
Mode of Death after Extracorporeal Cardiopulmonary Resuscitation

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Setting
2.2. Local ECPR Algorithm
2.3. ECMO Cannulation and Maintenance
2.4. Coronary Angiography after ECPR
2.5. Neuroprognostication
2.6. Definition of Refractory Shock during VA-ECMO
2.7. Data Collection
2.8. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Permissions Information
Abbreviations
| CPR | cardiopulmonary resuscitation |
| CT | computed tomography |
| ECLS | extracorporeal life support |
| ECPR | extracorporeal cardiopulmonary resuscitation |
| ELSO | extracorporeal life support organization |
| IHCA | intra-hospital cardiac arrest |
| OHCA | out-of-hospital cardiac arrest |
| ROSC | return of spontaneous circulation |
| SAVE | survival after veno-arterial ECMO score |
| SCPC | Sorin centrifugal pump console |
| SIRS | systemic inflammatory response syndrome |
| SPSS | statistical analysis software |
| VA-ECMO | veno-arterial extracorporeal membrane oxygenation |
References
- Yan, S.; Gan, Y.; Jiang, N.; Wang, R.; Chen, Y.; Luo, Z.; Zong, Q.; Chen, S.; Lv, C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: A systematic review and meta-analysis. Crit. Care 2020, 24, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bougouin, W.; Cariou, A. Mode of death after cardiac arrest: We need to know. Resuscitation 2019, 138, 282–283. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K.; Sandroni, C. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015. Resuscitation 2015, 95, 202–222. [Google Scholar] [CrossRef]
- Bougouin, W.; Lamhaut, L.; Marijon, E.; Jost, D.; Dumas, F.; Deye, N.; Beganton, F.; Empana, J.-P.; Chazelle, E.; Cariou, A.; et al. Characteristics and prognosis of sudden cardiac death in Greater Paris. Intensiv. Care Med. 2014, 40, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C.; Booth, S.; Ji, C.; Brace-McDonnell, S.J.; Whittington, A.; Mapstone, J.; Cooke, M.W.; Deakin, C.D.; Gale, C.P.; Fothergill, R.; et al. Epidemiology and outcomes from out-of-hospital cardiac arrests in England. Resuscitation 2017, 110, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Witten, L.; Gardner, R.; Holmberg, M.J.; Wiberg, S.; Moskowitz, A.; Mehta, S.; Grossestreuer, A.V.; Yankama, T.; Donnino, M.W.; Berg, K.M. Reasons for death in patients successfully resuscitated from out-of-hospital and in-hospital cardiac arrest. Resuscitation 2019, 136, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Nadkarni, V.; Bahr, J.; Berg, R.A.; Billi, J.E.; Bossaert, L.; Cassan, P.; Coovadia, A.; D’Este, K.; Finn, J.; et al. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports. Circulation 2004, 110, 3385–3397. [Google Scholar] [CrossRef] [PubMed]
- Kovács, E.; Pilecky, D.; Szakál-Tóth, Z.; Fekete-Győr, A.; Gyarmathy, V.; Gellér, L.; Hauser, B.; Gál, J.; Merkely, B.; Zima, E. The role of age in post-cardiac arrest therapy in an elderly patient population. Physiol. Int. 2020, 107, 319–336. [Google Scholar] [CrossRef] [PubMed]
- Busch, H.-J.; Schmid, B.; Kron, J.; Fink, K.; Busche, C.; Danner, T.; Veits, O.; Gottlieb, D.; Benk, C.; Trummer, G.; et al. Freiburger Cardiac Arrest Receiving Team (CART). Med. Klin. Intensiv. Notf. 2019, 115, 292–299. [Google Scholar] [CrossRef]
- Staudacher, D.L.; Gold, W.; Biever, P.M.; Bode, C.; Wengenmayer, T. Early fluid resuscitation and volume therapy in venoarterial extracorporeal membrane oxygenation. J. Crit. Care 2017, 37, 130–135. [Google Scholar] [CrossRef]
- Wengenmayer, T.; Schroth, F.; Biever, P.M.; Duerschmied, D.; Benk, C.; Trummer, G.; Kaier, K.; Bode, C.; Staudacher, D.L. Albumin fluid resuscitation in patients on venoarterial extracorporeal membrane oxygenation (VA-ECMO) therapy is associated with improved survival. Intensiv. Care Med. 2018, 44, 2312–2314. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Hear. J. 2018, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Stammet, P.; Target Temperature Management after Out-of-Hospital Cardiac Arrest (TTM) trial investigators; Dankiewicz, J.; Nielsen, N.; Fays, F.; Collignon, O.; Hassager, C.; Wanscher, M.; Undèn, J.; Wetterslev, J.; et al. Protein S100 as outcome predictor after out-of-hospital cardiac arrest and targeted temperature management at 33 °C and 36 °C. Crit. Care 2017, 21, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Extracorporeal Life Support Organization. ELSO International Summary. 2020. Available online: https://www.elso.org/Registry/Statistics/InternationalSummary.aspx (accessed on 13 March 2021).
- Patricio, D.; Peluso, L.; Brasseur, A.; Lheureux, O.; Belliato, M.; Vincent, J.-L.; Creteur, J.; Taccone, F.S. Comparison of extracorporeal and conventional cardiopulmonary resuscitation: A retrospective propensity score matched study. Crit. Care 2019, 23, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zavalichi, M.A.; Nistor, I.; Nedelcu, A.-E.; Zavalichi, S.D.; Georgescu, C.M.A.; Stătescu, C.; Covic, A. Extracorporeal Membrane Oxygenation in Cardiogenic Shock due to Acute Myocardial Infarction: A Systematic Review. BioMed Res. Int. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bréchot, N.; Hajage, D.; Kimmoun, A.; Demiselle, J.; Agerstrand, C.; Montero, S.; Schmidt, M.; Luyt, C.-E.; Lebreton, G.; Hékimian, G.; et al. Venoarterial extracorporeal membrane oxygenation to rescue sepsis-induced cardiogenic shock: A retrospective, multicentre, international cohort study. Lancet 2020, 396, 545–552. [Google Scholar] [CrossRef]
- Pasrija, C.; Kronfli, A.; George, P.; Raithel, M.; Boulos, F.; Herr, D.L.; Gammie, J.S.; Pham, S.M.; Griffith, B.P.; Kon, Z.N. Utilization of Veno-Arterial Extracorporeal Membrane Oxygenation for Massive Pulmonary Embolism. Ann. Thorac. Surg. 2018, 105, 498–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falk, L.; Hultman, J.; Broman, L.M. Extracorporeal Membrane Oxygenation for Septic Shock. Crit. Care Med. 2019, 47, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Zotzmann, V.; Rilinger, J.; Lang, C.N.; Kaier, K.; Benk, C.; Duerschmied, D.; Biever, P.M.; Bode, C.; Wengenmayer, T.; Staudacher, D.L. Epinephrine, inodilator, or no inotrope in venoarterial extracorporeal membrane oxygenation implantation: A single-center experience. Crit. Care 2019, 23, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonizzoli, M.; Lazzeri, C.; Cianchi, G.; Boddi, M.; Cozzolino, M.; Di Valvasone, S.; Terenzi, P.; Batacchi, S.; Chiostri, M.; Peris, A. Serial Lactate Measurements as a Prognostic Tool in Venovenous Extracorporeal Membrane Oxygenation Support. Ann. Thorac. Surg. 2017, 103, 812–818. [Google Scholar] [CrossRef] [Green Version]
- Vinclair, C.; De Montmollin, E.; Sonneville, R.; Reuter, J.; Lebut, J.; Cally, R.; Mourvillier, B.; Neuville, M.; Ruckly, S.; Timsit, J.-F.; et al. Factors associated with major adverse kidney events in patients who underwent veno-arterial extracorporeal membrane oxygenation. Ann. Intensiv. Care 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilburn, D.J.; Shekar, K.; Fraser, J.F. The Complex Relationship of Extracorporeal Membrane Oxygenation and Acute Kidney Injury: Causation or Association? BioMed Res. Int. 2016, 2016, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrage, B.; Rübsamen, N.; Becher, P.M.; Roedl, K.; Söffker, G.; Schwarzl, M.; Dreher, A.; Schewel, J.; Ghanem, A.; Grahn, H.; et al. Neuron-specific-enolase as a predictor of the neurologic outcome after cardiopulmonary resuscitation in patients on ECMO. Resuscitation 2019, 136, 14–20. [Google Scholar] [CrossRef]
- Geocadin, R.G.; Callaway, C.W.; Fink, E.L.; Golan, E.; Greer, D.M.; Ko, N.U.; Lang, E.; Licht, D.J.; Marino, B.S.; McNair, N.D.; et al. Standards for Studies of Neurological Prognostication in Comatose Survivors of Cardiac Arrest: A Scientific Statement from the American Heart Association. Circulation 2019, 140, e517–e542. [Google Scholar] [CrossRef] [PubMed]
- Bossaert, L.L.; Perkins, G.D.; Askitopoulou, H.; Raffay, V.I.; Greif, R.; Haywood, K.L.; Mentzelopoulos, S.D.; Nolan, J.P.; Van de Voorde, P.; Xanthos, T.T.; et al. European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation 2015, 95, 302–311. [Google Scholar] [CrossRef] [Green Version]
- Welbourn, C.; Efstathiou, N. How does the length of cardiopulmonary resuscitation affect brain damage in patients surviving cardiac arrest? A systematic review. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 77. [Google Scholar] [CrossRef] [PubMed]
- Zotzmann, V.; Rilinger, J.; Lang, C.N.; Duerschmied, D.; Benk, C.; Bode, C.; Wengenmayer, T.; Staudacher, D.L. Early full-body computed tomography in patients after extracorporeal cardiopulmonary resuscitation (eCPR). Resuscitation 2020, 146, 149–154. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
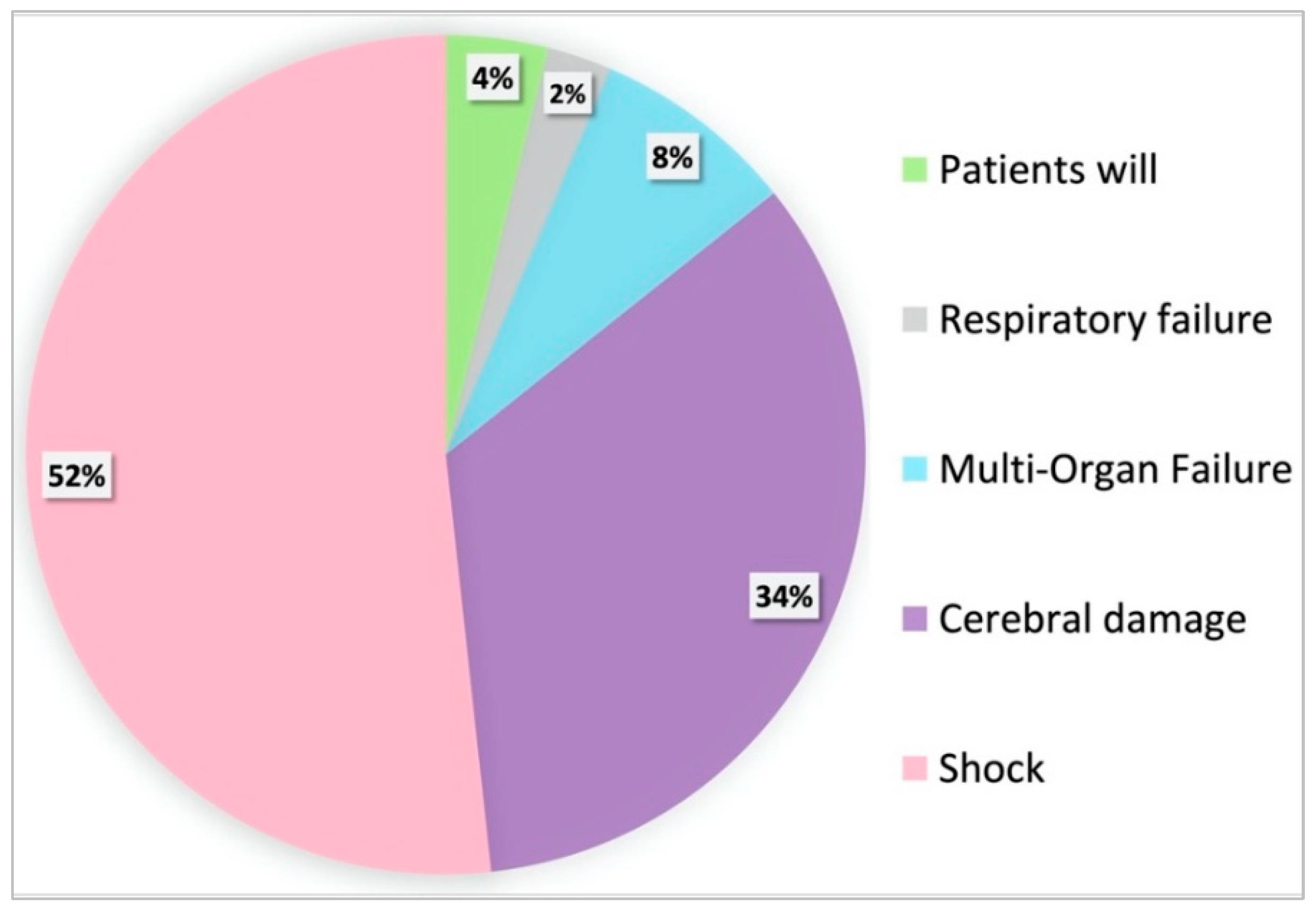
| Reasons for Death Following ECPR in Five Categories | |
|---|---|
| Neurological Withdrawal | Withdrawal of care based on expectations of a poor neurological recovery. If an assessment off sedation is not done, e.g., in the early hours during targeted temperature management (TTM), there must be other evidence of severe neurologic injury (e.g., severe cerebral edema or herniation). |
| Persisting Cardiogenic/Post-Resuscitation Shock | Withdrawal from therapy in either progressive, refractory hemodynamic shock due to refractory vasoplegia in post-resuscitation shock, with inadequate VA-ECMO despite aggressive catecholamine therapy and volume substitution. Or, Withdrawal in case of lack of hemodynamic stabilization with persisting dependency of a cardiac support system (VA-ECMO or Impella®) without the possibility of definitive care using an LV-assist device (LVAD) or heart transplantation. |
| Multi-Organ Failure | Withdrawal of therapy due to a multi-organ failure (for example in the context of an uncontrollable septic shock) or persistent liver failure. |
| Respiratory Failure | Withdrawal of care based on respiratory failure. Respiratory failure with hypoxemia, hypercapnia or a combination of these despite maximum support with respirator plus VA-ECMO or even VVA-ECMO. |
| Presumed Patients Will | This category includes the withdrawal if the patient’s presumed will was against resuscitation. Or, Withdrawal of therapy and termination of intensive care treatment due to an expected poor quality of life (e.g., in context of previously existing serious illness such as dementia or an advanced cancer disease). |
| Parameter | (1) Whole Cohort | (2) Survivor | (3) Non-Survivor | p-Value (2) vs. (3) |
|---|---|---|---|---|
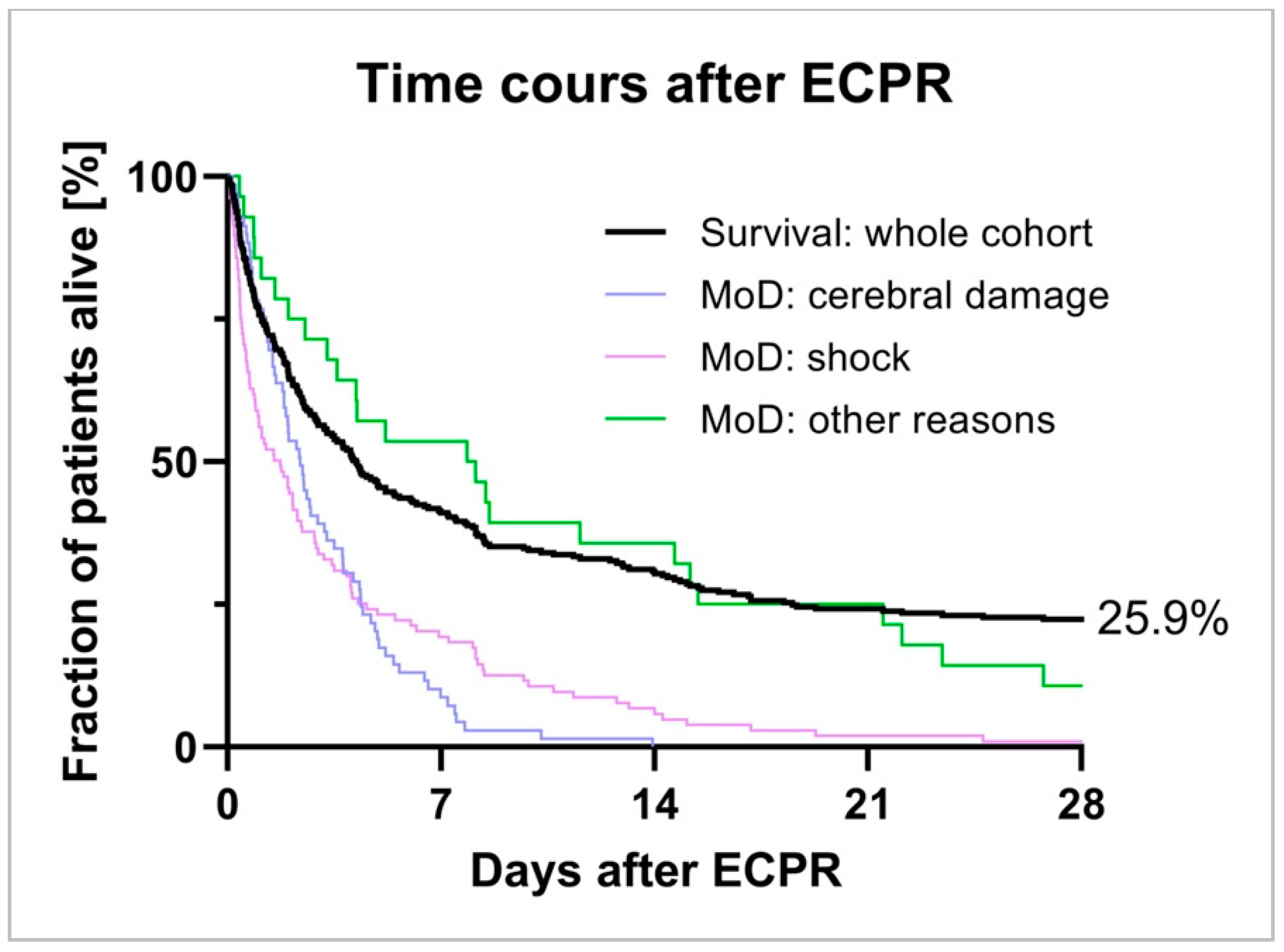
| Number of Patients | 274 (100%) | 71 (25.9%) | 203 (74.1%) | |
| Mean Age [years] | 60.0 ± 14.3 | 59.8 ± 14.6 | 60.0 ± 14.2 | 0.9085 |
| Female Gender | 73 (26.6%) | 22 (32.0%) | 50 (24.6%) | 0.2720 |
| Low-Flow Time [min] | 53.8 ± 28.9 | 46.0 ± 27.9 | 56.6 ± 28.8 | 0.0086 |
| Shockable Initial Rhythm | 129 (47.1%) | 42 (59.2%) | 87 (42.8%) | 0.0162 |
| SAPS 2 | 70.7 ± 7.4 | 70.0 ± 8.0 | 71.0 ± 7.2 | 0.3187 |
| SOFA | 11.7 ± 2.3 | 11.6 ± 2.4 | 11.8 ± 2.2 | 0.5266 |
| SAVE | −0.47 ± 4.5 | 0.35 ± 4.8 | −0.76 ± 4.4 | 0.0743 |
| PREDICT Score 6h [%] | 32 ± 22 | 42 ± 17 | 29 ± 23 | <0.0001 |
| Out-of-Hospital Cardiac Arrest | 127 (46.4%) | 35 (49.3%) | 92 (45.3%) | 0.5631 |
| Initial Lactate Level [mmol/L] | 10.6 ± 7.8 | 7.9 ± 4.5 | 11.6 ± 8.4 | 0.0005 |
| Comorbidities: | ||||
| Arterial Hypertension | 104 (38.0%) | 30 (42.5%) | 74 (36.4%) | 0.3860 |
| Chronic Kidney Disease | 48 (17.5%) | 12 (16.9%) | 36 (17.7%) | 0.8738 |
| Chronic Liver Disease | 16 (5.8%) | 6 (8.5%) | 10 (4.9%) | 0.2756 |
| Chronic Lung Disease | 38 (13.9%) | 10 (14.1%) | 28 (13.8%) | 0.9512 |
| Coronary Artery Disease | 152 (55.5%) | 41 (57.8%) | 111 (54.7%) | 0.6545 |
| Diabetes Mellitus | 61 (22.3%) | 16 (22.5%) | 45 (22.2%) | 0.9489 |
| Hypercholesterinemia | 52 (19.0%) | 15 (21.1%) | 37 (20.3%) | 0.5917 |
| Nicotine | 68 (24.8%) | 25 (35.2%) | 43 (23.6%) | 0.0185 |
| Peripheral Artery Disease | 17 (6.2%) | 7 (9.9%) | 10 (4.9%) | 0.1380 |
| Positive Cardiovascular Family History | 25 (9.1%) | 6 (8.5%) | 19 (10.4%) | 0.8189 |
| Parameter | (1) Whole Cohort | (2) Survivor | (3) Non-Survivor | p-Value (2) vs. (3) |
|---|---|---|---|---|
| Hospital Survival | 71 (25.9%) | 71 (100%) | 0 (0%) | <0.0001 |
| Lenght of ICU Stay [days] | 9.0 ± 13.9 | 19.8 ± 16.5 | 5.2 ± 10.6 | <0.0001 |
| TTM 33 °C | 208 (75.9%) | 46 (64.8%) | 152 (74.9%) | 0.7531 |
| NSE-Day 1 | 96.1 ± 101.4 | 68.6 ± 48.3 | 109.3 ± 115.6 | 0.0158 |
| NSE-Day 2 | 116.5 ± 98.7 | 74.5 ± 47.7 | 147.3 ± 114.2 | <0.0001 |
| NSE-Day 3 | 136.9 ± 150.2 | 73.9 ± 76.2 | 184.5 ± 1773.8 | 0.0005 |
| Respiratory Support [h] | 124.7 ± 140.9 | 228.4 ± 177.7 | 88.5 ± 104.0 | <0.0001 |
| Renal Replacement Therapy | 59 (21.3%) | 14 (19.7%) | 45 (22.2%) | 0.6565 |
| (1) Survivors | (2) Cerebral Damage | (3) Shock | p-Value 1 vs. 2 vs. 3 | p-Value 2 vs. 3 | |
|---|---|---|---|---|---|
| Patients in Group | 71 (25.9%) | 69 (25.2%) | 105 (38.3%) | ||
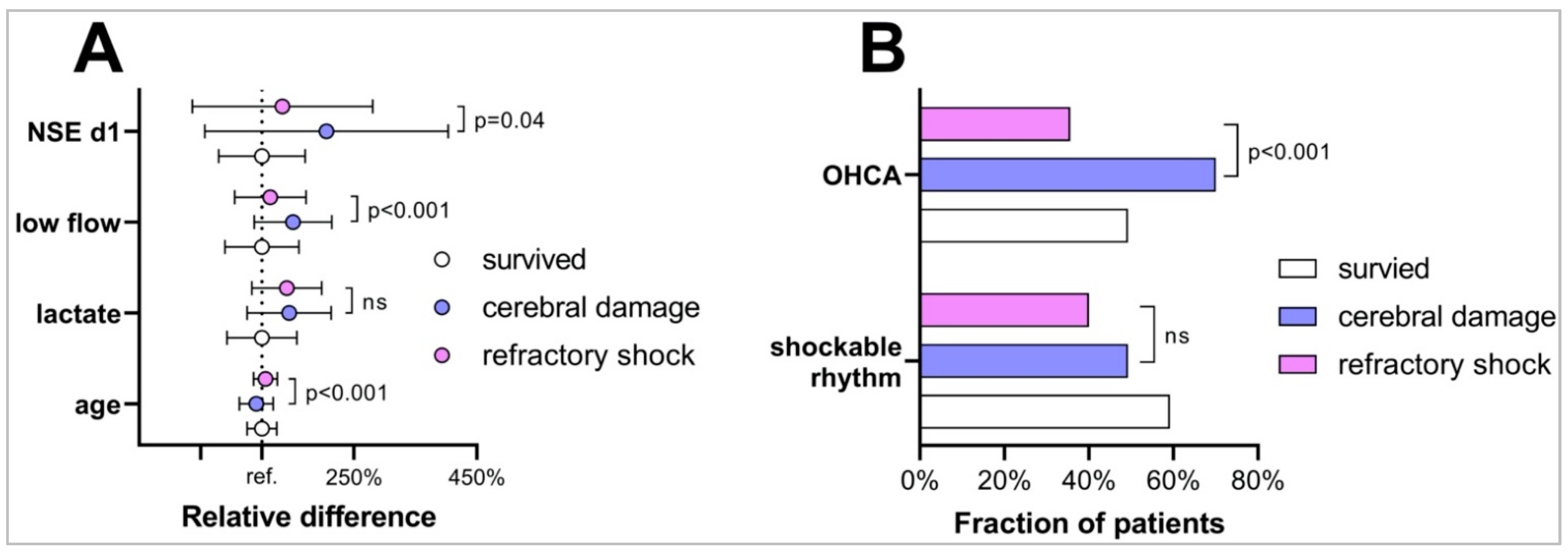
| Age | 59.8 ± 14.5 | 54.3 ± 16.5 | 63.2 ± 11.5 | 0.0003 | <0.0001 |
| Female Gender | 23 (32.4%) | 16 (23.2%) | 26 (24.8%) | 0.4033 | 0.8124 |
| OHCA | 35 (49.3%) | 47 (70.1%) | 37 (35.6%) | <0.0001 | <0.0001 |
| Shockable Rhythm | 42 (59.2%) | 34 (49.3%) | 42 (40.0%) | 0.0434 | 0.2275 |
| First Lactate | 7.9 ± 4.5 | 11.4 ± 5.4 | 11.1 ± 4.5 | <0.0001 | 0.6899 |
| Low-Flow Duration | 46.0 ± 27.7 | 69.3 ± 29.1 | 52.3 ± 26.8 | <0.0001 | 0.0001 |
| NSE D 1 | 68.6 ± 48.3 | 140.7 ± 136.0 | 91.5 ± 100.9 | 0.0015 | 0.0446 |
| S100 D 1 | 0.7 ± 1.9 | 5.4 ± 4.7 | 2.6 ± 3.7 | <0.0001 | 0.0160 |
| SAPS2 Score | 70.0 ± 8.0 | 69.9 ± 7.9 | 71.3 ± 6.8 | 0.3478 | 0.2010 |
| SAVE Score | 0.4 ± 4.8 | 0.4 ± 4.2 | −1.3 ± 4.3 | 0.0111 | 0.0080 |
| SOFA Score | 11.6 ± 2.4 | 11.8 ± 2.1 | 11.6 ± 2.2 | 0.9081 | 0.6955 |
| PREDICT 6h Score | 42 ± 17 | 25 ± 17 | 25 ± 20 | <0.0001 | 0.9528 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zotzmann, V.; Lang, C.N.; Bemtgen, X.; Jäckel, M.; Fluegler, A.; Rilinger, J.; Benk, C.; Bode, C.; Supady, A.; Wengenmayer, T.; et al. Mode of Death after Extracorporeal Cardiopulmonary Resuscitation. Membranes 2021, 11, 270. https://doi.org/10.3390/membranes11040270
Zotzmann V, Lang CN, Bemtgen X, Jäckel M, Fluegler A, Rilinger J, Benk C, Bode C, Supady A, Wengenmayer T, et al. Mode of Death after Extracorporeal Cardiopulmonary Resuscitation. Membranes. 2021; 11(4):270. https://doi.org/10.3390/membranes11040270
Chicago/Turabian StyleZotzmann, Viviane, Corinna N. Lang, Xavier Bemtgen, Markus Jäckel, Annabelle Fluegler, Jonathan Rilinger, Christoph Benk, Christoph Bode, Alexander Supady, Tobias Wengenmayer, and et al. 2021. "Mode of Death after Extracorporeal Cardiopulmonary Resuscitation" Membranes 11, no. 4: 270. https://doi.org/10.3390/membranes11040270