
Effects of a Rehabilitation Exercise Program Using Electro Muscle Stimulation following Anterior Cruciate Ligament Reconstruction on the Circumference, Activity, and Function of the Quadriceps Muscle
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants Characteristics
2.2. Experimental Design
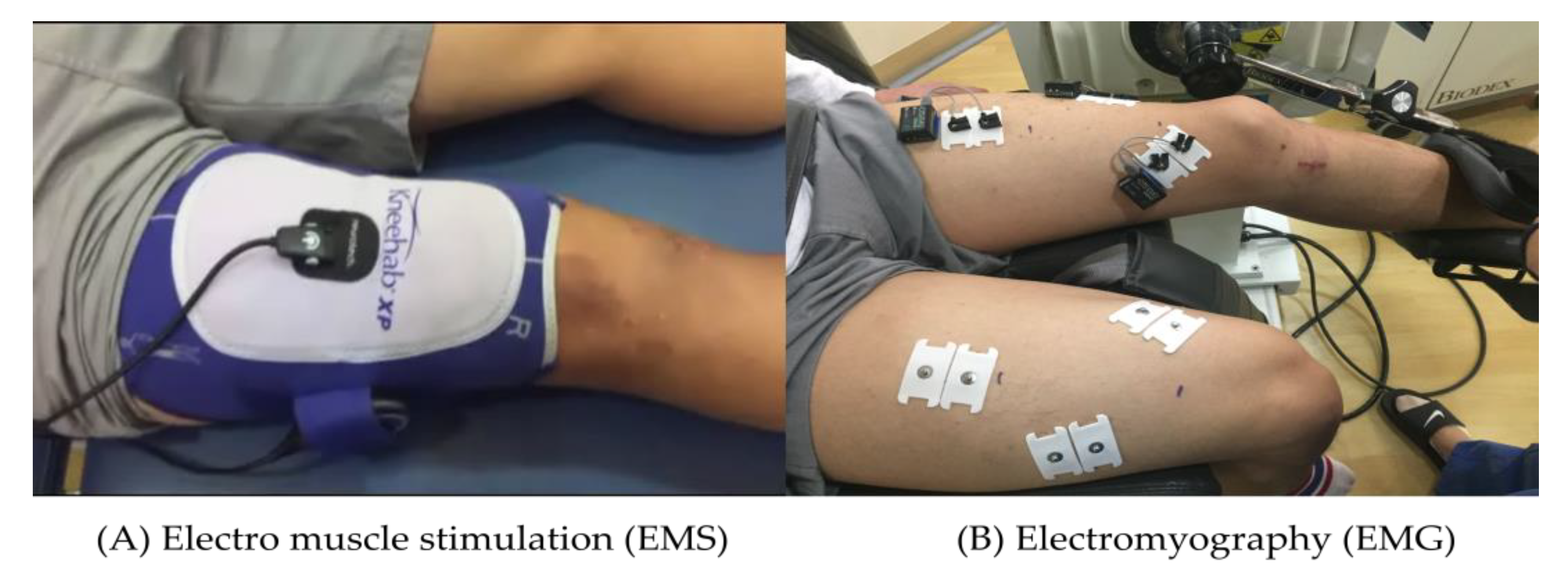
2.3. Electro Muscle Stimulation
2.4. Anthropometry
2.5. Clinical Evaluation Parameters of the Subjective Knee Functional State
2.6. Thigh Circumference
2.7. Muscle Activity
2.8. Isokinetic Muscular Function
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sandberg, R.; Balkfors, B.; Nilsson, B.; Westlin, N. Operative versus non-operative treatment of recent injuries to the ligaments of the knee. A prospective randomized study. J. Bone Joint Surg. Am. 1987, 69, 1120–1126. [Google Scholar] [CrossRef]
- Giove, T.P.; Miller, S.J., 3rd; Kent, B.E.; Sanford, T.L.; Garrick, J.G. Non-operative treatment of the torn anterior cruciate ligament. J. Bone Joint Surg. Am. 1983, 65, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Tsepis, E.; Vagenas, G.; Giakas, G.; Georgoulis, A. Hamstring weakness as an indicator of poor knee function in ACL-deficient patients. Knee Surg. Sports Traumatol. Arthrosc. 2004, 12, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.J.; Park, S.K.; Uhm, Y.H.; Park, S.H.; Chun, D.W.; Kim, J.H. The correlation between muscle activity of the quadriceps and balance and gait in stroke patients. J. Phys. Ther. Sci. 2016, 28, 2289–2292. [Google Scholar] [CrossRef] [Green Version]
- Thomas, A.C.; Villwock, M.; Wojtys, E.M.; Palmieri-Smith, R.M. Lower extremity muscle strength after anterior cruciate ligament injury and reconstruction. J. Athl. Train. 2013, 48, 610–620. [Google Scholar] [CrossRef] [Green Version]
- Malone, T.; Blackburn, T.A.; Wallace, L.A. Knee rehabilitation. Phys. Ther. 1980, 60, 1602–1610. [Google Scholar] [CrossRef]
- Lindström, M.; Strandberg, S.; Wredmark, T.; Felländer-Tsai, L.; Henriksson, M. Functional and muscle morphometric effects of ACL reconstruction. A prospective CT study with 1 year follow-up. Scand. J. Med. Sci. Sports 2013, 23, 431–442. [Google Scholar] [CrossRef]
- Ithurburn, M.P.; Paterno, M.V.; Thomas, S.; Pennell, M.L.; Evans, K.D.; Magnussen, R.A.; Schmitt, L.C. Clinical measures associated with knee function over two years in young athletes after ACL reconstruction. Knee 2019, 26, 355–363. [Google Scholar] [CrossRef]
- Jenkins, S.M.; Guzman, A.; Gardner, B.B.; Bryant, S.A.; Del Sol, S.R.; McGahan, P.; Chen, J. Rehabilitation After Anterior Cruciate Ligament Injury: Review of Current Literature and Recommendations. Curr. Rev. Musculoskelet Med. 2022, 15, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Hauger, A.V.; Reiman, M.P.; Bjordal, J.M.; Sheets, C.; Ledbetter, L.; Goode, A.P. Neuromuscular electrical stimulation is effective in strengthening the quadriceps muscle after anterior cruciate ligament surgery. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 399–410. [Google Scholar] [CrossRef]
- Buckthorpe, M.; La Rosa, G.; Villa, F.D. Restoring knee extensor strength after anterior cruciate ligament reconstruction: A clinical commentary. Int. J. Sports Phys. Ther. 2019, 14, 159–172. [Google Scholar] [CrossRef] [Green Version]
- Bremner, C.B.; Holcomb, W.R.; Miller, M.G. Recommendations to Increase Neuromuscular Electrical Stimulation Training Intensity During Quadriceps Treatments for Orthopedic Knee Conditions. Clin. J. Sport Med. 2021, 31, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.E.; Mizner, R.L.; Snyder-Mackler, L. Neuromuscular electrical stimulation for quadriceps muscle strengthening after bilateral total knee arthroplasty: A case series. J. Orthop. Sports Phys. Ther. 2004, 34, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaviano, N.R.; Saliba, S. Can the Use of Neuromuscular Electrical Stimulation Be Improved to Optimize Quadriceps Strengthening? Sports Health 2016, 8, 79–85. [Google Scholar] [CrossRef]
- Lieber, R.L.; Silva, P.D.; Daniel, D.M. Equal effectiveness of electrical and volitional strength training for quadriceps femoris muscles after anterior cruciate ligament surgery. J. Orthop. Res. 1996, 14, 131–138. [Google Scholar] [CrossRef]
- Moritani, T.; Muro, M.; Kijima, A.; Gaffney, F.A.; Parsons, D. Electromechanical changes during electrically induced and maximal voluntary contractions: Surface and intramuscular EMG responses during sustained maximal voluntary contraction. Exp. Neurol. 1985, 88, 484–499. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A.; Vivodtzev, I.; Minetto, M.A.; Place, N. A new paradigm of neuromuscular electrical stimulation for the quadriceps femoris muscle. Eur. J. Appl. Physiol. 2014, 114, 1197–1205. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Thomé, G.R.; Costa, R.A.; Marquezi, M.L.; Aparecido, J.M.; Durigan, J.L.Q.; Amorim, C.F.; Liebano, R.E. Effects of neuromuscular electrical stimulation on torque and performance in recreational distance runners: A randomized controlled trial. J. Bodyw. Mov. Ther. 2021, 28, 369–375. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Collins, D.F.; Millet, G.Y.; Vaz, M.A.; Maffiuletti, N.A. Enhancing Adaptations to Neuromuscular Electrical Stimulation Training Interventions. Exerc. Sport Sci. Rev. 2021, 49, 244–252. [Google Scholar] [CrossRef]
- Soderberg, G.L.; Ballantyne, B.T.; Kestel, L.L. Reliability of lower extremity girth measurements after anterior cruciate ligament reconstruction. Physiother. Res. Int. 1996, 1, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.R.; Richardson, A.B.; Kikuchi, C.K.; Goldberg, D.B.; Marumoto, J.M.; Kan, D.M. Effectiveness of Accelerated Recovery Performance for Post-ACL Reconstruction Rehabilitation. Hawaii J. Health Soc. Welf. 2019, 78, 41–46. [Google Scholar] [PubMed]
- Tillin, N.A.; Folland, J.P. Maximal and explosive strength training elicit distinct neuromuscular adaptations, specific to the training stimulus. Eur. J. Appl. Physiol. 2014, 114, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Matos, F.; Amaral, J.; Martinez, E.; Canário-Lemos, R.; Moreira, T.; Cavalcante, J.; Peixoto, R.; Pinheiro, B.N.; Junior, L.S.; Uchoa, P.; et al. Changes in Muscle Thickness after 8 Weeks of Strength Training, Electromyostimulation, and Both Combined in Healthy Young Adults. Int. J. Environ. Res. Public Health 2022, 19, 3184. [Google Scholar] [CrossRef]
- Lepley, L.K.; Wojtys, E.M.; Palmieri-Smith, R.M. Combination of eccentric exercise and neuromuscular electrical stimulation to improve quadriceps function post-ACL reconstruction. Knee 2015, 22, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Zhang, Q.; Li, Y. Clinical Study of Neuromuscular Electrical Stimulation in the Prevention of Deep Venous Thrombosis of Lower Extremities after Anterior Cruciate Ligament Reconstruction. J. Healthc. Eng. 2022, 2022, 7857272. [Google Scholar] [CrossRef]
- Glattke, K.E.; Tummala, S.V.; Chhabra, A. Anterior Cruciate Ligament Reconstruction Recovery and Rehabilitation: A Systematic Review. J. Bone Jt. Surg. Am. 2022, 104, 739–754. [Google Scholar] [CrossRef]
- Feil, S.; Newell, J.; Minogue, C.; Paessler, H.H. The effectiveness of supplementing a standard rehabilitation program with superimposed neuromuscular electrical stimulation after anterior cruciate ligament reconstruction: A prospective, randomized, single-blind study. Am. J. Sports Med. 2011, 39, 1238–1247. [Google Scholar] [CrossRef]
- Hasegawa, S.; Kobayashi, M.; Arai, R.; Tamaki, A.; Nakamura, T.; Moritani, T. Effect of early implementation of electrical muscle stimulation to prevent muscle atrophy and weakness in patients after anterior cruciate ligament reconstruction. J. Electromyogr. Kinesiol. 2011, 21, 622–630. [Google Scholar] [CrossRef] [Green Version]
- Martin, L.; Cometti, G.; Pousson, M.; Morlon, B. Effect of electrical stimulation training on the contractile characteristics of the triceps surae muscle. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 67, 457–461. [Google Scholar] [CrossRef]
- Oliveira, P.; Modesto, K.A.G.; Bottaro, M.; Babault, N.; Durigan, J.L.Q. Training Effects of Alternated and Pulsed Currents on the Quadriceps Muscles of Athletes. Int. J. Sports Med. 2018, 39, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Mancinelli, R.; Toniolo, L.; Di Filippo, E.S.; Doria, C.; Marrone, M.; Maroni, C.R.; Verratti, V.; Bondi, D.; Maccatrozzo, L.; Pietrangelo, T.; et al. Neuromuscular Electrical Stimulation Induces Skeletal Muscle Fiber Remodeling and Specific Gene Expression Profile in Healthy Elderly. Front. Physiol. 2019, 10, 1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taradaj, J.; Halski, T.; Kucharzewski, M.; Walewicz, K.; Smykla, A.; Ozon, M.; Slupska, L.; Dymarek, R.; Ptaszkowski, K.; Rajfur, J.; et al. The effect of neuromuscular electrical stimulation on quadriceps strength and knee function in professional soccer players: Return to sport after ACL reconstruction. BioMed Res. Int. 2013, 2013, 802534. [Google Scholar] [CrossRef]
- Deng, W.; Lin, M.; Yu, S.; Liang, H.; Zhang, Z.; Tang, C.; Liu, C. Effects of Hip Joint Angle on Quadriceps Recruitment Pattern During Knee Extension in Healthy Individuals: Analysis by Ultrasound-Based Shear-Wave Elastography. Front. Physiol. 2022, 13, 836435. [Google Scholar] [CrossRef] [PubMed]
- Laprade, J.; Culham, E.; Brouwer, B. Comparison of five isometric exercises in the recruitment of the vastus medialis oblique in persons with and without patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 1998, 27, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brownstein, B.; Lamb, R.E.; Mangine, R.E. Quadriceps torque and integrated electromyography*. J. Orthop. Sports Phys. Ther. 1985, 6, 309–314. [Google Scholar] [CrossRef]
- Hammami, N.; Jdidi, H.; Khezami, M.A.; Ghidaoui, L.; Talbi, A.; Hannachi, C.; Farinha, P.M.; Behlouli, E.; Bouassida, A.; Dziri, C.; et al. Isokinetic strengthening and neuromuscular electrical stimulation protocol impact on physical performances, functional status and quality of life in knee osteoarthritis overweight/obese women. Knee 2022, 39, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Werner, S.; Arvidsson, H.; Arvidsson, I.; Eriksson, E. Electrical stimulation of vastus medialis and stretching of lateral thigh muscles in patients with patello-femoral symptoms. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 85–92. [Google Scholar] [CrossRef]
- Gondin, J.; Cozzone, P.J.; Bendahan, D. Is high-frequency neuromuscular electrical stimulation a suitable tool for muscle performance improvement in both healthy humans and athletes? Eur. J. Appl. Physiol. 2011, 111, 2473–2487. [Google Scholar] [CrossRef]
- Kim, K.M.; Croy, T.; Hertel, J.; Saliba, S. Effects of neuromuscular electrical stimulation after anterior cruciate ligament reconstruction on quadriceps strength, function, and patient-oriented outcomes: A systematic review. J. Orthop. Sports Phys. Ther. 2010, 40, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Toth, M.J.; Tourville, T.W.; Voigt, T.B.; Choquette, R.H.; Anair, B.M.; Falcone, M.J.; Failla, M.J.; Stevens-Lapslaey, J.E.; Endres, N.K.; Slauterbeck, J.R.; et al. Utility of Neuromuscular Electrical Stimulation to Preserve Quadriceps Muscle Fiber Size and Contractility After Anterior Cruciate Ligament Injuries and Reconstruction: A Randomized, Sham-Controlled, Blinded Trial. Am. J. Sports Med. 2020, 48, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- Langeard, A.; Bigot, L.; Chastan, N.; Gauthier, A. Does neuromuscular electrical stimulation training of the lower limb have functional effects on the elderly?: A systematic review. Exp. Gerontol. 2017, 91, 88–98. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Melo, M.; Aragão, F.A.; Vaz, M.A. Neuromuscular electrical stimulation for muscle strengthening in elderly with knee osteoarthritis—A systematic review. Complement. Ther. Clin. Pract. 2013, 19, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, E.L.; Houghton, P.; Anthony, J.; Rennie, S.; Shay, B.L.; Hoens, A.M. Neuromuscular Electrical Stimulation for Treatment of Muscle Impairment: Critical Review and Recommendations for Clinical Practice. Physiother. Can. 2017, 69, 1–76. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | CONG (n = 12) | EMSG (n = 12) | p-Value |
|---|---|---|---|
| Gender (male/female) | 10/2 | 9/3 | - |
| Age (years) | 30.4 ± 13.0 | 28.8 ± 10.6 | 0.542 |
| Height (cm) | 173.3 ± 8.0 | 171.1 ± 7.7 | 0.611 |
| Body weight (kg) | 66.6 ± 12.2 | 66.2 ± 18.3 | 0.917 |
| Body mass index (kg·m−2) | 22.8 ± 3.2 | 22.2 ± 4.0 | 0.854 |
| Tegner activity scale | 6.8 ± 1.6 | 6.4 ± 1.6 | 0.620 |
| ACL reconstruction side (Rt/Lt) | 7/5 | 5/7 | - |
| Exercise | Weeks of Program | ||||
|---|---|---|---|---|---|
| 0–2 | 3–4 | 5–6 | 7–8 | 9–12 | |
| |||||
| 0–90° | o | ||||
| 0–130° | o | ||||
| o | o | o | o | o |
| o | o | |||
| o | o | o | o | |
| |||||
| Leg extension (90~60°) | o | o | |||
| Leg curl (non-weight) | o | o | |||
| Leg curl (weight) | o | o | |||
| |||||
| Weight shifting, cup walking | o | o | |||
| One leg balance | o | o | o | ||
| o | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, S.-I.; Kim, J.-W.; Nam, S.-S.; Moon, H.-W.; Jung, W.-S. Effects of a Rehabilitation Exercise Program Using Electro Muscle Stimulation following Anterior Cruciate Ligament Reconstruction on the Circumference, Activity, and Function of the Quadriceps Muscle. Appl. Sci. 2023, 13, 4153. https://doi.org/10.3390/app13074153
Cho S-I, Kim J-W, Nam S-S, Moon H-W, Jung W-S. Effects of a Rehabilitation Exercise Program Using Electro Muscle Stimulation following Anterior Cruciate Ligament Reconstruction on the Circumference, Activity, and Function of the Quadriceps Muscle. Applied Sciences. 2023; 13(7):4153. https://doi.org/10.3390/app13074153
Chicago/Turabian StyleCho, Seung-Ik, Jeong-Weon Kim, Sang-Seok Nam, Hwang-Woon Moon, and Won-Sang Jung. 2023. "Effects of a Rehabilitation Exercise Program Using Electro Muscle Stimulation following Anterior Cruciate Ligament Reconstruction on the Circumference, Activity, and Function of the Quadriceps Muscle" Applied Sciences 13, no. 7: 4153. https://doi.org/10.3390/app13074153