Abstract
Background and Aims: Previous observational studies found inconsistent associations between serum vitamin D levels and dental caries risk. A dose-response meta-analysis of cross-sectional studies was performed to investigate the association. Methods: To April 2023, the ISI Web of Science, PubMed, Scopus, and Google Scholar databases were searched for published papers. Finally, 13 cross-sectional studies were considered that provided odds ratios (ORs) with 95% confidence intervals (CIs) for dental caries in relation to serum vitamin D levels across all age groups. Two reviewers conducted a thorough screening of the studies, data extraction, bias risk assessment, and evidence quality. A random-effect model was used to assess the pooled estimated odd ratios (with 95% confidence intervals). A weighted mixed-effects dose-response meta-analysis in one stage was carried out. Results: Dental caries was significantly more likely to occur when serum vitamin D levels were low compared to high (OR: 1.41; 95% CI: 1.18, 1.68; GRADE = poor confidence). With a 10 nmol/L increase in serum vitamin D level, linear dose-response analysis showed a significant 3% (OR: 0.97; 95% CI: 0.96, 0.99) decrease in the likelihood of dental caries. Serum vitamin D levels and dental caries were found to be inversely correlated, with a significant dose-response relationship at levels greater than 78 nmol/L. Conclusion: This meta-analysis showed that vitamin D insufficiency was strongly associated with dental caries, and that a 10 nmol/L increase in blood 25(OH)D levels was linked to a 3% decrease in dental caries. However, the findings may have less clinical significance due to the uncertainty of the evidence.
1. Introduction
The essential fat-soluble prohormone vitamin D, also known as the “sunshine vitamin,” plays a fundamental biological role in the human body [1]. It is vital for maintaining normal growth, controlling calcium and phosphorus levels, and promoting the mineralization of bones and other calcified tissues, such as teeth [2,3,4]. Vitamin D deficiency is a common issue in many communities because of limited dietary sources and fortified foods with vitamin D [5]. Epidemiological studies provide compelling evidence that vitamin D deficiency represents a pervasive global epidemic, posing a substantial risk to approximately 1 billion of the world’s population [6,7]. Vitamin D deficiency can cause musculoskeletal disorders or non-communicable diseases [8]. Since 25-hydroxyvitamin D (25[OH] D) plays a role in tooth formation, this deficit makes teeth susceptible to caries because of enamel defects [3,9]. Therefore, a lack of vitamin D has been linked to enamel abnormalities and a higher chance of developing dental caries [10].
Dental caries, also known as tooth decay, is a multifaceted infectious condition characterized by the adherence of bacteria to teeth and their metabolic conversion of sugars into acid [11,12]. This acid attack on dental tissue leads to discomfort, pain, chewing difficulties, and having a negative effect on overall quality of life [13,14,15]. The available evidence substantiates that individuals across all age groups are susceptible to dental caries [12,16,17,18]. Moreover, as indicated by reports from the World Health Organization (WHO), dental caries ranks as the fourth most costly chronic disease to manage [19]. Dental caries prevalence, according to the researchers, is linked to a number of variables, including low socioeconomic position, restricted dental access, sugar consumption, parental education, frequency of brushing, regular dental visits, and fluoride intake [20,21,22,23,24]. Because dental caries and weakened oral conditions impede people’s ability to chew and bite, inadequate 25[OH] D levels can also induce vitamin D insufficiency and nutritional issues [25].
Numerous epidemiological studies have suggested a possible connection between vitamin D levels in the general population and the development of dental caries [9,26,27,28]. Nevertheless, current research evidence remains inconclusive in establishing a definitive relationship [29,30]. A systematic review and meta-analysis of studies that involved controlled clinical trials revealed that vitamin D supplementation in children may have the potential to lessen caries experience [31]. Low levels of 25[OH] D and childhood dental caries were linked, according to a recent systematic review [32]. In addition, a Chinese meta-analysis discovered that children’s dental caries risk may be increased by vitamin D insufficiency [33].
The existing literature indicates an association between serum vitamin D levels and dental caries. However, previous review studies are limited as they often lack meta-analyses [32], fail to evaluate the certainty of the evidence [32,33], and their study population consisted of only children [31,32,33]. Therefore, this study aims to address these limitations by (1) including new studies not covered in previous systematic reviews and meta-analyses [16,18,34,35,36,37], (2) conducting a meta-analysis of cross-sectional studies, (3) assessing the certainty of the evidence, and (4) including all age groups. Hence, the aim of this study was to provide a systematic review of the available cross-sectional data on measurements of dental caries status and serum vitamin level in all age groups.
2. Materials and Methods
Following PRISMA’s (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) recommended procedures, the current systematic review and meta-analysis was conducted [38]. In addition, this systematic review questions followed the population, intervention, comparator(s), and outcomes (PICO) framework [39]. The study protocol for this investigation is available online through PROSPERO, with the registration number CRD42023424195 from: https://www.crd.york.ac.uk/prospero/#searchadvanced (accessed on 16 May 2023).
2.1. Literature Search
Two authors (MM and RL) independently conducted systematic searches across three databases, namely ISI Web of Science, PubMed, and Scopus, to include observational studies published up until 30 April 2023. In addition, a manual search was performed using Google Scholar. The electronic search strategy is shown in Supplementary Table S1. The search method did not include any limitations on publishing date or language.
2.2. Study Selection
Based on the following criteria, primary studies were deemed eligible for inclusion in this systematic review and meta-analysis: (1) cross-sectional population-based epidemiological studies; (2) participants from all age groups; (3) measurement of serum 25[OH]D levels as the exposure variable; (4) examination of dental caries as the outcome of interest; and (5) provision of odds ratios (ORs) and 95% confidence intervals (CIs) to assess the relationship between serum vitamin D levels and dental caries. In studies that reported ORs for two cut-off points for vitamin D status, one OR was selected to avoid populations overlap. Studies with (1) design of the randomized clinical trial, case-control, and cohort, (2) gray literature (book chapters, conference abstracts, letters, theses, case reports, and review articles), (3) patient population, (4) standardized regression coefficient (ß) for the association between serum vitamin D levels and dental caries, and (5) absence of multivariate adjustment, were excluded from the meta-analysis.
2.3. Data Extraction
The articles were originally reviewed by title and abstract; studies with possibly pertinent data were then extracted and sent for full-text evaluation. Two authors (MM and DT) independently extracted the data, and any disagreements were settled through conversation until an agreement was reached. It was not essential to contact the included studies’ authors at any point in the procedure. The primary author’s last name, the year of publication, the study’s location, its population, its design, and its sample size were all extracted from each eligible study. Additional information extracted included the number of patients with caries and the total number of individuals, gender distribution, age range, mean serum vitamin D levels, the unit of measurement for serum vitamin D levels, methods used to measure serum vitamin D levels, information about each vitamin D category, midpoint serum vitamin D levels, odds ratios (ORs), and 95% confidence intervals (CIs) from multi-adjusted models for serum vitamin D levels.
2.4. Risk of Bias Assessment
The “Newcastle-Ottawa Quality Assessment Scale” (NOS) was used to evaluate the studies that were included in this systematic review and meta-analysis [40]. Two authors (MM and RL) independently performed the quality evaluation. Participant selection, comparability, and outcome evaluation are the three main factors of bias that the NOS uses in its “star system” to rank research. Each study is assigned a score based on the number of criteria met within these categories, indicating low, medium, or high quality. The maximum score that can be awarded to each study is nine. According to the NOS criteria, studies with quality scores > 7 were considered to be of high quality, those with scores of 6 or 7 were considered to be of medium quality, and studies with quality ratings of 6 or below were considered to be of low quality for this meta-analysis. Discussion between the authors helped to clarify any disagreements.
2.5. Grading of the Evidence
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach was used to grade the strength of the evidence, which was classified as very low, low, moderate, or high [41]. Several factors were considered within this approach that could lead to the downgrading of evidence, such as indirectness, risk of bias, inconsistency, imprecision, and publication bias. In addition, it was also considered whether there was a dose-response gradient, whether the effect size was large, and how thoroughly confounding variables were taken into account.
2.6. Statistical Analysis
Pooled OR and 95% CIs were calculated to assess the relationship between serum vitamin D levels and dental caries. A random-effects pairwise meta-analysis was used to evaluate the overall effect size for the lowest category of vitamin D level compared to the highest category [42].
I2 and the Cochrane Q statistic were used as measures of heterogeneity [43] and I2 was divided into four categories: maybe not important (0–40%), moderate heterogeneity (30–60%), substantial heterogeneity (50–90%), and considerable heterogeneity (75–100%) [44].
To find potential sources of heterogeneity, we conducted a number of studies on pre-specified subgroups based on the age group, race/ethnicity, sugar consumption, gender, family income, quality score, vitamin D levels categories, and 25[OH] D assessment. Sensitivity analyses were performed by gradually excluding each study from the main analysis to determine how much conclusions might be influenced by a specific study. Visual inspection of funnel plots and the Egger’s regression asymmetry test were used to assess publication bias [45].
We conducted a random-effects dose-response meta-analysis to determine the combined odds ratio (OR) for a 10 nmol/L increase in vitamin D levels. Studies that provided effect sizes specifically for a 10 nmol/L increase in vitamin D levels were included in our analysis. If studies reported the OR for a 1 nmol/L increase instead, we transformed the effect size to reflect a 10 nmol/L increase. This involved calculating the natural logarithm of the OR and its 95% confidence interval, multiplying it by 10, and then exponentiation of the results. In cases where studies reported effect sizes based on different categories of vitamin D levels without providing continuous estimates, we estimated the OR for a 10 nmol/L rise in vitamin D levels using the approach suggested by Greenland and colleagues [46,47]. A random-effects model was used to incorporate the effect sizes from each study. Ultimately, we performed a one-stage weighted mixed-effects meta-analysis to show how the dose-response relationship between vitamin D and dental caries takes shape [48].
By computing the mean of lower and upper bounds for studies that reported serum 25[OH]D levels as ranges, the midpoint for each group was approximated. The interval length was taken to be the same as the adjacent interval in the situations of the open-ended lowest and highest category. The lower threshold of the open-ended lowest category was typically regarded as zero.
STATA version 16.0 (STATA Corp, College Station, TX, USA) was used for the statistical analyses. All tests, including the Cochran’s Q-test, were considered significant if the p value was less than 0.05.
3. Results
3.1. Literature Search
A thorough, systematic literature search was carried out, and 1178 citations were found in three different databases, including PubMed, Scopus, and Web of Science ISI. Through a meticulous screening process, a total of 432 duplicate citations and 717 articles deemed irrelevant based on their titles and abstracts were excluded from further consideration. Subsequently, 29 publications were recognized as potentially relevant records. A comprehensive full-text screening resulted in the exclusion of 16 articles due to their failure to meet the eligible inclusion criteria, lack of sufficient data, or duplication of study content [16,17,49,50,51,52,53,54,55,56,57,58,59,60,61,62] (Supplementary Table S2). As a result, the current systematic review and meta-analysis included a total of 13 cross-sectional studies. (Figure 1).
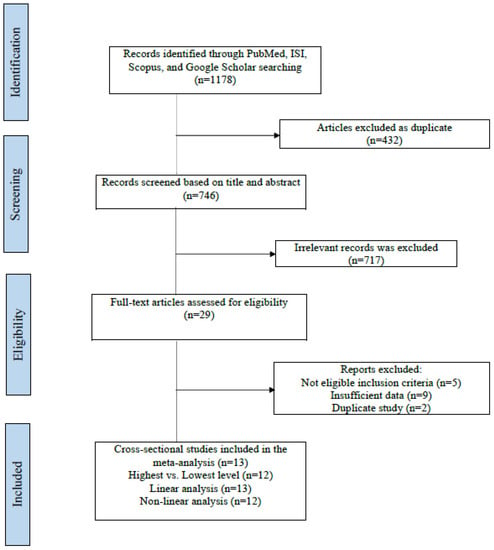
Figure 1.
Flowchart of the study selection process.
3.2. Characteristics of Included Studies
Table 1 provides a summary of the characteristics of the included studies. The studies were published within the timeframe of 2013-2023, encompassing locations such as the USA [18,29,30,34,36,37], Qatar [26], Northern Portugal [16], Korea [9,17], China [35], and Canada [27], and involving participants of both genders. Participants in the studies ranged in age from 1 to 80 years, and the sample size varied from 335 to 8896 individuals across all age groups. The levels of 25[OH] D were assessed using various techniques including radioimmunoassay [9,17,18,26,30,37], chromatography [29,34,35,36], and chemiluminescence methods [16,27]. Out of the total studies reviewed, four were classified as having high quality [17,29,30,34], six were categorized as having medium quality [9,18,26,27,36,37], while only two exhibited low quality based on the Newcastle-Ottawa Scale [16,35] (Supplementary Table S3).

Table 1.
Main characteristics of included cross-sectional studies.
3.3. Findings from the Meta-Analysis on Vitamin D Levels
By utilizing information from 12 studies with a total of 29,883 individuals and 13,436 cases, the link between serum vitamin D levels and dental caries was analyzed. A cross-sectional design was used in each of the included studies. The findings showed a significant association between the exposure and the outcome. Individuals with the lowest serum vitamin D levels, in contrast to those with the highest levels, had a 41% higher chance of developing dental caries (OR: 1.41; 95% CI: 1.18, 1.68; P: 0.001; Figure 2). Even though the results were statistically significant, the certainty of the evidence was rated as poor (Supplementary Table S4). Additionally, there was substantial heterogeneity among the included studies (I2 = 61.9%; P heterogeneity = 0.001).
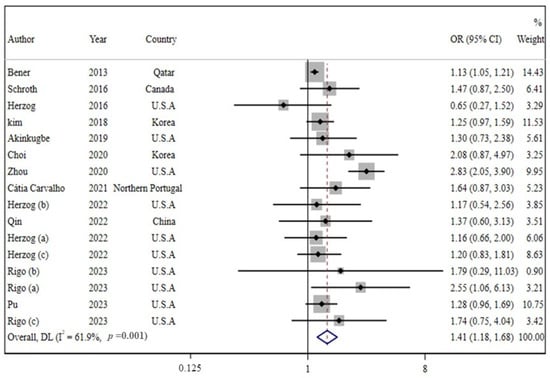
Figure 2.
Forest plot of cross-sectional studies that examined the association between lowest vs. highest level of serum vitamin D and risk of dental caries. The red dashed line shows the effect size of the study which is 1.41. The blue triangle represents the confidence interval. Gray squares show the weight of the input studies, the horizontal lines indicate the confidence intervals and the effect size of each study. (a), (b) and (c) show different effect sizes of a single study.
3.4. Linear and Non-Linear Dose-Response Analysis
Each 10 nmol/L rise in serum vitamin D levels was significantly associated with a 3% decrease in the odds ratio of dental caries, according to a linear dose-response analysis of 13 studies with 17 effect sizes (OR: 0.97; 95% CI: 0.96, 0.99; P: 0.084; Figure 3). In the dose-response meta-analysis, it was found that there was a negative linear correlation between vitamin D levels and dental caries. This finding was based on analyzing 16 effect sizes from 12 studies (P non-linearity = 0.598, P dose-response = 0.002, Figure 4). The effect sizes in different doses from 12.5 to 162.5 nmol/L are reported in Supplementary Table S5. As the level of vitamin D increases, there is a corresponding decrease in the odds ratio of developing dental caries. Notably, when the vitamin D level exceeds 78 nmol/L, this reduction becomes statistically significant (Figure 4 and Supplementary Table S5).
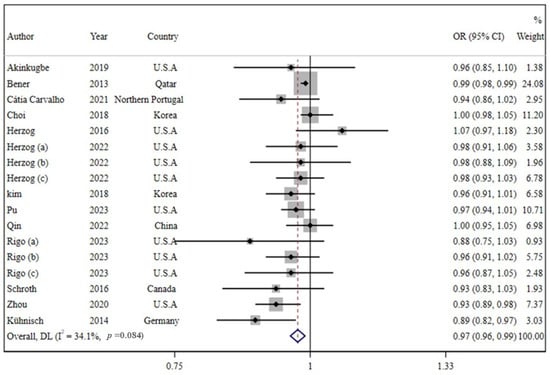
Figure 3.
Forest plots of the estimated odd ratios (OR) of the association between 10 nmol/L increase in vitamin D levels and dental caries. The red dashed line shows the effect size of the analysis. The blue triangle represents the confidence interval of the analysis. Gray squares show the weight of the input studies, the horizontal lines indicate the confidence intervals and the effect size of each study. (a), (b) and (c) letters show different effect sizes of a single study.
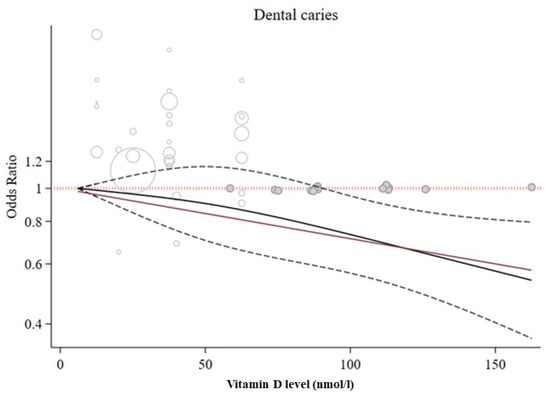
Figure 4.
Non-linear dose-response association between vitamin D levels and dental caries. The lowest level of serum vitamin D (12.5 nmol/L) was considered as the reference. The circles represent the input into the analysis. Dashed red line shows value of 1, which is the OR criterion and the effect sizes are compared to it. The dashed black lines illustrate the confidence interval limits. The solid black line is the study’s overall effect size. The red line shows the direction and the proportion of the association which is linear and inversely proportional.
3.5. Subgroup, Sensitivity Analyses, and Publication Bias
Given the presence of heterogeneity among the studies included, a pre-defined subgroup analysis was conducted to identify its source (Table 2). Through subgroup analysis, we find that age group (P heterogeneity between: < 0.001) and family income (P heterogeneity between: 0.041) are two sources of high heterogeneity. In all subgroups, a rise in the odds ratio of dental caries was associated with a drop in vitamin D serum levels; although this trend was not significant in vitamin D categories of T3 vs. T1, quality scores of high and low, adjusted for sugar consumption, and children and youth subgroups.
Table 2.
Results of subgroup analyses of serum vitamin D levels with dental caries.
Sensitivity analysis showed that none of the excluded studies had an impact on the final estimate significantly, and the results are robust (OR range: 1.17–1.78). Egger’s test and the funnel plot revealed no evidence of publication bias (P: 0.069; Figure 5).
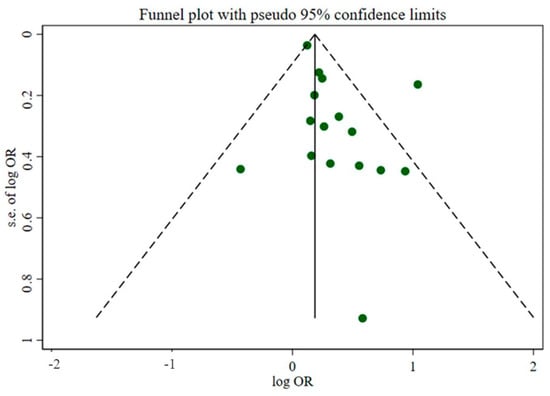
Figure 5.
The funnel plot of the association between vitamin D levels and dental caries. The green circles represent the effect sizes of the input studies. The dashed black lines are the upper and lower limits of the confidence interval. The solid black line shows the overall effect of the analysis.
4. Discussion
In the analysis, a total of 13 studies were included. The studies were published within the timeframe of 2013–2023, encompassing locations such as the USA [18,29,30,34,36,37], Qatar [26], Northern Portugal [16], Korea [9,17], China [35], and Canada [27], and involving participants of both genders. The age of participants in the studies ranged from 1 to 80 years, and the sample size varied from 335 to 8896 individuals across all age groups. Out of the total studies reviewed, four were classified as having high quality [17,29,30,34], six were categorized as having medium quality [9,18,26,27,36,37], while only two exhibited low quality based on the Newcastle-Ottawa Scale [16,35].
The present study examines the relationship between vitamin D levels and dental caries through a comprehensive systematic review and meta-analysis. For this association, no dose-response research has ever conducted done before. The findings of this systematic review and dose-response meta-analysis show a statistically significant relationship between the lowest 25[OH]D level and a higher risk of dental caries when compared to the highest level. However, it is crucial to note that the evidence’s degree of certainty was rated as low. In addition, a linear dose-response study revealed that for every 10 nmol/L rise in 25[OH] D levels, there was an apparent 3% decrease in the risk of dental caries. Nonlinear dose-response analysis revealed a linear dose-dependent association as well.
The relationship between serum vitamin D levels and the risk of dental caries has been evaluated in a number of prior systematic studies and meta-analyses. Although subgroup analysis according to the type of study revealed that cross-sectional and cohort studies found no significant difference in the relationship between the suboptimal vitamin D levels and dental caries risk, a recent meta-analysis found that suboptimal vitamin D concentration significantly increased caries risk in children (11%), which is similar to our finding [33]. In another meta-analysis which included 24 controlled clinical trials of children participants, where 22 of them were conducted before the modern design of trials, the conclusion was a low-certain evidence in favor of the positive effect of vitamin D supplements to reduce caries risk in children [31]. Furthermore, a systematic review by Silva et al. found evidence of an association between low 25[OH] D levels (75 nmol/L) and caries experience in children [32].
Primary studies have uncovered conflicting data. According to our research, dental caries risk was inversely related to vitamin D status. Studies by Benner et al. and Kim et al. supported our findings by showing children with low vitamin D levels had increased dental caries [9,26], additionally, Kuhnisch et al. and Schroth et al. illustrated that there is a significant association between lower caries incidence in children and greater 25[OH] D levels [27,63]. On the other hand, several studies found no link between children’s oral caries experience and 25[OH] D levels [29,30,34].
The inconsistency between results could be because of diversity in age range, sample sizes, or race/ethnicity. However, subgroup analysis was conducted to see where the heterogeneity came from. The subgroup analysis indicated that age group and family income are heterogeneity sources. Reduced vitamin D serum levels were linked to higher risks of dental caries in all subgroups; however, they were not significant in all subgroups.
A 10 nmol/mL increase in 25[OH] D levels, according to earlier research by Zhou et al. and Pu et al., respectively, was associated with a 7% and 10% reduction in the likelihood of developing dental caries [18,36]; these results support our findings, which showed that a 10 nmol/L rise in 25[OH] D concentration resulted in a 3% decrease in the risk of developing dental caries.
Although the precise mechanism linking vitamin D to dental caries is not entirely understood, it has been stated that vitamin D improves calcium metabolism [64]. Plasma levels of calcium and phosphate are regulated by vitamin D during dentin development and promote mineralization by attaching to dental cells [65,66]. Tooth surfaces demineralize by acid-producing bacteria, but vitamin D could maintain adequate calcium and phosphate levels in saliva for remineralization after demineralization [67]. Additionally, vitamin D has lytic activity against cariogenic bacteria [68], so an insufficient vitamin D level can cause development flaws in tooth structure and incomplete response to caries.
Additionally, vitamin D is a vital agent in maintaining the balance of saliva electrolytes which could influence saliva production [69]. In addition, the higher risk of caries is due to lower flow and higher viscosity of saliva [70]. Furthermore, studies revealed that vitamin D regulates the immune system, causing the development of antimicrobial proteins such defensins, cathelicidins, and proteases that attack cariogenic bacteria [71,72,73]. Figure 6 summarizes the possible roles of vitamin D in caries prevention.
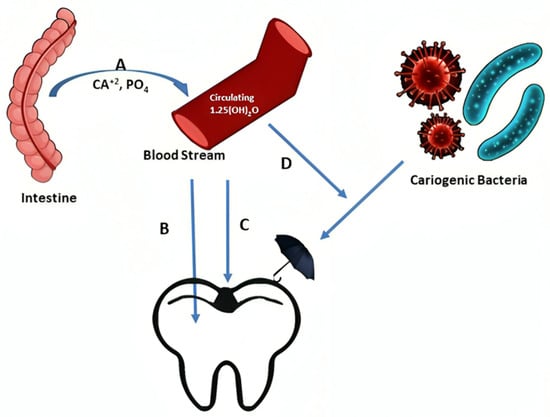
Figure 6.
Possible biological mechanisms of vitamin D in caries prevention: A. Enhances absorption of calcium and phosphorus from the intestine. B. Regulates the deposition of adequate amount of calcium and phosphorus in the tooth structure during development. C. Helps remineralization of tooth surface after demineralization. D. Antimicrobial effects against cariogenic bacteria.
The current study is an updated dose-response meta-analysis that examined the association between dental caries and vitamin D levels across all age groups, and thus the findings could be generalized to the entire population. We attempted to decrement the confounding effects and searched databases without language and time restrictions. Additionally, we only included studies that were carried out on healthy populations, conducted a one-stage weighted mixed-effects meta-analysis to ascertain a subgroup analysis to determine the effect of any potential confounding factors (such as race/ethnicity, sugar consumption, gender, and family income), conducted the Egger’s asymmetry test to determine the impact of publication bias, and calculated the linear and non-linear relationships between the variables. Moreover, the evidence quality for the study outcome was evaluated utilizing the GRADE approach.
The use of cross-sectional research, which could only assess if there was an association between vitamin D level and dental caries but could not demonstrate the causal relationship between them, constituted one of the study’s shortcomings. The included studies have also evaluated the level of serum vitamin D in various ways. Based on the GRADE approach, the overall quality of the evidence was “low”.
5. Conclusions
In conclusion, despite the limited certainty of the data, dental caries risk was considerably increased by low serum vitamin D levels. The risk of dental caries decreased linearly with an increase in vitamin D concentration, and this association was dose-dependent. A 10 nmol/L increase of 25[OH] D levels was significantly associated with a 3% lower risk of dental caries, according to the linear dose-response analysis. Hence, clinically, serum vitamin D level and dental caries status can be seen as markers and predictors for each other, especially in high-risk groups. It is suggested that high-quality studies, e.g., controlled trials or prospective cohort studies with large sample sizes could be an appropriate way to design future research and produce reliable results.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/app13179883/s1, Table S1: Search strategy, last updated April 2023; Table S2: List of excluded articles; Table S3: Quality Assessment of Included Articles (Modified Newcastle-Ottawa Quality Assessment Scale); Table S4: The GRADE quality of evidence; Table S5: The association of different vitamin D levels on dental caries forms the nonlinear dose-response meta-analysis (odds ratio and 95% confidence interval).
Author Contributions
M.K.M. and R.L. contributed to study design, literature search, screening of manuscripts, and drafting the paper. D.T. and H.T. analyzed the data. M.K.M. and R.L. assessed risk of bias and quality of evidence. D.T. and H.T. commented on the manuscript, and revised the study. All authors were involved in the final approval version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80 (Suppl. S6), 1678S–1688S. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.J.; Jeal, N.S.; Kliewer, E.; Sellers, E.A. The relationship between vitamin D and severe early childhood caries: A pilot study. Int. J. Vitam. Nutr. Res. 2012, 82, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.J.; Lavelle, C.; Tate, R.; Bruce, S.; Billings, R.J.; Moffatt, M.E. Prenatal Vitamin D and Dental Caries in Infants. Pediatrics 2014, 133, e1277–e1284. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.J.; A Levi, J.; A Sellers, E.; Friel, J.; Kliewer, E.; Moffatt, M.E. Vitamin D status of children with severe early childhood caries: A case–control study. BMC Pediatr. 2013, 13, 174. [Google Scholar] [CrossRef]
- Hossein-Nezhad, A.; Holick, M.F. Vitamin D for Health: A Global Perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 138–145. [Google Scholar] [CrossRef]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar]
- Holick, M.F. Vitamin D: A millenium perspective. J. Cell. Biochem. 2002, 88, 296–307. [Google Scholar] [CrossRef]
- Kim, I.-J.; Lee, H.-S.; Ju, H.-J.; Na, J.-Y.; Oh, H.-W. A cross-sectional study on the association between vitamin D levels and caries in the permanent dentition of Korean children. BMC Oral Health 2018, 18, 43. [Google Scholar] [CrossRef]
- Foster, B.L.; Hujoel, P.P. (Eds.) Vitamin D in Dentoalveolar and Oral Health; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef]
- Rathee, M.; Sapra, A. Dental Caries; StatPearls: Tampa, FL, USA, 2019. [Google Scholar]
- Dudding, T.; Thomas, S.J.; Duncan, K.; Lawlor, D.A.; Timpson, N.J. Re-Examining the Association between Vitamin D and Childhood Caries. PLoS ONE 2015, 10, e0143769. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Barbero, J.G. Patología y Terapéutica Dental; Síntesis: Madrid, Spain, 2000. [Google Scholar]
- Tanaka, K.; Hitsumoto, S.; Miyake, Y.; Okubo, H.; Sasaki, S.; Miyatake, N.; Arakawa, M. Higher vitamin D intake during pregnancy is associated with reduced risk of dental caries in young Japanese children. Ann. Epidemiol. 2015, 25, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.C.; Gavinha, S.; Manso, M.C.; Rodrigues, R.; Martins, S.; Guimarães, J.T.; Santos, A.C.; Melo, P. Serum Levels of Vitamin D and Dental Caries in 7-Year-Old Children in Porto Metropolitan Area. Nutrients 2021, 13, 166. [Google Scholar] [CrossRef]
- Choi, S.; Seo, D.-G.; Hwang, J.-Y. Serum 25-hydroxyvitamin D levels are associated with dental caries experience in Korean adolescents: The 2010~2014 Korean National Health and Nutrition Examination Surveys. J. Nutr. Health 2018, 51, 287–294. [Google Scholar] [CrossRef]
- Zhou, F.; Zhou, Y.; Shi, J. The association between serum 25-hydroxyvitamin D levels and dental caries in US adults. Oral Dis. 2020, 26, 1537–1547. [Google Scholar] [CrossRef]
- Petersen, P.E. World Health Organization global policy for improvement of oral health-World Health Assembly 2007. Int. Dent. J. 2008, 58, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferro, E.P.d.S.; Pereira, A.C.; Meneghim, M.d.C.; Ambrosano, G.M.B. Assessment of Dental Caries Predictors in a Seven-year Longitudinal Study. J. Public Health Dent. 2006, 66, 169–173. [Google Scholar] [CrossRef]
- Gedicke, K. Rickets and dental caries; possibilities of dental caries prevention with vitamin D preparations with reference to social hygiene uses. Der Offentliche Gesundheitsdienst 1959, 20, 419–432. [Google Scholar]
- Pereira, S.M.; Tagliaferro, E.P.D.S.; Ambrosano, G.M.B.; Cortellazzi, K.L.; Meneghim, M.D.C.; Pereira, A.C. Dental caries in 12-year-old schoolchildren and its relationship with socioeconomic and behavioural variables. Oral Health Prev. Dent. 2007, 5, 299–306. [Google Scholar] [CrossRef]
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health Surveys: Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Linas, N.; Peyron, M.; Hennequin, M.; Eschevins, C.; Nicolas, E.; Delfosse, C.; Collado, V. Masticatory behavior for different solid foods in preschool children according to their oral state. J. Texture Stud. 2019, 50, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Bener, A.; Hoffmann, G.F.; Al Darwish, M.S. Vitamin D deficiency and risk of dental caries among young children: A public health problem. Indian J. Oral Sci. 2013, 4, 75. [Google Scholar] [CrossRef]
- Schroth, R.; Rabbani, R.; Loewen, G.; Moffatt, M. Vitamin D and Dental Caries in Children. J. Dent. Res. 2015, 95, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, M.K.; Lan, R.; Tassery, H.; Tardivo, D. Association between Malnutrition and Dental Caries in Iraqi Kurdish Children. Dent. J. 2023, 11, 141. [Google Scholar] [CrossRef]
- Akinkugbe, A.A.; Moreno, O.; Brickhouse, T.H. Serum cotinine, vitamin D exposure levels and dental caries experience in US adolescents. Community Dent. Oral Epidemiol. 2019, 47, 185–192. [Google Scholar] [PubMed]
- Herzog, K.; Scott, J.M.; Hujoel, P.; Seminario, A.L. Association of vitamin D and dental caries in children Findings from the National Health and Nutrition Examination Survey, 2005–2006. J. Am. Dent. Assoc. 2016, 147, 413–420. [Google Scholar] [CrossRef]
- Hujoel, P.P. Vitamin D and dental caries in controlled clinical trials: Systematic review and meta-analysis. Nutr. Rev. 2012, 71, 88–97. [Google Scholar] [CrossRef]
- Carvalho Silva, C.; Mendes, R.; Manso, M.D.C.; Gavinha, S.; Melo, P. Prenatal or Childhood Serum Levels of Vitamin D and Dental Caries in Paediatric Patients: A Systematic Review. Oral Health Prev. Dent. 2020, 18, 653–667. [Google Scholar]
- Zheng, J.W.; Zheng, T.J.; Liu, H.H.; Wang, P. Correlation of vitamin D levels in children to the risk of dental caries: A Meta-analysis. MJCPLA 2020, 45, 192–199. [Google Scholar]
- Herzog, K.; Ordóñez-Mena, J.M. The association between vitamin D levels and caries experience in children and youth participating in National Health and Nutrition Examination Survey 2011-2016. J. Am. Dent. Assoc. 2022, 153, 848–858.e2. [Google Scholar] [CrossRef]
- Qin, X.; Han, J.; Zhang, Y.; Liu, S.; Shao, L. Correlation between vitamin D level and caries risk in early childhood caries. J. Prev. Treat. Stomatol. Dis. 2022, 30, 111–116. [Google Scholar]
- Pu, R.; Fu, M.; Li, N.; Jiang, Z. A certain protective effect of vitamin D against dental caries in US children and youth: A cross-sectional study. J. Public Health Dent. 2023, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rigo, L.; Bidinotto, A.B.; Hugo, F.N.; Neves, M.; Hilgert, J.B. Untreated caries and serum vitamin D levels in children and youth of the United States: NHANES 2013–2014. Braz. Dent. J. 2023, 34, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Stern, C.; Jordan, Z.; McArthur, A. Developing the Review Question and Inclusion Criteria. AJN Am. J. Nurs. 2014, 114, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson j Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Ottawa Hospital Research Institute Website. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 March 2016).
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar]
- Der Simonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.; Chandler, J.; Welch, V.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Greenland, S.; Longnecker, M.P. Methods for Trend Estimation from Summarized Dose-Response Data, with Applications to Meta-Analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized Least Squares for Trend Estimation of Summarized Dose–response Data. Stata Journal: Promot. Commun. Stat. Stata 2006, 6, 40–57. [Google Scholar] [CrossRef]
- Crippa, A.; Discacciati, A.; Bottai, M.; Spiegelman, D.; Orsini, N. One-stage dose–response meta-analysis for aggregated data. Stat. Methods Med. Res. 2018, 28, 1579–1596. [Google Scholar] [CrossRef]
- Ahmed, H.A.; Ahmed, G.S.; Maktoof, Z.A. Association of vitamin D and dental caries in children in Basra. Int. J. Pharm. Res. 2020, 12, 34–51. [Google Scholar]
- Ali, N.; Rahim, A.; Ali, S.; Iqbal, M. Impact of Vitamin D on development of early childhood caries. Pak. Armed Forces Med. J. 2017, 67, 429–433. [Google Scholar]
- Ali, N.; Rahim, A.; Ali, S.M. Correlation of Hypovitaminosis D with Socioeconomic Status and Dental Caries in Children. J. Islam. Int. Med. Coll. 2019, 14, 202–206. [Google Scholar]
- Antonenko, O.; Bryk, G.; Brito, G.; Pellegrini, G.; Zeni, S.N. Oral health in young women having a low calcium and vitamin D nutritional status. Clin. Oral Investig. 2014, 19, 1199–1206. [Google Scholar] [CrossRef]
- Cetrelli, L.; Bletsa, A.; Lundestad, A.; Gil, E.G.; Fischer, J.; Halbig, J.; Frid, P.; Angenete, O.; Lillevoll, I.; Rosén, A.; et al. Vitamin D, oral health, and disease characteristics in juvenile idiopathic arthritis: A multicenter cross-sectional study. BMC Oral Health 2022, 22, 333. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Lv, X.; Hu, W.; Qian, X.; Wu, T.; Zhu, Y. Vitamin D Status and Its Influence on the Health of Preschool Children in Hangzhou. Front. Public Health 2021, 9, 675403. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Seo, D.-G.; Hwang, J.-Y. Relationship between Serum 25-Hydroxyvitamin D Levels and Experience of Dental Caries according to Calcium Intake in Korean Adolescents. J. Korean Soc. Food Sci. Nutr. 2018, 47, 926–933. [Google Scholar] [CrossRef]
- Ferrillo, M.; Migliario, M.; Marotta, N.; Lippi, L.; Antonelli, A.; Calafiore, D.; Ammendolia, V.; Fortunato, L.; Renò, F.; Giudice, A.; et al. Oral Health in Breast Cancer Women with Vitamin D Deficiency: A Machine Learning Study. J. Clin. Med. 2022, 11, 4662. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, A.; Kashani, A.T.; Shamollaghamsari, S.; Mohammadi, A.H.; Banafshe, H.R. A cross-sectional study on the association between oral health and vitamin D levels in methadone maintenance treatment program of Iranian population. Int. Arch. Health Sci. 2022, 9, 53–57. [Google Scholar] [CrossRef]
- Pratyusha, N.; Vinay, C.; Uloopi, K.S.; RojaRamya, K.S.; Ahalya, P.; Devi, C. Association of serum Vitamin D and salivary calcium and phosphorus levels in 3-11-year-old schoolchildren with dental caries. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 240–245. [Google Scholar]
- Putneva, A.; Academy, C.S.M.; Mishchenko, M.; Karavaeva, T.; Mudrov, V.; Maksimenya, M.; Drozdova, A.; Tsybikov, N.; Pateyuk, A.; Chita Medical College; et al. Correlation between the level of 25(OH)D3 in blood, the content of antimicrobial peptides in oral fluid and dental caries intensity in young individuals. Sib. Med. Rev. 2022, 2022, 62–68. [Google Scholar] [CrossRef]
- Saboktakin, L. The relationship between vitamin D and calcium serum levels with dental caries in 6-12 years old children. J. Parathyr. Dis. 2022, 10, e9141. [Google Scholar] [CrossRef]
- Sohanian, S.; Sadrabad, M.J. Evaluation of the relationship between serum level of Vitamin D and decayed, missing, and filled teeth (DMFT) in young women in Semnan, Iran (2018–2019). J. Sci. Soc. 2020, 47, 69. [Google Scholar] [CrossRef]
- Seminario, A.L.; Jumani, K.; Velan, E.; Scott, J.; Latimer, J.; Schroth, R. Suboptimal Serum Vitamin D Associated with Early Childhood Caries in Special Health Care Needs Children. J. Dent. Child. 2018, 85, 93–101. [Google Scholar]
- Kühnisch, J.; Thiering, E.; Kratzsch, J.; Heinrich-Weltzien, R.; Hickel, R.; Heinrich, J.; Wichmann, H.; Sausenthaler, S.; Zutavern, A.; Chen, C.-M.; et al. Elevated Serum 25(OH)-Vitamin D Levels Are Negatively Correlated with Molar-Incisor Hypomineralization. J. Dent. Res. 2014, 94, 381–387. [Google Scholar] [CrossRef]
- Mellanby, M.; Pattison, C.L. The Action of vitamin D in preventing the spread and promoting the arrest of caries in children. Br. Med. J. 1928, 2, 1079–1082. [Google Scholar] [CrossRef]
- Berdal, A.; Papagerakis, P.; Hotton, D.; Bailleul-Forestier, I.; Davideau, J.-L. Ameloblasts and odontoblasts, target-cells for 1,25-dihydroxyvitamin D3: A review. Int. J. Dev. Biol. 1995, 39, 257–262. [Google Scholar]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Saputo, S.; Faustoferri, R.C.; Quivey, R.G. Vitamin D Compounds Are Bactericidal against Streptococcus mutans and Target the Bacitracin-Associated Efflux System. Antimicrob. Agents Chemother. 2018, 62, e01675-17. [Google Scholar] [CrossRef]
- Dietrich, T.; Nunn, M.; Dawson-Hughes, B.; Bischoff-Ferrari, H.A. Association between serum concentrations of 25-hydroxyvitamin D and gingival inflammation. Am. J. Clin. Nutr. 2005, 82, 575–580. [Google Scholar] [CrossRef]
- Lukacs, J.R.; Largaespada, L.L. Explaining sex differences in dental caries prevalence: Saliva, hormones, and “life-history” etiologies. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2006, 18, 540–555. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P.; Lingström, P. Nutrition, dental caries and periodontal disease: A narrative review. J. Clin. Periodontol. 2017, 44 (Suppl. S18), S79–S84. [Google Scholar] [CrossRef]
- Svensson, D.; Nebel, D.; Nilsson, B.O. Vitamin D3 modulates the innate immune response through regulation of the hCAP-18/LL-37 gene expression and cytokine production. Inflamm. Res. 2016, 65, 25–32. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Proença, L.; Delgado, A.S.; Mendes, J.J. Vitamin D Deficiency and Oral Health: A Comprehensive Review. Nutrients 2020, 12, 1471. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).