

Drug-Food Interactions with a Focus on Mediterranean Diet




Department of Nursing, School of Health Sciences, Hellenic Mediterranean University, GR-71410 Heraklion, Crete, Greece
*
Author to whom correspondence should be addressed.
Appl. Sci. 2022, 12(20), 10207; https://doi.org/10.3390/app122010207
Submission received: 31 August 2022
/
Revised: 5 October 2022
/
Accepted: 7 October 2022
/
Published: 11 October 2022
(This article belongs to the Special Issue Dietary Interventions for Human General and Oral Health and Disease Reduction)
Abstract
:There is a growing interest among people in western countries for adoption of healthier lifestyle habits and diet behaviors with one of the most known ones to be Mediterranean diet (Med-D). Med-D is linked with daily consumption of food products such as vegetables, fruits, whole grains, seafood, beans, nuts, olive oil, low-fat food derivatives and limited consumption of meat or full fat food products. Med-D is well-known to promote well-being and lower the risk of chronic conditions such as cardiovascular diseases, diabetes, and metabolic syndrome. On the other hand bioactive constituents in foods may interfere with drugs’ pharmacological mechanisms, modulating the clinical outcome leading to drug-food interactions (DFIs). This review discusses current evidence for food products that are included within the Med-Dand available scientific data suggest a potential contribution in DFIs with impact on therapeutic outcome. Most cases refer to potential modulation of drugs’ absorption and metabolism such as foods’ impact on drugs’ carrier-mediated transport and enzymatic metabolism as well as potential synergistic or antagonistic effects that enhance or reduce the pharmacological effect for some drugs. Adherence to Med-D can improve disease management and overall well-being, but specific foods should be consumed with caution so as to not hinder therapy outcome. Proper patient education and consultation from healthcare providers is important to avoid any conflicts and side effects due to clinically significant DFIs.
1. Introduction
Mediterranean diet (Med-D) represents one of the most famous and well received diet food habits, particularly in the western countries [1]. Med-D originates from the eating patterns that people around Mediterranean basin have been following since the ancient years, along with the adoption of food products that were cultivated later in the area (i.e., potatoes) [2,3]. Med-D promotes the consumption of all food types but focuses on vegetables, fruits, the nearly exclusive use of olive oil in food preparation, routine consumption of marine food, low fat white meat (chicken, turkey) along with cereals, grains, nuts, wine and lesser consumption of high-fat meat products [3]. UNESCO states regarding Med-D: “The Mediterranean diet is characterized by a nutritional model that has remained constant over time and space, consisting mainly of olive oil, cereals, fresh or dried fruit and vegetables, a moderate amount of fish, dairy and meat, and many condiments and spices, all accompanied by wine or infusions, always respecting beliefs of each community” [4]. Since the first observations in 1960s [5], Med-D has shown undisputable, longitudinal, and high-quality evidence to support its health benefits against specific diseases for people that remain adherent to Med-D dietary patterns [6,7,8,9]. A reduced risk of overall mortality related with metabolic syndrome, cardiovascular diseases, coronary heart disease, myocardial infarction, cancer incidence, diabetes, neurodegenerative diseases, kidney disease and arthritis are mostly identified regarding clinical data availability [10,11,12,13,14,15,16,17,18,19,20,21]. Moreover, for Med-D food products we can recognize specific active constituents (i.e., oleuropein, resveratrol, retinoids, flavonoids, terpenes, catechins, ω-3-fatty acids etc.) with pharmacological effects (i.e., anti-oxidant and anti-inflammatory) that are related with the health benefits from adherence in Med-D [22,23,24,25,26,27,28,29,30,31]. In this respect, the question that arises is whether there could be cases in which pharmacologically active compounds that are present in Med-D foods could potentially interfere with the pharmacological action of drugs and lead in clinically significant DFIs.
Drug interactions are an important clinical issue for optimum healthcare provision. The proper drug administration and drug combinations ensures the minimization of risks for adverse drug reactions (ADRs) due to drug-drug interactions [32,33,34]. Moreover, drug interactions can emerge due to co-administration of several complementary and alternative medicine (CAM) products such as herbal medicinal products (HMPs) as well as dietary supplements (DS) and food products [35,36,37,38]. A DFI describes the physical, biochemical or physiological modulation of a pharmacological process that a drug is following due to the presence of one or more constituents within a food product or other nutraceuticals [39,40]. These bioactive constituents that are present in dietary products may interfere with drugs’ biological pathways and alter drugs’ pharmacological action or levels in the body. Especially for food products there are well-established clinical examples of drug-food interaction (DFI) such as foods containing tyramine and monoamine-oxidase inhibitors (MAOIs), alcoholic beverages or spirits with central nervous system (CNS) drugs as well as grapefruit and its impact in systemic concentration of several drugs [38,41,42,43]. Overall, DFIs can occur during the habitual use of certain foods whose components can modify pharmacological processes and pathways that take place in the body for drugs. These pathways can be related with the absorption, distribution, metabolism, and elimination processes (pharmacokinetic drug-food interactions, PK-DFIs) or with biological pathways related with the main—or secondary—pharmacological action of a drug (pharmacodynamic drug-food interactions, PD-DFIs) [44,45].
The aim of this review is to summarize available knowledge regarding DFIs focusing mostly on products that are included within Med-D diet. The analysis focuses on the most common and known food products considering cultural, ethnic, agricultural variations among the regions around Mediterranean area which account for alterations in Med-D dietary habits. The level of evidence is following the general principle of evidence pyramid characterized as: (i) “theoretical” if mechanisms can be proposed; (ii) “low” if in vitro data are available; (iii) “moderate” if in vivo data are available; (iv) “good” if the DFI is observed clinically and (v) “high” if the level of evidence is adequate with randomized clinical studies and other data sources available [46,47,48,49]. The review is structured to present initially general pharmacological mechanisms of potentially clinically significant DFIs with some characteristic examples. Subsequently available scientific data and the level of evidence regarding DFIs between Med-D foods and drugs are presented and discussed. The potential impact of heavy metal or other pollutants is not included.
2. Pharmacological Mechanisms of Drug-Food Interactions
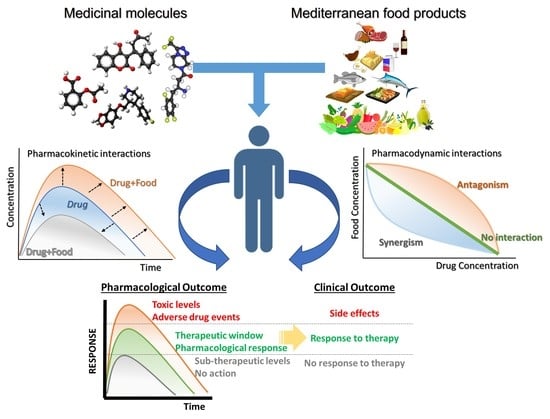
Pharmacological mechanisms of DFIs include the influence of PK processes and/or the PD effect of drugs in organs and secondary tissues (Figure 1). For a DFI to have a clinically significant impact it must modulate the pharmacological profile of a drug out of its therapeutic window. For example, in cases of PK-DFIs, one or more constituents of a food product must increase or decrease drug’s concentration out of the minimum or maximum effective concentration, respectively, and/or change the time of drugs action. (Figure 2). Therefore, clinically significant DFIs occur when one or more food constituents are (i) contained in fair and consistent amounts in the product; (ii) can reach systemic circulation and biological ways in adequate concentrations and (iii) modulate meaningfully the drug’s pharmacological action [50,51].
2.1. Pharmacokinetic Drug-Food Interactions (PK-DFIs)
2.1.1. Absorption
Drug’s absorption—for orally administered drugs—is determined by its physicochemical properties, formulation, the capability of transportation (active or passive) across epithelial cells in the gastro-intestinal (GI) tract and the administration during fasted/fed state (Figure 3) [52]. Any modulation of intestinal transit time can change the drug’s bioavailability—the fraction that reaches systemic circulation—and alter its systemic concentration. This is very important for drugs with reduced aqueous solubility but sufficient permeability [53,54]. Dietary compounds can modulate absorption either through biological activities or due to physicochemical mechanisms that change GI-environment, thus altering the biopharmaceutical properties of a drug formulation. For example, radish extract has been shown to stimulate GI motility in vitro through activation of muscarinic pathways [55]. Oat brans and fibers, although assisting in lowering cholesterol, also inhibit the intestinal absorption of statins, altering their PD properties, thus concurrent administration and consumption is proposed to be avoided or limited [56,57]. High-fat diets may lead in raised bile salt secretion which may increase the solubilization and absorption of lipophilic drugs such as anticancer drugs pazopanib, vemurafenib and lapatinib [58,59]. Generally the impact of fasted/fed state seems to be an important factor for orally administered drugs and especially for drugs used in oncology [60,61]. Thus, it is important relative information to be placed on drug labels since certain foods can change the pH in the stomach, alter the solubility, delay gastric emptying, change the stimulation of bile and blood flow, create unabsorbed chelate ligands, or change the gut microflora [50,62].
Following dispersion and dissolution in the GI track, a drug molecule is transported across epithelial GI-cells to the portal vein through active transport. Drug carriers can be classified into two major superfamilies, (i) ATP-binding cassette (ABC) transporters with efflux activity and (ii) solute carrier (SLC) transporters with influx activity [63,64,65,66,67]. P-glycoprotein (P-gp) is the most well-known efflux carrier regulating the absorption of drugs (i.e., anticancer, immunosuppressants, cardiovascular and lipid-modifying agents, antivirals, antibiotics, antiepileptics). Additional efflux transporters are: (i) the breast cancer resistance protein (BCRP) alleged to prevent absorption of toxic compounds and regulate the absorption of chemotherapeutics, and drugs such as prazosin, glyburide, cimetidine, sulfasalazine, rosuvastatin etc.; and (ii) the multidrug resistance-associated protein 2 (MRP2) that plays a role in the absorption of chemotherapeutic products [64,66,67]. Regarding influx transport, it is regulated by SLCs superfamily and includes a wide number of carriers such as organic anion transporters proteins (OATPs); organic cation transporters (OCTs); proton-dependent oligopeptide transporters (PEPTs); plasma membrane monoamine transporters (PMATs); and the monocarboxylate transporters (MCTs), all of which have been shown to play roles in drug transport across cell membranes [65,67].
Constituents of food products and DS can influence transporter’s activity [68,69,70,71]. The efflux activity of P-gp has been shown in vitro to be inhibited from rosemary extracts, orange juices, strawberry and apricot extracts, dietary fatty acids, mint extracts, and spices constituents found in black pepper (piperine), chili peppers (capsaicin), and sesame oil (sesamin) [72]. Flavonoids such as quercetin, rutin, genistein, and silymarin, and terpenoids such as glycyrrhetinic acid are typical examples inhibiting activity in P-gp and in some cases for BCRP [73,74,75,76]. Green tea beverages have been shown in vivo to inhibit hepatic OATP2 reducing hepatic drug uptake and increase plasma exposure to atorvastatin [77].
2.1.2. Distribution
Drug distribution describes the reversible transfer of a drug from the blood to organs through vascular permeability into interstitial-intracellular space, and from there inside the cells [78]. Drug’s physicochemical properties, plasma and/or tissue protein binding, tissue composition and the presence of several barriers (i.e., blood-brain barrier) are factors that play roles in distribution [79]. Drug’s distribution is often related with the volume of distribution (Vd). It is defined as the apparent volume in which the existing amount of drug in the body must be dissolved to give its measured plasma concentration. Low Vd values are for drugs that remain mainly in plasma while high values are for lipophilic molecules that are distributed in tissues with high body-fat (i.e., CNS drugs). Regarding drugs in plasma, they are either bound (fb) or unbound (fu) to plasma proteins (i.e., human serum albumin (HAS), a1-acid-glycoprotein) depending on their affinity with them. This is important since only unbound drugs are distributed in the tissues and give the pharmacological action, as well as are eliminated. Protein binding is a site of potential drug interactions and alteration of protein binding can be significant in cases of fu < 0.05, low Vd (high plasma concentration) and narrow therapeutic index (NTI) [80]. For example, if a drug with fu = 0.05 changes it to fu = 0.1 and no added elimination occurs, the drug will double its action which can potentially lead in ADRs. Phenolic derivatives (i.e., flavonoids, phenolic acids, anthocyanidins, gallic acid derivatives, stilbene derivatives etc.) can form reversible complexes with plasma proteins such as albumin [81,82]. Flavonoids such as baicalin, rutin and quercetin that are found in several DS have been suggested to alter the albumin binding of drugs such as theophylline, nifedipine, promethazine, and ticagrelor [82]. As far as displacement of warfarin, experimental results vary from no risk up to clinically significant DFIs. For DFIs in protein binding with warfarin, an allosteric alteration of different binding regions is proposed, but the interaction is a minor one due also to the fact that S-warfarin (the active enantiomer) has lower protein binding [83].
2.1.3. Metabolism
Metabolic transformation of drugs occurs through a series of pathways in the liver and is divided in two phases (phase I and phase II) (Figure 2). Phase I reactions encompass the formation, or the modification of a functional group through oxidation, reduction, or hydrolysis while phase II are conjugation reactions.
Cytochromes P450 (CYPs) are responsible for 80% of the total phase I oxidation reactions [84]. Of the total 18 CYP families described in humans, the first three participate the most in drug metabolism. Variations in CYP genes among individuals results in phenotypes of different metabolic activity and usually classifying them as ultra-rapid, extensive, intermediate, and poor metabolizers [85,86,87]. CYP2D6 is the most recognized example regarding inter-individual and inter-population variability regarding phenotypes [88]. Pharmacogenetic testing for CYP2D6 has become an important clinical aspect of personalized therapy, especially since it is responsible for the metabolism of 20–25% of drugs such as CNS and cardiovascular medications [87,88]. This unique characteristic of CYP2D6 often makes it a focus point for potential drug interactions, including DFIs. CYP3A subfamily is the most abundant isoenzyme that plays role in drugs pharmacokinetics. CYP3A isoenzymes (CYP3A4 and CYP3A5) are expressed in the small intestine and the liver, and their metabolic activity accounts for 70–75% of drug metabolism [86]. Over the previous years it has become evident that CYP3A4 and P-gp play complementary roles for absorption, disposition, and metabolism processes. Hence, in many cases, interaction mechanisms for drugs often include both biological pathways of transport and metabolism [89].
The roles of food products in drug metabolism have been extensively evaluated [51]. St John’s Wort (SJW) is a well-known example of DS involved in drug interactions through CYP3A4 and P-g. SJW has been promoted as a well-documented natural antidepressant supplement after long term use [90]. SJW’s constituents (mainly hyperforin) can initially inhibit and subsequently induce the expression of CYP3A in the liver as well as induce the expression of P-pg [91,92]. The overall effect is an initial increase in drug exposure but the later induction of P-gp and CYP3A leads in reduced and sub-therapeutic concentration of CYP3A and P-gp substrates. The impact of SJW on P-gp and CYP3A is correlated with the hyperforin content in the product [93]. As of today there are several drug categories reported to interact with SJW such as anticancer drugs (i.e., imatinib, irinotecan, docetaxel), HIV drugs (i.e., indinavir), immunosuppressants (cyclosporine, tacrolimus), anticoagulants (i.e., coumarin analogues), cardiovascular medications and lipid modifying agents (i.e., digoxin, statins etc.), antiepileptics (i.e., carbamazepine), and oral contraceptives (i.e., levonorgestrel etc.) [92]. Hence, SJW, although promoted as a good natural antidepressant, needs special precautions when it is used form patients under therapies with NTI drugs [94].
Other important CYP enzymes are the CYP1A1 and CYP1A2, CYP2C9 and CYP2C19 that also metabolize a wide number of drugs. Polycyclic aromatic hydrocarbons (PAHs) present in tobacco are bio-transformed by CYP1A1 and CYP1A2 to oxy-derivatives, which can bind to DNA and initiate carcinogenesis. Tobacco can also induce CYP1A1 and CYP1A2 expression and modulate the systemic concentration of drugs that are substrates for these enzymes [95]. Isothiocyanates and other natural occurring polyphenols that are present in several vegetables have been shown to reduce the CYP1A enzyme activity, thus limiting the effect of PAHs [96]. CYP2C9 participates in the metabolism of coumarin anticoagulants (i.e., warfarin and acenocoumarol), thus is a site of potential interactions for anticoagulation treatment. A known case is that of gingko biloba, where ginkgolic acid I and II can inhibit CYP2C9, however the interaction is negligible [97,98].
In Phase II, metabolism transferases such as UDP-glucuronosyltransferases, sulfotransferases, N-acetyltransferases, glutathione S-transferases and methyltransferases insert hydrophilic groups to the initial drug or the formed metabolite prior to renal elimination. Dietary polyphenols found in fruits, vegetables, wine, olive oil, tea and cocoa products are potential substrates and/or inhibitors of Phase II enzymes due to the presence of hydroxylic groups (-OH) that gives them structural similarity with drugs’ metabolites. Until now, studies (mostly in vitro) have shown natural polyphenols’ potential inhibitory activities on UDP-glucuronosyltransferases. For example, molecules such as glycyrrhetinic acid (licorice), chrysin (passiflora, mushrooms), silymarin (milk thistle), quercetin (onions, apples, grapes, berries, broccoli etc.), myricetin (tomatoes, oranges, berries, red wine etc.), naringenin (citrus fruits), luteolin (celery, parsley, broccoli, onion leaves), phloretin (apples), piceatannol (passion fruit and blueberries), resveratrol (grapes, wine, grape juice) etc. have been found to exhibit inhibitory activity against UGTs thus they can play role during Phase II metabolism of drugs and possibly contribute in DFIs [99,100,101,102].
2.1.4. Elimination
Drug’s removal from the body is occurring through excretion processes for an unmetabolized drug or its metabolite. Kidneys are the main organ of drug elimination and drugs (or their metabolites) are filtered through them into the urine and excreted. A secondary pathway is through the bile where the bio-transformed drugs in the liver are excreted in the bile and eliminated through enterohepatic circulation in the feces (Figure 3). Renal elimination of drugs involves the processes of glomerular filtration (drug passive diffusion from blood stream into the urine), proximal tubular secretion, and distal tubular reabsorption from passive diffusion or active transport. For renal elimination, two factors are playing roles for potential DFIs. The first is the urinary pH since drug’s ionization—depending on the alkaline or acidic environment—plays a role in its capability to passively diffuse through membranes, trapped in ionized form and excreted, whereas the non-ionized form is re-absorbed. The second factor is the transporter-mediated interactions which can impact drugs’ elimination profile or accumulation in renal tubular cells, leading to drug-induced nephrotoxicity. Diet habits play a key role in the acidity or alkalinity of urine pH. Vegetables and fresh fruits are mostly related with alkaline diets, whereas high protein content diets usually acidify the urine [103]. An alkaline urine pH can reduce the excretion rate of weakly basic drugs and an acidic urine pH from diet may decrease the excretion amount for weakly acidic drugs. Memantine and flecainide are two characteristic examples where their elimination profile is changing based on the urine pH conditions [104,105].
2.2. Pharmacodynamic Drug-Food Interactions (PD-DFIs)
Pharmacodynamic interactions refer to modulation of the pharmacological action of a drug in the site of action or in secondary tissues that can induce ADRs and side effects. PD-DFIs are usually related with additive, synergistic, or antagonistic effects from food compounds on the pharmacological pathways of a drug. One of the most well-known DFIs is for foods containing tyramine (i.e., wine and cheese). These foods are to be avoided from patients treated with monoamine oxidase inhibitors (MAOIs) [42]. Another typical example is the potential modulation of anticoagulating action of coumarin analogues (warfarin, acenocoumarol, phenprocoumon) from vitamin K (Vit-K) [106]. Vit-K1 (dihydroquinone, KH2) is the necessary cofactor for activation of the clotting factors, thus coumarin analogues and Vit-K are antagonizing each other. Foods rich in Vit-K such as kale, collard greens, broccoli, spinach, cabbage, and lettuce should be consumed from patients under anticoagulation treatment keeping in mind potential alterations in international normalized ration (INR). The general guidance is that patients need to sustain a stable diet, so the daily intake of Vit-K must remain constant throughout their treatment [107,108]. Similarly to Vit-K, special precautions should be taken for diets rich in minerals such as Potassium (K+) in cases of cardiovascular diseases treated with K+ sparing diuretics (spironolactone, amiloride, triamterene etc.) or agents acting on the renin–angiotensin system (i.e., angiotensin-converting enzyme inhibitors, ACEs, angiotensin receptor blockers, ARBs, etc.). In this respect, fruits such as bananas, oranges, and apricots, and vegetables such as spinach, potatoes, mushrooms, and peas should be consumed keeping in mind that high intake may lead to hyperkaliemia resulting in cardiac side effects and arrhythmias [109,110].
3. Mediterranean Food Products and Potential DFIs
3.1. Med-D Food Products
Med-D allows the intake of all types of foods following a general food guidance pyramid (Figure 4) [2,3]. In its base (level 1) are vegetables, fruits, nuts, and cereals that should be consumed in greater amounts and at daily frequency. Above them (level-2), sea food proteins and omega-3-fatty acids (n-3 FAs) are suggested to be consumed biweekly. Animal food products (level3) such as dairy, cheese, and eggs can be consumed in moderate portions during the week. Red meat (level 4) should be consumed in less proportions during the week along with saturated fat products and sweets. Regarding alcohol, a moderate consumption of wine and other fermented beverages is recommended (one to two glasses with meals). The pyramid is complete considering daily activities and physical exercise. Table 1, Table 2 and Table 3 summarize available data regarding potential DFIs for food products of level1 in the Med-D pyramid.
3.2. Drug-Med Diet Interactions
3.2.1. Vegetables, Herbals, Olive Oil, Cereals, and Nuts
The Med-D has its basis in foods of plant-origin with a wide variety of vegetables along with other herbals. It contains an extensive list of domestic and imported vegetables that reached the area through historical trading routes. The most common vegetables include artichokes, arugula, asparagus, beetroots, broccoli, brussel sprouts, cabbage, carrots, celery, collard greens, cucumbers, dandelion greens, eggplant, fennel, garlic leeks, lettuce, mushrooms, mustard greens, onions (all types), peas, peppers, potatoes, pumpkin, radishes, spinach, turnips, zucchini. Case reports and clinical data suggest that potential PK-DFIs can result from consumption of artichoke, broccoli, brussel sprouts, cabbage, cauliflower, and tomatoes [111,112,113]. A pharmacological mechanism can be attributed to the isothiocyanate content (i.e., broccoli, cauliflower etc.) and their capability to modulate drugs’ CYP-mediated metabolism or transport (ABC-transporters) [112]. Especially for CYP1A2, it has been shown through clinical trial that brassica vegetables can induce CYP1A2 metabolic activity modulating caffeine’s pharmacokinetics [114]. In addition, celery and other apiaceous vegetables (i.e., carrot, celery, dill, cilantro, parsnip, parsley etc.) can decrease cytochrome CYP1A2 activity as has been shown through several studies [112,114]. Garlic components have shown inhibitory action for CYPs 2C, 2D, and 3A-mediated metabolism in vitro but in a later clinical pharmacokinetic study, long-term use of garlic caplets led to a significant decline in the plasma concentrations of saquinavir which is metabolized from CYP3A4 [115,116]. Tomato juice was shown in vitro to contain mechanism-based and competitive inhibitor(s) of CYP3A4 [117,118]. Cabbage and onion juices have also shown potential inhibiting activities on CYP3A4 in vitro [119]. Basil demonstrated in vitro potential reversible and time-dependent inhibition of CYP2B6 and CYP3A4 as well as esterase-mediated metabolism of rifampicin, but the concentrations were higher than the ones used in daily food consumption [120]. The significance of these potential PK-DFIs is currently unresolved and the level of evidence for most of the cases is low. The frequent consumption of these foods may contribute in an observed inter-individual variability within the treatment goals. A recent systematic review and meta-analysis of twenty-three dietary intervention trials in humans analyzed the effect of cruciferous vegetable-enriched diets on drug metabolism. The meta-analyses showed a significant effect on CYP1A2 and glutathione S-transferase-alpha (GSTa) [113]. Thus, healthcare advice is needed in case patients habitually consume excessive amounts of vegetables such as broccoli, brussel sprouts, cabbage, cauliflower, radish, and watercress and are under treatment with CYP1A2 substrates (i.e., clozapine, olanzapine, fluvoxamine, haloperidol, melatonin, ramelteon, tizanidine, and theophylline).
Regarding PD-DFIs, arugula, asparagus, bell peppers, broccoli, celery, collard greens, kale, onions and leeks, spinach, and chard due to their content of vitamin-K could modulate the INR for people treated with coumadin analogues such as warfarin or acenocoumarol. However, despite this, DFI represents a clinically significant case; it is estimated to be of moderate importance and has a low level of evidence with studies suggesting that a balanced consumption of vegetables does not interfere with INR in a clinically significant way [107,108]. Concerning other potential PD-DFIs, anise and aniseed’s essential oil (used to enhance the flavor of Greek Ouzo and mastic) in vivo enhanced the effects of CNS drugs (codeine, diazepam, midazolam, pentobarbital, imipramine and fluoxetine) in mice suggesting potential synergism and a clinically significant PD-DFI if it is used in extensive doses [121]. Garlic has shown promising data as an antidiabetic agent; thus it may enhance the pharmacologic effect of antidiabetic medicines [122]. Turnips have demonstrated synergism with antidiabetic drugs towards hypoglycemia while yams have a good quality of evidence for synergy with estrogens and thus special precautions should be made for patients under estrogen therapy [123,124]. Naturally occurring levodopa and carbidopa have been quantified in fava beans in fair amounts, thus patients with Parkinson’s under treatment should be aware of possible synergism with co-administered medications [125].
Concerning olive oil, its protective role against inflammation-related chronic non-communicable diseases (cardiovascular, diabetes, cancer etc.) have been described thoroughly [126]. Proposed mechanisms involve the action of bioactive constituents of olive oil on interleukin-6 (IL-6) and platelet activating factor (PAF) inflammation pathways. In particular, PAF, which is a class of lipid chemical mediators with messenger functions, has gained research attention as a potential drug target due to its involvement in inflammatory diseases such as allergies, asthma, atherosclerosis, diabetes etc. [127]. Moreover, it is a point of focus as a contributing biological mechanism for anti-inflammatory action of several food products with protective roles against inflammation [31]. Several bioactive phytochemical compounds such as terpenes and constituents in olive oil with PAF action have been related to protective mechanisms against atherosclerosis [128,129]. In addition, as of today there is no contribution of olive oil or its constituents in potential DFIs. On the other hand, for some terpenes with PAF action, i.e., cedrol, inhibiting properties against human P450 have been described in vitro and further studies are needed to clarify potential DFIs [130]. Regarding potential PD-DFIs of PAF modulators with anti-platelet medications, there are not any reports suggesting potential contribution in DFIs.
3.2.2. Fruits and Fruit Juices
The Mediterranean fruits are among the most famous and widely consumed food products globally. Apples, apricots, avocados, cherries, clementines, figs, grapefruits, grapes, melons, nectarines, oranges, peaches, pears, pomegranates, strawberries, tangerines are the most common ones that are consumed by people following the Med-D style. Regarding fruit juices, the fermentable but unfermented product obtained from the edible part of the fruit and preserved fresh, they sometimes contain (due to the extraction process) different constituents or quantities from the original fruit.
The most notorious DFI regarding fruits and/or fruit juice with medications is that of grapefruit and its juice (GFJ) [41,131,132,133]. GFJ constituents (i.e., furanocoumarins etc.) can inhibit CYP activity (mainly CYP3A) through mechanism-based inhibition as well as transporter proteins in the intestine and liver (i.e., P-gp) [131,133,134,135,136]. This can elevate drugs’ bioavailability which, along with reduction in drugs’ intrinsic clearance, can result in increased concentrations and potential side effects. Typical examples are the concomitant use of GFJ with: (i) Ca2+ channel antagonists that result in low blood pressure; (ii) HMG-CoA reductase inhibitors that may lead to rhabdomyolysis and renal impairment; and (iii) adverse pulmonary effects caused by amiodarone co-administration [41,70,131,137].
Grapefruit as a plant belongs to the plant family of Rutaceae within the genus of Citrus fruits such as lemons, oranges, limes, tangerines fruits that are widely consumed. As a result, the frequent consumption of these products alerted the previous years the scientific community to the need to examine if DFIs could be further observed [138,139,140]. Until today, the most often described mechanism for potential DFIs are related with modulation of the activity of OATP transporters and CYPs metabolic activities [141,142,143]. Citrus fruits such as orange, lemon, pomelo, and lime have been assessed for potential DFIs and compared with GFJ. Pomelo juice increased the bioavailability of cyclosporine in an open-label crossover PK study probably due to inhibition of CYP3A4 and P-gp [144]. Orange juice reduced the bioavailability of alendronate and aliskiren [145,146], whereas Seville orange juice interacts with felodipine in a similar way to GFJ [147]. Lime juice has been shown in vivo to increase (similarly to GFJ) the bioavailability and systemic concentrations of carbamazepine with a clinically significant risk for liver and kidney toxicity [148]. Although tangerine (fruit and juice) showed some effect in vitro on CYP3A4-mediated metabolism of midazolam, this was of no clinical significance [149]. Narirutin found in Citrus fruits has also been observed in vivo to inhibit OATP1A2 and OATP2B1 [150].
Regarding apple juice, there is evidence from in vitro, in vivo and clinical studies of inhibiting activity on OATPs and modulation of the PK profile of drugs such as fexofenadine, montelukast and aliskiren [142,143,146,151]. It also contributed to a DFI with atenolol in a dose-response relationship but with limited effect on the PD-profile of the drug [152]. Cranberry juice and its constituent avicularin inhibited uptake transporters OATP1A2 and AOATP2B1 in vitro [153]. In addition, in vitro data indicated inhibition of CYP-mediated metabolism (CYP2C9 and CYP3A4) similar to ketoconazole and fluconazole. The effect is mainly attributed to anthocyanins content but these compounds show poor bioavailability, thus in vitro data were not repeated in vivo or through clinical studies [154,155,156]. Pomegranate juice has demonstrated in vitro/in vivo inhibiting action against CYP2C9 and CYP3A4 but with no clinical impact based on the available clinical data [157].
Drug interactions with fruits, fruit juices or pulps can also be related with PD-DFIs, and especially for fruits that contain considerable amounts of potassium (K+). Bananas, apricots, and oranges are some typical examples of high-K+ fruits and in theory their over consumption can be implicated in potential PD-DFIs with ARBs and diuretics [109,110]. Although this effect is based in theoretical statements, an in vivo study with palm fruits and lisinopril demonstrated elevated serum K+ levels [158]. The risk of potential hyperkaliemia is clinically significant, especially in cases of kidney diseases. Although observational studies suggest that adherence to Med-D improves survival for CKD patients, there is a lack of conclusive clinical data regarding DFIs and hyperkaliemia, hence vigilance should be advised from healthcare providers [159,160].
3.2.3. Fish and Sea Food
Fish and sea food (clams, cockles, crabs, groupers, lobsters, mackerel, mussels, octopuses, oysters, salmons, sardines, sea basses, shrimps, squids, sea breams, tunas, etc.) are the main sources of protein and fat within the Med-D diet. They contain high amounts of essential amino acids along with n-3 fatty acids (FA) (i.e., eicosapentaenoic acid and docosahexaenoic acid) especially the pelagic fishes (sardines, anchovies, mackerels etc.) [161]. Apart of the nutritional value in Med-D, marine n-3 FAs are known to have positive effects on human health such as a protecting role in cardiovascular diseases, inflammation, diabetes, neurocognitive disorders etc. [162]. Regarding DFIs, omega-3 FAs seem to reduce coagulation factors (i.e., fibrinogen and prothrombin), thus in theory can potentiate the effects of anticoagulants [163]. As of today there have been some case reports of interactions between warfarin co-administration with fish-oil supplements, but the results were not repeated in a retrospective study of a larger cohort of patients with atrial fibrillation and deep vein thrombosis [164,165,166]. Considering also that DS usually have a higher content of n-3 FAs than the consumed food, the potential DFI is of minor importance and negligible for patients that remain adherent in their treatment plan.
3.2.4. Milk Dairy Products, White and Red Meat
Milk and dairy products (yoghurt, cheese) are part of the traditional domestic livestock practices around the Mediterranean basin and are part of the historical heritage of the dietary habits for the region. In medicine, milk and dairy products are an old case of potential DFIs due to their content in Ca2+ and tyramine. The presence of Ca2+ in milk and dairy products can create unabsorbed chelate ligands with antibiotic classes of tetracyclines and quinolones resulting in reduced bioavailability (PK-DFIs) [62]. Tyramine is a precursor of catecholamines and the inhibition of their metabolism from MAOIs can lead to increased catecholamine levels which can cause hypertension. Tyramine is known to interact with mono-amino oxidase inhibitors (MAOIs) resulting in an effect known as tyramine pressor response with high blood pressure and risk of cerebral hemorrhage which can be fatal [42,167]. Finally, another important PK-DFI is the reduced bioavailability of ferrous from cow milk. Caseins in cow milk bind Fe2+ by clusters of phosphoserines, keeping it soluble in GI’s alkaline pH, preventing its free form from being available for absorption, thus decreasing its bioavailability in cases of ferrous supplement co-administration [168]. In addition, co-administration of mercaptopurine and cow milk in patients with chronic myelogenous leukemias reduces the bioavailability of the drug due to milk’s high content of xanthine oxidase, thus this co-administration should be avoided [169,170].
Meat products within Med-D, although consumed to a limited extent, are a valuable source of nutrients for a healthy and balanced diet. Their dietary value lies in their high protein content with essential amino acids, ferrous from red meat, vitamin B12 and other vitamins of B-complex, zinc, selenium, and phosphorus. Fat content is dependent on meat species, feeding system, as well as the meat part that is used in food [171]. As stated earlier, high-fat content may lead to raised salt and increase the solubilization of lipophilic drugs [38].
3.2.5. Wine and Other Beverages
Wines, except for their alcohol content (~11% for whites and 15% for reds), have a rich composition of bioactive compounds such as polyphenols. Resveratrol, anthocyanins, catechins, and tannins (proanthocyanins and ellagitannins) are some of the most often found polyphenols with a higher content in red wines which also explicate the beneficial effect of from wine consumption [172,173]. One of the most known examples is the French paradox, the epidemiological observation of low coronary heart disease death rates despite high intake of dietary cholesterol and saturated fat in southern France which is attributed in red wine consumption in those populations [174]. Regarding DFIs, polyphenols can modulate the phase I and II metabolism as stated earlier but for wine this effect can be considered minimal compared to the effects of alcohol in the case of regular or heavy drinking.
Alcohol can enhance the effects of medications, especially in cases of chronic conditions. PK-DFIs of alcohol are related mostly with induction of CYP2E1 and to a lesser extent CYP3A3 and CYP2A1. Heavy alcohol drinking can lead to PD-DFIs of alcohol such as sedation when combined with CNS acting drugs (sedatives, antihistamines, antidepressants, antipsychotics etc.), induce gastric bleeding when combined with aspirin and relative painkillers or anticoagulants, and hypoglycemia with antidiabetic drugs [43,175]. Regarding the vexed issue, the widespread opinion that concomitant drink of alcohol with antibiotics or other antimicrobials will cause toxicity or treatment failure, a recent review of the available evidence suggested that the data are poor and sometimes controversial [176]. The reduced efficacy refers mostly to erythromycin and doxycycline. Disulfiram-like reaction (distress, pain, flushes, irregular heartbeat) can occurs in co-administration of metronidazole, ketoconazole, griseofulvin and cephalosporines (i.e., cefuroxime, cefotetan, ceftriaxone, cefoperazone, ceftriazone). Ambiguous data for ADRs exist for trimethoprim sulfamethoxazole. On the other hand, penicillins, fluoroquinolones, azithromycin, tetracyclines, nitrofurantoin, secnidazole, tinidazole, and fluconazole have not been causally related to ADRs [176]. Another mechanism involved is the reduction in the immune response and epidemiological studies have shown alcohol abuse to be associated with an increased incidence of infectious diseases. But this is related mostly to cases of alcohol abuse, consumption of high content alcoholic drinks and overall, a poor quality of life regarding well-being and disease prevention. Thus, it is a good idea from the healthcare perspective, especially for heavy-drinking patients under treatment, to advise towards drinking cessation [177,178]. On the other hand, the moderate consumption of red wine seems to be beneficial in cases of immune protection due to its polyphenol content [177]. Thus, although the quality and quantity of data are vague, the avoidance of or reduction in consuming alcohol in low or moderate amounts (e.g., a social occasion with one glass of wine or beer) as is suggested through Med-D can be enjoyed.
4. Discussion
It is of no debate that a healthy diet and nutrition is essential for good health and shields from several chronic non-communicable diseases, such as cardiovascular heart disease, diabetes, CNS disorders, autoimmune disease and cancer [11,17,22,26,31,163,179,180] Thus, in the context of optimum healthcare provision is important to support patients as well as the general population to embrace a healthier balanced diet and remain adherent and compliant to it along with their medication [181]. Healthcare providers should be able to educate patients and in the context of precision medicine era, to individualize their consultation so as to empower patients to improve their health and well-being [182,183,184].
Med-D remains one of the most valuable and widely studied dietary habits for promoting well-being. The clinical evidence supports that long-term adherence to Med-D is valuable against metabolic disorders and cardiovascular diseases. Numerous studies demonstrate the anti-inflammatory and anti-oxidative properties of constituents found within the Med-D foods against risk factors and pathophysiological mechanisms lowering the risk for developing most of the major non-communicable disorders [2,6,8,23,28,185,186]. All those food products and nutraceuticals that promote well-being have been the focus of research the recent years for the identification of bioactive compounds that can be related with molecular mechanisms by which dietary components promote health and prevent diseases [187,188,189]. On the other hand, these bioactive dietary compounds can share same biological mechanisms with drug molecules and interfere with pharmacological mechanisms modulating the clinical outcome due to DFIs [45].
The DFIs, although seeming to be summarized in a simple clinical question “shall I take this drug with this food?” are more than that. DFIs depend on the type and amount of food consumed on daily basis, patient’s health status, comorbidities, drug categories that are prescribed, time of drug administration and meal intake, the clinical significance of the DFI and whether it is beneficial or not [50,52]. Briguglio et al. in their work [45] described that DFIs can be categorized in three groups: (i) pharmaceutical, (ii) pharmacokinetic and (iii) pharmacodynamic based on the mechanism involved. Alternatively, four types can be considered based on the process prior to systemic concentration. Hence, pre-systemic interactions are referred to as type I ex-vivo interactions or type II modulation of enzyme (subtype a) or carriers (subtype b) and/or other deactivations in GI-track (subtype c). Post-systemic interactions are described as type III for modulation of distribution and metabolism in the body and type IV as modulation of drug’s renal or enterohepatic clearance. The latter description omits the PD-DFIs which could be considered as a type V post-systemic phase interaction.
This work aimed to provide a literature review regarding DFIs focusing on examples of foods that are included in the Med-D and discuss cases in which they can be related with significant DFIs. DFIs for Med-D food products are associated with modulation of PK processes and primarily with drugs’ first pass effect from the GI-track to reach the systemic circulation. The majority the cases discussed refer to type II and III (subtypes a and b) with the addition of PD-effects that can occur for some products (Figure 5). Absorption and metabolism are the two main processes that should be considered when the question comes to food effects for a drug and the main pathways involved are the carrier-mediated transport across membranes and/or the mediated metabolism from Phase I and Phase II enzymes [39,112]. As shown in Table 1, Table 2 and Table 3, there is a good quality of evidence that cruciferous vegetables may impact drug metabolism, and fruits (or juices) such as grapefruit, apples, pomelo, pomegranates, and Seville orange juice can modulate the PK profile of some drugs which can be clinically significant in cases of drugs with narrow therapeutic index [57,113,131,139,142]. In addition, oat brans and fibers can modulate the absorption of statins whereas the high-fat content foods can modulate the bioavailability of some orally administered cancer medications [56,57,58,59]. Regarding PD-effects, the high content in Vit-K and K+ in some vegetables and fruits can modulate the pharmacological action for coumadin analogue anticoagulants (Vit-K) and contribute to hyperkaliemia with ACEs, ARBs, and diuretics [106,109]. Although there are case reports and general literature discussion, the currently accepted scientific point of view is that patients who remain adherent and compliant to a balanced diet prior to and during any therapy initiation can keep on consuming these food products in a similar way to before [45]. They key issue here is the communication of patient with healthcare provider in case any adverse event occurs and the healthcare provider’s awareness to report it and examine whether a DFI is related with it.
In addition, for cases where the food effect is negligible, or the pharmacological effect is sustained (Figure 2), it should be noted that Med-D diet can be considered as a collaborating partner with drugs [7,10,19,180,190]. For example, it may empower patients to better manage their health status and improve biochemical disease markers (i.e., blood glucose, cholesterol etc.) thus avoiding complicated therapeutic regimens with multiple medications that also raise the risk for adverse drug events from drug-drug interactions [32,191].
Apart from the well-documented cases (Table 1, Table 2 and Table 3) there are a lot of additional examples where data are scarce, theoretical, or poor. Hence, future studies are needed to further advance our knowledge in the field of DFIs. As the research is progressing on how dietary constituents engage in body homeostasis and health status, new knowledge is emerging towards prediction of food effects on drug’s action. Increasing our understanding on PK and PD interaction mechanisms and utilization of novel experimental procedures will allow the gap on the available evidence regarding food effects on drugs to decrease. The incorporation of biomedical methods will allow the better prediction of potential interactions even through in silico methods during drug development or through big-data analysis [192,193,194]. From the citizen’s perspective, the harnessing of digital evolution in relation to health promotion also cannot go unnoticed. Patient’s oriented eHealth tools and apps are constantly emerging as means for patient empowerment to better manage their health status and well-being [195,196,197,198,199,200]. Even for Med-D, smartphone apps are available to assist people to remain adherent with the Med-D principles [201]. Moreover, a recent analysis of Android Google Play and Apple App Store Apps suggested that currently available apps can deliver information on the Med-D, but the integration of more behavioral change techniques within them is needed to expand the potential for improved adherence to Med-D [202]. Finally, eHealth evolution for patient empowerment can also assist in the dissemination of knowledge regarding DFIs, assisting patients to avoid potential interactions with DS and improve their communication with their healthcare providers [35,37,203,204].
5. Conclusions
The prediction, prevention, and management of DFIs is an essential element of optimum healthcare provision. Even for Med-D, one of the most effective diets, there can be cases where food habits may have negative impact on therapeutic outcome. Proper patient consultation is important, so they are aware to avoid any potential conflicts between administered treatment and dietary habits. Adherence to a diet program similar to the one that is proposed through Med-D and individualized patient consultation and education from healthcare providers for potential DFIs will help patients to manage their disease and their overall well-being.
Author Contributions
Conceptualization M.S.; Methodology, M.S. and A.P.; investigation M.S. and E.P.; Resources E.P.; writing—original draft preparation M.S., writing review and editing M.S. and A.P.; Visualization M.S.; Supervision, A.P.; project administration E.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Martínez-González, M.Á.; Hershey, M.S.; Zazpe, I.; Trichopoulou, A. Transferability of the Mediterranean Diet to Non-Mediterranean Countries. What Is and What Is Not the Mediterranean Diet. Nutrients 2017, 9, 1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean Diet Pyramid: A Cultural Model for Healthy Eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean Diet Pyramid Today. Science and Cultural Updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations Educational, S. and C.O. The Mediterranean Diet. Intangible Heritage. Available online: https://www.unesco.org/archives/multimedia/document-1680-eng-2 (accessed on 8 August 2022).
- Wright, C.M. Biographical Notes on Ancel Keys and Salim Yusuf: Origins and Significance of the Seven Countries Study and the INTERHEART Study. J. Clin. Lipidol. 2011, 5, 434–440. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.N.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and Potential Health Benefits of the Mediterranean Diet: Views from Experts around the World. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [Green Version]
- El Amrousy, D.; Elashry, H.; Salamah, A.; Maher, S.; Abd-Elsalam, S.M.; Hasan, S. Adherence to the Mediterranean Diet Improved Clinical Scores and Inflammatory Markers in Children with Active Inflammatory Bowel Disease: A Randomized Trial. J. Inflamm. Res. 2022, 15, 2075–2086. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [Green Version]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in Children and Adolescents: A Systematic Review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef]
- García-Fernández, E.; Rico-Cabanas, L.; Estruch, R.; Estruch, R.; Estruch, R.; Bach-Faig, A. Mediterranean Diet and Cardiodiabesity: A Review. Nutrients 2014, 6, 3474–3500. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean Diet and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses of Observational Studies and Randomised Trials. Eur. J. Clin. Nutr. 2017, 72, 30–43. [Google Scholar] [CrossRef]
- Du, H.; Cao, T.; Lu, X.; Zhang, T.; Luo, B.; Li, Z. Mediterranean Diet Patterns in Relation to Lung Cancer Risk: A Meta-Analysis. Front. Nutr. 2022, 9, 844382. [Google Scholar] [CrossRef]
- Bayán-Bravo, A.; Banegas, J.R.; Donat-Vargas, C.; Sandoval-Insausti, H.; Gorostidi, M.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. The Mediterranean Diet Protects Renal Function in Older Adults: A Prospective Cohort Study. Nutrients 2022, 14, 432. [Google Scholar] [CrossRef]
- Forsyth, C.; Kouvari, M.; D’Cunha, N.M.; Georgousopoulou, E.N.; Panagiotakos, D.B.; Mellor, D.D.; Kellett, J.; Naumovski, N. The Effects of the Mediterranean Diet on Rheumatoid Arthritis Prevention and Treatment: A Systematic Review of Human Prospective Studies. Rheumatol. Int. 2018, 38, 737–747. [Google Scholar] [CrossRef]
- Morales-Ivorra, I.; Romera-Baures, M.; Roman-Viñas, B.; Serra-Majem, L. Osteoarthritis and the Mediterranean Diet: A Systematic Review. Nutrients 2018, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-Style Diet for the Primary and Secondary Prevention of Cardiovascular Disease; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2019; Volume 2019. [Google Scholar]
- García-Casares, N.; Fuentes, P.G.; Barbancho, M.Á.; López-Gigosos, R.; García-Rodríguez, A.; Gutiérrez-Bedmar, M. Alzheimer’s Disease, Mild Cognitive Impairment and Mediterranean Diet. A Systematic Review and Dose-Response Meta-Analysis. J. Clin. Med. 2021, 10, 4642. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Chrysoula, L.; Leonida, I.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to the Mediterranean Diet on Blood Pressure: A Systematic Review and Meta-Analysis of Observational Studies. Clin. Nutr. 2021, 40, 5771–5780. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Chrysoula, L.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2021, 13, 1514. [Google Scholar] [CrossRef]
- Finicelli, M.; Di Salle, A.; Galderisi, U.; Peluso, G. The Mediterranean Diet: An Update of the Clinical Trials. Nutrients 2022, 14, 2956. [Google Scholar] [CrossRef]
- Castro-Espin, C.; Agudo, A. The Role of Diet in Prognosis among Cancer Survivors: A Systematic Review and Meta-Analysis of Dietary Patterns and Diet Interventions. Nutrients 2022, 14, 348. [Google Scholar] [CrossRef]
- Rufino-Palomares, E.E.; Pérez-Jiménez, A.; García-Salguero, L.; Mokhtari, K.; Reyes-Zurita, F.J.; Peragón-Sánchez, J.; Lupiáñez, J.A. Nutraceutical Role of Polyphenols and Triterpenes Present in the Extracts of Fruits and Leaves of Olea Europaea as Antioxidants, Anti-Infectives and Anticancer Agents on Healthy Growth. Molecules 2022, 27, 2341. [Google Scholar] [CrossRef]
- Caponio, G.R.; Lippolis, T.; Tutino, V.; Gigante, I.; De Nunzio, V.; Milella, R.A.; Gasparro, M.; Notarnicola, M. Nutraceuticals: Focus on Anti-Inflammatory, Anti-Cancer, Antioxidant Properties in Gastrointestinal Tract. Antioxidants 2022, 11, 1274. [Google Scholar] [CrossRef]
- Abenavoli, L.; Procopio, A.C.; Paravati, M.R.; Costa, G.; Milić, N.; Alcaro, S.; Luzza, F. Mediterranean Diet: The Beneficial Effects of Lycopene in Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2022, 11, 3477. [Google Scholar] [CrossRef]
- Scoditti, E.; Capurso, C.; Capurso, A.; Massaro, M. Vascular Effects of the Mediterranean Diet-Part II: Role of Omega-3 Fatty Acids and Olive Oil Polyphenols. Vascul. Pharmacol. 2014, 63, 127–134. [Google Scholar] [CrossRef]
- Massaro, M.; Scoditti, E.; Carluccio, M.A.; De Caterina, R. Nutraceuticals and Prevention of Atherosclerosis: Focus on Omega-3 Polyunsaturated Fatty Acids and Mediterranean Diet Polyphenols. Cardiovasc. Ther. 2010, 28, e13–e19. [Google Scholar] [CrossRef] [Green Version]
- Augimeri, G.; Bonofiglio, D. The Mediterranean Diet as a Source of Natural Compounds: Does It Represent a Protective Choice against Cancer? Pharmaceuticals 2021, 14, 920. [Google Scholar] [CrossRef]
- Vivancos, M.; Moreno, J.J. Effect of Resveratrol, Tyrosol and Beta-Sitosterol on Oxidised Low-Density Lipoprotein-Stimulated Oxidative Stress, Arachidonic Acid Release and Prostaglandin E2 Synthesis by RAW 264.7 Macrophages. Br. J. Nutr. 2008, 99, 1199–1207. [Google Scholar] [CrossRef] [Green Version]
- Roman, G.C.; Jackson, R.E.; Gadhia, R.; Roman, A.N.; Reis, J. Mediterranean Diet: The Role of Long-Chain Omega-3 Fatty Acids in Fish; Polyphenols in Fruits, Vegetables, Cereals, Coffee, Tea, Cacao and Wine; Probiotics and Vitamins in Prevention of Stroke, Age-Related Cognitive Decline, and Alzheimer Disease. Rev. Neurol. 2019, 175, 724–741. [Google Scholar] [CrossRef]
- Nadtochiy, S.M.; Redman, E.K. Mediterranean Diet and Cardioprotection: The Role of Nitrite, Polyunsaturated Fatty Acids, and Polyphenols. Nutrition 2011, 27, 733–744. [Google Scholar] [CrossRef] [Green Version]
- Nomikos, T.; Fragopoulou, E.; Antonopoulou, S.; Panagiotakos, D.B. Mediterranean Diet and Platelet-Activating Factor: A Systematic Review. Clin. Biochem. 2018, 60, 1–10. [Google Scholar] [CrossRef]
- Chatsisvili, A.; Sapounidis, I.; Pavlidou, G.; Zoumpouridou, E.; Karakousis, V.A.; Spanakis, M.; Teperikidis, L.; Niopas, I. Potential Drug-Drug Interactions in Prescriptions Dispensed in Community Pharmacies in Greece. Pharm. World Sci. 2010, 32, 187–193. [Google Scholar] [CrossRef]
- Kohler, G.I.; Bode-Boger, S.M.; Busse, R.; Hoopmann, M.; Welte, T.; Boger, R.H. Drug-Drug Interactions in Medical Patients: Effects of in-Hospital Treatment and Relation to Multiple Drug Use. Int. J. Clin. Pharmacol. Ther. 2000, 38, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Dechanont, S.; Maphanta, S.; Butthum, B.; Kongkaew, C. Hospital Admissions/Visits Associated with Drug-Drug Interactions: A Systematic Review and Meta-Analysis. Pharmacoepidemiol. Drug Saf. 2014, 23, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Spanakis, M.; Spanakis, E.G.; Kondylakis, H.; Sfakianakis, S.; Genitsaridi, I.; Sakkalis, V.; Tsiknakis, M.; Marias, K. Addressing drug-drug and drug-food interactions through personalized empowerment services for healthcare. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS 2016), Orlando, FL, USA, 16–20 August 2016. [Google Scholar]
- Vizirianakis, I.S.; Spanakis, M.; Termentzi, A.; Niopas, I.; Kokkalou, E. Clinical and Pharmacogenomic Assessment of Herb-Drug Interactions to Improve Drug Delivery and Pharmacovigilance. In Plants in Traditional and Modern Medicine: Chemistry and Activity; Kokkalou, E., Ed.; Transworld Research Network: Kerala, India, 2010; ISBN 978-81-7895-432-5. [Google Scholar]
- Spanakis, M.; Sfakianakis, S.; Sakkalis, V.; Spanakis, E.G. PharmActa: Empowering Patients to Avoid Clinical Significant Drug(-)Herb Interactions. Medicines 2019, 6, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, M.; Coimbra, M.A.; Costa, M.D.C.; Ramos, F. Food supplement vitamins, minerals, amino-acids, fatty acids, phenolic and alkaloid-based substances: An overview of their interaction with drugs. Crit. Rev. Food Sci. Nutr. 2021, 1–35. [Google Scholar] [CrossRef]
- Won, C.S.; Oberlies, N.H.; Paine, M.F. Mechanisms Underlying Food-Drug Interactions: Inhibition of Intestinal Metabolism and Transport. Pharmacol. Ther. 2012, 136, 186. [Google Scholar] [CrossRef] [Green Version]
- Frankel, E.H.; McCabe, B.J.; Wolfe, J.J. Handbook of Food-Drug Interactions; CRC Press: Boca Raton, FL, USA, 2003; ISBN 1135504571. [Google Scholar]
- Kirby, B.J.; Unadkat, J.D. Grapefruit Juice, a Glass Full of Drug Interactions? Clin. Pharmacol. Ther. 2007, 81, 631–633. [Google Scholar] [CrossRef]
- Brown, C.; Taniguchi, G.; Yip, K. The Monoamine Oxidase Inhibitor-Tyramine Interaction. J. Clin. Pharmacol. 1989, 29, 529–532. [Google Scholar] [CrossRef]
- Chan, L.N.; Anderson, G.D. Pharmacokinetic and Pharmacodynamic Drug Interactions with Ethanol (Alcohol). Clin. Pharmacokinet. 2014, 53, 1115–1136. [Google Scholar] [CrossRef]
- Amadi, C.N.; Mgbahurike, A.A. Selected Food/Herb-Drug Interactions: Mechanisms and Clinical Relevance. Am. J. Ther. 2018, 25, e423–e433. [Google Scholar] [CrossRef]
- Briguglio, M.; Hrelia, S.; Malaguti, M.; Serpe, L.; Canaparo, R.; Dell’Osso, B.; Galentino, R.; De Michele, S.; Dina, C.Z.; Porta, M.; et al. Food Bioactive Compounds and Their Interference in Drug Pharmacokinetic/Pharmacodynamic Profiles. Pharmaceutics 2018, 10, 277. [Google Scholar] [CrossRef]
- Spanakis, M.; Patelarou, A.; Patelarou, E.; Tzanakis, N. Drug Interactions for Patients with Respiratory Diseases Receiving COVID-19 Emerged Treatments. Int. J. Environ. Res. Public Health 2021, 18, 1711. [Google Scholar] [CrossRef]
- Spanakis, M.; Roubedaki, M.; Tzanakis, I.; Zografakis-Sfakianakis, M.; Patelarou, E.; Patelarou, A. Impact of Adverse Drug Reactions in Patients with End Stage Renal Disease in Greece. Int. J. Environ. Res. Public Health 2020, 17, 9101. [Google Scholar] [CrossRef]
- Spanakis, M.; Melissourgaki, M.; Lazopoulos, G.; Patelarou, A.E.; Patelarou, E. Prevalence and Clinical Significance of Drug–Drug and Drug–Dietary Supplement Interactions among Patients Admitted for Cardiothoracic Surgery in Greece. Pharmaceutics 2021, 13, 239. [Google Scholar] [CrossRef]
- Murad, M.H.; Asi, N.; Alsawas, M.; Alahdab, F. New Evidence Pyramid. Evid. Based Med. 2016, 21, 125–127. [Google Scholar] [CrossRef] [Green Version]
- Deng, J.; Zhu, X.; Chen, Z.; Fan, C.H.; Kwan, H.S.; Wong, C.H.; Shek, K.Y.; Zuo, Z.; Lam, T.N. A Review of Food-Drug Interactions on Oral Drug Absorption. Drugs 2017, 77, 1833–1855. [Google Scholar] [CrossRef]
- Koziolek, M.; Alcaro, S.; Augustijns, P.; Basit, A.W.; Grimm, M.; Hens, B.; Hoad, C.L.; Jedamzik, P.; Madla, C.M.; Maliepaard, M.; et al. The Mechanisms of Pharmacokinetic Food-Drug Interactions—A Perspective from the UNGAP Group. Eur. J. Pharm. Sci. 2019, 134, 31–59. [Google Scholar] [CrossRef]
- Schmidt, L.E.; Dalhoff, K. Food-Drug Interactions. Drugs 2012, 62, 1481–1502. [Google Scholar] [CrossRef]
- Wu, C.Y.; Benet, L.Z. Predicting Drug Disposition via Application of BCS: Transport/Absorption/Elimination Interplay and Development of a Biopharmaceutics Drug Disposition Classification System. Pharm. Res. 2005, 22, 11–23. [Google Scholar] [CrossRef]
- Sharma, S.; Prasad, B. Meta-Analysis of Food Effect on Oral Absorption of Efflux Transporter Substrate Drugs: Does Delayed Gastric Emptying Influence Drug Transport Kinetics? Pharmaceutics 2021, 13, 1035. [Google Scholar] [CrossRef]
- Jung, K.Y.; Choo, Y.K.; Kim, H.M.; Choi, B.K. Radish Extract Stimulates Motility of the Intestine via the Muscarinic Receptors. J. Pharm. Pharmacol. 2000, 52, 1031–1036. [Google Scholar] [CrossRef]
- Eussen, S.R.B.M.; Rompelberg, C.J.M.; Andersson, K.E.; Klungel, O.H.; Hellstrand, P.; Öste, R.; Van Kranen, H.; Garssen, J. Simultaneous Intake of Oat Bran and Atorvastatin Reduces Their Efficacy to Lower Lipid Levels and Atherosclerosis in LDLr-/- Mice. Pharmacol. Res. 2011, 64, 36–43. [Google Scholar] [CrossRef]
- Vaquero, M.P.; Muniz, F.J.S.; Redondo, S.J.; Oliván, P.P.; Higueras, F.J.; Bastida, S. Major Diet-Drug Interactions Affecting the Kinetic Characteristics and Hypolipidaemic Properties of Statins. Nutr. Hosp. 2010, 25, 193–206. [Google Scholar]
- Willemsen, A.E.C.A.B.; Lubberman, F.J.E.; Tol, J.; Gerritsen, W.R.; Van Herpen, C.M.L.; Van Erp, N.P. Effect of Food and Acid-Reducing Agents on the Absorption of Oral Targeted Therapies in Solid Tumors. Drug Discov. Today 2016, 21, 962–976. [Google Scholar] [CrossRef]
- Lewis, L.D.; Koch, K.M.; Reddy, N.J.; Cohen, R.B.; Lewis, N.L.; Whitehead, B.; Mackay, K.; Stead, A.; Beelen, A.P. Effects of Food on the Relative Bioavailability of Lapatinib in Cancer Patients. J. Clin. Oncol. 2009, 27, 1191–1196. [Google Scholar] [CrossRef]
- Kang, S.P.; Ratain, M.J. Inconsistent Labeling of Food Effect for Oral Agents across Therapeutic Areas: Differences between Oncology and Non-Oncology Products. Clin. Cancer Res. 2010, 16, 4446–4451. [Google Scholar] [CrossRef] [Green Version]
- Omachi, F.; Kaneko, M.; Iijima, R.; Watanabe, M.; Itagaki, F. Relationship between the Effects of Food on the Pharmacokinetics of Oral Antineoplastic Drugs and Their Physicochemical Properties. J. Pharm. Health Care Sci. 2019, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.; Perergina, A.A.; Rodriguez, J.M.; Moreno- Esparza, R. The Influence of Coffee with Milk and Tea with Milk on the Bioavailability of Tetracycline. Biopharm. Drug Dispos. 1997, 18, 459–463. [Google Scholar] [CrossRef]
- Estudante, M.; Morais, J.G.; Soveral, G.; Benet, L.Z. Intestinal Drug Transporters: An Overview. Adv. Drug Deliv. Rev. 2013, 65, 1340–1356. [Google Scholar] [CrossRef]
- Terada, T.; Hira, D. Intestinal and Hepatic Drug Transporters: Pharmacokinetic, Pathophysiological, and Pharmacogenetic Roles. J. Gastroenterol. 2015, 50, 508–519. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Yee, S.W.; Kim, R.B.; Giacomini, K.M. SLC transporters as therapeutic targets: Emerging opportunities. Nat. Rev. Drug Discov. 2015, 14, 543–560. [Google Scholar] [CrossRef] [Green Version]
- Giacomini, K.M.; Huang, S.M.; Tweedie, D.J.; Benet, L.Z.; Brouwer, K.L.R.; Chu, X.; Dahlin, A.; Evers, R.; Fischer, V.; Hillgren, K.M.; et al. Membrane Transporters in Drug Development. Nat. Rev. Drug Discov. 2010, 9, 215–236. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liu, K. The Transporters of Intestinal Tract and Techniques Applied to Evaluate Interactions between Drugs and Transporters. Asian J. Pharm. Sci. 2013, 8, 151–158. [Google Scholar] [CrossRef] [Green Version]
- Glaeser, H.; Bailey, D.G.; Dresser, G.K.; Gregor, J.C.; Schwarz, U.I.; McGrath, J.S.; Jolicoeur, E.; Lee, W.; Leake, B.F.; Tirona, R.G.; et al. Intestinal Drug Transporter Expression and the Impact of Grapefruit Juice in Humans. Clin. Pharmacol. Ther. 2007, 81, 362–370. [Google Scholar] [CrossRef]
- Bailey, D.G. Fruit Juice Inhibition of Uptake Transport: A New Type of Food-Drug Interaction. Br. J. Clin. Pharmacol. 2010, 70, 645–655. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Lim, L.Y.; Chowbay, B. Herbal Modulation of P-Glycoprotein. Drug Metab. Rev. 2004, 36, 57–104. [Google Scholar] [CrossRef]
- Nakanishi, T.; Tamai, I. Interaction of Drug or Food with Drug Transporters in Intestine and Liver. Curr. Drug Metab. 2015, 16, 753–764. [Google Scholar] [CrossRef]
- Deferme, S.; Augustijns, P. The Effect of Food Components on the Absorption of P-Gp Substrates: A Review. J. Pharm. Pharmacol. 2003, 55, 153–162. [Google Scholar] [CrossRef]
- Kim, T.H.; Shin, S.; Yoo, S.D.; Shin, B.S. Effects of Phytochemical P-Glycoprotein Modulators on the Pharmacokinetics and Tissue Distribution of Doxorubicin in Mice. Molecules 2018, 23, 349. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Zhou, P.; Asenso, J.; Yang, X.D.; Wang, C.; Wei, W. Advances in Plant-Based Inhibitors of P-Glycoprotein. J. Enzyme Inhib. Med. Chem. 2016, 31, 867–881. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, A.I.; Real, R.; Pérez, M.; Mendoza, G.; Prieto, J.G.; Merino, G. Modulation of the Activity of ABC Transporters (P-Glycoprotein, MRP2, BCRP) by Flavonoids and Drug Response. J. Pharm. Sci. 2010, 99, 598–617. [Google Scholar] [CrossRef]
- Katayama, K.; Masuyama, K.; Yoshioka, S.; Hasegawa, H.; Mitsuhashi, J.; Sugimoto, Y. Flavonoids Inhibit Breast Cancer Resistance Protein-Mediated Drug Resistance: Transporter Specificity and Structure-Activity Relationship. Cancer Chemother. Pharmacol. 2007, 60, 789–797. [Google Scholar] [CrossRef]
- Yao, H.T.; Hsu, Y.R.; Li, M.L. Beverage–Drug Interaction: Effects of Green Tea Beverage Consumption on Atorvastatin Metabolism and Membrane Transporters in the Small Intestine and Liver of Rats. Membranes 2020, 10, 233. [Google Scholar] [CrossRef]
- Onetto, A.J.; Shariff, S. Drug Distribution; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Caldwell, J.; Gardner, I.; Swales, N. An introduction to drug disposition: The basic principles of absorption, distribution, metabolism, and excretion. Toxicol. Pathol. 1995, 23, 102–114. [Google Scholar] [CrossRef]
- McElnay, J.C.; D’Arcy, P.F. Protein Binding Displacement Interactions and Their Clinical Importance. Drugs 1983, 25, 495–513. [Google Scholar] [CrossRef]
- Xiao, J.; Kai, G. A Review of Dietary Polyphenol-Plasma Protein Interactions: Characterization, Influence on the Bioactivity, and Structure-Affinity Relationship. Crit. Rev. Food Sci. Nutr. 2012, 52, 85–101. [Google Scholar] [CrossRef]
- López-Yerena, A.; Perez, M.; Vallverdú-Queralt, A.; Escribano-Ferrer, E. Insights into the Binding of Dietary Phenolic Compounds to Human Serum Albumin and Food-Drug Interactions. Pharmaceutics 2020, 12, 1123. [Google Scholar] [CrossRef]
- Rimac, H.; Dufour, C.; Debeljak, Ž.; Zorc, B.; Bojić, M. Warfarin and Flavonoids Do Not Share the Same Binding Region in Binding to the IIA Subdomain of Human Serum Albumin. Molecules 2017, 22, 1153. [Google Scholar] [CrossRef] [Green Version]
- Sim, S.C.; Ingelman-Sundberg, M. The Human Cytochrome P450 (CYP) Allele Nomenclature Website: A Peer-Reviewed Database of CYP Variants and Their Associated Effects. Hum. Genomics 2010, 4, 278–281. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.F.; Liu, J.P.; Chowbay, B. Polymorphism of Human Cytochrome P450 Enzymes and Its Clinical Impact. Drug Metab. Rev. 2009, 41, 89–295. [Google Scholar] [CrossRef]
- Zanger, U.M.; Schwab, M. Cytochrome P450 Enzymes in Drug Metabolism: Regulation of Gene Expression, Enzyme Activities, and Impact of Genetic Variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef]
- Ingelman-Sundberg, M.; Sim, S.C.; Gomez, A.; Rodriguez-Antona, C. Influence of Cytochrome P450 Polymorphisms on Drug Therapies: Pharmacogenetic, Pharmacoepigenetic and Clinical Aspects. Pharmacol. Ther. 2007, 116, 496–526. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.K.; Brockmoller, J.; Broly, F.; Eichelbaum, M.; Evans, W.E.; Gonzalez, F.J.; Huang, J.D.; Idle, J.R.; Ingelman-Sundberg, M.; Ishizaki, T.; et al. Nomenclature for Human CYP2D6 Alleles. Pharmacogenetics 1996, 6, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, Y.; Huang, S.M. Scientific and Regulatory Perspectives on Metabolizing Enzyme-Transporter Interplay and Its Role in Drug Interactions: Challenges in Predicting Drug Interactions. Mol. Pharm. 2009, 6, 1766–1774. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, G.; Borrelli, F.; Ernst, E.; Izzo, A.A. St John’s Wort: Prozac from the Plant Kingdom. Trends Pharmacol. Sci. 2001, 22, 292–297. [Google Scholar] [CrossRef]
- Chrubasik-Hausmann, S.; Vlachojannis, J.; McLachlan, A.J. Understanding Drug Interactions with St John’s Wort (Hypericum Perforatum L.): Impact of Hyperforin Content. J. Pharm. Pharmacol. 2019, 71, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Madabushi, R.; Frank, B.; Drewelow, B.; Derendorf, H.; Butterweck, V. Hyperforin in St. John’s Wort Drug Interactions. Eur. J. Clin. Pharmacol. 2006, 62, 225–233. [Google Scholar] [CrossRef]
- Nicolussi, S.; Drewe, J.; Butterweck, V.; Meyer zu Schwabedissen, H.E. Clinical Relevance of St. John’s Wort Drug Interactions Revisited. Br. J. Pharmacol. 2020, 177, 1212–1226. [Google Scholar] [CrossRef]
- Soleymani, S.; Bahramsoltani, R.; Rahimi, R.; Abdollahi, M. Clinical Risks of St John’s Wort (Hypericum Perforatum) Co-Administration. Expert Opin. Drug Metab. Toxicol. 2017, 13, 1047–1062. [Google Scholar] [CrossRef]
- Van Der Weide, J.; Steijns, L.S.W.; Van Weelden, M.J.M. The Effect of Smoking and Cytochrome P450 CYP1A2 Genetic Polymorphism on Clozapine Clearance and Dose Requirement. Pharmacogenetics 2003, 13, 169–172. [Google Scholar] [CrossRef]
- Skupinska, K.; Misiewicz-Krzeminska, I.; Lubelska, K.; Kasprzycka-Guttman, T. The effect of isothiocyanates on CYP1A1 and CYP1A2 activities induced by polycyclic aromatic hydrocarbons in Mcf7 cells. Toxicol. In Vitro 2009, 23, 763–771. [Google Scholar] [CrossRef]
- Jiang, X.; Williams, K.M.; Liauw, W.S.; Ammit, A.J.; Roufogalis, B.D.; Duke, C.C.; Day, R.O.; McLachlan, A.J. Effect of Ginkgo and Ginger on the Pharmacokinetics and Pharmacodynamics of Warfarin in Healthy Subjects. Br. J. Clin. Pharmacol. 2005, 59, 425. [Google Scholar] [CrossRef]
- Von Moltke, L.L.; Weemhoff, J.L.; Bedir, E.; Khan, I.A.; Harmatz, J.S.; Goldman, P.; Greenblatt, D.J. Inhibition of Human Cytochromes P450 by Components of Ginkgo Biloba. J. Pharm. Pharmacol. 2004, 56, 1039–1044. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, L.; Duan, L.; Wu, J.J.; Hu, M.; Liu, Z.Q.; Wang, C. yan Potential of Herb-Drug/Herb Interactions between Substrates and Inhibitors of UGTs Derived from Herbal Medicines. Pharmacol. Res. 2019, 150, 104510. [Google Scholar] [CrossRef]
- Li, X.; Wang, C.; Chen, J.; Hu, X.; Zhang, H.; Li, Z.; Lan, B.; Zhang, W.; Su, Y.; Zhang, C. Potential Interactions among Myricetin and Dietary Flavonols through the Inhibition of Human UDP-Glucuronosyltransferase in Vitro. Toxicol. Lett. 2022, 358, 40–47. [Google Scholar] [CrossRef]
- Jiang, L.; Wang, Z.; Wang, X.; Wang, S.; Wang, Z.; Liu, Y. Piceatannol exhibits potential food-drug interactions through the inhibition of human UDP-glucuronosyltransferase (UGT) in Vitro. Toxicol. In Vitro 2020, 67, 104890. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, H.; Hu, X.; Xu, M.; Su, Y.; Zhang, C.; Yue, Y.; Zhang, X.; Wang, X.; Cui, W.; et al. Phloretin exhibits potential food-drug interactions by inhibiting human UDP-glucuronosyltransferases in vitro. Toxicol. In Vitro 2022, 84, 105447. [Google Scholar] [CrossRef]
- Remer, T.; Manz, F. Potential Renal Acid Load of Foods and Its Influence on Urine PH. J. Am. Diet. Assoc. 1995, 95, 791–797. [Google Scholar] [CrossRef]
- Freudenthaler, S.; Meineke, I.; Schreeb, K.H.; Boakye, E.; Gundert-Remy, U.; Gleiter, C.H. Influence of Urine PH and Urinary Flow on the Renal Excretion of Memantine. Br. J. Clin. Pharmacol. 1998, 46, 541. [Google Scholar] [CrossRef] [Green Version]
- Hertrampf, R.; Gundert-Remy, U.; Beckmann, J.; Hoppe, U.; Elsäßer, W.; Stein, H. Elimination of Flecainide as a Function of Urinary Flow Rate and PH. Eur. J. Clin. Pharmacol. 1991, 41, 61–63. [Google Scholar] [CrossRef]
- Couris, R.; Tataronis, G.; McCloskey, W.; Oertel, L.; Dallal, G.; Dwyer, J.; Blumberg, J.B. Dietary Vitamin K Variability Affects International Normalized Ratio (INR) Coagulation Indices. Int. J. Vitam. Nutr. Res. 2006, 76, 65–74. [Google Scholar] [CrossRef]
- Kim, K.H.; Choi, W.S.; Lee, J.H.; Lee, H.; Yang, D.H.; Chae, S.C. Relationship between Dietary Vitamin K Intake and the Stability of Anticoagulation Effect in Patients Taking Long-Term Warfarin. Thromb. Haemost. 2010, 104, 755–759. [Google Scholar] [CrossRef]
- Mahtani, K.R.; Heneghan, C.J.; Nunan, D.; Roberts, N.W. Vitamin K for improved anticoagulation control in patients receiving warfarin. Cochrane Database Syst. Rev. 2014, 5, CD009917. [Google Scholar] [CrossRef]
- Mohamed Pakkir Maideen, N.; Balasubramanian, R.; Muthusamy, S.; Nallasamy, V. An Overview of Clinically Imperative and Pharmacodynamically Significant Drug Interactions of Renin-Angiotensin-Aldosterone System (RAAS) Blockers. Curr. Cardiol. Rev. 2022, 18, e110522204611. [Google Scholar] [CrossRef]
- Batra, V.; Villgran, V. Hyperkalemia from Dietary Supplements. Cureus 2016, 8, e859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campos, M.G.; Machado, J.; Costa, M.L.; Lino, S.; Correia, F.; Maltez, F. Case Report: Severe Hematological, Muscle and Liver Toxicity Caused by Drugs and Artichoke Infusion Interaction in an Elderly Polymedicated Patient. Curr. Drug Saf. 2018, 13, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Fragoso, L.; Martínez-Arismendi, J.L.; Orozco-Bustos, D.; Reyes-Esparza, J.; Torres, E.; Burchiel, S.W. Potential Risks Resulting from Fruit/Vegetable–Drug Interactions: Effects on Drug-Metabolizing Enzymes and Drug Transporters. J. Food Sci. 2011, 76, R112–R124. [Google Scholar] [CrossRef] [PubMed]
- Eagles, S.K.; Gross, A.S.; McLachlan, A.J. The Effects of Cruciferous Vegetable-Enriched Diets on Drug Metabolism: A Systematic Review and Meta-Analysis of Dietary Intervention Trials in Humans. Clin. Pharmacol. Ther. 2020, 108, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Lampe, J.W.; King, I.B.; Li, S.; Grate, M.T.; Barale, K.V.; Chen, C.; Feng, Z.; Potter, J.D. Brassica Vegetables Increase and Apiaceous Vegetables Decrease Cytochrome P450 1A2 Activity in Humans: Changes in Caffeine Metabolite Ratios in Response to Controlled Vegetable Diets. Carcinogenesis 2000, 21, 1157–1162. [Google Scholar] [CrossRef]
- Foster, B.C.; Foster, M.S.; Vandenhoek, S.; Krantis, A.; Budzinski, J.W.; Arnason, J.T.; Gallicano, K.D.; Choudri, S. An in Vitro Evaluation of Human Cytochrome P450 3A4 and P-Glycoprotein Inhibition by Garlic. J. Pharm. Pharm. Sci. 2001, 4, 176–184. [Google Scholar]
- Piscitelli, S.C.; Burstein, A.H.; Welden, N.; Gallicano, K.D.; Falloon, J. The Effect of Garlic Supplements on the Pharmacokinetics of Saquinavir. Clin. Infect. Dis. 2002, 34, 234–238. [Google Scholar] [CrossRef]
- Sunaga, K.; Ohkawa, K.; Nakamura, K.; Ohkubo, A.; Harada, S.; Tsuda, T. Mechanism-Based Inhibition of Recombinant Human Cytochrome P450 3A4 by Tomato Juice Extract. Biol. Pharm. Bull. 2012, 35, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Ohkubo, A.; Chida, T.; Kikuchi, H.; Tsuda, T.; Sunaga, K. Effects of Tomato Juice on the Pharmacokinetics of CYP3A4-Substrate Drugs. Asian J. Pharm. Sci. 2017, 12, 464. [Google Scholar] [CrossRef]
- Tsujimoto, M.; Agawa, C.; Ueda, S.; Yamane, T.; Kitayama, H.; Terao, A.; Fukuda, T.; Minegaki, T.; Nishiguchi, K. Inhibitory Effects of Juices Prepared from Individual Vegetables on CYP3A4 Activity in Recombinant CYP3A4 and LS180 Cells. Biol. Pharm. Bull. 2017, 40, 1561–1565. [Google Scholar] [CrossRef]
- Kumar, S.; Bouic, P.J.; Rosenkranz, B. In Vitro Assessment of the Interaction Potential of Ocimum Basilicum (L.) Extracts on CYP2B6, 3A4, and Rifampicin Metabolism. Front. Pharmacol. 2020, 11, 517. [Google Scholar] [CrossRef]
- Samojlik, I.; Mijatović, V.; Petković, S.; Škrbić, B.; Božin, B. The Influence of Essential Oil of Aniseed (Pimpinella Anisum, L.) on Drug Effects on the Central Nervous System. Fitoterapia 2012, 83, 1466–1473. [Google Scholar] [CrossRef]
- Gupta, R.C.; Chang, D.; Nammi, S.; Bensoussan, A.; Bilinski, K.; Roufogalis, B.D. Interactions between Antidiabetic Drugs and Herbs: An Overview of Mechanisms of Action and Clinical Implications. Diabetol Metab Syndr 2017, 9, 59. [Google Scholar] [CrossRef]
- Hassanzadeh-Taheri, M.; Hassanpour-Fard, M.; Doostabadi, M.; Moodi, H.; Vazifeshenas-Darmiyan, K.; Hosseini, M. Co-Administration Effects of Aqueous Extract of Turnip Leaf and Metformin in Diabetic Rats. J. Tradit. Complement. Med. 2018, 8, 178. [Google Scholar] [CrossRef]
- Zeng, M.; Zhang, L.; Li, M.; Zhang, B.; Zhou, N.; Ke, Y.; Feng, W.; Zheng, X. Estrogenic Effects of the Extracts from the Chinese Yam (Dioscorea Opposite Thunb.) and Its Effective Compounds in Vitro and in Vivo. Molecules 2018, 23, 11. [Google Scholar] [CrossRef] [Green Version]
- Mohseni, M.S.M.; Golshani, B. Simultaneous Determination of Levodopa and Carbidopa from Fava Bean, Green Peas and Green Beans by High Performance Liquid Gas Chromatography. J. Clin. Diagn. Res. 2013, 7, 1004. [Google Scholar] [CrossRef]
- Fernandes, J.; Fialho, M.; Santos, R.; Peixoto-Plácido, C.; Madeira, T.; Sousa-Santos, N.; Virgolino, A.; Santos, O.; Vaz Carneiro, A. Is olive oil good for you? A systematic review and meta-analysis on anti-inflammatory benefits from regular dietary intake. Nutrition 2020, 69, 110559. [Google Scholar] [CrossRef]
- Papakonstantinou, V.D.; Lagopati, N.; Tsilibary, E.C.; Demopoulos, C.A.; Philippopoulos, A.I. A Review on Platelet Activating Factor Inhibitors: Could a New Class of Potent Metal-Based Anti-Inflammatory Drugs Induce Anticancer Properties? Bioinorg. Chem. Appl. 2017, 2017, 6947034. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Krause, M.; Schmucker, C.; Hoffmann, G.; Rücker, G.; Meerpohl, J.J. Impact of Different Types of Olive Oil on Cardiovascular Risk Factors: A Systematic Review and Network Meta-Analysis. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1030–1039. [Google Scholar] [CrossRef]
- Albadawi, D.A.I.; Ravishankar, D.; Vallance, T.M.; Patel, K.; Osborn, H.M.I.; Vaiyapuri, S. Impacts of Commonly Used Edible Plants on the Modulation of Platelet Function. Int. J. Mol. Sci. 2022, 23, 605. [Google Scholar] [CrossRef]
- Jeong, H.U.; Kwon, S.S.; Kong, T.Y.; Kim, J.H.; Lee, H.S. Inhibitory Effects of Cedrol, β-Cedrene, and Thujopsene on Cytochrome P450 Enzyme Activities in Human Liver Microsomes. J. Toxicol. Environ. Health A 2014, 77, 1522–1532. [Google Scholar] [CrossRef]
- Bailey, D.G. Grapefruit-Medication Interactions. CMAJ 2013, 185, 507–508. [Google Scholar] [CrossRef] [Green Version]
- Hanley, M.J.; Cancalon, P.; Widmer, W.W.; Greenblatt, D.J. The Effect of Grapefruit Juice on Drug Disposition. Expert Opin. Drug Metab. Toxicol. 2011, 7, 267–286. [Google Scholar] [CrossRef]
- Seden, K.; Dickinson, L.; Khoo, S.; Back, D. Grapefruit-Drug Interactions. Drugs 2010, 70, 2373–2407. [Google Scholar] [CrossRef]
- Guo, L.Q.; Yamazoe, Y. Inhibition of Cytochrome P450 by Furanocoumarins in Grapefruit Juice and Herbal Medicines. Acta Pharmacol. Sin. 2004, 25, 129–136. [Google Scholar] [PubMed]
- Lown, K.S.; Bailey, D.G.; Fontana, R.J.; Janardan, S.K.; Adair, C.H.; Fortlage, L.A.; Brown, M.B.; Guo, W.; Watkins, P.B. Grapefruit Juice Increases Felodipine Oral Availability in Humans by Decreasing Intestinal CYP3A Protein Expression. J. Clin. Investig. 1997, 99, 2545–2553. [Google Scholar] [CrossRef] [Green Version]
- Bailey, D.G.; Dresser, G.; Arnold, J.M. Grapefruit-Medication Interactions: Forbidden Fruit or Avoidable Consequences? CMAJ 2013, 185, 309–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, D.G. Better to Avoid Grapefruit with Certain Statins. Am. J. Med. 2016, 129, e301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, D.G.; Dresser, G.K.; Bend, J.R. Bergamottin, Lime Juice, and Red Wine as Inhibitors of Cytochrome P450 3A4 Activity: Comparison with Grapefruit Juice. Clin. Pharmacol. Ther. 2003, 73, 529–537. [Google Scholar] [CrossRef]
- Chen, M.; Zhou, S.Y.; Fabriaga, E.; Zhang, P.H.; Zhou, Q. Food-Drug Interactions Precipitated by Fruit Juices Other than Grapefruit Juice: An Update Review. J. Food Drug Anal. 2018, 26, S61–S71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petric, Z.; Žuntar, I.; Putnik, P.; Kovačević, D.B. Food–Drug Interactions with Fruit Juices. Foods 2021, 10, 33. [Google Scholar] [CrossRef]
- An, G.; Mukker, J.K.; Derendorf, H.; Frye, R.F. Enzyme- and transporter-mediated beverage-drug interactions: An update on fruit juices and green tea. J. Clin. Pharmacol. 2015, 55, 1313–1331. [Google Scholar] [CrossRef]
- Dresser, G.K.; Bailey, D.G.; Leake, B.F.; Schwarz, U.I.; Dawson, P.A.; Freeman, D.J.; Kim, R.B. Fruit Juices Inhibit Organic Anion Transporting Polypeptide-Mediated Drug Uptake to Decrease the Oral Availability of Fexofenadine. Clin. Pharmacol. Ther. 2002, 71, 11–20. [Google Scholar] [CrossRef]
- Kamath, A.V.; Yao, M.; Zhang, Y.; Chong, S. Effect of Fruit Juices on the Oral Bioavailability of Fexofenadine in Rats. J. Pharm. Sci. 2005, 94, 233–239. [Google Scholar] [CrossRef]
- Grenier, J.; Fradette, C.; Morelli, G.; Merritt, G.J.; Vranderick, M.; Ducharme, M.P. Pomelo Juice, but Not Cranberry Juice, Affects the Pharmacokinetics of Cyclosporine in Humans. Clin. Pharmacol. Ther. 2006, 79, 255–262. [Google Scholar] [CrossRef]
- Gertz, B.J.; Holland, S.D.; Kline, W.F.; Matuszewski, B.K.; Freeman, A.; Quan, H.; Lasseter, K.C.; Mucklow, J.C.; Porras, A.G. Studies of the Oral Bioavailability of Alendronate. Clin. Pharmacol. Ther. 1995, 58, 288–298. [Google Scholar] [CrossRef]
- Tapaninen, T.; Neuvonen, P.J.; Niemi, M. Orange and Apple Juice Greatly Reduce the Plasma Concentrations of the OATP2B1 Substrate Aliskiren. Br. J. Clin. Pharmacol. 2011, 71, 718–726. [Google Scholar] [CrossRef]
- Malhotra, S.; Bailey, D.G.; Paine, M.F.; Watkins, P.B. Seville Orange Juice-Felodipine Interaction: Comparison with Dilute Grapefruit Juice and Involvement of Furocoumarins. Clin. Pharmacol. Ther. 2001, 69, 14–23. [Google Scholar] [CrossRef]
- Karmakar, S.; Biswas, S.; Bera, R.; Mondal, S.; Kundu, A.; Ali, M.A.; Sen, T. Beverage-Induced Enhanced Bioavailability of Carbamazepine and Its Consequent Effect on Antiepileptic Activity and Toxicity. J. Food Drug Anal. 2015, 23, 327–334. [Google Scholar] [CrossRef]
- Backman, J.T.; Mäenpää, J.; Belle, D.J.; Wrighton, S.A.; Kivistö, K.T.; Neuvonen, P.J. Lack of Correlation between in Vitro and m Vivo Studies on the Effects of Tangeretin and Tangerine Juice on Midazolam Hydroxylation. Clin. Pharmacol. Ther. 2000, 67, 382–390. [Google Scholar] [CrossRef]
- Morita, T.; Akiyoshi, T.; Sato, R.; Uekusa, Y.; Katayama, K.; Yajima, K.; Imaoka, A.; Sugimoto, Y.; Kiuchi, F.; Ohtani, H. Citrus Fruit-Derived Flavanone Glycoside Narirutin Is a Novel Potent Inhibitor of Organic Anion-Transporting Polypeptides. J. Agric. Food Chem. 2020, 68, 14182–14191. [Google Scholar] [CrossRef]
- Akamine, Y.; Miura, M.; Komori, H.; Saito, S.; Kusuhara, H.; Tamai, I.; Ieiri, I.; Uno, T.; Yasui-Furukori, N. Effects of One-Time Apple Juice Ingestion on the Pharmacokinetics of Fexofenadine Enantiomers. Eur. J. Clin. Pharmacol. 2014, 70, 1087–1095. [Google Scholar] [CrossRef]
- Jeon, H.; Jang, I.J.; Lee, S.; Ohashi, K.; Kotegawa, T.; Ieiri, I.; Cho, J.Y.; Yoon, S.H.; Shin, S.G.; Yu, K.S.; et al. Apple Juice Greatly Reduces Systemic Exposure to Atenolol. Br. J. Clin. Pharmacol. 2013, 75, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Morita, T.; Akiyoshi, T.; Tsuchitani, T.; Kataoka, H.; Araki, N.; Yajima, K.; Katayama, K.; Imaoka, A.; Ohtani, H. Inhibitory Effects of Cranberry Juice and Its Components on Intestinal OATP1A2 and OATP2B1: Identification of Avicularin as a Novel Inhibitor. J. Agric. Food Chem. 2022, 70, 3310–3320. [Google Scholar] [CrossRef]
- Srinivas, N.R. Cranberry Juice Ingestion and Clinical Drug-Drug Interaction Potentials; Review of Case Studies and Perspectives. J. Pharm. Pharm. Sci. 2013, 16, 289–303. [Google Scholar] [CrossRef] [Green Version]
- Greenblatt, D.J.; Von Moltke, L.L.; Perloff, E.S.; Luo, Y.; Harmatz, J.S.; Zinny, M.A. Interaction of Flurbiprofen with Cranberry Juice, Grape Juice, Tea, and Fluconazole: In Vitro and Clinical Studies. Clin. Pharmacol. Ther. 2006, 79, 125–133. [Google Scholar] [CrossRef]
- Lilja, J.J.; Backman, J.T.; Neuvonen, P.J. Effects of Daily Ingestion of Cranberry Juice on the Pharmacokinetics of Warfarin, Tizanidine, and Midazolam—Probes of CYP2C9, CYP1A2, and CYP3A4. Clin. Pharmacol. Ther. 2007, 81, 833–839. [Google Scholar] [CrossRef]
- Srinivas, N.R. Is Pomegranate Juice a Potential Perpetrator of Clinical Drug-Drug Interactions? Review of the in Vitro, Preclinical and Clinical Evidence. Eur. J. Drug Metab. Pharmacokinet. 2013, 38, 223–229. [Google Scholar] [CrossRef]
- Yusuff, K.B.; Emeka, P.M.; Attimarad, M. Concurrent Administration of Date Palm Fruits with Lisinopril Increases Serum Potassium Level in Male Rabbits. Int. J. Pharmacol. 2018, 14, 93–98. [Google Scholar] [CrossRef]
- St-Jules, D.E.; Goldfarb, D.S.; Sevick, M.A. Nutrient Non-Equivalence: Does Restricting High-Potassium Plant Foods Help to Prevent Hyperkalemia in Hemodialysis Patients? J. Ren. Nutr. 2016, 26, 282–287. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Jiménez-Molén, J.J.; Lindholm, B.; Cederholm, T.; Ärnlöv, J.; Risérus, U.; Sjögren, P.; Carrero, J.J. Mediterranean Diet, Kidney Function, and Mortality in Men with CKD. Clin. J. Am. Soc. Nephrol. 2013, 8, 1548–1555. [Google Scholar] [CrossRef] [Green Version]
- Molina-Vega, M.; Gómez-Pérez, A.M.; Tinahones, F.J. Fish in the Mediterranean diet. In The Mediterranean Diet: An Evidence-Based Approach, 2nd ed.; Preedy, V.R., Watson, R.R., Eds.; Elsevier Science: Amsterdam, The Netherlands, 2020; pp. 275–284. [Google Scholar] [CrossRef]
- Méndez, L.; Dasilva, G.; Taltavull, N.; Romeu, M.; Medina, I. Marine Lipids on Cardiovascular Diseases and Other Chronic Diseases Induced by Diet: An Insight Provided by Proteomics and Lipidomics. Mar. Drugs 2017, 15, 258. [Google Scholar] [CrossRef] [Green Version]
- Vanschoonbeek, K.; Feijge, M.A.; Paquay, M.; Rosing, J.; Saris, W.; Kluft, C.; Giesen, P.L.; de Maat, M.P.; Heemskerk, J.W. Variable Hypocoagulant Effect of Fish Oil Intake in Humans: Modulation of Fibrinogen Level and Thrombin Generation. Arter. Thromb Vasc Biol 2004, 24, 1734–1740. [Google Scholar] [CrossRef]
- Buckley, M.S.; Goff, A.D.; Knapp, W.E. Fish Oil Interaction with Warfarin. Ann. Pharmacother. 2004, 38, 50–53. [Google Scholar] [CrossRef]
- Jalili, M.; Dehpour, A.R. Extremely Prolonged INR Associated with Warfarin in Combination with Both Trazodone and Omega-3 Fatty Acids. Arch. Med. Res. 2007, 38, 901–904. [Google Scholar] [CrossRef]
- Pryce, R.; Bernaitis, N.; Davey, A.K.; Badrick, T.; Anoopkumar-Dukie, S. The Use of Fish Oil with Warfarin Does Not Significantly Affect Either the International Normalised Ratio or Incidence of Adverse Events in Patients with Atrial Fibrillation and Deep Vein Thrombosis: A Retrospective Study. Nutrients 2016, 8, 578. [Google Scholar] [CrossRef] [Green Version]
- KANEKO, J.; TANIMUKAI, H. MONOAMINE OXIDASE INHIBITORS (MAO). Sogo. Rinsho. 1964, 13, 833–846. [Google Scholar] [CrossRef]
- Kibangou, I.B.; Bouhallab, S.; Henry, G.; Bureau, F.; Allouche, S.; Blais, A.; Guérin, P.; Arhan, P.; Bouglé, D.L. Milk Proteins and Iron Absorption: Contrasting Effects of Different Caseinophosphopeptides. Pediatr. Res. 2005, 58, 731–734. [Google Scholar] [CrossRef] [PubMed]
- De Lemos, M.L.; Hamata, L.; Jennings, S.; Leduc, T. Interaction between Mercaptopurine and Milk. J. Oncol. Pharm. Pract. 2007, 13, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Sofianou-Katsoulis, A.; Khakoo, G.; Kaczmarski, R. Reduction in Bioavailability of 6-Mercaptopurine on Simultaneous Administration with Cow’s Milk. Pediatr. Hematol. Oncol. 2006, 23, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.M.C.C.; Vicente, A.F.R.B. Meat Nutritional Composition and Nutritive Role in the Human Diet. Meat Sci. 2013, 93, 586–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, I.; Pérez-Gregorio, R.; Soares, S.; Mateus, N.; De Freitas, V.; Santos-Buelga, C.; Feliciano, A.S. Wine Flavonoids in Health and Disease Prevention. Molecules 2017, 22, 292. [Google Scholar] [CrossRef] [PubMed]
- Snopek, L.; Mlcek, J.; Sochorova, L.; Baron, M.; Hlavacova, I.; Jurikova, T.; Kizek, R.; Sedlackova, E.; Sochor, J. Contribution of Red Wine Consumption to Human Health Protection. Molecules 2018, 23, 1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renaud, S.; de Lorgeril, M. Wine, Alcohol, Platelets, and the French Paradox for Coronary Heart Disease. Lancet 1992, 339, 1523–1526. [Google Scholar] [CrossRef]
- Weathermon, R.; Crabb, D.W. Alcohol and Medication Interactions. Alcohol Res. Health 1999, 23, 40. [Google Scholar]
- Mergenhagen, K.A.; Wattengel, B.A.; Skelly, M.K.; Clark, C.M.; Russo, T.A. Fact versus Fiction: A Review of the Evidence behind Alcohol and Antibiotic Interactions. Antimicrob. Agents Chemother. 2020, 64, e02167-19. [Google Scholar] [CrossRef]
- Romeo, J.; Würnberg, J.; Nova, E.; Díaz, L.E.; Gómez-Martinez, S.; Marcos, A. Moderate Alcohol Consumption and the Immune System: A Review. Br. J. Nutr. 2007, 98, S111–S115. [Google Scholar] [CrossRef]
- Foster, J.H.; Powell, J.E.; Marshall, E.J.; Peters, T.J. Quality of Life in Alcohol-Dependent Subjects--a Review. Qual. Life Res. 1999, 8, 255–261. [Google Scholar] [CrossRef]
- Pauwels, E.K.J. The Protective Effect of the Mediterranean Diet: Focus on Cancer and Cardiovascular Risk. Med. Princ. Pract. 2011, 20, 103–111. [Google Scholar] [CrossRef]
- Tsigalou, C.; Konstantinidis, T.; Paraschaki, A.; Stavropoulou, E.; Voidarou, C.; Bezirtzoglou, E. Mediterranean diet as a tool to combat inflammation and chronic diseases. An overview. Biomedicines 2020, 8, 201. [Google Scholar] [CrossRef]
- Baute, V.; Sampath-Kumar, R.; Nelson, S.; Basil, B. Nutrition Education for the Health-care Provider Improves Patient Outcomes. Glob. Adv. Health Med. 2018, 7, 2164956118795995. [Google Scholar] [CrossRef]
- Spanakis, M.; Patelarou, A.E.; Patelarou, E. Nursing Personnel in the Era of Personalized Healthcare in Clinical Practice. J. Pers. Med. 2020, 10, 56. [Google Scholar] [CrossRef]
- Thorpe, M.G.; Milte, C.M.; Crawford, D.; McNaughton, S.A. Education and lifestyle predict change in dietary patterns and diet quality of adults 55 years and over. Nutr. J. 2019, 18, 67. [Google Scholar] [CrossRef] [Green Version]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [Green Version]
- Aljefree, N.M.; Almoraie, N.M.; Shatwan, I.M. Association of two types of dietary pattern scores with cardiovascular disease risk factors and serum 25 hydroxy vitamin D levels in Saudi Arabia. Food Nutr. Res. 2021, 65. [Google Scholar] [CrossRef]
- Herrera-Marcos, L.V.; Lou-Bonafonte, J.M.; Arnal, C.; Navarro, M.A.; Osada, J. Transcriptomics and the Mediterranean Diet: A Systematic Review. Nutrients 2017, 9, 472. [Google Scholar] [CrossRef] [Green Version]
- Badimon, L.; Vilahur, G.; Padro, T. Systems biology approaches to understand the effects of nutrition and promote health. Br. J. Clin. Pharmacol. 2017, 83, 38. [Google Scholar] [CrossRef] [Green Version]
- Yeh, C.T.; Yen, G.C. Effect of Vegetables on Human Phenolsulfotransferases in Relation to Their Antioxidant Activity and Total Phenolics. Free Radic. Res. 2005, 39, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Harasym, J.; Oledzki, R. Effect of Fruit and Vegetable Antioxidants on Total Antioxidant Capacity of Blood Plasma. Nutrition 2014, 30, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Ravera, A.; Carubelli, V.; Sciatti, E.; Bonadei, I.; Gorga, E.; Cani, D.; Vizzardi, E.; Metra, M.; Lombardi, C. Nutrition and Cardiovascular Disease: Finding the Perfect Recipe for Cardiovascular Health. Nutrients 2016, 8, 363. [Google Scholar] [CrossRef] [PubMed]
- Bjerrum, L.; Lopez-Valcarcel, B.G.; Petersen, G. Risk Factors for Potential Drug Interactions in General Practice. Eur. J. Gen. Pract. 2008, 14, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guttman, Y.; Kerem, Z. Computer-Aided (In Silico) Modeling of Cytochrome P450-Mediated Food-Drug Interactions (FDI). Int. J. Mol. Sci. 2022, 23, 8498. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Vadrev, S.M.; Magana-Mora, A.; Levman, J.; Soufan, O. A novel graph mining approach to predict and evaluate food-drug interactions. Sci. Rep. 2022, 12, 1061. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.Y.; Kim, H.U.; Lee, S.Y. Deep Learning Improves Prediction of Drug–Drug and Drug–Food Interactions. Proc. Natl. Acad. Sci. USA 2018, 115, E4304–E4311. [Google Scholar] [CrossRef] [Green Version]
- Car, J.; Tan, W.S.; Huang, Z.; Sloot, P.; Franklin, B.D. eHealth in the future of medications management: Personalisation, monitoring and adherence. BMC Med. 2017, 15, 73. [Google Scholar] [CrossRef] [Green Version]
- Spanakis, E.G.; Santana, S.; Tsiknakis, M.; Marias, K.; Sakkalis, V.; Teixeira, A.; Janssen, J.H.; de Jong, H.; Tziraki, C. Technology-Based Innovations to Foster Personalized Healthy Lifestyles and Well-Being: A Targeted Review. J. Med. Internet Res. 2016, 18, e128. [Google Scholar] [CrossRef]
- Ware, P.; Bartlett, S.J.; Paré, G.; Symeonidis, I.; Tannenbaum, C.; Bartlett, G.; Poissant, L.; Ahmed, S. Using EHealth Technologies: Interests, Preferences, and Concerns of Older Adults. Interact. J. Med. Res. 2017, 6, e3. [Google Scholar] [CrossRef] [Green Version]
- Ossebaard, H.C.; Van Gemert-Pijnen, L. EHealth and Quality in Health Care: Implementation Time. Int. J. Qual. Health Care 2016, 28, 415–419. [Google Scholar] [CrossRef] [Green Version]
- Black, A.D.; Car, J.; Pagliari, C.; Anandan, C.; Cresswell, K.; Bokun, T.; McKinstry, B.; Procter, R.; Majeed, A.; Sheikh, A. The Impact of EHealth on the Quality and Safety of Health Care: A Systematic Overview. PLoS Med. 2011, 8, e1000387. [Google Scholar] [CrossRef] [Green Version]
- Maniadi, E.; Kondylakis, H.; Spanakis, E.G.; Spanakis, M.; Tsiknakis, M.; Marias, K.; Dong, F. Designing a digital patient avatar in the context of the MyHealthAvatar project initiative. In Proceedings of the 13th IEEE International Conference on BioInformatics and BioEngineering (BIBE 2013), Chania, Greece, 10–13 November 2013. [Google Scholar]
- Vasiloglou, M.F.; Lu, Y.; Stathopoulou, T.; Papathanail, I.; Faeh, D.; Ghosh, A.; Baumann, M.; Mougiakakou, S. Assessing Mediterranean Diet Adherence with the Smartphone: The Medipiatto Project. Nutrients 2020, 12, 3763. [Google Scholar] [CrossRef]
- McAleese, D.; Linardakis, M.; Papadaki, A. Quality and Presence of Behaviour Change Techniques in Mobile Apps for the Mediterranean Diet: A Content Analysis of Android Google Play and Apple App Store Apps. Nutrients 2022, 14, 1290. [Google Scholar] [CrossRef]
- Spanakis, M.; Sfakianakis, S.; Spanakis, E.G.; Kallergis, G.; Sakkalis, V. PDCA: An EHealth Service for the Management of Drug Interactions with Complementary and Alternative Medicines. In Proceedings of the 2018 IEEE EMBS International Conference on Biomedical and Health Informatics (BHI), Las Vegas, NV, USA, 4–7 March 2018. [Google Scholar]
- Spanakis, M.; Sfakianakis, S.; Kallergis, G.; Spanakis, E.G.; Sakkalis, V. PharmActa: Personalized Pharmaceutical Care EHealth Platform for Patients and Pharmacists. J. Biomed. Inform. 2019, 100, 103336. [Google Scholar] [CrossRef]
Figure 1.
Representation of pharmacological mechanisms of DFIs and their impact on clinical outcome.
Figure 1.
Representation of pharmacological mechanisms of DFIs and their impact on clinical outcome.

Figure 2.
Graphical representation of food effect on the PK profile of a drug that leads in clinically significant DFIs (MEC maximum effective concentration, MIC: minimum effective concentration).
Figure 2.
Graphical representation of food effect on the PK profile of a drug that leads in clinically significant DFIs (MEC maximum effective concentration, MIC: minimum effective concentration).

Figure 3.
Pharmacokinetic processes for orally administered drugs and sites of potential PK-DFIs.

Figure 4.
The Mediterranean diet pyramid along with examples of characteristic constituents that can be found in Med-D’s food products.
Figure 4.
The Mediterranean diet pyramid along with examples of characteristic constituents that can be found in Med-D’s food products.
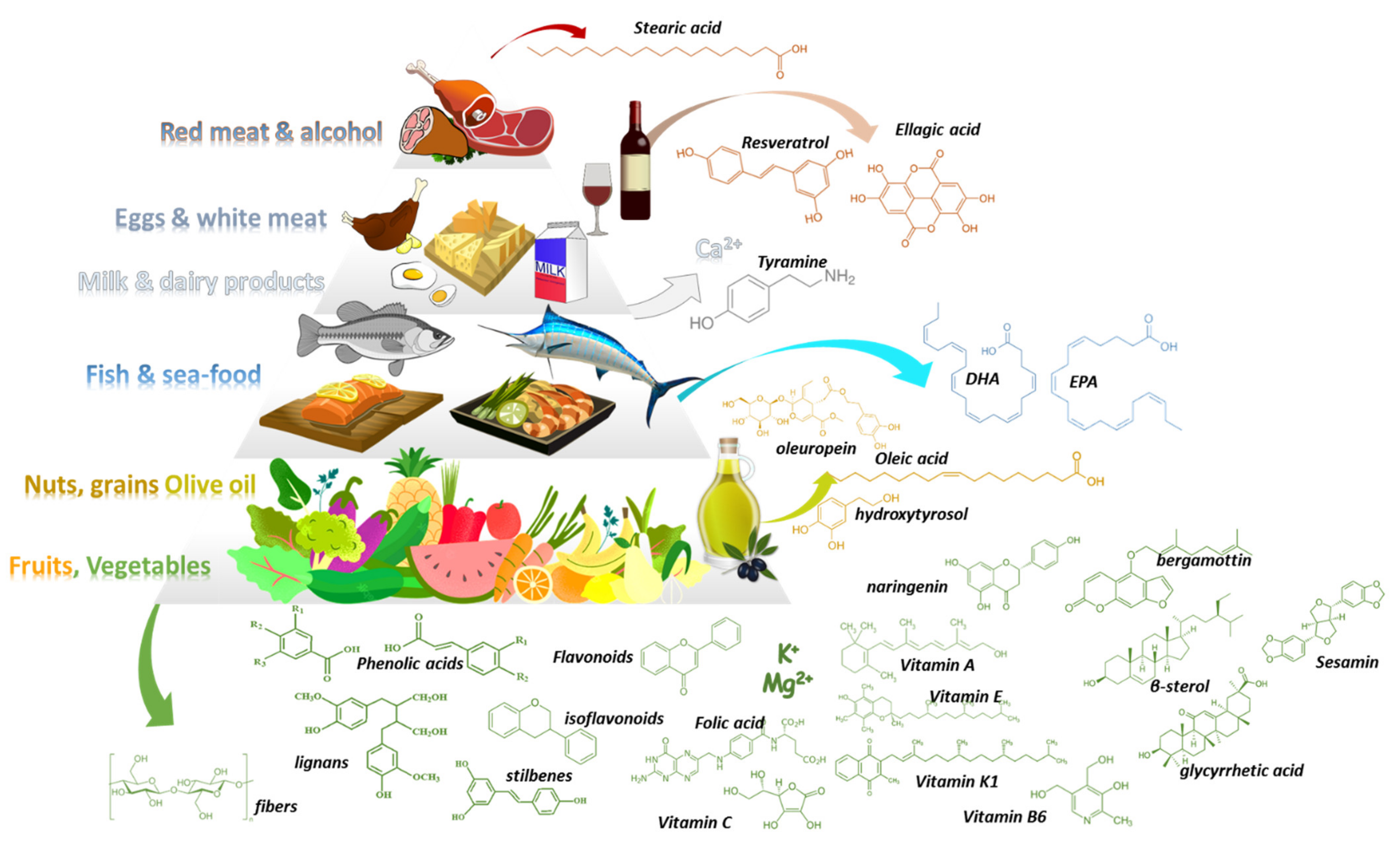
Figure 5.
DFIs of Med-D food products regarding relation with type II and type III (subtypes a and b) interactions.
Figure 5.
DFIs of Med-D food products regarding relation with type II and type III (subtypes a and b) interactions.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
DFIs, pharmacological mechanism, significance, and level of evidence for vegetables and herbs that are contained in the base of Med-D pyramid (PK: pharmacokinetic, PD: Pharmacodynamic, DFI: drug-food interaction).
Table 1.
DFIs, pharmacological mechanism, significance, and level of evidence for vegetables and herbs that are contained in the base of Med-D pyramid (PK: pharmacokinetic, PD: Pharmacodynamic, DFI: drug-food interaction).
| Food | Type of DFIs | Suggested Mechanism | Clinical Significance | Level of Evidence |
|---|---|---|---|---|
| Artichoke | PK | CYP mediated drug metabolism | Moderate | Moderate |
| Arugula | PD | Anticoagulants—Vitamin K | Moderate | Theoretical |
| Asparagus | PD | Anticoagulants—Vitamin K | Moderate | Theoretical |
| Beetroots | - | - | - | |
| Bell pepper | PD | Anticoagulants—Vitamin K | Moderate | Theoretical |
| Broccoli | PD | Anticoagulants—Vitamin K | Moderate | Theoretical |
| Brussel Sprouts | PK | CYP mediated drug metabolism | Moderate | Moderate |
| Cabbage | PK | CYP mediated drug metabolism | Moderate | Good |
| Carrots | PK | CYP mediated drug metabolism | Minor | Low |
| Cauliflower | PK | CYP mediated drug metabolism | Minor | Moderate |
| Celery | PD | Synergism sedatives | Minor | Good |
| Collard greens | PD | Synergism antidiabetic medications | Minor | Low |
| Cucumbers | - | - | - | - |
| Dandelion greens | PD | Lithium | Moderate | Low |
| Eggplant | - | - | - | - |
| Fennel | - | - | - | - |
| Fava beans | PD | synergism with anti-parkinson drugs (L-dopa content) | Moderate | Low |
| Garlic | PK | Moderate | Good | |
| Green beans | - | - | - | - |
| Kale | PD | Anticoagulants—Vitamin K | Moderate | Theoretical |
| Leeks | PD | Anticoagulants—Vitamin K | Minor | Theoretical |
| Mushrooms | - | - | - | - |
| Onions | PD | Anticoagulants—Vitamin K | Minor | Theoretical |
| Potatoes | - | - | - | - |
| Radish | PK | stimulate GI motility & transit time | Minor | Moderate |
| Scallions | PD | Anticoagulants—Vitamin K | Minor | Theoretical |
| Shallots | PD | Anticoagulants—Vitamin K | Minor | Theoretical |
| Spinach | PD | Anticoagulants—Vitamin K | Moderate | Theoretical |
| Squash | PD | stimulant laxative may alter Κ+ | Minor | Theoretical |
| Sweet potatoes | - | - | - | - |
| Swiss chard | PD | Anticoagulants—Vitamin K | Minor | Theoretical |
| Tomatoes | PK | CYP mediated drug metabolism | Minor | Moderate |
| Turnips | PD | Synergism antidiabetic medications | Minor | Moderate |
| Yams | PD | Synergism with estrogens | Moderate | Good |
| Zucchini | - | - | - | - |
| Anise | PK | CYP mediated metabolism | Moderate | Good |
| Basil | PD | Anticoagulants, n-3 FAs | Moderate | Low |
| Bayleaf | PD | Synergism with antidiabetics & sedatives | Minor | Low |
| Cinnamon | PD | Synergism antidiabetic & hepatoxicity | Minor | Low |
| Cloves | PD | potentiate the effects of drugs that affect hemostasis | Moderate | Moderate |
| Cumin | PD | Synergism antidiabetic medications | Moderate | Moderate |
| Fennel | - | - | - | - |
| Lavender | PD | Synergism with sedatives | Moderate | Low |
| Marjoram | PD | Potentiate effects of drugs for hemostasis | Moderate | Low |
| Mint | - | - | - | - |
| Oregano | PD | Potentiate effects of drugs for hemostasis | Moderate | Low |
| Parsley | - | - | - | - |
| Pepper | PK | CYP mediated drug metabolism | Minor | Moderate |
| Rosemary | - | - | - | - |
| Sage | PD | Synergism with sedatives | Moderate | Low |
| Savory | PD | Anticoagulants, n-3 FAs | Moderate | Low |
| Sumac | PD | Induce nephrotoxicity of drugs | Minor | Low |
| Tarragon | PD | Anticoagulants, n-3 FAs | Moderate | Low |
| Thyme | PD | Anticoagulants, n-3 FAs | Moderate | Low |
Level of evidence: (i) Theoretical (ii) low: in vitro data (iii) moderate (in vitro/in vivo) Good (in vitro/in vivo/clinical); (iv) High (in vitro/in vivo/clinical observations/clinical trials).
Table 2.
DFIs, pharmacological mechanism, significance, and level of evidence for fruits that are contained in the base of Med-D pyramid (PK: pharmacokinetic, PD: Pharmacodynamic, DFI: drug-food interaction).
Table 2.
DFIs, pharmacological mechanism, significance, and level of evidence for fruits that are contained in the base of Med-D pyramid (PK: pharmacokinetic, PD: Pharmacodynamic, DFI: drug-food interaction).
| Fruit | Type of DFIs | Suggested Mechanism | Clinical Significance | Level of Evidence |
|---|---|---|---|---|
| Apples | PK | OAT transporter inhibition | Moderate | Good |
| Apricots | - | - | - | - |
| Avocados | PD | Anticoagulants—Vitamin K | Moderate | Theoretical |
| Bananas | PD | Hyperkaliemia, high K+ | Moderate | Theoretical |
| Cherries | - | - | - | - |
| Clementines | PK | CYP mediated drug metabolism | Moderate | Moderate |
| Grapefruit | PK | P-gp transport & CYP mediated drug metabolism | Serious-avoid | High |
| Grapes | PK | UGT mediated drug metabolism | Moderate | Good |
| Lime | PK | |||
| Melons | PD | Synergism antidiabetic medications | Low | Theoretical |
| Oranges | PK | OAT transporter inhibition | Moderate | Good |
| Peaches | PD | Hyperkaliemia, high K+ | Moderate | Theoretical |
| Pears | - | - | - | - |
| Pomegranates | PK | CYP mediated drug metabolism | None | High |
| Pomelo | PK | P-gp transport & CYP mediated drug metabolism | Use with caution | Good |
| Strawberries | PK/PD | Metabolism & anticoagulation | Low | Theoretical |
| Tangerines | PK | CYP mediated drug metabolism | Moderate | Moderate |
Level of evidence: (i) Theoretical (ii) low: in vitro data (iii) moderate (in vitro/in vivo) Good (in vitro/in vivo/clinical); (iv) High (in vitro/in vivo/clinical observations/clinical trials).
Table 3.
DFIs, pharmacological mechanism, significance, and level of evidence for nuts, and cereals that are contained in the base of Med-D pyramid.
Table 3.
DFIs, pharmacological mechanism, significance, and level of evidence for nuts, and cereals that are contained in the base of Med-D pyramid.
| Food | Type of DFIs | Suggested Mechanism | Clinical Significance | Level of Evidence |
|---|---|---|---|---|
| Barley | PK | Modulation GI absorption | Moderate | Low |
| Buckwheat | - | - | - | - |
| Bulgur | - | - | - | - |
| Farro-flax seed | PD | Anticoagulants, n-3 FAs | Moderate | Low |
| Millet | - | - | - | - |
| Oats & fibers | PK | Modulation GI absorption | Moderate | Good |
| Polenta | - | - | - | - |
| Rice | - | - | - | - |
| Wheat Berries | PK | Modulation GI absorption | Moderate | Low |
| Breads | - | - | - | - |
| Couscous | - | - | - | - |
| Almonds | - | - | - | - |
| Cashews | PD | Synergism antidiabetic medications | Minor | Low |
| Chickpeas | ||||
| Fava beans | PD | Synergism with anti-Parkinson drugs (high L-dopa content) | Moderate | Low |
| Green peas | - | - | - | - |
| Hazelnuts | ||||
| Kidney beans | PK | Modulation GI absorption | Minor | Low |
| Lentils | PD | Hyperkaliemia, high K+ | Minor | Low |
| Peanuts | PD | Tyramine pressure effect (MAOIs) | Use with caution | Low |
| Pistachios | - | - | - | - |
| Sesame seeds (tachini) | PK | CYP mediated metabolism | None | Moderate |
| Split peas | PK | Modulation GI absorption | Minor | Theoretical |
| Walnuts | PK | Modulation GI absorption | Moderate | Theoretical |
Level of evidence: (i) Theoretical (ii) low: in vitro data (iii) moderate (in vitro/in vivo) Good (in vitro/in vivo/clinical); (iv) High (in vitro/in vivo/clinical observations/clinical trials).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Spanakis, M.; Patelarou, E.; Patelarou, A. Drug-Food Interactions with a Focus on Mediterranean Diet. Appl. Sci. 2022, 12, 10207. https://doi.org/10.3390/app122010207
AMA Style
Spanakis M, Patelarou E, Patelarou A. Drug-Food Interactions with a Focus on Mediterranean Diet. Applied Sciences. 2022; 12(20):10207. https://doi.org/10.3390/app122010207
Chicago/Turabian StyleSpanakis, Marios, Evridiki Patelarou, and Athina Patelarou. 2022. "Drug-Food Interactions with a Focus on Mediterranean Diet" Applied Sciences 12, no. 20: 10207. https://doi.org/10.3390/app122010207
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.