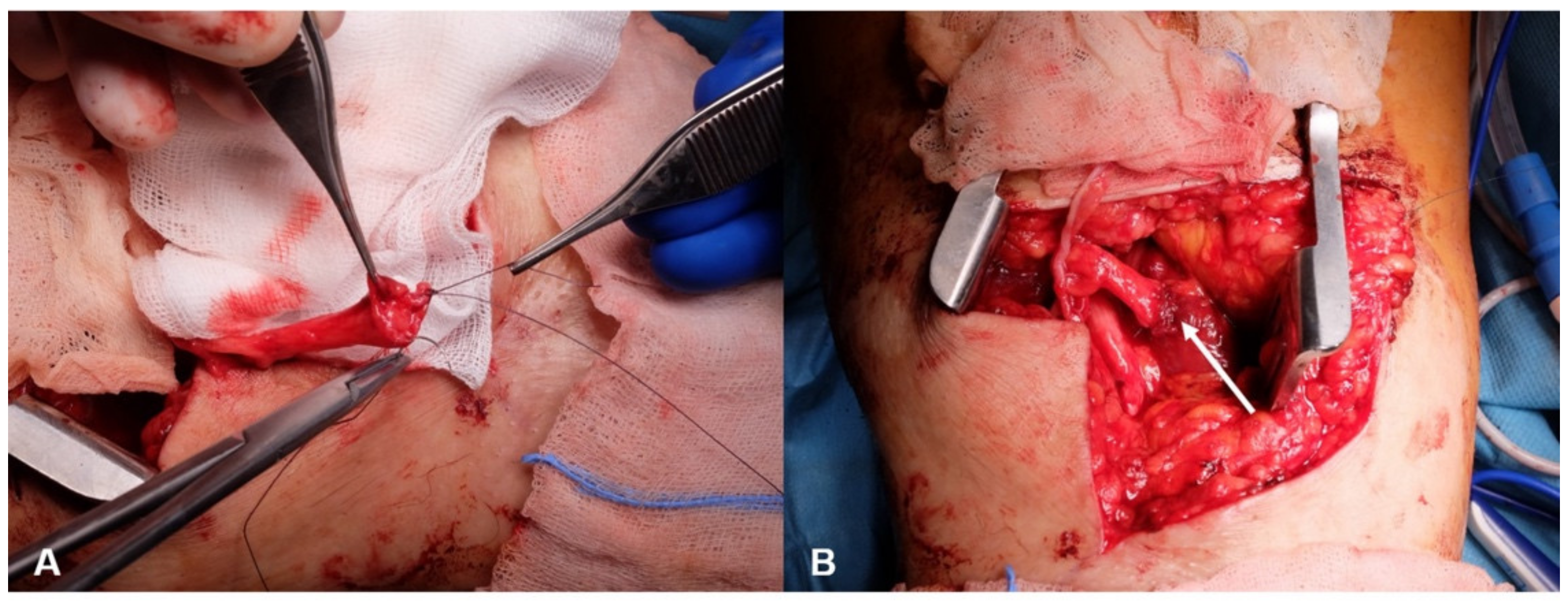
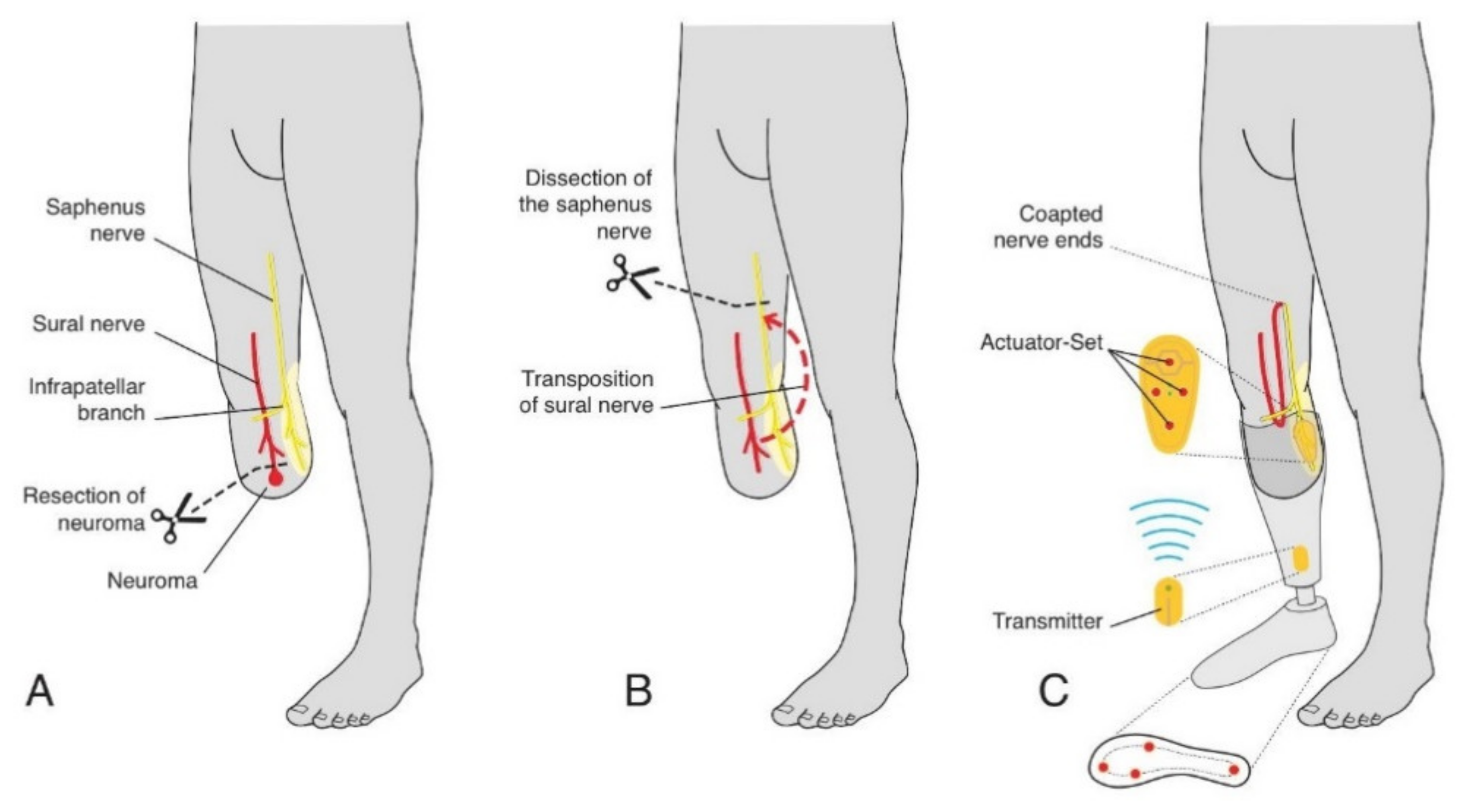
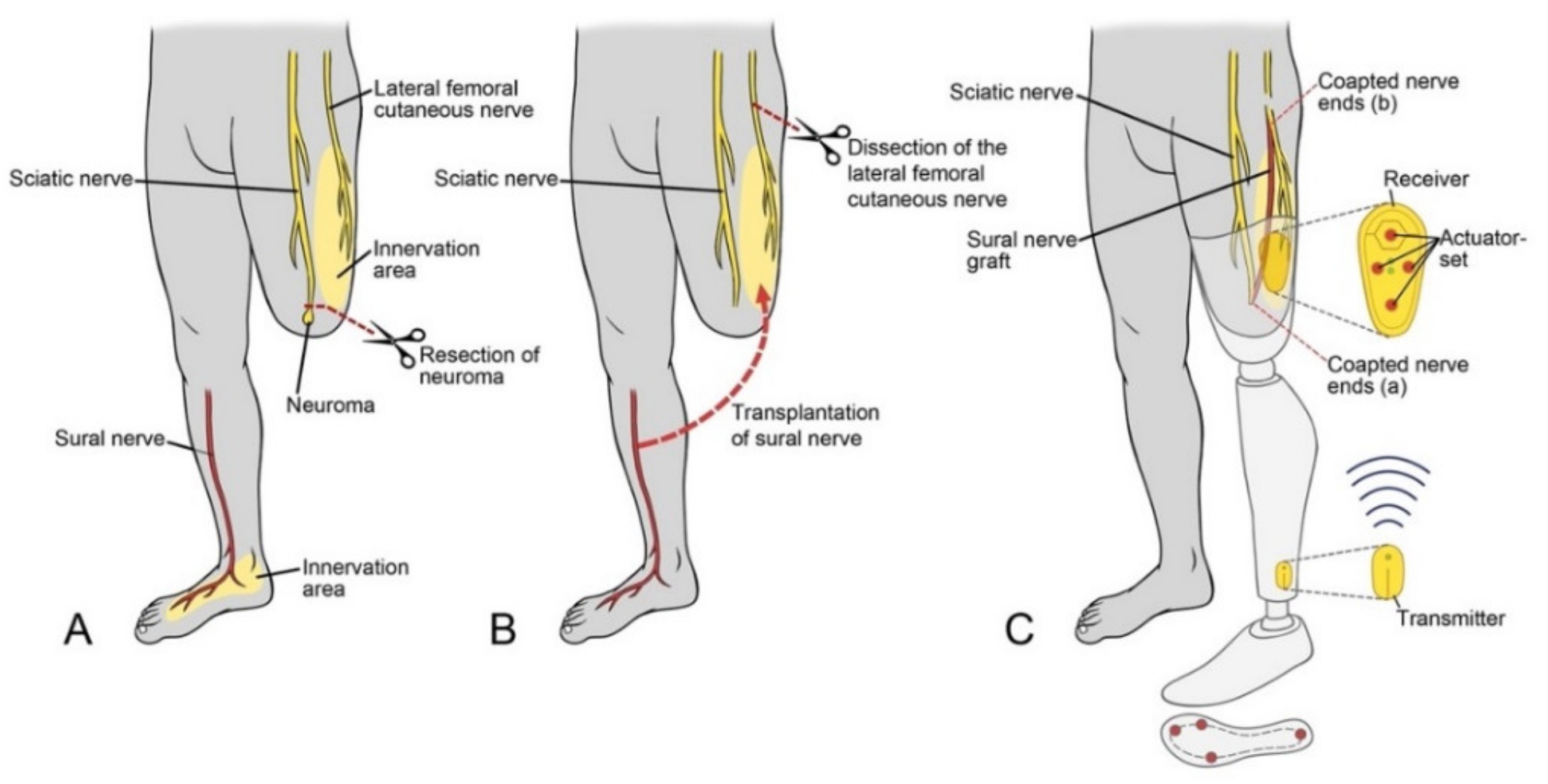
2.5. Surgical Techniques
2.6. Rehabilitation
2.7. Physical Therapy
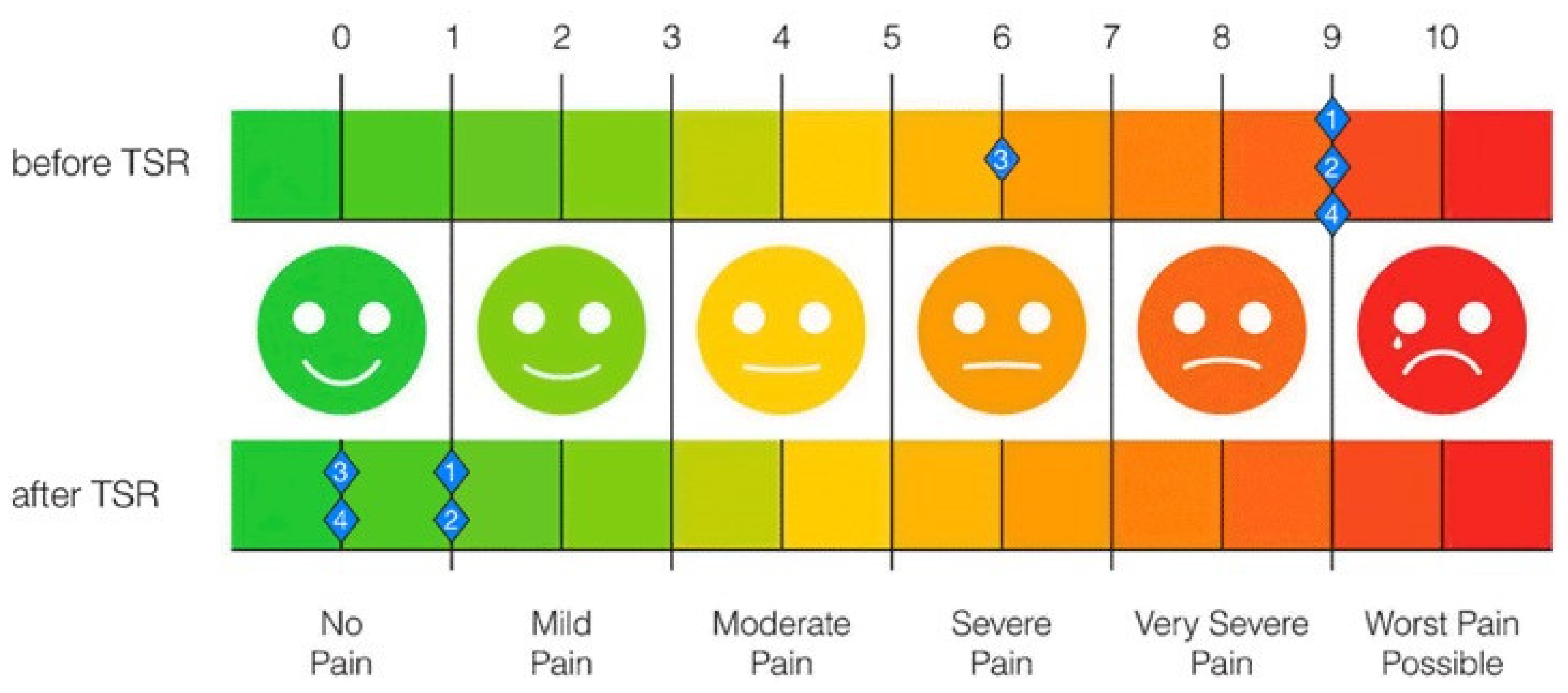
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ephraim, P.L.; Wegener, S.T.; MacKenzie, E.J.; Dillingham, T.R.; Pezzin, L.E. Phantom pain, residual limb pain, and back pain in amputees: Results of a national survey. Arch. Phys. Med. Rehabil. 2005, 86, 1910–1919. [Google Scholar] [CrossRef]
- Flor, H.; Nikolajsen, L.; Staehelin Jensen, T. Phantom limb pain: A case of maladaptive CNS plasticity? Nat. Rev. Neurosci. 2006, 7, 873–881. [Google Scholar] [CrossRef]
- Hsu, E.; Cohen, S.P. Postamputation pain: Epidemiology, mechanisms, and treatment. J. Pain Res. 2013, 6, 121–136. [Google Scholar] [CrossRef] [Green Version]
- Economides, J.M.; DeFazio, M.V.; Attinger, C.E.; Barbour, J.R. Prevention of Painful Neuroma and Phantom Limb Pain after Transfemoral Amputations Through Concomitant Nerve Coaptation and Collagen Nerve Wrapping. Neurosurgery 2016, 79, 508–513. [Google Scholar] [CrossRef]
- Pet, M.A.; Ko, J.H.; Friedly, J.L.; Mourad, P.D.; Smith, D.G. Does targeted nerve implantation reduce neuroma pain in amputees? Clin. Orthop. Relat. Res. 2014, 472, 2991–3001. [Google Scholar] [CrossRef] [Green Version]
- Alviar, M.J.; Hale, T.; Dungca, M. Pharmacologic interventions for treating phantom limb pain. Cochrane Database Syst. Rev. 2016, 10, CD006380. [Google Scholar] [CrossRef]
- Borghi, B.; D’Addabbo, M.; White, P.F.; Gallerani, P.; Toccaceli, L.; Raffaeli, W.; Tognu, A.; Fabbri, N.; Mercuri, M. The use of prolonged peripheral neural blockade after lower extremity amputation: The effect on symptoms associated with phantom limb syndrome. Anesth. Analg. 2010, 111, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Poppler, L.H.; Parikh, R.P.; Bichanich, M.J.; Rebehn, K.; Bettlach, C.R.; Mackinnon, S.E.; Moore, A.M. Surgical interventions for the treatment of painful neuroma: A comparative meta-analysis. Pain 2018, 159, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Catalan, M.; Guethmundsdottir, R.A.; Kristoffersen, M.B.; Zepeda-Echavarria, A.; Caine-Winterberger, K.; Kulbacka-Ortiz, K.; Widehammar, C.; Eriksson, K.; Stockselius, A.; Ragno, C.; et al. Phantom motor execution facilitated by machine learning and augmented reality as treatment for phantom limb pain: A single group, clinical trial in patients with chronic intractable phantom limb pain. Lancet 2016, 388, 2885–2894. [Google Scholar] [CrossRef]
- Serino, A.; Akselrod, M.; Salomon, R.; Martuzzi, R.; Blefari, M.L.; Canzoneri, E.; Rognini, G.; van der Zwaag, W.; Iakova, M.; Luthi, F.; et al. Upper limb cortical maps in amputees with targeted muscle and sensory reinnervation. Brain 2017, 140, 2993–3011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuiken, T. Targeted reinnervation for improved prosthetic function. Phys. Med. Rehabil. Clin. N. Am. 2006, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kuiken, T.A.; Dumanian, G.A.; Lipschutz, R.D.; Miller, L.A.; Stubblefield, K.A. The use of targeted muscle reinnervation for improved myoelectric prosthesis control in a bilateral shoulder disarticulation amputee. Prosthet. Orthot. Int. 2004, 28, 245–253. [Google Scholar] [CrossRef] [Green Version]
- Oh, C.; Carlsen, B.T. New Innovations in Targeted Muscle Reinnervation: A Critical Analysis Review. JBJS Rev. 2019, 7, e3. [Google Scholar] [CrossRef]
- Kuiken, T.A.; Marasco, P.D.; Lock, B.A.; Harden, R.N.; Dewald, J.P. Redirection of cutaneous sensation from the hand to the chest skin of human amputees with targeted reinnervation. Proc. Natl. Acad. Sci. USA 2007, 104, 20061–20066. [Google Scholar] [CrossRef] [Green Version]
- Hebert, J.S.; Olson, J.L.; Morhart, M.J.; Dawson, M.R.; Marasco, P.D.; Kuiken, T.A.; Chan, K.M. Novel targeted sensory reinnervation technique to restore functional hand sensation after transhumeral amputation. IEEE Trans. Neural. Syst. Rehabil. Eng. 2014, 22, 765–773. [Google Scholar] [CrossRef]
- Miller, L.A.; Stubblefield, K.A.; Lipschutz, R.D.; Lock, B.A.; Kuiken, T.A. Improved myoelectric prosthesis control using targeted reinnervation surgery: A case series. IEEE Trans. Neural. Syst. Rehabil. Eng. 2008, 16, 46–50. [Google Scholar] [CrossRef] [Green Version]
- Nghiem, B.T.; Sando, I.C.; Gillespie, R.B.; McLaughlin, B.L.; Gerling, G.J.; Langhals, N.B.; Urbanchek, M.G.; Cederna, P.S. Providing a sense of touch to prosthetic hands. Plast. Reconstr. Surg. 2015, 135, 1652–1663. [Google Scholar] [CrossRef] [PubMed]
- Petrini, F.M.; Valle, G.; Strauss, I.; Granata, G.; Di Iorio, R.; D’Anna, E.; Cvancara, P.; Mueller, M.; Carpaneto, J.; Clemente, F.; et al. Six-Month Assessment of a Hand Prosthesis with Intraneural Tactile Feedback. Ann. Neurol. 2019, 85, 137–154. [Google Scholar] [CrossRef]
- Svensson, P.; Wijk, U.; Bjorkman, A.; Antfolk, C. A review of invasive and non-invasive sensory feedback in upper limb prostheses. Expert. Rev. Med. Devices. 2017, 14, 439–447. [Google Scholar] [CrossRef]
- Crea, S.; Cipriani, C.; Donati, M.; Carrozza, M.C.; Vitiello, N. Providing time-discrete gait information by wearable feedback apparatus for lower-limb amputees: Usability and functional validation. IEEE Trans. Neural. Syst. Rehabil. Eng. 2015, 23, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.; Nehrdich, S.; Seifert, S.; Blume, K.R.; Miltner, W.H.R.; Hofmann, G.O.; Weiss, T. Leg Prosthesis With Somatosensory Feedback Reduces Phantom Limb Pain and Increases Functionality. Front. Neurol. 2018, 9, 270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raspopovic, S.; Valle, G.; Petrini, F.M. Sensory feedback for limb prostheses in amputees. Nat. Mater. 2021, 20, 925–939. [Google Scholar] [CrossRef] [PubMed]
- Petrini, F.M.; Bumbasirevic, M.; Valle, G.; Ilic, V.; Mijovic, P.; Cvancara, P.; Barberi, F.; Katic, N.; Bortolotti, D.; Andreu, D.; et al. Sensory feedback restoration in leg amputees improves walking speed, metabolic cost and phantom pain. Nat. Med. 2019, 25, 1356–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelechowski, M.; Valle, G.; Raspopovic, S. A computational model to design neural interfaces for lower-limb sensory neuroprostheses. J. Neuroeng. Rehabil. 2020, 17, 24. [Google Scholar] [CrossRef] [PubMed]
- Jay, S.J. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 2000, 161, 1396. [Google Scholar] [CrossRef]
- Moore, M.; Barker, K. The validity and reliability of the four square step test in different adult populations: A systematic review. Syst. Rev. 2017, 6, 187. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed ″Up & Go″: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Bartusch, S.L.; Sanders, B.J.; D’Alessio, J.G.; Jernigan, J.R. Clonazepam for the treatment of lancinating phantom limb pain. Clin. J. Pain 1996, 12, 59–62. [Google Scholar] [CrossRef]
- Mucke, M.; Cuhls, H.; Radbruch, L.; Weigl, T.; Rolke, R. Evidence of heterosynaptic LTD in the human nociceptive system: Superficial skin neuromodulation using a matrix electrode reduces deep pain sensitivity. PLoS ONE 2014, 9, e107718. [Google Scholar] [CrossRef]
- Souza, J.M.; Cheesborough, J.E.; Ko, J.H.; Cho, M.S.; Kuiken, T.A.; Dumanian, G.A. Targeted muscle reinnervation: A novel approach to postamputation neuroma pain. Clin. Orthop. Relat. Res. 2014, 472, 2984–2990. [Google Scholar] [CrossRef] [Green Version]
- Bowen, J.B.; Wee, C.E.; Kalik, J.; Valerio, I.L. Targeted Muscle Reinnervation to Improve Pain, Prosthetic Tolerance, and Bioprosthetic Outcomes in the Amputee. Adv. Wound Care New Rochelle 2017, 6, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Kubiak, C.A.; Kemp, S.W.P.; Cederna, P.S.; Kung, T.A. Prophylactic Regenerative Peripheral Nerve Interfaces to Prevent Postamputation Pain. Plast. Reconstr. Surg. 2019, 144, 421e–430e. [Google Scholar] [CrossRef]
- Alexander, J.H.; Jordan, S.W.; West, J.M.; Compston, A.; Fugitt, J.; Bowen, J.B.; Dumanian, G.A.; Pollock, R.; Mayerson, J.L.; Scharschmidt, T.J.; et al. Targeted muscle reinnervation in oncologic amputees: Early experience of a novel institutional protocol. J. Surg. Oncol. 2019, 120, 348–358. [Google Scholar] [CrossRef]
- Chappell, A.G.; Jordan, S.W.; Dumanian, G.A. Targeted Muscle Reinnervation for Treatment of Neuropathic Pain. Clin. Plast. Surg. 2020, 47, 285–293. [Google Scholar] [CrossRef]
- Valerio, I.L.; Dumanian, G.A.; Jordan, S.W.; Mioton, L.M.; Bowen, J.B.; West, J.M.; Porter, K.; Ko, J.H.; Souza, J.M.; Potter, B.K. Preemptive Treatment of Phantom and Residual Limb Pain with Targeted Muscle Reinnervation at the Time of Major Limb Amputation. J. Am. Coll Surg. 2019, 228, 217–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumanian, G.A.; Potter, B.K.; Mioton, L.M.; Ko, J.H.; Cheesborough, J.E.; Souza, J.M.; Ertl, W.J.; Tintle, S.M.; Nanos, G.P.; Valerio, I.L.; et al. Targeted Muscle Reinnervation Treats Neuroma and Phantom Pain in Major Limb Amputees: A Randomized Clinical Trial. Ann. Surg. 2019, 270, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Arakeri, T.J.; Hasse, B.A.; Fuglevand, A.J. Object discrimination using electrotactile feedback. J. Neural. Eng. 2018, 15, 046007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strbac, M.; Isakovic, M.; Belic, M.; Popovic, I.; Simanic, I.; Farina, D.; Keller, T.; Dosen, S. Short- and Long-Term Learning of Feedforward Control of a Myoelectric Prosthesis with Sensory Feedback by Amputees. IEEE Trans. Neural. Syst. Rehabil. Eng. 2017, 25, 2133–2145. [Google Scholar] [CrossRef]
- Rokhmanova, N.; Rombokas, E. Vibrotactile Feedback Improves Foot Placement Perception on Stairs for Lower-Limb Prosthesis Users. IEEE Int. Conf. Rehabil. Robot. 2019, 2019, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Rusaw, D.; Hagberg, K.; Nolan, L.; Ramstrand, N. Can vibratory feedback be used to improve postural stability in persons with transtibial limb loss? J. Rehabil. Res. Dev. 2012, 49, 1239–1254. [Google Scholar] [CrossRef] [PubMed]
- Antfolk, C.; D’Alonzo, M.; Controzzi, M.; Lundborg, G.; Rosen, B.; Sebelius, F.; Cipriani, C. Artificial redirection of sensation from prosthetic fingers to the phantom hand map on transradial amputees: Vibrotactile versus mechanotactile sensory feedback. IEEE Trans. Neural. Syst. Rehabil. Eng. 2013, 21, 112–120. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age at Injury (Year of Injury) | Mechanism of Injury | Side of Injury | Number of Operations | Age at Amputation (Year of Amputation) | Time between Injury and Amputation | Height of Amputation | Massive Phantom Limb and Neuroma Pain | Date of TSR Surgery | Donor Nerve | Target Nerve |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 46 (2007) | Stroke and deep vein thrombosis | Left | 4 | 46 (2007) | 4 months | Posttraumatic Limb | Yes | October 2014 | Ipsilateral sural nerve | Saphenous nerve |
| 2 | Male | 25 (1989) | Motorcycle accident | Left | 35 | 41 (2005) | 16 years | Posttraumatic Thigh | Yes | November 2018 | Contralateral sural nerve | Lateral femoral cutaneous nerve |
| 3 | Male | 42 (2017) | Car accident | Left | 12 | 44 (2019) | 2 years | Elective Thigh | No | November 2019 | Ipsilateral sural nerve | Lateral femoral cutaneous nerve |
| 4 | Female | 50 (2011) | Motorcycle accident | Left | 6 | 50 (2011) | 1 day | Acute Limb | Yes | February 2020 | Contralateral sural nerve | Lateral femoral cutaneous nerve |
| TSR Operation | Begin of Physical Therapy | Type of Physical Therapy | Begin of Sensation | Sensation of the Foot on Reinnervated Skin Area | Phantom Limb Pain | Permanent Pain Medication | Status | |
|---|---|---|---|---|---|---|---|---|
| 1 | October 2014 | 3 weeks after surgery | Tens and Vibro | 5 months after surgery | Whole foot with toes, heel, Achilles tendon | No | Yes, for residual limb pain | Regeneration completed |
| 2 | November 2018 | 2 weeks after surgery | Tens and Vibro | 6 months after surgery | Whole foot with toes, heel, Achilles tendon | No | None | Regeneration completed |
| 3 | November 2019 | 2 weeks after surgery | Tens and Vibro | 4 months after surgery | Whole foot with toes, heel, Achilles tendon | No | None | Regeneration completed |
| 4 | February 2020 | 2 weeks after surgery | Tens and Vibro | 5 months after surgery | heel, lateral part of the foot and foot sole, 4th and 5th toe, Achilles tendon | No | None | Regeneration in final phase |
| Type of Medication | Before TSR [P#] | After TSR [P#] |
|---|---|---|
| Opioids | 4, 3, 2, 1 | 1 |
| Anticonvulsants | 4, 2, 3, 1 | 0 |
| NSAID | 4 | 0 |
| Novalminsulfon | 4, 3 | 0 |
| Antidepressant | 1, 3 | 0 |
| Cannabinoids | 0 | 1 |
| Frequency of Medication | ||
| Nothing | 0 | 2, 3, 4 |
| on demand | 0 | 1 (Opioids) |
| 2–3 a day | 2 | 1 (Cannabinoid) |
| 4–5 a day | 4, 3 | |
| 6 and more a day | 1 |
| Conventional Prosthesis | Medical Device Suralis after 90 Days | Improvement in % | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Δ% | |
| Timed Up the Go Test [s] | 8.10 ± 0.31 | 7.44 ± 0.2 | 8.2% |
| Four Step Square Test [s] | 10.03 ± 0.39 | 7.15 ± 0.28 | 40.1% |
| 6 MWT [m] | 450 ± 0 | 500 ± 0 | 11.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gardetto, A.; Baur, E.-M.; Prahm, C.; Smekal, V.; Jeschke, J.; Peternell, G.; Pedrini, M.T.; Kolbenschlag, J. Reduction of Phantom Limb Pain and Improved Proprioception through a TSR-Based Surgical Technique: A Case Series of Four Patients with Lower Limb Amputation. J. Clin. Med. 2021, 10, 4029. https://doi.org/10.3390/jcm10174029
Gardetto A, Baur E-M, Prahm C, Smekal V, Jeschke J, Peternell G, Pedrini MT, Kolbenschlag J. Reduction of Phantom Limb Pain and Improved Proprioception through a TSR-Based Surgical Technique: A Case Series of Four Patients with Lower Limb Amputation. Journal of Clinical Medicine. 2021; 10(17):4029. https://doi.org/10.3390/jcm10174029
Chicago/Turabian StyleGardetto, Alexander, Eva-Maria Baur, Cosima Prahm, Vinzenz Smekal, Johannes Jeschke, Gerfried Peternell, Michael T. Pedrini, and Jonas Kolbenschlag. 2021. "Reduction of Phantom Limb Pain and Improved Proprioception through a TSR-Based Surgical Technique: A Case Series of Four Patients with Lower Limb Amputation" Journal of Clinical Medicine 10, no. 17: 4029. https://doi.org/10.3390/jcm10174029
APA StyleGardetto, A., Baur, E.-M., Prahm, C., Smekal, V., Jeschke, J., Peternell, G., Pedrini, M. T., & Kolbenschlag, J. (2021). Reduction of Phantom Limb Pain and Improved Proprioception through a TSR-Based Surgical Technique: A Case Series of Four Patients with Lower Limb Amputation. Journal of Clinical Medicine, 10(17), 4029. https://doi.org/10.3390/jcm10174029