
Mobile Health App for Adolescents: Motion Sensor Data and Deep Learning Technique to Examine the Relationship between Obesity and Walking Patterns

 , and
, and
Abstract
:1. Introduction
2. Experiment Methods
2.1. Mobile Health Application
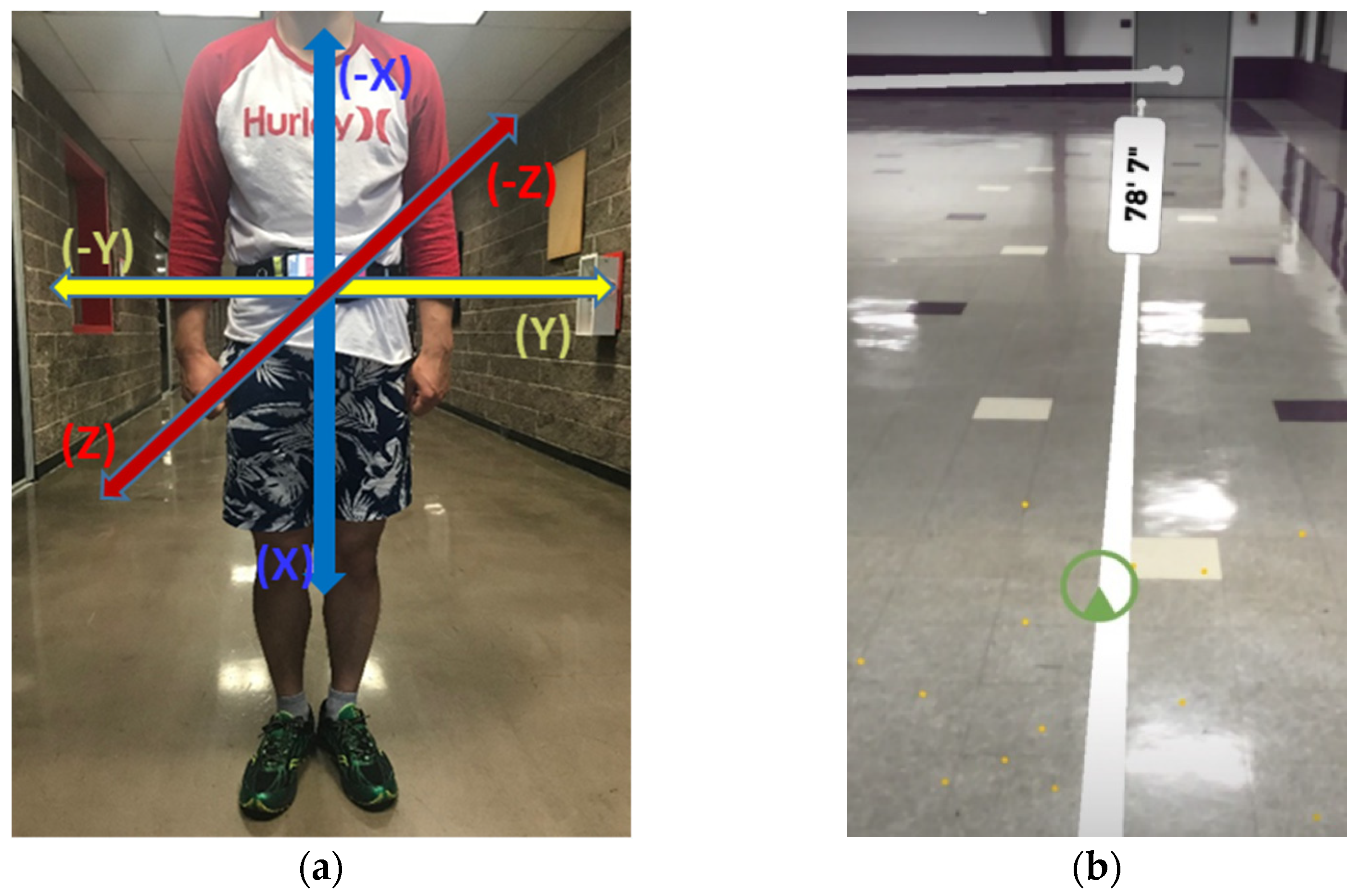
2.2. Data Collection
2.3. Data Preprocessing
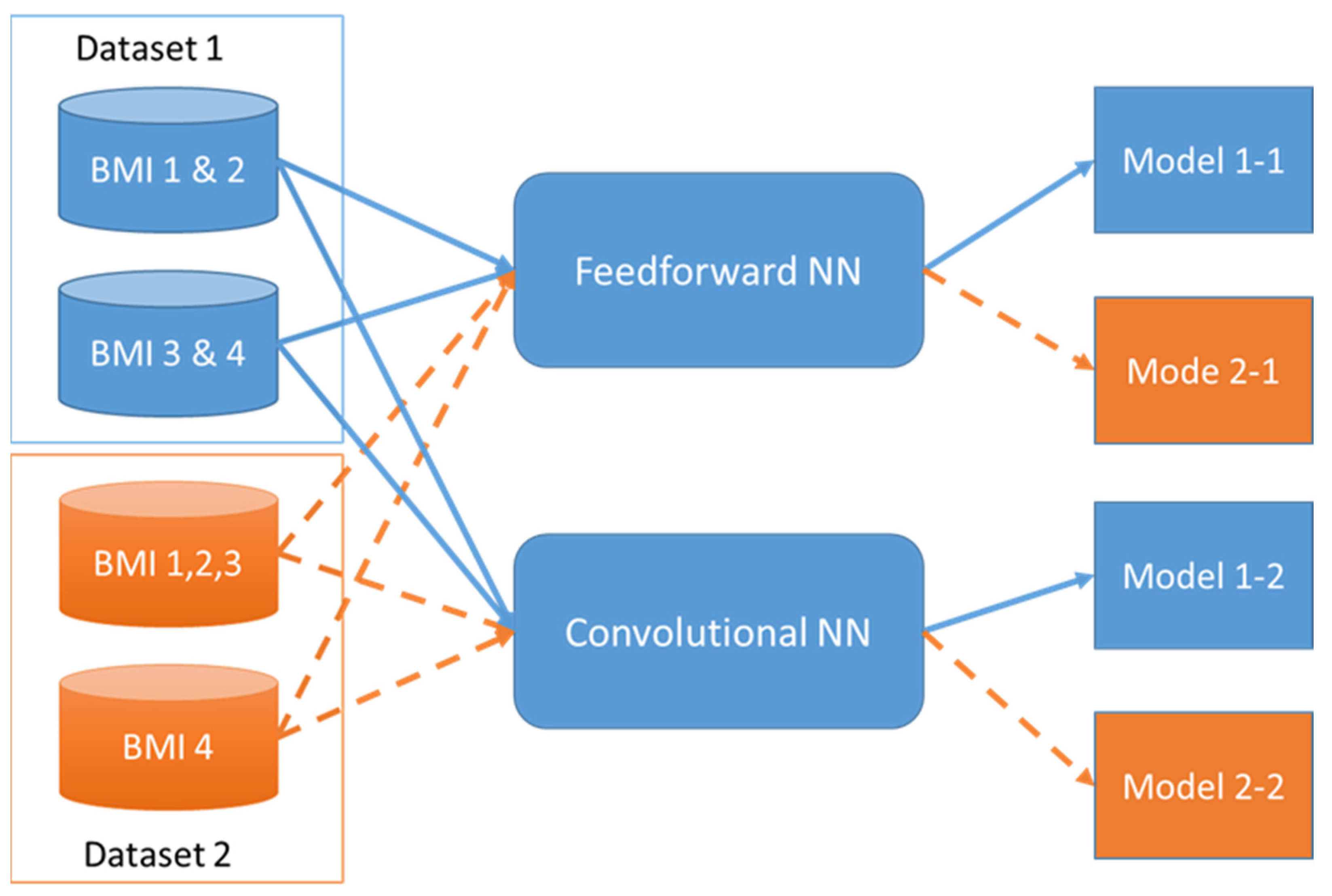
3. Analysis Model
| Algorithm 1. Feedforward NN |
| #init model model <- keras_model_sequential() initializer <- tf$keras$initializers$GlorotNormal() unit<-512 # Build Model model <- model %>% layer_dense (units = unit, activation = ‘relu’, input_shape = shape(data_dim), kernel_initializer = initializer, name = “input_layer”) %>% layer_dropout (rate = 0.5) %>% layer_dense (units = unit,activation = ‘relu’, kernel_initializer = initializer,name=“hidden_layer1”) %>% layer_dropout(rate = 0.5) %>% layer_dense(units = unit,activation = ‘relu’, kernel_initializer = initializer,name=“hidden_layer2”) %>% layer_dropout(rate = 0.5) %>% layer_dense(units = unit,activation = ‘relu’, kernel_initializer = initializer,name=“hidden_layer3”) %>% layer_dropout(rate = 0.5) %>% layer_dense(units = unit,activation = ‘relu’, kernel_initializer = initializer,name=“hidden_layer4”) %>% layer_dropout(rate = 0.5) %>% layer_dense(units = unit,activation = ‘relu’, kernel initializer = initializer,name=“hidden_layer5”) %>% layer_dropout (rate = 0.5) %>% layer dense (units = nb_classes,name = “output_layer”)%>% layer_activation (activation = ‘softmax’) model$summary # Compile model model %>% compile ( loss = ‘categorical_crossentropy’, optimizer = optimizer_adam(), metrics = c(‘accuracy’) ) model %>% fit ( x_train, y_train, batch_size = 500, epoch=50 ) scores<-model%>%evaluate (x_test, y_test,verbose=0) print(scores) |
| Algorithm 2. Convolutional NN |
| #init model model <- keras_model_sequential() n_filter<-512 # Build Model model <- model %>% layer_conv_2d (filters = n_filter, kernel_size = c (3,3), activation = ‘relu’, input_shape = input_shape, padding = ‘same’,strides = c(2,2)) %>% layer_dropout(rate = 0.50) %>% layer_conv_2d (filters = (n_filter*2), kernel_size = c (3,3), activation = ‘relu’, padding = ‘same’,strides = c(2,2)) %>% layer_dropout(rate = 0.5) %>% layer_conv_2d (filters = (n_filter*4), kernel_size = c (3,3), activation = ‘relu’, padding = ‘same’,strides = c(2,2)) %>% layer_max_pooling_2d (pool_size = c (2, 2), padding = ‘same’) %>% layer_dropout(rate = 0.5) %>% layer_flatten() %>% # 2D ->1D layer_dense(units = n_filter, activation = ‘relu’) %>% layer_dropout(rate = 0.5) %>% layer_dense(units = nb_classes, activation = ‘softmax’) # Compile model model %>% compile ( loss = ‘categorical_crossentropy’, optimizer = optimizer_adadelta(), metrics = c(‘accuracy’) ) # Train model model %>% fit ( x_train, y_train, batch_size = 500, epochs = 50, verbose=1 ) scores <- model %>% evaluate ( x_test, y_test, verbose = 0 ) |
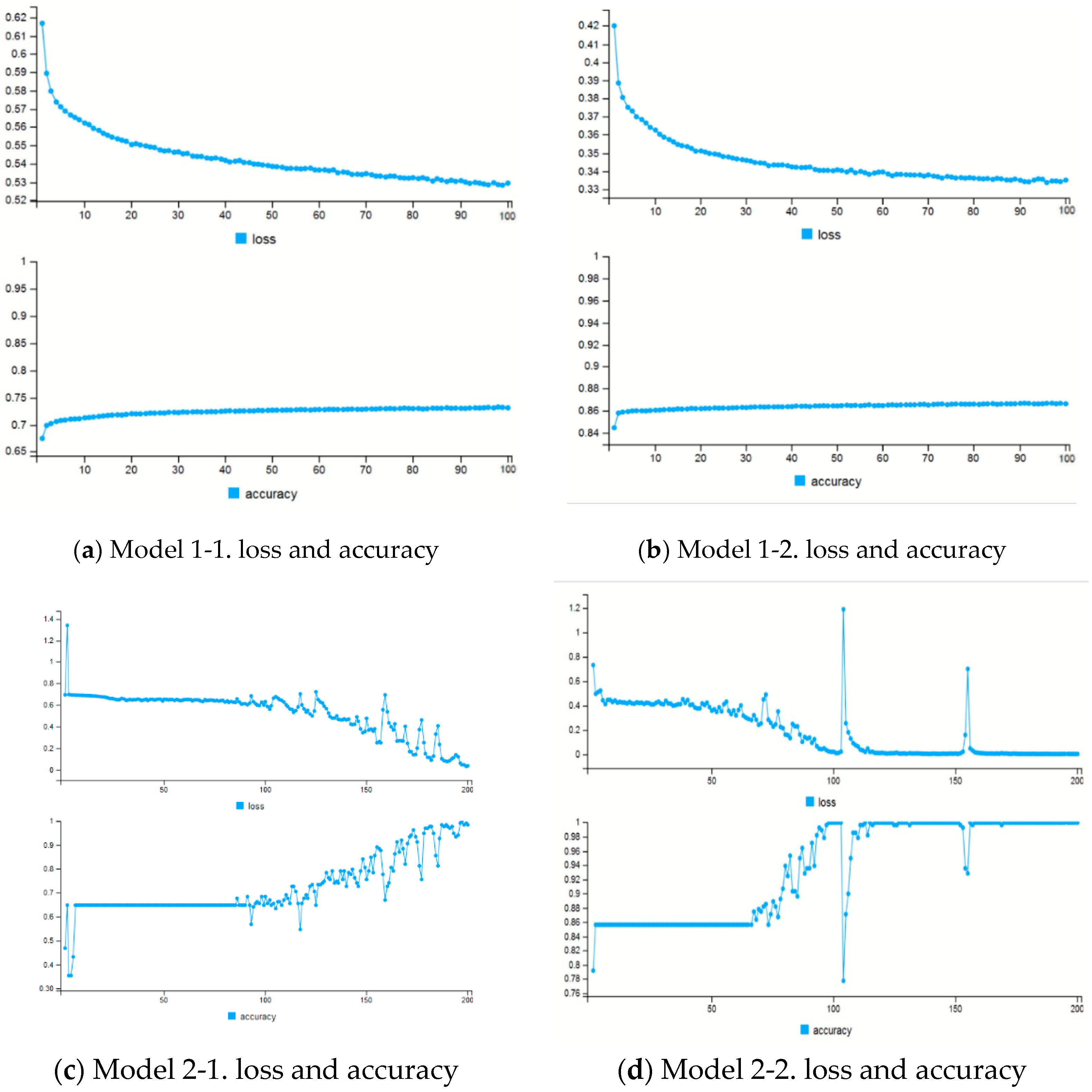
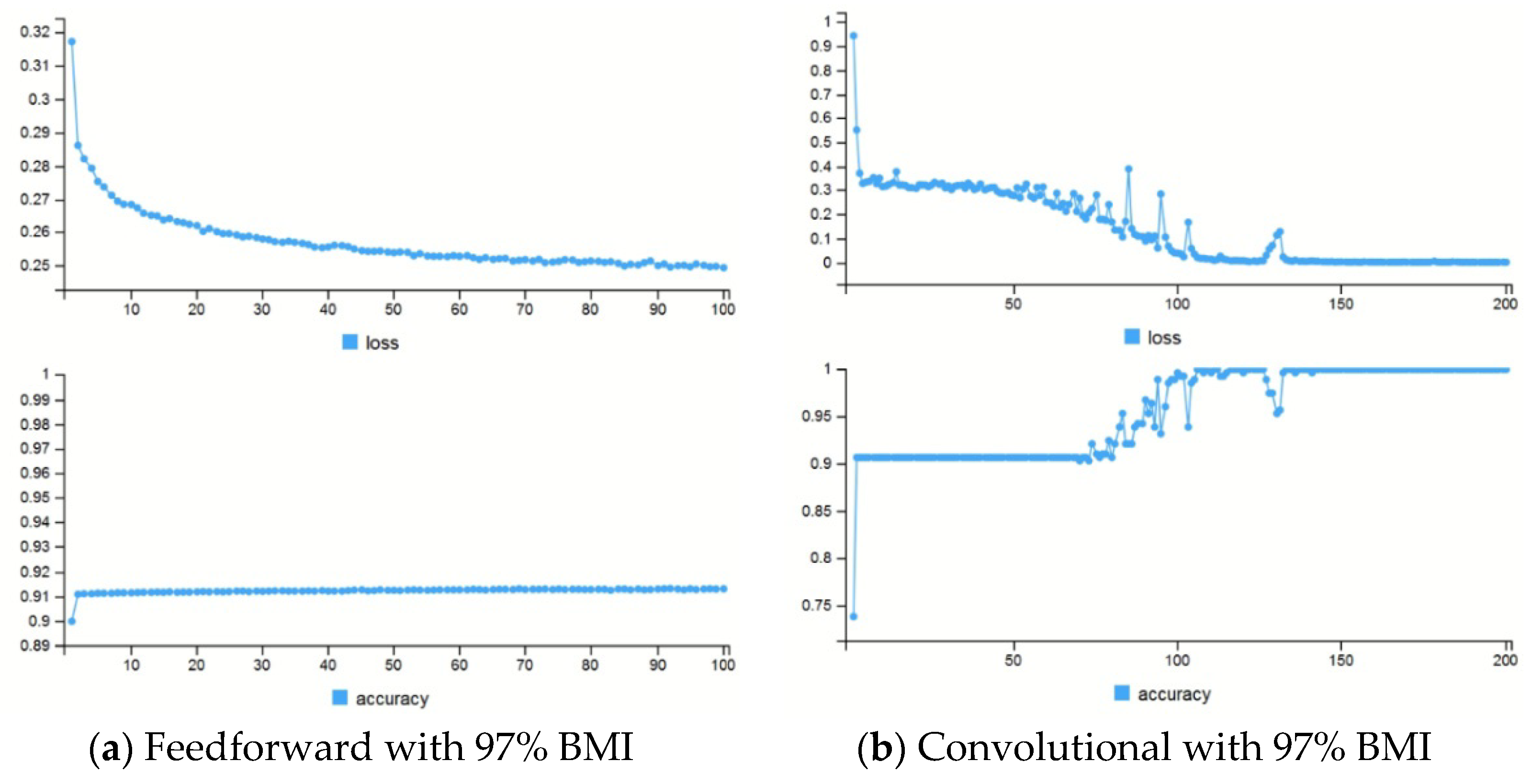
4. Experimental Result
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- NIH. Why Obesity Is a Health Problem. NIH. 13 February 2013. Available online: https://www.nhlbi.nih.gov/health/educational/wecan/healthy-weight-basics/obesity.htm#:~:text=Health%20Problems%20Linked%20to%20Obesity,-Obesity%20in%20childhood&text=In%20adults%2C%20overweight%20and%20obesity,overweight%20or%20obese%20as%20adults (accessed on 6 July 2020).
- Lawrence, V.J.; Kopelman, P. Medical consequences of obesity. Clinics in Dermatology. Clin. Dermatol. 2004, 22, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Allison, D.B.; Fontaine, K.R.; Manson, J.E.; Stevens, J.; VanItallie, T.B. Annual Deaths Attributable to Obesity in the United States. JAMA 1999, 282, 1530–1538. [Google Scholar] [CrossRef] [PubMed]
- Office of the Surgeon General (US); Office of Disease Prevention and Health Promotion (US); Centers for Disease Control and Prevention (US); National Institutes of Health (US). The Surgeon General’s Call To Action To Prevent and Decrease Overweight and Obesity. Rockville (MD): Office of the Surgeon General (US); 2001. Section 1: Overweight and Obesity as Public Health Problems in America. Available online: https://www.ncbi.nlm.nih.gov/books/NBK44210/ (accessed on 26 December 2011).
- Daniels, S.R.; Arnett, D.K.; Eckel, R.H.; Gidding, S.S.; Hayman, L.L.; Kumanyika, S.; Robinson, T.N.; Scott, B.J.; Jeor, S.S.; Williams, C.L. Overweight in Children and Adolescents: Pathophysiology, Consequences, Prevention, and Treatment. Circulation 2005, 111, 1999–2012. [Google Scholar] [CrossRef] [Green Version]
- Dehghan, M.; Akhtar-Danesh, N.; Merchant, A.T. Childhood obesity, prevalence and prevention. Nutr. J. 2005, 4, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, A.G.; Auman, N.L.; Collier, D.N.; Blaise Williams, D.S. Frontal Plane Lower Extremity Biomechanics during Walking in. Pediatric Phys. Ther. 2009, 21, 187–193. [Google Scholar] [CrossRef]
- Dufeka, J.S.; Curriea, R.L.; Gouwsa, P.-L.; Candelab, L.; Gutierrezb, A.P.; Mercera, J.A.; Putney, G. Effects of Overweight and Obesity on Walking Characteristics in Adolescents. Hum. Mov. Sci. 2012, 31, 897–906. [Google Scholar] [CrossRef]
- DeVita, P.; Devita, T.H. Obesity Is Not Associated with Increased Knee Joint Torque and Power during Level Walking. J. Biomech. 2003, 36, 1355–1362. [Google Scholar] [CrossRef]
- Browning, R.C.; Kram, R. Effects of Obesity on the Biomechanics of Walking at Different Speeds. Med. Sci. Sports Exerc. 2007, 39, 1632–1641. [Google Scholar] [CrossRef]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The Impact of Childhood Obesity on Musculoskeletal Form. Obes. Rev. 2006, 7, 209–218. [Google Scholar] [CrossRef]
- Gaerlan, M.G. The Role of Visual, Vestibular, and Somatosensory Systems in Postural Balance. UNLV Dissertation, University of Nevada, Las Vegas, LV, USA, 2010. [Google Scholar]
- Paillard, T.; Noé, F. Techniques and Methods for Testing the Postural Function in Healthy and Pathological Subjects. BioMed Res. Int. 2015, 891390. [Google Scholar] [CrossRef] [Green Version]
- Bruttini, C.; Esposti, R.; Bolzoni, F.; Vanotti, A.; Mariotti, C.; Cavallari, P. Temporal Disruption of Upper-Limb Anticipatory Postural Adjustments in Cerebellar Ataxic Patients. Exp. Brain Res. 2014, 233, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Tangen, G.G.; Engedal, K.; Bergland, A.; Moger, T.A.; Mengshoel, A.M. Relationships between Balance and Cognition in Patients with Subjective Cognitive Impairment, Mild Cognitive Impairment, and Alzheimer Disease. Phys. Ther. 2014, 94, 1126–1134. [Google Scholar] [CrossRef] [Green Version]
- Montecchi, M.G.; Muratori, A.; Lombardi, F.; Morrone, E.; Brianti, R. Recovery Scale: A New Tool to Measure Posture Control in Patients with Severe Acquired Brain Injury. A Study of the Psychometric Properties. Eur. J. Phys. Rehabil. Med. 2013, 49, 341–351. [Google Scholar] [PubMed]
- Dirnberger, G.; Jahanshahi, M. Executive Dysfunction in Parkinson’s Disease: A Review. J. Neuropsychol. 2013, 7, 193–224. [Google Scholar] [CrossRef] [PubMed]
- Chastan, N.; Do, M.C.; Bonneville, F.; Torny, F.; Bloch, F.; Westby, G.W.M.; Dormont, D.; Agid, Y.; Welter, M.-L. Gait and Balance Disorders in Parkinson’s Disease: Impaired Active Braking of the Fall of Centre of Gravity. Mov. Disord. 2009, 24, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Tomomitsu, M.S.V.; Alonso, A.C.; Morimoto, E.; Bobbio, T.G.; Greve, J. Static and Dynamic Postural Control in Low-Vision and Normal-Vision Adults. Clinics 2013, 68, 517–521. [Google Scholar] [CrossRef]
- Huiying, L.; Sakari, L.; Iiro, H. A Heart Sound Segmentation Algorithm Using Wavelet Decomposition and Reconstruction. In Proceedings of the 19th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 30 October–2 November 1997. [Google Scholar]
- Tsuruoka, R.S.Y. Spectral Analysis in Walking Balance by Elderly Subjects. In Proceedings of the 28th IEEE EMBS Annual International Conference, New York, NY, USA, 30 August–3 September 2006. [Google Scholar]
- Tsuruoka, M.; Tsuruoka, Y.; Shibasaki, R.; Yasuoka, Y. Spectral Analysis of Walking with Shoes and without Shoes. In Proceedings of the International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006. [Google Scholar]
- Ali, N.S. Prediction of Coronary Heart Disease Preventive Behaviors in Women: A Test of the Health Belief Model. Women Health 2002, 35, 83–96. [Google Scholar] [CrossRef]
- Rosenstock, I.M.I. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–333. [Google Scholar] [CrossRef]
- Sivalingam, S.K.; Ashraf, J.; Vallurupalli, N.; Friderici, J.; Cook, J.; Rothberg, M.B. Ethnic Differences in the Self-Recognition of Obesity and Obesity-Related Comorbidities: A Cross-Sectional Analysis. J. Gen. Intern. Med. 2011, 26, 616–620. [Google Scholar] [CrossRef] [Green Version]
- Sidorov, J.E.; Fitzner, K. Obesity Disease Management Opportunities and Barriers. Obesity 2006, 14, 645–649. [Google Scholar] [CrossRef] [Green Version]
- DrAnderson, J.W.; Konz, E.C. Obesity and Disease Management: Effects of Weight Loss on Comorbid Conditions. Obes. Res. 2001, 9, 326–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Lee, S.; Salado, L.; Estrada, J.; White, J.; Muthukumar, V.; Lee, S.-P.; Mohapatra, S. Proof-of-Concept Testing of a Real-Time mHealth Measure to Estimate Postural Control during Walking: A Potential Application for Mild Traumatic Brain Injuries. Application for Mild Traumatic Brain Injuries. Asian/Pac. Isl. Nurs. J. 2018, 3, 177–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Developers, A. Motion Sensors. Available online: https://developer.android.com/guide/topics/sensors/sensors_motion (accessed on 10 December 2020).
- Developers, A. API Reference. Available online: https://developer.android.com/reference (accessed on 10 April 2020).
- BMI Percentile Calculator for Child and Teen: Results on a Growth Chart. Available online: https://www.cdc.gov/healthyweight/bmi/resultgraph.html?&method=english&gender=m&age_y=14&age_m=7&hft=5&hin=10&twp=200 (accessed on 20 July 2020).
- Data Table of BMI-for-age Charts. 2001. Available online: https://www.cdc.gov/growthcharts/html_charts/bmiagerev.htm (accessed on 4 August 2020).
- Lee, S.; Walker, R.M.; Kim, Y.; Lee, H. Measurement of Human Walking Movements by Using a Mobile Health App: Motion Sensor Data Analysis. JMIR mHealth uHealth 2021, 9, e24194. [Google Scholar] [CrossRef]
- Incel, O.D. Analysis of Movement, Orientation and Rotation-Based Sensing for Phone Placement Recognition. Sensors 2015, 15, 25474–25506. [Google Scholar] [CrossRef]
- Sabatini, A.M. Estimating Three-Dimensional Orientation of Human Body Parts by Inertial/Magnetic Sensing. Sensors 2011, 11, 1489–1525. [Google Scholar] [CrossRef] [Green Version]
- Davenport, P.B. Rotations about Non orthogonal Axes. Aeronaut. Astronaut. J. (AIAA) 1973, 11, 853–858. [Google Scholar] [CrossRef]
- RDocumentation. Random Samples and Permutations. Available online: https://www.rdocumentation.org/packages/base/versions/3.6.2/topics/sample (accessed on 21 May 2020).
- RStudio. Keras. Available online: https://keras.rstudio.com/ (accessed on 22 May 2020).
- TensorFlow. Available online: https://www.tensorflow.org/ (accessed on 4 June 2021).
- Glorot, X.; Bengio, Y. Understanding the Difficulty of Training Deep Feedforward Neural Networks. In Proceedings of the 13th International Conference on Artificial Intelligence and Statistics (AISTATS), Sardinia, Italy, 13–15 May 2010. [Google Scholar]
- Nair, V.; Hinton, G.E. Rectified Linear Units Improve Restricted Boltzmann Machines. In Proceedings of the 27th International Conference on Machine Learning, Haifa, Israel, 21 June 2010; pp. 807–814. [Google Scholar]
- Bishop, C.M. Pattern Recognition and Machine Learning; Springer AG: New York, NY, USA, 2012; Available online: https://link.springer.com/book/9780387310732 (accessed on 1 January 2022).
- Freedman, D.S.; Khan, L.K.; Serdula, M.K.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. The Relation of Childhood BMI to Adult Adiposity: The Bogalusa Heart Study. Pediatrics 2005, 115, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscogiuri, G.; Palomba, S.; Laganà, A.S.; Orio, F. Current Insights into Inositol Isoforms, Mediterranean and Ketogenic Diets for Polycystic Ovary Syndrome: From Bench to Bedside. Curr. Pharm. Des. 2016, 22, 5554–5557. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
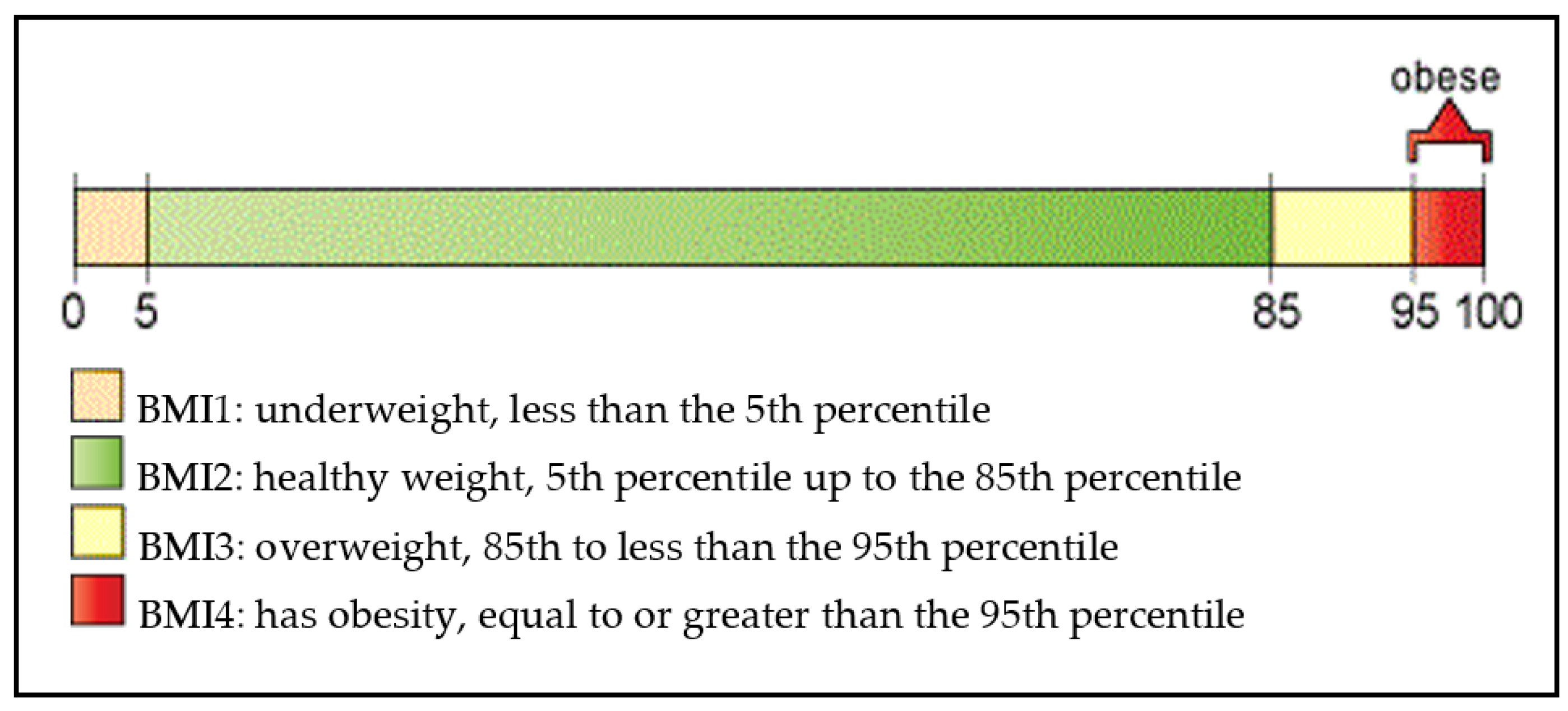
| Gender | 3% | 5% | 10% | 25% | 50% | 75% | 85% | 90% | 95% | 97% |
|---|---|---|---|---|---|---|---|---|---|---|
| Female | 15.69 | 16.06 | 16.68 | 17.91 | 19.65 | 22.02 | 23.71 | 25.10 | 27.70 | 28.27 |
| Male | 15.93 | 16.27 | 16.84 | 17.95 | 19.51 | 21.60 | 23.06 | 24.25 | 26.45 | 29.9 |
| Characteristic | Overall (n = 170) | BMI 1 (<=5%) | BMI 2 (>5% & <=85%) | BMI 3 (>85% & <95%) | BMI 4 (>=95%) |
|---|---|---|---|---|---|
| Gender | |||||
| Female | 86 (50.59%) | 2 (2.33%) | 55 (63.95%) | 21 (24.42%) | 8 (9.30%) |
| Male | 84 (49.41%) | 2 (2.38%) | 51 (60.71%) | 14 (16.67%) | 17 (20.24%) |
| Race | |||||
| Hispanic | 18 (10.59%) | 0 | 13 (72.22%) | 4 (22.22%) | 1 (5.56%) |
| White | 133 (78.24%) | 4 (3.01%) | 83 (62.41%) | 26 (19.55%) | 20 (15.04%) |
| Black | 3 (1.76%) | 0 (0.00%) | 0 (0.00%) | 3 (100.00%) | 0 (0.00%) |
| Asian | 4 (2.35%) | 0 (0.00%) | 2 (50.00%) | 1 (25.00%) | 1 (25.00%) |
| Other | 12 (7.06%) | 0 (0.00%) | 5 (41.67%) | 4 (33.33%) | 3 (25.00%) |
| Total | 170 | 4 (2.35%) | 106 (62.35%) | 35 (20.59%) | 25 (14.71%) |
| Dataset | Loss (Feedforward) | Accuracy (Feedforward) | Loss (Convolutional) | Accuracy (Convolutional) |
|---|---|---|---|---|
| Dataset 1 | 4.998 (Model 1-1) | 61.8% (Model 1-1) | 3.551 (Model 2-1) | 54.8% (Model 2-1) |
| Dataset 2 | 0.979 (Model 1-2) | 90.5% (Model 1-2) | 2.12 (Model 2-2) | 79% (Model 2-2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Hwang, E.; Kim, Y.; Demir, F.; Lee, H.; Mosher, J.J.; Jang, E.; Lim, K. Mobile Health App for Adolescents: Motion Sensor Data and Deep Learning Technique to Examine the Relationship between Obesity and Walking Patterns. Appl. Sci. 2022, 12, 850. https://doi.org/10.3390/app12020850
Lee S, Hwang E, Kim Y, Demir F, Lee H, Mosher JJ, Jang E, Lim K. Mobile Health App for Adolescents: Motion Sensor Data and Deep Learning Technique to Examine the Relationship between Obesity and Walking Patterns. Applied Sciences. 2022; 12(2):850. https://doi.org/10.3390/app12020850
Chicago/Turabian StyleLee, Sungchul, Eunmin Hwang, Yanghee Kim, Fatih Demir, Hyunhwa Lee, Joshua J. Mosher, Eunyoung Jang, and Kiho Lim. 2022. "Mobile Health App for Adolescents: Motion Sensor Data and Deep Learning Technique to Examine the Relationship between Obesity and Walking Patterns" Applied Sciences 12, no. 2: 850. https://doi.org/10.3390/app12020850