A New Modified Experimental Meibomian Gland Injury Model: Partial Loss of Gland Due to Orifice Cauterization and the Alleviating Potential of 22-Oxacalcitriol



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Establishment of an Experimental Meibomian Gland Injury Model and the Treatment with Maxacalcitol Ointment or Vaseline®
2.3. Whole-Mount Tissue Meibography and Analyses
2.4. Histochemical Examination and Immunofluorescent Staining
2.5. Statistical Analysis
3. Results
3.1. Identification of the Glandular Loss (Dropout) Following Meibomian Gland Orifice Cauterization
3.2. Effect of Maxacalcitol on the Recovery of Injured Meibomian Gland
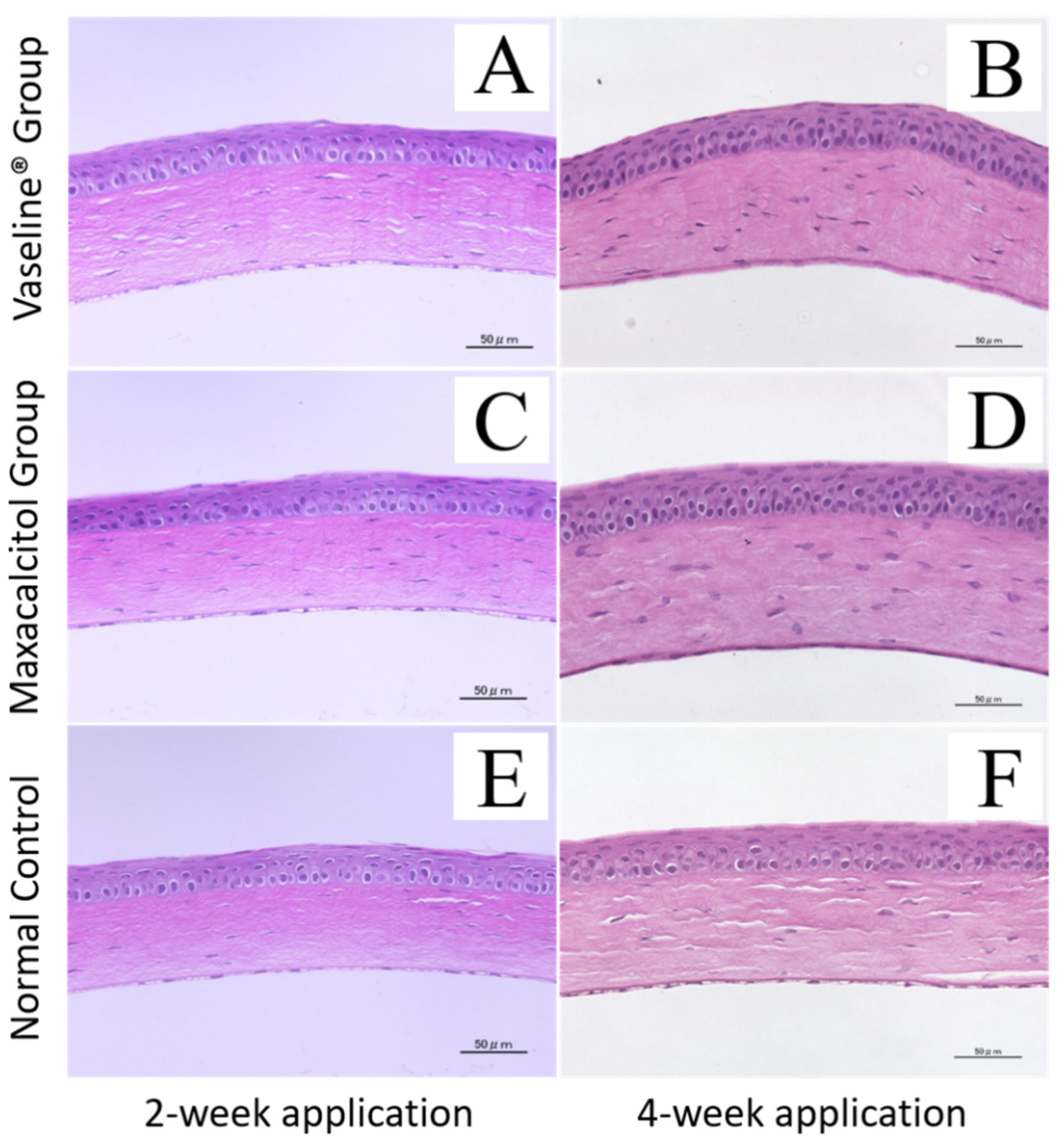
3.3. Adverse Effects on the Cornea and Other Ocular Tissues
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lemp, M.A.; Foulks, G.N. The definition and classification of dry eye disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop. Ocul. SuFrf. 2007, 5, 75–92. [Google Scholar]
- Knop, E.; Knop, N.; Millar, T.; Obata, H.; Sullivan, D.A. The International Workshop on Meibomian Gland Dysfunction: Report of the Subcommittee on Anatomy, Physiology, and Pathophysiology of the Meibomian Gland. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1938–1978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Y.; Gao, Z.; Feng, K.; Qu, H.; Hong, J. Meibomian gland dropout in patients with dry eye disease in China. Curr. Eye Res. 2014, 39, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, C.; Messmer, E.M.; Aragona, P.; Geerling, G.; Akova, Y.A.; Benítez-Del-Castillo, J.; Boboridis, K.G.; Merayo-Lloves, J.; Rolando, M.; Labetoulle, M. Revisiting the vicious circle of dry eye disease: A focus on the pathophysiology of meibomian gland dysfunction. Br. J. Ophthalmol. 2016, 100, 300–306. [Google Scholar] [CrossRef]
- Jester, J.V.; Parfitt, G.J.; Brown, D.J. Meibomian gland dysfunction: Hyperkeratinization or atrophy? BMC Ophthalmol. 2015, 15, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obata, H. Anatomy and histopathology of human meibomian gland. Cornea 2002, 21, S70–S74. [Google Scholar] [CrossRef]
- Arita, R.; Itoh, K.; Inoue, K.; Amano, S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmolgy 2008, 115, 911–915. [Google Scholar] [CrossRef]
- Menzies, K.L.; Srinivasan, S.; Prokopich, C.L.; Jones, L. Infrared imaging of meibomian glands and evaluation of the lipid layer in Sjögren’s syndrome patients and non-dry eye control. Investig. Ophthalmol. Vis. Sci. 2015, 56, 836–841. [Google Scholar] [CrossRef] [Green Version]
- Machalińska, A.; Zakrzewska, A.; Markowska, A.; Safranow, K.; Wiszniewska, B.; Parafiniuk, M.; Machalinski, B. Morphological and Functional Evaluation of Meibomian Gland Dysfunction in Rosacea Patients. Curr. Eye Res. 2015, 7, 1–6. [Google Scholar] [CrossRef]
- Sutu, C.; Fukuoka, H.; Afshari, N.A. Mechanisms and management of dry eye in cataract surgery patients. Curr. Opin. Ophthalmol. 2016, 27, 24–30. [Google Scholar] [CrossRef]
- Engel, L.A.; Wittig, S.; Bock, F.; Sauerbier, L.; Scheid, C.; Holtick, U.; Chemnitz, J.-M.; Hallek, M.; Cursiefen, C.; Steven, P. Meibography and meibomian gland measurements in ocular graft-versus-host disease. Bone Marrow Transplant. 2015, 50, 961–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.B.; Kim, J.J.; Hyon, J.Y.; Wee, W.R.; Shin, Y.J. Eyelid Tattooing Induces Meibomian Gland Loss and Tear Film Instability. Cornea 2015, 34, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Geerling, G.; Tauber, J.; Baudouin, C.; Goto, E.; Matsumoto, Y.; O’Brien, T.; Rolando, M.; Tsubota, K.; Nichols, K.K. The international workshop on meibomian gland dysfunction: Report of the subcommittee on management and treatment of meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2050–2064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vegunta, S.; Patel, D.; Shen, J.F. Combination Therapy of Intense Pulsed Light Therapy and Meibomian Gland Expression (IPL/MGX) Can Improve Dry Eye Symptoms and Meibomian Gland Function in Patients With Refractory Dry Eye: A Retrospective Analysis. Cornea 2016, 35, 318–322. [Google Scholar] [CrossRef]
- Maskin, S.L. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea 2010, 29, 1145–1152. [Google Scholar] [CrossRef]
- Nakayama, N.; Kawashima, M.; Kaido, M.; Arita, R.; Tsubota, K. Analysis of Meibum Before and After Intraductal Meibomian Gland Probing in Eyes With Obstructive Meibomian Gland Dysfunction. Cornea 2015, 34, 1206–1208. [Google Scholar] [CrossRef]
- Ding, N.; Yu, R.T.; Subramaniam, N.; Sherman, M.H.; Wilson, C.; Rao, R.; Leblanc, M.; Coulter, S.; He, M.; Scott, C.; et al. A vitamin D receptor/SMAD genomic circuit gates hepatic fibrotic response. Cell 2013, 153, 601–613. [Google Scholar] [CrossRef] [Green Version]
- Sherman, M.H.; Yu, R.T.; Engle, D.D.; Ding, N.; Atkins, A.R.; Tiriac, H.; Collisson, E.A.; Connor, F.; Van Dyke, T.; Kozlov, S.; et al. Vitamin D receptor-mediated stromal reprogramming suppresses pancreatitis and enhances pancreatic cancer therapy. Cell 2014, 159, 80–93. [Google Scholar] [CrossRef] [Green Version]
- Reins, R.Y.; McDermott, A.M. Vitamin D: Implications for ocular disease and therapeutic potential. Exp. Eye. Res. 2015, 134, 101–110. [Google Scholar] [CrossRef] [Green Version]
- AlSalem, J.A.; Patel, D.; Susarla, R.; Coca-Prados, M.; Bland, R.; Walker, E.A.; Rauz, S.; Wallace, G.R. Characterization of vitamin D production by human ocular barrier cells. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2140–2147. [Google Scholar] [CrossRef] [Green Version]
- Schrader, S.; Mircheff, A.K.; Geerling, G. Animal models of dry eye. Dev. Ophthalmol. 2008, 41, 298–312. [Google Scholar] [PubMed]
- Nelson, J.D.; Shimazaki, J.; Benitez-Del-Castillo, J.M.; Craig, J.P.; McCulley, J.P.; Den, S.; Foulks, G.N. The International Workshop on Meibomian Gland Dysfunction: Report of the Definition and Classification Subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1930–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Le, Q.; Zhao, F.; Hong, J.; Xu, J.; Zheng, T.; Sun, X. Application of in vivo laser scanning confocal microscopy for evaluation of ocular surface diseases: Lessons learned from pterygium, meibomian gland disease, and chemical burns. Cornea 2011, 30, S25–S28. [Google Scholar] [CrossRef] [PubMed]
- Gilbard, J.P.; Rossi, S.R.; Heyda, K.G. Tear film and ocular surface changes after closure of the meibomian gland orifices in the rabbit. Ophthalmology 1989, 96, 1180–1186. [Google Scholar] [CrossRef]
- Nichols, K.K.; Hanlon, S.D.; Nichols, J.J. A murine model for characterizing glandular changes in obstructive meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2014, 55, 14. [Google Scholar]
- Milani, C.; Katayama, M.L.H.; De Lyra, E.C.; Welsh, J.; Campos, L.T.; Brentani, M.M.; Maciel, M.D.S.; Roela, R.A.; Del Valle, P.R.; Goes, J.C.S.; et al. Transcriptional effects of 1,25-Dihydroxyvitamin D3 physiological and supra-physiological concentrations in breast cancer organotypic culture. BMC Cancer 2013, 13, 119. [Google Scholar] [CrossRef]
- Rinkevich, Y.; Walmsley, G.G.; Hu, M.S.; Naan, Z.; Newman, A.M.; Drukker, M.; Januszyk, M.; Krapitz, G.W.; Gutner, G.C.; Lorenz, H.P.; et al. Skin fibrosis. Identification and isolation of a dermal lineage with intrinsic fibrogenic potential. Science 2015, 17, 348. [Google Scholar]
- Suzuki, T.; Sano, Y.; Kinoshita, S. Effects of 1alpha, 25-dihydroxyvitamin D3 on Langerhans cell migration and corneal neovascularization in mice. Investig. Ophthalmol Vis. Sci. 2000, 41, 154–158. [Google Scholar]
- Haussler, M.R.; Jurutka, P.W.; Mizwicki, M.; Norman, A.W. Vitamin D receptor (VDR)-mediated actions of 1α,25-(OH)2-vitamin D3: Genomic and non-genomic mechanisms. Best Pr. Res. Clin. Endocrinol. Metab. 2011, 25, 543–559. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, K.; Kawashima, M.; Ito, M.; Arita, R.; Sano, K.; Tsubota, K. A New Modified Experimental Meibomian Gland Injury Model: Partial Loss of Gland Due to Orifice Cauterization and the Alleviating Potential of 22-Oxacalcitriol. J. Clin. Med. 2021, 10, 6. https://doi.org/10.3390/jcm10010006
Jin K, Kawashima M, Ito M, Arita R, Sano K, Tsubota K. A New Modified Experimental Meibomian Gland Injury Model: Partial Loss of Gland Due to Orifice Cauterization and the Alleviating Potential of 22-Oxacalcitriol. Journal of Clinical Medicine. 2021; 10(1):6. https://doi.org/10.3390/jcm10010006
Chicago/Turabian StyleJin, Kai, Motoko Kawashima, Masataka Ito, Reiko Arita, Kokoro Sano, and Kazuo Tsubota. 2021. "A New Modified Experimental Meibomian Gland Injury Model: Partial Loss of Gland Due to Orifice Cauterization and the Alleviating Potential of 22-Oxacalcitriol" Journal of Clinical Medicine 10, no. 1: 6. https://doi.org/10.3390/jcm10010006