
Real-Time Evaluation of Optic Nerve Sheath Diameter (ONSD) in Awake, Spontaneously Breathing Patients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. ONSD Measurement
2.3. Statistical Analysis
3. Results
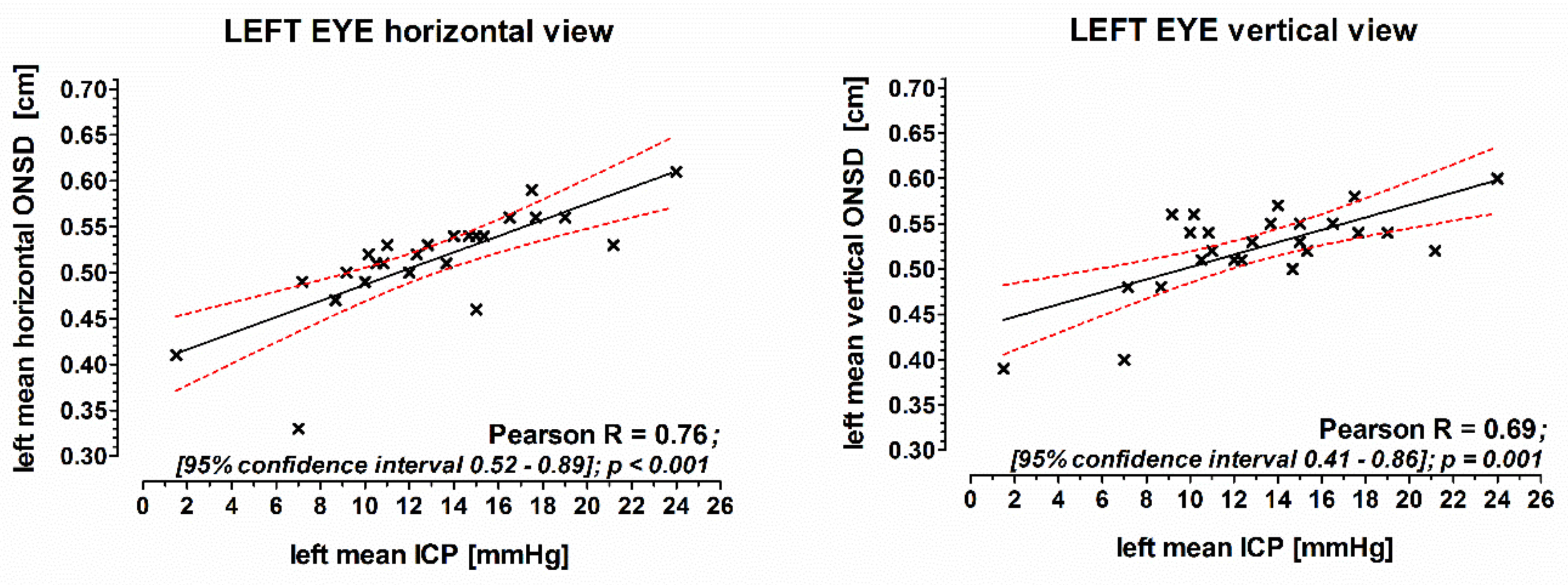
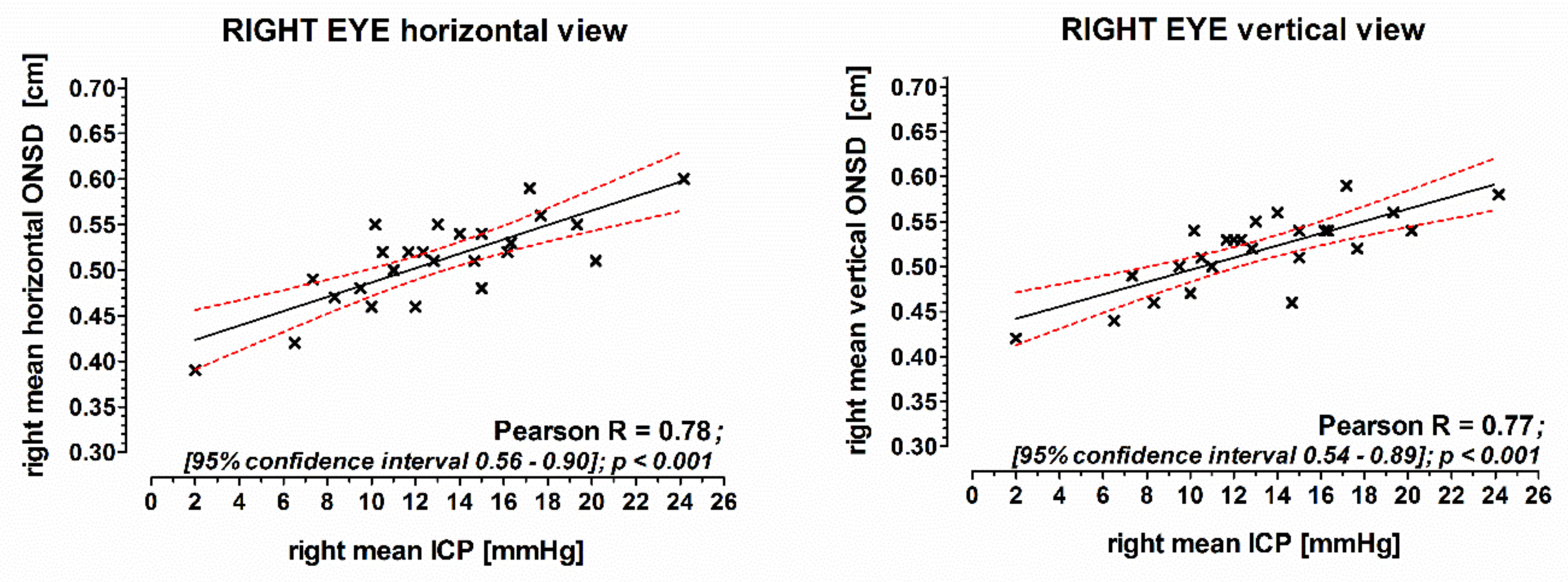
3.1. Correlation of the ONSD with Intracranial Pressure
3.2. Accuracy and Precision of ONSD Measurements
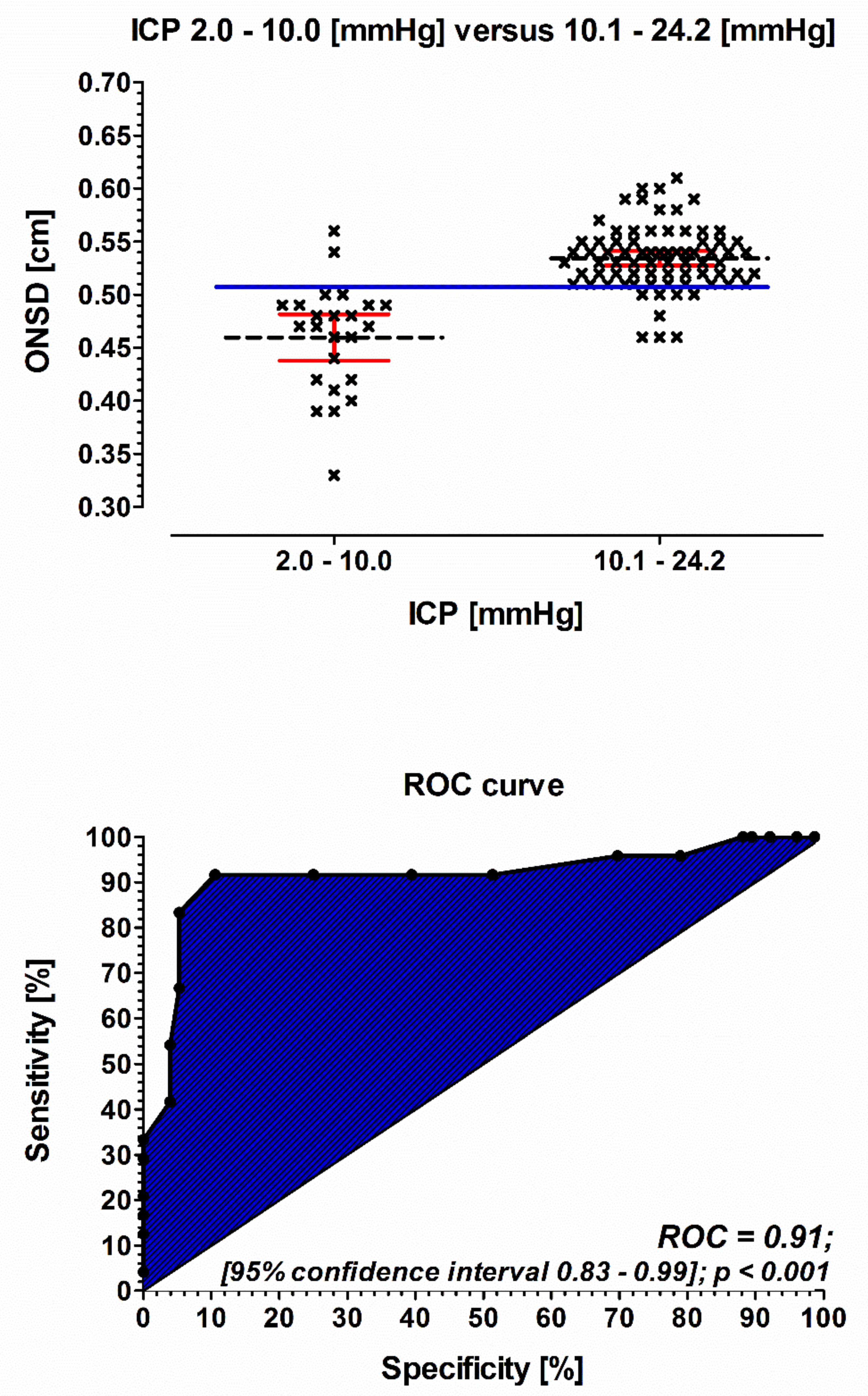
3.3. ROC Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Juul, N.; Morris, G.F.; Marshall, S.B.; Marshall, L.F. Intracranial hypertension and cerebral perfusion pressure: Influence on neurological deterioration and outcome in severe head injury. The Executive Committee of the International Selfotel Trial. J. Neurosurg. 2000, 92, 1–6. [Google Scholar] [CrossRef]
- Balestreri, M.; Czosnyka, M.; Hutchinson, P.; Steiner, L.A.; Hiler, M.; Smielewski, P.; Pickard, J.D. Impact of intracranial pressure and cerebral perfusion pressure on severe disability and mortality after head injury. Neurocritical Care 2006, 4, 8–13. [Google Scholar] [CrossRef]
- Sacco, T.L.; Davis, J.G. Management of Intracranial Pressure Part II: Nonpharmacologic Interventions. Dimens. Crit. Care Nurs. 2019, 38, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Kochanek, P.M.; Carney, N.; Adelson, P.D.; Ashwal, S.; Bell, M.J.; Bratton, S.; Carson, S.; Chesnut, R.M.; Ghajar, J.; Goldstein, B.; et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents--second edition. Pediatr. Crit. Care Med. 2012, 13 (Suppl. S1), S1–S82. [Google Scholar] [CrossRef] [PubMed]
- Wilberger, J.E., Jr. Outcomes analysis: Intracranial pressure monitoring. Clin. Neurosurg. 1997, 44, 439–448. [Google Scholar] [PubMed]
- Hiler, M.; Czosnyka, M.; Hutchinson, P.; Balestreri, M.; Smielewski, P.; Matta, B.; Pickard, J.D. Predictive value of initial computerized tomography scan, intracranial pressure, and state of autoregulation in patients with traumatic brain injury. J. Neurosurg. 2006, 104, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Winkler, F.; Kastenbauer, S.; Yousry, T.A.; Maerz, U.; Pfister, H.W. Discrepancies between brain CT imaging and severely raised intracranial pressure proven by ventriculostomy in adults with pneumococcal meningitis. J. Neurol. 2002, 249, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Czosnyka, M.; Hutchinson, P.J.; Balestreri, M.; Hiler, M.; Smielewski, P.; Pickard, J.D. Monitoring and interpretation of intracranial pressure after head injury. Acta Neurochir. Suppl. 2006, 96, 114–118. [Google Scholar]
- Bender, M.; Lakicevic, S.; Pravdic, N.; Schreiber, S.; Malojcic, B. Optic nerve sheath diameter sonography during the acute stage of intracerebral hemorrhage: A potential role in monitoring neurocritical patients. Ultrasound J. 2020, 12, 47. [Google Scholar] [CrossRef] [PubMed]
- Galetta, S.; Byrne, S.F.; Smith, J.L. Echographic correlation of optic nerve sheath size and cerebrospinal fluid pressure. J. Clin. Neuro-Ophthalmol. 1989, 9, 79–82. [Google Scholar]
- Hansen, H.C.; Helmke, K. Validation of the optic nerve sheath response to changing cerebrospinal fluid pressure: Ultrasound findings during intrathecal infusion tests. J. Neurosurg. 1997, 87, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Helmke, K.; Hansen, H.C. Fundamentals of transorbital sonographic evaluation of optic nerve sheath expansion under intracranial hypertension II. Patient study. Pediatr. Radiol. 1996, 26, 706–710. [Google Scholar] [CrossRef]
- Geeraerts, T.; Launey, Y.; Martin, L.; Pottecher, J.; Vigue, B.; Duranteau, J.; Benhamou, D. Ultrasonography of the optic nerve sheath may be useful for detecting raised intracranial pressure after severe brain injury. Intensiv. Care Med. 2007, 33, 1704–1711. [Google Scholar] [CrossRef] [PubMed]
- Geeraerts, T.; Merceron, S.; Benhamou, D.; Vigue, B.; Duranteau, J. Non-invasive assessment of intracranial pressure using ocular sonography in neurocritical care patients. Intensiv. Care Med. 2008, 34, 2062–2067. [Google Scholar] [CrossRef]
- Soldatos, T.; Karakitsos, D.; Chatzimichail, K.; Papathanasiou, M.; Gouliamos, A.; Karabinis, A. Optic nerve sonography in the diagnostic evaluation of adult brain injury. Crit. Care 2008, 12, R67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Launey, Y.; Nesseler, N.; Le Maguet, P.; Malledant, Y.; Seguin, P. Effect of osmotherapy on optic nerve sheath diameter in patients with increased intracranial pressure. J. Neurotrauma 2014, 31, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Chen, L.M.; Chen, Y.; Bao, L.Y.; Zheng, N.N.; Wang, Y.Z.; Xing, Y.Q. Ultrasonography Assessments of Optic Nerve Sheath Diameter as a Noninvasive and Dynamic Method of Detecting Changes in Intracranial Pressure. JAMA Ophthalmol. 2018, 136, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.M.; Wang, L.J.; Hu, Y.; Jiang, X.H.; Wang, Y.Z.; Xing, Y.Q. Ultrasonic measurement of optic nerve sheath diameter: A non-invasive surrogate approach for dynamic, real-time evaluation of intracranial pressure. Br. J. Ophthalmol. 2019, 103, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Society and College of Radiographers and British Medical Ultrasound Society. Guidelines for Professional Ultrasound Practice. Available online: https://www.bmus.org/static/uploads/resources/GUIDELINES_FOR_PROFESSIONAL_ULTRASOUND_PRACTICE.pdf (accessed on 19 April 2021).
- Food and Drug Administration. Marketing Clearance of Diagnostic Ultrasound Systems and Transducers. Guidance for Industry and Food and Drug Administration Staff. Available online: https://www.fda.gov/media/71100/download (accessed on 19 April 2021).
- Dubourg, J.; Javouhey, E.; Geeraerts, T.; Messerer, M.; Kassai, B. Ultrasonography of optic nerve sheath diameter for detection of raised intracranial pressure: A systematic review and meta-analysis. Intensiv. Care Med. 2011, 37, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.; Varelas, P.N.; Gronseth, G.S.; Greer, D.M. Evidence-based guideline update: Determining brain death in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2010, 74, 1911–1918. [Google Scholar] [CrossRef] [Green Version]
- Bauerle, J.; Lochner, P.; Kaps, M.; Nedelmann, M. Intra- and interobsever reliability of sonographic assessment of the optic nerve sheath diameter in healthy adults. J. Neuroimaging 2012, 22, 42–45. [Google Scholar] [CrossRef]
- Du Toit, G.J.; Hurter, D.; Nel, M. How accurate is ultrasound of the optic nerve sheath diameter performed by inexperienced operators to exclude raised intracranial pressure? S. Afr. J. Radiol. 2015, 19, 1–5. [Google Scholar] [CrossRef]
- Bauerle, J.; Nedelmann, M. Sonographic assessment of the optic nerve sheath in idiopathic intracranial hypertension. J. Neurol. 2011, 258, 2014–2019. [Google Scholar] [CrossRef] [PubMed]
- Kimberly, H.H.; Shah, S.; Marill, K.; Noble, V. Correlation of optic nerve sheath diameter with direct measurement of intracranial pressure. Acad. Emerg. Med. 2008, 15, 201–204. [Google Scholar] [CrossRef]
- Tsung, J.W.; Blaivas, M.; Cooper, A.; Levick, N.R. A rapid noninvasive method of detecting elevated intracranial pressure using bedside ocular ultrasound: Application to 3 cases of head trauma in the pediatric emergency department. Pediatr. Emerg. Care 2005, 21, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Messerer, M.; Berhouma, M.; Messerer, R.; Dubourg, J. Interest of optic nerve sheath diameter ultrasonography in dectecting non-invasively raised intracranial pressure. Neuro-Chirurgie 2013, 59, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koziarz, A.; Nath, S.; Almenawer, S.A. Bedside Optic Nerve Ultrasonography for Diagnosing Increased Intracranial Pressure. Ann. Intern. Med. 2020, 172, 772. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICP 1.0–10.0 mmHg | ICP 10.1–24.2 mmHg | p-Value | |||
|---|---|---|---|---|---|
| (n = 6) | (n = 19) | ||||
| Male (%) | 2 | (33) | 5 | (26) | 0.4 |
| Age (mean ± SD) | 54 | ±24 | 57 | ±17 | 0.8 |
| Body mass index (kg/m2) | 29 | ±6 | 30 | ±8 | 0.9 |
| Mean arterial pressure (mmHg) | 94 | ±15 | 98 | ±18 | 0.6 |
| Heart rate (beats per minute) | 79 | ±4 | 77 | ±14 | 0.5 |
| Peripheral capillary oxygen saturation (%) | 97 | ±2 | 96 | ±2 | 0.2 |
| Diagnosis (%) | |||||
| Hydrocephalus | 2 | (33) | 9 | (47) | 0.1 |
| Normal pressure hydrocephalus | 2 | (33) | 5 | (26) | 1 |
| Shunt dysfunction | 2 | (33) | 4 | (21) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weidner, N.; Kretschmann, J.; Bomberg, H.; Antes, S.; Leonhardt, S.; Tschan, C.; Oertel, J.; Volk, T.; Meiser, A.; Groesdonk, H.V. Real-Time Evaluation of Optic Nerve Sheath Diameter (ONSD) in Awake, Spontaneously Breathing Patients. J. Clin. Med. 2021, 10, 3549. https://doi.org/10.3390/jcm10163549
Weidner N, Kretschmann J, Bomberg H, Antes S, Leonhardt S, Tschan C, Oertel J, Volk T, Meiser A, Groesdonk HV. Real-Time Evaluation of Optic Nerve Sheath Diameter (ONSD) in Awake, Spontaneously Breathing Patients. Journal of Clinical Medicine. 2021; 10(16):3549. https://doi.org/10.3390/jcm10163549
Chicago/Turabian StyleWeidner, Nick, Jessica Kretschmann, Hagen Bomberg, Sebastian Antes, Steffen Leonhardt, Christoph Tschan, Joachim Oertel, Thomas Volk, Andreas Meiser, and Heinrich V. Groesdonk. 2021. "Real-Time Evaluation of Optic Nerve Sheath Diameter (ONSD) in Awake, Spontaneously Breathing Patients" Journal of Clinical Medicine 10, no. 16: 3549. https://doi.org/10.3390/jcm10163549