Misperception of Visual Verticality in Patients with Primary Headache Disorders: A Systematic Review with Meta-Analysis

 ,
,  , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Protocol Review
2.2. Data Sources and Search Strategy
2.3. Study Selection and Inclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
2.7. Additional Analysis
2.8. Subgroup Analysis
3. Results
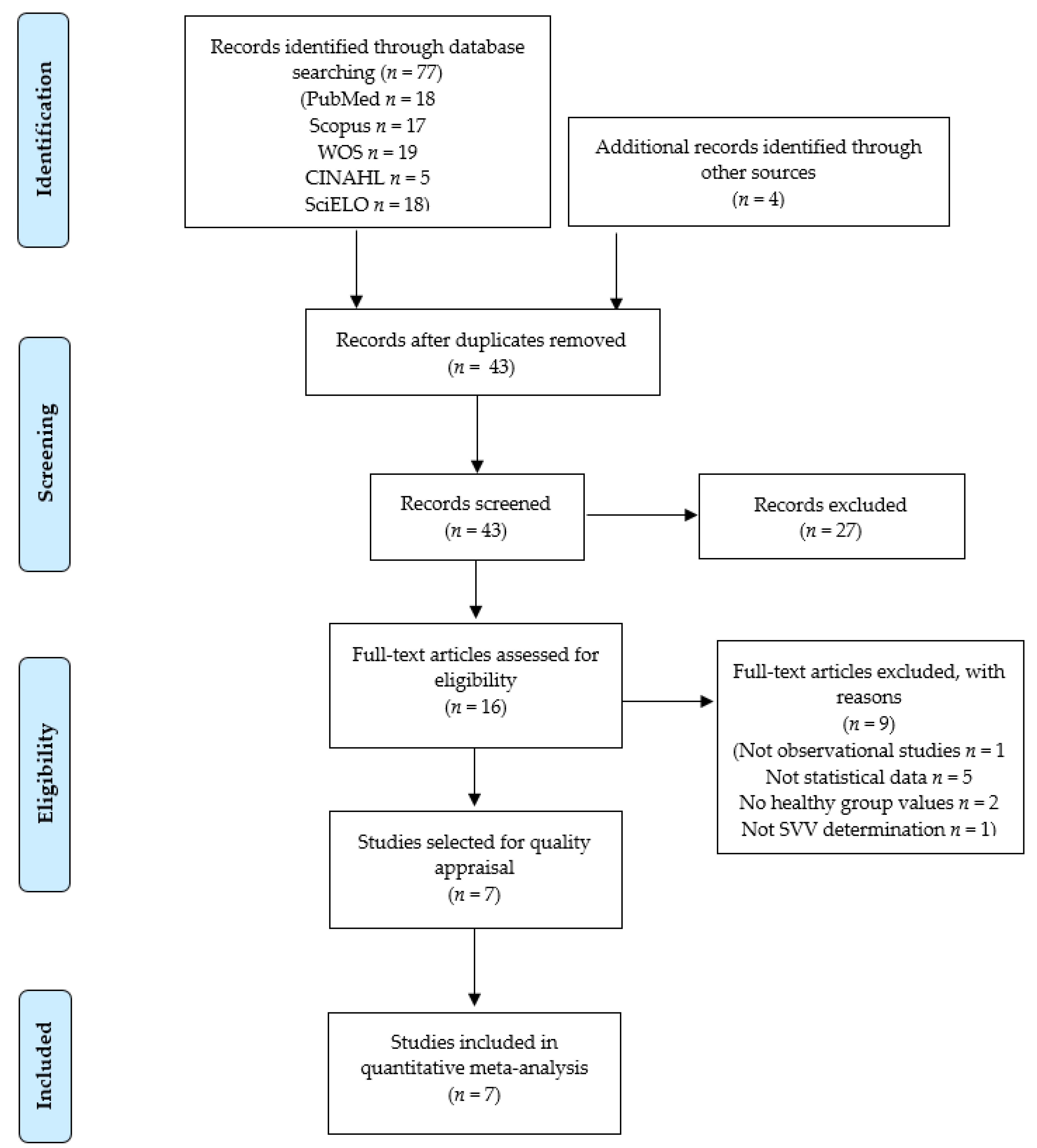
3.1. Study Selection
3.2. Characteristics of the Seven Studies Included in the Meta-Analysis
3.3. Quality Assessment of the Studies Included in the Meta-Analysis
3.4. Results of the Overall Meta-Analysis on Perception of Visual Verticality in Patients with Primary Headache Disorders
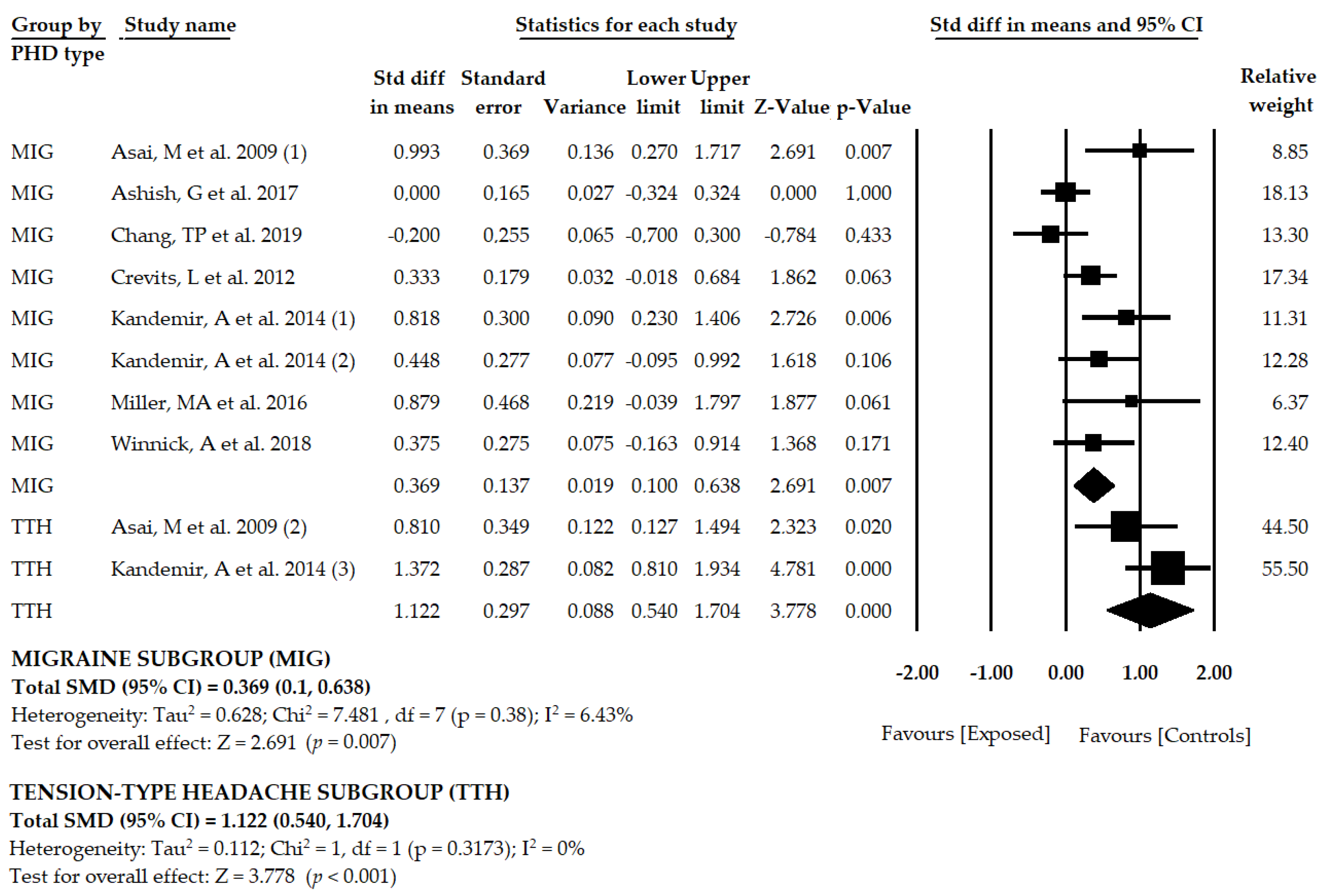
3.5. Results of the Meta-Analysis in Patients with Migraine
3.6. Results of the Meta-Analysis in Patients with Tension-Type Headache
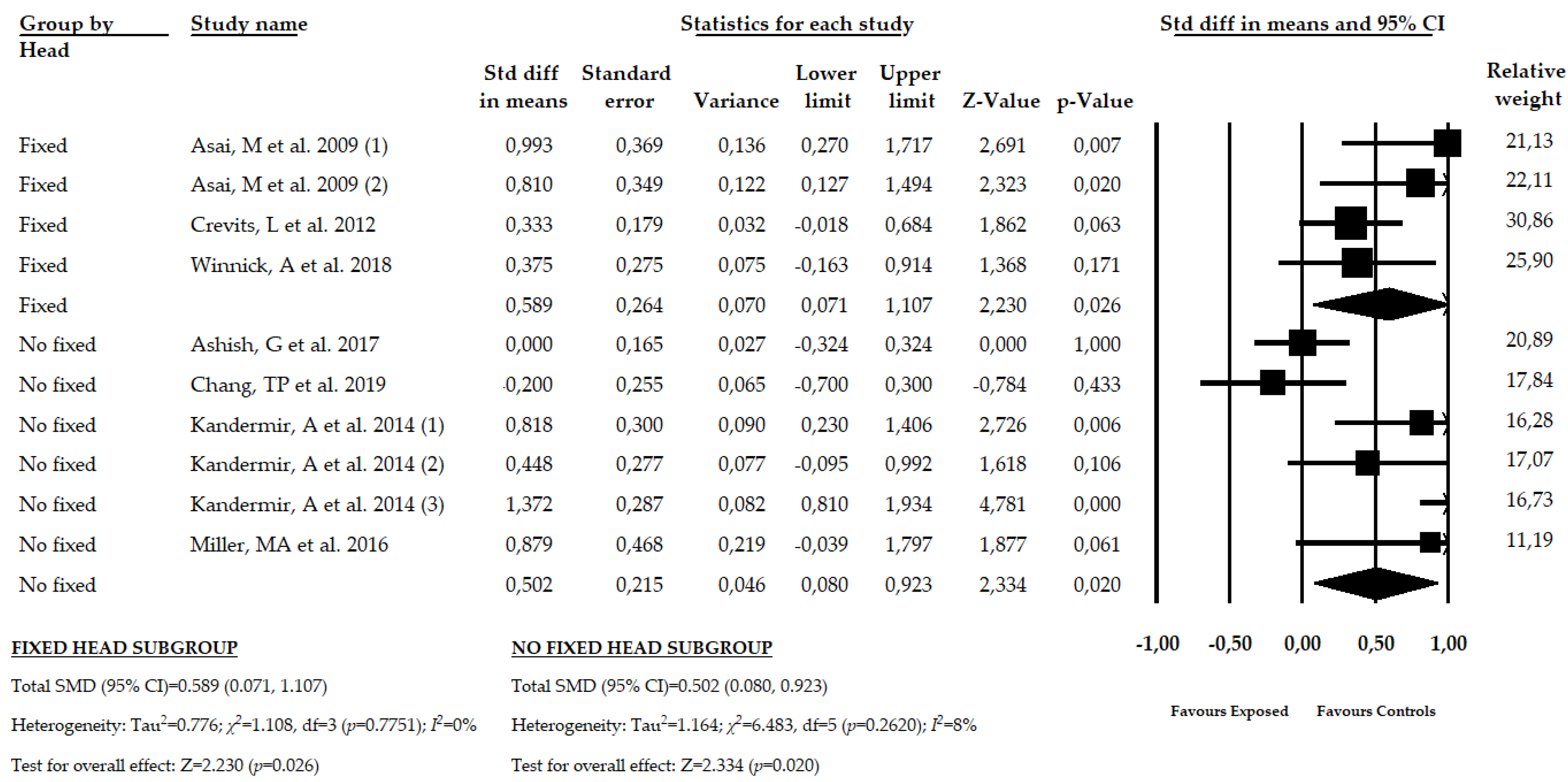
3.7. Results of the Meta-Analysis in Patients with PHD with Fixed and Non-Fixed Head Condition
3.8. Results of the Meta-Analysis in Patients with PHD Using the Bucket Test or the Rod Projected Screen Test
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Stovner, L.J.; Nichols, E.; Steiner, T.J.; Abd-Allah, F.; Abdelalim, A.; Al-Raddadi, R.M.; Ansha, M.G.; Barac, A.; Bensenor, I.M.; Doan, L.P.; et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef] [Green Version]
- Vos, T.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Woldeamanuel, Y.W.; Cowan, R.P. Migraine affects 1 in 10 people worldwide featuring recent rise: A systematic review and meta-analysis of community-based studies involving 6 million participants. J. Neurol. Sci. 2017, 372, 307–315. [Google Scholar] [CrossRef]
- Linde, M.; Gustavsson, A.; Stovner, L.J.; Steiner, T.J.; Barré, J.; Katsarava, Z.; Lainez, J.M.; Lampl, C.; Lantéri-Minet, M.; Rastenyte, D.; et al. The cost of headache disorders in Europe: The Eurolight project. Eur. J. Neurol. 2012, 19, 703–711. [Google Scholar] [CrossRef]
- Ford, S.; Calhoun, A.; Kahn, K.; Mann, J.; Finkel, A. Predictors of Disability in Migraineurs Referred to a Tertiary Clinic: Neck Pain, Headache Characteristics, and Coping Behaviors. Headache J. Head Face Pain 2008, 48, 523–528. [Google Scholar] [CrossRef]
- Blaschek, A.; Milde-Busch, A.; Straube, A.; Schankin, C.; Langhagen, T.; Jahn, K.; Schröder, S.A.; Reiter, K.; Von Kries, R.; Heinen, F. Self-reported muscle pain in adolescents with migraine and tension-type headache. Cephalalgia 2012, 32, 241–249. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, G.F.; Chaves, T.C.; Gonçalves, M.C.; Florencio, L.L.; Braz, C.A.; Dach, F.; De Las Peñas, C.F.; Bevilaqua-Grossi, D. Comparison between neck pain disability and cervical range of motion in patients with episodic and chronic migraine: A cross-sectional study. J. Manipulative Physiol. Ther. 2014, 37, 641–646. [Google Scholar] [CrossRef]
- Ashina, S.; Bendtsen, L.; Lyngberg, A.C.; Lipton, R.B.; Hajiyeva, N.; Jensen, R. Prevalence of neck pain in migraine and tension-type headache: A population study. Cephalalgia 2015, 35, 211–219. [Google Scholar] [CrossRef]
- de Tommaso, M.; Sciruicchio, V. Migraine and Central Sensitization: Clinical Features, Main Comorbidities and Therapeutic Perspectives. Curr. Rheumatol. Rev. 2016, 12, 113–126. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C. Myofascial Head Pain. Curr. Pain Headache Rep. 2015, 19, 1–7. [Google Scholar] [CrossRef]
- Bendtsen, L.; Fernández-De-La-Peñas, C. The role of muscles in tension-type headache. Curr. Pain Headache Rep. 2011, 15, 451–458. [Google Scholar] [CrossRef]
- Schmidt-Hansen, P.T.; Svensson, P.; Jensen, T.S.; Graven-Nielsen, T.; Bach, F.W. Patterns of experimentally induced pain in pericranial muscles. Cephalalgia 2006, 26, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Cachinero-Torre, A.; Díaz-Pulido, B.; Asúnsolo-Del-Barco, Á. Relationship of the Lateral Rectus Muscle, the Supraorbital Nerve, and Binocular Coordination with Episodic Tension-Type Headaches Frequently Associated with Visual Effort. Pain Med. 2017, 18, 969–979. [Google Scholar] [CrossRef]
- Teggi, R.; Manfrin, M.; Balzanelli, C.; Gatti, O.; Mura, F.; Quaglieri, S.; Pilolli, F.; Redaelli de Zinis, L.O.; Benazzo, M.; Bussi, M. Point prevalence of vertigo and dizziness in a sample of 2672 subjects and correlation with headaches. Acta Otorhinolaryngol. Ital. Organo Uff. Della Soc. Ital. Otorinolaringol. Chir. Cerv. Facc. 2016, 36, 215–219. [Google Scholar] [CrossRef]
- Swaminathan, A.; Smith, J.H. Migraine and Vertigo. Curr. Neurol. Neurosci. Rep. 2015, 15, 1–5. [Google Scholar] [CrossRef]
- Bisdorff, A.; Andrée, C.; Vaillant, M.; Sándor, P.S. Headache-associated dizziness in a headache population: Prevalence and impact. Cephalalgia 2010, 30, 815–820. [Google Scholar] [CrossRef]
- Watson, D.H.; Drummond, P.D. The Role of the Trigemino Cervical Complex in Chronic Whiplash Associated Headache: A Cross Sectional Study. Headache J. Head Face Pain 2016, 56, 961–975. [Google Scholar] [CrossRef]
- Marano, E.; Marcelli, V.; Di Stasio, E.; Bonuso, S.; Vacca, G.; Manganelli, F.; Marciano, E.; Perretti, A. Trigeminal Stimulation Elicits a Peripheral Vestibular Imbalance in Migraine Patients. Headache J. Head Face Pain 2005, 45, 325–331. [Google Scholar] [CrossRef]
- Kheradmand, A.; Winnick, A. Perception of Upright: Multisensory Convergence and the Role of Temporo-Parietal Cortex. Front. Neurol. 2017, 8. [Google Scholar] [CrossRef]
- Mazibrada, G.; Tariq, S.; Perennou, D.; Gresty, M.; Greenwood, R.; Bronstein, A.M. The peripheral nervous system and the perception of verticality. Gait Posture 2008, 27, 202–208. [Google Scholar] [CrossRef]
- Selge, C.; Schoeberl, F.; Bergmann, J.; Kreuzpointner, A.; Bardins, S.; Schepermann, A.; Schniepp, R.; Koenig, E.; Mueller, F.; Brandt, T.; et al. Subjective body vertical: A promising diagnostic tool in idiopathic normal pressure hydrocephalus? J. Neurol. 2016, 263, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Min, K.K.; Ha, J.S.; Kim, M.J.; Cho, C.H.; Cha, H.E.; Lee, J.H. Clinical use of subjective visual horizontal and vertical in patients of unilateral vestibular neuritis. Otol. Neurotol. 2007, 28, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Piscicelli, C.; Barra, J.; Davoine, P.; Chrispin, A.; Nadeau, S.; Pérennou, D. Inter- and Intra-Rater Reliability of the Visual Vertical in Subacute Stroke. Stroke 2015, 46, 1979–1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohmer, A.; Mast, F. Assessing otolith function by the subjective visual vertical. Ann. N. Y. Acad. Sci. 1999, 871, 221–231. [Google Scholar] [CrossRef]
- Funabashi, M.; Santos-Pontelli, T.E.G.; Colafêmina, J.F.; Pavan, T.Z.; Carneiro, A.A.O.; Takayanagui, O.M. A New Method to Analyze the Subjective Visual Vertical in Patients With Bilateral Vestibular Dysfunction. Clinics 2012, 67, 1127–1131. [Google Scholar] [CrossRef]
- Zwergal, A.; Rettinger, N.; Frenzel, C.; Dieterich, M.; Brandt, T.; Strupp, M. A bucket of static vestibular function. Neurology 2009, 72, 1689–1692. [Google Scholar] [CrossRef]
- Docherty, S.; Schärer, R.; Bagust, J.; Humphreys, B.K. Perception of subjective visual vertical and horizontal in patients with chronic neck pain: A cross-sectional observational study. Man. Ther. 2012, 17, 133–138. [Google Scholar] [CrossRef]
- Bagust, J.; Docherty, S.; Haynes, W.; Telford, R.; Isableu, B. Changes in rod and frame test scores recorded in schoolchildren during development--A longitudinal study. PLoS ONE 2013, 8, e65321. [Google Scholar] [CrossRef] [Green Version]
- Perennou, D.; Piscicelli, C.; Barbieri, G.; Jaeger, M.; Marquer, A.; Barra, J. Measuring verticality perception after stroke: Why and how? Neurophysiol. Clin. 2014, 44, 25–32. [Google Scholar] [CrossRef]
- Alrwaily, M.; Sparto, P.J.; Whitney, S.L. Perception of verticality is altered in people with severe chronic low back pain compared to healthy controls: A cross-sectional study. Musculoskelet. Sci. Pract. 2020, 45, 102074. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) Group. J. Am. Med. Assoc. 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Intervention Version 5.1.0; Updated March 2011; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 13 May 2020).
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Meader, N.; King, K.; Llewellyn, A.; Norman, G.; Brown, J.; Rodgers, M.; Moe-Byrne, T.; Higgins, J.P.; Sowden, A.; Stewart, G. A checklist designed to aid consistency and reproducibility of GRADE assessments: Development and pilot validation. Syst. Rev. 2014, 3, 82. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Software Version 3. Available online: https://www.meta-analysis.com/ (accessed on 22 September 2020).
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis; Russell Sage Foundation: New York, NY, USA, 2009. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. Pharm. Ther. 2008, 33, 700–711. [Google Scholar]
- Rücker, G.; Schwarzer, G. Beyond the forest plot: The drapery plot. Res. Synth. Methods 2020. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Comparison of two methods to detect publication bias in meta-analysis. JAMA 2006, 295, 676–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Shi, L.; Lin, L.; Omboni, S. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Statistical heterogeneity in systematic reviews of clinical trials: A critical appraisal of guidelines and practice. J. Health Serv. Res. Policy 2002, 7, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Asai, M.; Aoki, M.; Hayashi, H.; Yamada, N.; Mizuta, K.; Ito, Y. Subclinical deviation of the subjective visual vertical in patients affected by a primary headache. Acta Otolaryngol. 2009, 129, 30–35. [Google Scholar] [CrossRef]
- Ashish, G.; Augustine, A.M.; Tyagi, A.K.; Lepcha, A.; Balraj, A. Subjective Visual Vertical and Horizontal in Vestibular Migraine. J. Int. Adv. Otol. 2017, 13, 254–258. [Google Scholar] [CrossRef]
- Chang, T.-P.; Winnick, A.A.; Hsu, Y.-C.; Sung, P.-Y.; Schubert, M.C. The bucket test differentiates patients with MRI confirmed brainstem/cerebellar lesions from patients having migraine and dizziness alone. BMC Neurol. 2019, 19, 219. [Google Scholar] [CrossRef] [Green Version]
- Crevits, L.; Vanacker, L.; Verraes, A. Patients with migraine correctly estimate the visual verticality. Clin. Neurol. Neurosurg. 2012, 114, 313–315. [Google Scholar] [CrossRef]
- Kandemir, A.; Çelebisoy, N.; Köse, T. Perception of verticality in patients with primary headache disorders. J. Int. Adv. Otol. 2014, 10, 138–143. [Google Scholar] [CrossRef]
- Winnick, A.; Sadeghpour, S.; Otero-Millan, J.; Chang, T.-P.; Kheradmand, A. Errors of Upright Perception in Patients With Vestibular Migraine. Front. Neurol. 2018, 9, 892. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.A.; Crane, B.T. Static and dynamic visual vertical perception in subjects with migraine and vestibular migraine. World J. Otorhinolaryngol. Head Neck Surg. 2016, 2, 175–180. [Google Scholar] [CrossRef]
- Rodríguez-Almagro, D.; Achalandabaso-Ochoa, A.; Molina-Ortega, F.J.; Obrero-Gaitán, E.; Ibáñez-Vera, A.J.; Lomas-Vega, R. Neck Pain- and Unsteadiness-Inducing Activities and their Relationship to the Presence, Intensity, Frequency, and Disability of Headaches. Brain Sci. 2020, 10, 425. [Google Scholar] [CrossRef]
- Molina, F.; Lomas-Vega, R.; Obrero-Gaitán, E.; Rus, A.; Almagro, D.R.; Del-Pino-Casado, R. Misperception of the subjective visual vertical in neurological patients with or without stroke: A meta-analysis. NeuroRehabilitation 2019, 44, 379–388. [Google Scholar] [CrossRef]
- Treleaven, J. Dizziness, Unsteadiness, Visual Disturbances, and Sensorimotor Control in Traumatic Neck Pain. J. Orthop. Sports Phys. Ther. 2017, 47, 492–502. [Google Scholar] [CrossRef]
- Kristjansson, E.; Treleaven, J. Sensorimotor function and dizziness in neck pain: Implications for assessment and management. J. Orthop. Sports Phys. Ther. 2009, 39, 364–377. [Google Scholar] [CrossRef] [Green Version]
- Dieterich, M.; Brandt, T. Perception of Verticality and Vestibular Disorders of Balance and Falls. Front. Neurol. 2019, 10, 172. [Google Scholar] [CrossRef] [Green Version]
- Vuralli, D.; Boran, H.E.; Cengiz, B.; Coskun, O.; Bolay, H. Somatosensory temporal discrimination remains intact in tension-type headache whereas it is disrupted in migraine attacks. Cephalalgia 2017, 37, 1241–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.-T.; Hsiao, F.-J.; Ko, Y.-C.; Liu, H.-Y.; Wang, P.-N.; Fuh, J.-L.; Lin, Y.-Y.; Wang, S.-J. Comparison of somatosensory cortex excitability between migraine and “strict-criteria” tension-type headache. Pain 2018, 159, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Obrero-Gaitán, E.; Molina, F.; Del-Pino-Casado, R.; Ibáñez-Vera, A.J.; Rodríguez-Almagro, D.; Lomas-Vega, R. Visual Verticality Perception in Spinal Diseases: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1725. [Google Scholar] [CrossRef] [PubMed]
- Anagnostou, E.; Gerakoulis, S.; Voskou, P.; Kararizou, E. Postural instability during attacks of migraine without aura. Eur. J. Neurol. 2019, 26, 319-e21. [Google Scholar] [CrossRef]
- Buisseret-Delmas, C.; Compoint, C.; Delfini, C.; Buisseret, P. Organisation of reciprocal connections between trigeminal and vestibular nuclei in the rat. J. Comp. Neurol. 1999, 409, 153–168. [Google Scholar] [CrossRef]
- Lampl, C.; Rapoport, A.; Levin, M.; Bräutigam, E. Migraine and episodic Vertigo: A cohort survey study of their relationship. J. Headache Pain 2019, 20, 33. [Google Scholar] [CrossRef] [Green Version]
- Grabherr, L.; Cuffel, C.; Guyot, J.P.; Mast, F.W. Mental transformation abilities in patients with unilateral and bilateral vestibular loss. Exp. Brain Res. 2011, 209, 205–214. [Google Scholar] [CrossRef] [Green Version]
- Byun, J.Y.; Hong, S.M.; Yeo, S.G.; Kim, S.H.; Kim, S.W.; Park, M.S. Role of subjective visual vertical test during eccentric rotation in the recovery phase of vestibular neuritis. Auris Nasus Larynx 2010, 37, 565–569. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Databases | Search Strategy |
|---|---|
| Medline PubMed | (headache disorders, primary[mh] OR headache disorders, primary[tiab] OR headache disorders[mh] OR headache disorders[tiab] OR headache[mh] OR headache[tiab] OR tension-type headache[mh] OR tension-type headache[tiab] OR headache*[tiab] OR migraine disorders[mh] OR migraine disorders[tiab] OR migraine with aura[mh] OR migraine with aura[tiab] OR migraine without aura[mh] OR migraine without aura[tiab] OR “vestibular migraine”[tiab]) AND (perception of verticality[tiab] OR visual vertical*[tiab] OR verticality sense[tiab] OR subjective visual vertical[tiab] OR “svv”[tiab]) |
| Scopus | (TITLE-ABS-KEY ((“migraine” OR “migraine disorders” OR “vestibular migraine” OR “migraine with aura” OR “migraine without aura” OR “headache disorders” OR “headache” OR “tension-type headache”)) AND TITLE-ABS-KEY ((“perception of verticality” OR “visual vertical*” OR “verticality sense” OR “subjective visual vertical”))) |
| Web of Science | TOPIC: ((*migraine* OR *migraine disorders* OR *vestibular migraine* OR *migraine with aura* OR *migraine without aura* OR *headache disorders* OR *headache* OR *tension-type headache* OR *headaches*)) AND TOPIC: ((*perception of verticality* OR *visual verticality* OR *verticality sense* OR *subjective visual vertical*)) |
| Cinahl | (MH headache, primary OR AB headache, primary OR MH migraine OR AB migraine OR MH OR AB vestibular migraine OR MH tension headache OR AB tension headache or AB headache) OR (AB perception of verticality OR AB verticality sense OR AB subjective visual vertical OR AB visual vertical) |
| Scielo | (migraine OR vestibular migraine OR headache) AND (verticality OR verticality perception OR verticality sense OR subjective visual vertical) |
| Exposed Group | Healthy Controls | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author and Year | N Comp | NS | N | Mean Age | Sex (M/F) | Type of PHD | Diag. Criteria | N | Mean Age | Sex (M/F) |
| Asai et al. 2009 [52] | 2 | 53 | 37 | 44 | 12/25 | MIG/TTH | IHS | 32 | 44 | 10/22 |
| Ashish et al. 2017 [53] | 1 | 148 | 66 | 39.8 | 26/40 | MIG | Neuh. | 82 | 37.2 | 52/30 |
| Chang et al. 2019 [54] | 1 | 63 | 36 | 43 | 5/31 | MIG | ICVD | 27 | NR | NR |
| Crevits et al. 2012 [55] | 1 | 143 | 47 | 38 | 6/41 | MIG | IHS | 96 | 39 | 30/66 |
| Kandemir et al. 2014 [56] | 3 | 94 | 64 | 35.5 | 6/58 | MIG/TTH | IHS | 30 | 32.8 | 5/25 |
| Miller et al. 2016 [58] | 1 | 20 | 10 | 33 | 2/8 | MIG | IHS | 10 | 27 | 6/4 |
| Winnick et al. 2018 [57] | 1 | 54 | 27 | 43 | 8/19 | MIG | ICVD | 27 | 41 | 11/19 |
| Author and Year | SVV Type | Rod Adjustment Method | Room Condition | Body Position | Head Position | Initial Angle | Number of Rep. | Final SVV Value Expressed |
|---|---|---|---|---|---|---|---|---|
| Asai et al. 2009 [52] | Rod projected | Potentiometer by rotating handle | Complete darkness | Upright sitting | 0º Fixed | Fixed 40° | 8 | Absolute error mean |
| Ashish et al. 2017 [53] | Screen rod projected | Joystick handle (potentiometer) | Dark room | Upright sitting | No fixed | Random range 5–20° | 6 | Absolute error mean |
| Chang et al. 2019 [54] | Bucket test | Hands in the bucket | Dark bucket | Upright sitting | No fixed | Random | 3 | Absolute error mean |
| Crevits et al. 2012 [55] | Screen rod projected | Infrared remote controlled potentiometer | Totally Dark room | Upright sitting | 0° fixed | Random | 10 | Error mean |
| Kandemir et al. 2014 [56] | Bucket test | Hands in the bucket | Translucent plastic bucket | Upright sitting | No fixed | Random | 10 | Error mean |
| Miller et al. 2016 [58] | Screen rod projected | Handle dial | Dark room | Upright sitting | No fixed | Random range ±30° | 8 | Error mean |
| Winnick et al. 2018 [57] | Screen rod projected | Handle controller | Dark room | Upright sitting | 0°, ±20° fixed | Random | 100 | Error mean |
| Study | S1 | S2 | S3 | S4 | C1 | E1 | E2 | E3 | Total |
|---|---|---|---|---|---|---|---|---|---|
| Asai et al. 2009 [52] | * | * | - | - | ** | * | * | - | 6 |
| Ashish et al. 2017 [53] | * | * | - | * | ** | * | * | - | 7 |
| Chang et al. 2019 [54] | * | * | - | - | ** | * | * | - | 6 |
| Crevits et al. 2012 [55] | * | * | - | - | ** | * | * | - | 6 |
| Kandemir et al. 2014 [56] | * | * | - | * | ** | * | * | - | 7 |
| Miller et al. 2016 [58] | * | * | - | - | ** | * | * | - | 6 |
| Winnick 2018 [57] | * | * | - | * | ** | * | * | - | 7 |
| Effect Size | Publication Bias | Heterogeneity | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Groups | K | N | Ns | SMD | 95% CI | p | Funnel Plot | Trim-and-Fill | q-Value | I2 | p | ||
| Adj SMD | % of Var | ||||||||||||
| Overall PHD | 10 | 816 | 81.6 | 0.530 | [0.225, 0.836] | <0.001 | Slight asym | 0.335 | 37% | 8.779 | 0% | 0.458 | |
| PHD subgroups | MIG | 8 | 669 | 83.7 | 0.369 | [0.1, 0.638] | 0.007 | Slight asym | 0.267 | 28% | 7.481 | 6.5% | 0.38 |
| TTH | 2 | 147 | 73.5 | 1.122 | [0.540, 1.704] | <0.001 | - | - | - | 1 | 0% | 0.317 | |
| Head position | Fixed | 4 | 303 | 75.75 | 0.589 | [0.071, 1.107] | 0.026 | Slight asym | 0.45 | 23% | 1.108 | 0% | 0.7751 |
| No fixed | 6 | 513 | 85.5 | 0.502 | [0.080, 0.923] | 0.020 | Sym | 0.502 | 0% | 6.483 | 8% | 0.2620 | |
| Type SVV measure | Rod Projected | 6 | 471 | 78.5 | 0.493 | [0.081, 0.906] | 0.019 | Asym | 0.21 | 53% | 4.880 | 0% | 0.4307 |
| Bucket test | 4 | 345 | 86.25 | 0.593 | [0.097, 1.090] | 0.019 | Sym | 0.593 | 0% | 2.856 | 0% | 0.4144 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obrero-Gaitán, E.; Manrique-Navarro, M.; Lérida-Ortega, M.Á.; Rodríguez-Almagro, D.; Osuna-Pérez, M.C.; Lomas-Vega, R. Misperception of Visual Verticality in Patients with Primary Headache Disorders: A Systematic Review with Meta-Analysis. Brain Sci. 2020, 10, 664. https://doi.org/10.3390/brainsci10100664
Obrero-Gaitán E, Manrique-Navarro M, Lérida-Ortega MÁ, Rodríguez-Almagro D, Osuna-Pérez MC, Lomas-Vega R. Misperception of Visual Verticality in Patients with Primary Headache Disorders: A Systematic Review with Meta-Analysis. Brain Sciences. 2020; 10(10):664. https://doi.org/10.3390/brainsci10100664
Chicago/Turabian StyleObrero-Gaitán, Esteban, María Manrique-Navarro, Miguel Ángel Lérida-Ortega, Daniel Rodríguez-Almagro, María Catalina Osuna-Pérez, and Rafael Lomas-Vega. 2020. "Misperception of Visual Verticality in Patients with Primary Headache Disorders: A Systematic Review with Meta-Analysis" Brain Sciences 10, no. 10: 664. https://doi.org/10.3390/brainsci10100664