
Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength


1
Faculty of Health Sciences, University of Primorska, 6310 Izola, Slovenia
2
Faculty of Kinesiology, University of Zagreb, 10000 Zagreb, Croatia
3
Motus Melior Ltd., 10000 Zagreb, Croatia
4
S2P, Science to Practice, Ltd., Laboratory for Motor Control and Motor Behavior, 1000 Ljubljana, Slovenia
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(8), 3391; https://doi.org/10.3390/app11083391
Submission received: 15 January 2021
/
Revised: 12 February 2021
/
Accepted: 7 April 2021
/
Published: 9 April 2021
(This article belongs to the Special Issue Applied Biomechanics for Injury Prevention and Performance)
Abstract
:The purpose of this study was to evaluate intra- and inter-session reliability of the new, portable, and externally fixated dynamometer called MuscleBoard® for assessing the strength of hip and lower limb muscles. Hip abduction, adduction, flexion, extension, internal and external rotation, knee extension, ankle plantarflexion, and Nordic hamstring exercise strength were measured in three sessions (three sets of three repetitions for each test) on 24 healthy and recreationally active participants. Average and maximal value of normalized peak torque (Nm/kg) from three repetitions in each set and agonist:antagonist ratios (%) were statistically analyzed; the coefficient of variation and intra-class correlation coefficient (ICC2,k) were calculated to assess absolute and relative reliability, respectively. Overall, the results display high to excellent intra- and inter-session reliability with low to acceptable within-individual variation for average and maximal peak torques in all bilateral strength tests, while the reliability of unilateral strength tests was moderate to good. Our findings indicate that using the MuscleBoard® dynamometer can be a reliable device for assessing and monitoring bilateral and certain unilateral hip and lower limb muscle strength, while some unilateral strength tests require some refinement and more extensive familiarization.
1. Introduction
Measurement of athletes’ hip and lower limb muscle strength is a common practice in amateur and professional sports. Indeed, numerous research studies have demonstrated the importance of muscular strength in athletic performance (for review, see Suchomel et al. [1]) and an association between insufficient hip and lower limb muscle strength and an increased muscle injury risk in field-based sports (e.g., soccer, rugby, ice hockey, American football, etc.) [2,3,4,5,6]. Aside from performance optimization and injury prevention in sports, assessment of hip and lower limb muscle strength is also relevant for prevention and treatment of injuries in older individuals [7].
Three main methods for measuring hip and lower limb muscle strength are being used in sports and clinical settings. Isokinetic dynamometry is currently considered as the gold standard for assessing human muscle strength; however, its use is often limited to a laboratory setting as these devices are expensive and not portable. Manual muscle testing is practical and a device-independent method; however, its reliability is questionable and depends to a large extent on the experience of the examiner [8]. Finally, hand-held dynamometry is a valid, reliable, portable, and more accessible strength assessment method compared with isokinetic dynamometry [9]. However, studies have shown that the validity and reliability of hand-held dynamometric measurements depend on external stabilization because measurement characteristics often rely on an examiner’s strength [10,11]. In addition, there is considerable variability in test procedures, with substantial effects of body position (supine, prone, side-lying, standing, sitting), stabilization methods (manually vs. non-elastic straps), and dynamometer placement (short vs. long lever arm) being reported [12].
Therefore, new, externally fixed (independent of examiner’s strength), portable, easy to use, and accessible dynamometers with standardized test protocols are needed. One externally fixed dynamometer called GroinBar (later renamed ForceFrame) has recently been introduced and evaluated [13,14,15]; however, this device does not allow the measurement of lower body muscles. To this end, a new portable dynamometer called MuscleBoard® was recently developed to assess the bilateral and unilateral strength of the hip muscles in all planes, as well as knee flexors, knee extensors, and plantar flexors. The purpose of the study was to verify the intra- and inter-session reliability of this novel strength testing device. We hypothesized that this new dynamometer system would produce good to excellent intra- and inter-session reliability results with low within-individual variation.
2. Materials and Methods
2.1. Participants
Twenty-four participants (17 males, 7 females) were included in the study (average ± SD: age = 21.9 ± 3.6 years, height = 1.79 ± 0.1 m, mass = 75.6 ± 13.8 kg, body mass index = 23.4 ± 2.2 kg/m2, body fat = 16.6 ± 4.7%, muscle mass = 79.2 ± 4.5%). All participants self-reported as being recreationally active (>three hours of physical activity per week). Twenty of them were current/former athletes who participated in the following sports: soccer (10), basketball (4), martial arts (3), volleyball (1), cheerleading (1), powerlifting (1). Exclusion criteria were neurological, muscular, skeletal, or connective tissue injuries during the last 12 months in the area of the back, hips, and/or legs. All participants were informed about the purpose and content of the study and gave written informed consent prior to participation. The study was approved by the National Medical Ethics Committee (0120-690/2017/8) and conducted in accordance with the latest revision of the Helsinki Declaration.
2.2. Study Protocol
Anthropometrical variables were assessed with a stadiometer and a multi-frequency bio-impedance scale (Tanita MC-980MA, Tanita, Tokyo, Japan). Participants then performed a standardized warm-up, consisting of: (a) 6 min stepping on/off a 25 cm high box, changing the lead leg every minute; (b) dynamic stretching exercises (8 repetitions of hip circles; forward, backward, and side hip bending; leg swings in frontal and sagittal plane); and (c) bodyweight strength exercises with emphasis on the trunk and lower limb muscles (10 repetitions of squats, heel raises, hip bridges, Jackknife sit-ups, and hip extensions). After the warm-up, the participants underwent isometric strength measurements with the dynamometer MuscleBoard®, as previously described by Marković et al. [16] on an earlier version of the device. Two “U”-shaped and padded aluminum braces (Figure 1), attached to uniaxial load cells (FL34-100 kg; Forsentek Co., Shenzhen, China), were used to measure forces (N), separately for each limb.
Nine tests (shown and described in Figure 2 and Table 1) were performed in a randomized order within a single session. Each test was repeated three times (maximal voluntary isometric contraction for 5 s) with 45–60 s break between repetitions. The break between the tests was set at 180 s. Three sessions were performed as follows: first and second sessions were performed on the same day, separated by a 45–60 min break (to analyze intra-session reliability), while the third session was performed one week after the first visit at the same hour (to analyze inter-session reliability). Hip abduction (HABD), hip adduction (HADD), hip internal rotation (HIR), hip external rotation (HER) were performed unilaterally and bilaterally, while knee extension (KEXT) and plantar flexion (PFLX) were performed only unilaterally. Nordic hamstring exercise (NHE) was performed bilaterally. In all unilateral variations, participant’s non-measured leg was next to the dynamometer to avoid any contact with the sensors. Unilateral contractions of the KEXT and PFLX were measured using a rigid bar that connected both sensor braces, so that a sum of forces from both load cells presented one (unilateral) measurement (shown in Figure 3).
For all isometric strength measurements, participants were instructed to place the measured limb(s) onto the appropriate side of the sensor braces or under the non-elastic strap (see Table 1 for more details) and asked to perform a maximum repetition by pushing their distal part of the lower leg against the brace/strap as hard as possible and holding it with maximum force for 5 s. For the NHE, participants were instructed to maintain straight knee-shoulder line during the descent, to hold arms and hands in front of the body, and to brake the forward fall for as long as possible. Standardized loud verbal encouragement was given during all measurements: “touch, get ready, push, push, push, relax”.
2.3. Data Analysis
Custom-developed software (ARS Dynamometry, S2P, Ljubljana, Slovenia; created in Labview 8.1., National Instruments, Austin, TX, USA) was used for recording and analyzing the signals, which were sampled at 1000 Hz and pre-processed with a 10 ms moving average filter. The signals were transferred to a computer using a two-channel amplifier (InsAmp, Isotel, Logatec, Slovenia) and an analogue-to-digital card (NIUSB-6009, National Instruments, Austin, TX, USA). The peak force values were multiplied by the lever arms (m) of the participants and normalized by their body mass to obtain normalized peak torques (Nm/kg) for each repetition. Lever arms were measured prior each test to the nearest 0.5 cm using the measurement scale on both edges of the dynamometer (shown in Figure 1) from sensor braces to: (i) greater trochanter for HFLX, HEXT, HABD, HADD; (ii) femoral epicondyle for HIR, HER, KEXT, and NHE; (iii) lateral malleoli for PFLX. Mean and maximal values of three repetitions, and agonist:antagonist ratio (%) for each test were calculated and statistically analyzed. No gravity corrections were performed for any strength test.
2.4. Statistical Analysis
The SPSS statistical package (version 25.0, IBM, New York, NY, USA) was used for statistical analysis. Descriptive statistics were calculated and reported as mean ± standard deviation, in addition to the 95% confidence intervals. Shapiro–Wilk test was used to verify normality of data. To assess absolute reliability, the coefficient of variation (CV) was calculated as the quotient between the typical measurement error and the mean value of both sessions, expressed in %. The relative reliability was assessed with intra-class correlation coefficient, using a 2-way random model with absolute agreement (ICC2,k) and was interpreted as poor (<0.5), moderate (0.5–0.75), good (0.75–0.9), and excellent (>0.9) [17]. The systematic bias was analyzed by analysis of variance with repeated measurements. The level of statistical significance was set at p < 0.05.
3. Results
3.1. Intra-Session Reliability
The peak torque values of all bilateral tests had very high intra-session reliability (Table 2). Specifically, no systematic bias, very high to excellent test-retest reliability (ICC2,k > 0.85), and low within-individual variation (CV < 9%) was shown for bilateral HADD (ICC2,k = 0.94; CV = 3.5–3.6%), HABD (ICC2,k = 0.86–0.87; CV = 7.8–8.6%), HIR (ICC2,k = 0.86–0.88; CV = 5.0–6.6%), HER (ICC2,k = 0.94–0.95; CV = 2.1–2.2%), and NHE (ICC2,k = 0.87–0.91; CV = 2.6–3.6%).
For unilateral strength tests, the peak torque values for HADD and HABD had high intra-session reliability, with no systematic bias, high test-retest reliability (ICC2,k = 0.77–0.90), and low within-individual variation (CV = 5.4–8.5%). For the remaining unilateral strength tests, the intra-session reliability of peak torques was moderate to good (Table 2). Specifically, no statistically significant systematic bias, moderate to good test-retest reliability, and low (CV < 9%) within-individual variation was shown for HEXT (ICC2,k = 0.69–0.81; CV = 3.9–6.4%), HFLX (ICC2,k = 0.60–0.69; CV = 7.3–8.2%), KEXT (ICC2,k = 0.67–0.84; CV = 5.6–10.0%). The exceptions were: peak torque of left leg during PFLX (ICC2,k = 0.43–0.44; CV = 6.3–6.4%) and peak torque of left leg during HFLX, which displayed statistically significant systematic bias (F = 7.56, p = 0.01; d = 0.46). Moderate to very high test-retest reliability (ICC2,k = 0.54–0.86) and low to moderate within-individual variation (CV = 6.2–18.7%) was shown for HIR and HER, with one unilateral measurement of HIR showing statistically significant systematic bias (F = 8.53, p = 0.01; d = 0.39).
Calculated agonist:antagonist ratios had in general lower intra-session reliability than peak torques (Table 3). In bilateral strength tests, the calculated agonist:antagonist ratios had no systematic bias, good to very good test-retest reliability (ICC2,k = 0.66–0.83), and acceptable within-individual variation (CV = 8.1–11.9%). In contrast, the calculated agonist:antagonist ratios for unilateral strength tests had lower intra-session reliability. Significant systematic bias was observed for unilateral HIR:HER and HFLX:HEXT ratios (d = 0.49 and 0.40, respectively), with ICC coefficients ranging from low (0.39 for the right HIR:HER ratio) to high (0.8 for the right FLX:EXT ratio) and CVs ranging from low (7.5% for the right FLX:EXT ratio) to high (22.5% for the right HIR:HER ratio).
3.2. Inter-Session Reliability
Results of inter-session reliability analysis are shown in Table 4. Again, the peak torque values of all bilateral tests had very high inter-session reliability. Specifically, no systematic bias, very high to excellent test-retest reliability (ICC2,k > 0.85), and low within-individual variation (CV < 9%) was shown for bilateral HADD (ICC2,k = 0.96–0.97; CV = 1.9–2.3%), HABD (ICC2,k = 0.94; CV = 2.7%), HIR (ICC2,k = 0.86–0.87; CV = 5.5–6.7%), HER (ICC2,k = 0.94–0.95; CV = 2.2–2.4%). The exception was NHE, which also had very high test-retest reliability and low within-individual variation (ICC2,k = 0.86–0.88; CV = 5.4–5.9%) but with systematic bias present for average peak torque (d = 0.29).
Regarding unilateral strength tests, the peak torque values for HADD, HABD, HIR, HEXT, and KEXT had generally high inter-session reliability, with no systematic bias, good to high test-retest reliability (ICC2,k = 0.66–0.90), and low to moderate within-individual variation (CV = 5.2–17.1%). For unilateral HER, statistically significant systematic bias was observed for one side (d = 0.49–0.50), ICC coefficients ranged from 0.68 to 0.76, and CVs ranged from 12.6% to 13.0%. For HFLX, statistically significant systematic bias was observed for all parameters: (ICC2,k = 0.58–0.81; CV = 7.4–14.7%; d = 0.45–0.76). The lowest inter-session reliability of peak torques was observed in PFLX, with ICC coefficients ranging from 0.44 to 0.68, CVs ranging from 5.7% to 7.2%, and with significant systematic bias for one side (F = 5.51–5.84, p = 0.02–0.03; d = 0.46–0.51).
The calculated agonist:antagonist ratios in bilateral strength tests had no systematic bias, with very high inter-session reliability for HADD:HABD ratios (ICC2,k = 0.89–0.92, CV = 3.2–4.4%) and good inter-session reliability for HIR:HER ratios (ICC2,k = 0.58–0.67; CV = 12.5–16.2%) (Table 5). For unilateral strength tests, the calculated agonist:antagonist ratios had lower inter-session reliability. Significant systematic bias was observed for unilateral left HFLX:HEXT ratios (d = 0.99), with ICC coefficients ranging from low (0.30 for the left HADD:HABD ratio) to high (0.78 for the right HIR:HER ratio) and CVs ranging from moderate (11.9% for the right HIR:HER ratio) to high (25.6% for the left HADD:HABD ratio).
4. Discussion
The purpose of this study was to evaluate inter- and intra-session reliability of the new, portable, and externally fixated dynamometer MuscleBoard® for assessing strength of hip and lower limb muscles. Overall, the results demonstrate high to excellent intra- and inter-session reliability with low to acceptable within-individual variation for average and maximal peak torques in all bilateral strength tests. Furthermore, the calculated agonist:antagonist ratios for bilateral strength tests also had good to high intra- and inter-session reliability. Conversely, the peak torques and calculated agonist:antagonist ratios for unilateral tests had lower intra- and inter-session reliability.
The results of strength assessments can be reported with different units of measurements (N, Nm, Nm/kg, N/kg, % of bodyweight, etc.), which makes the direct comparison of peak torques/forces from different studies difficult. Nevertheless, Tourville et al. (2013) [18] used externally fixated load cells to measure hip strength of ice hockey players and found similar results for HADD and HABD (157.5 ± 48.9 Nm vs. 158.8 ± 48.2 Nm and 155.7 ± 51.4 Nm vs. 154.8 ± 40.3 Nm from our study, respectively), higher HFLX (174.1 ± 66.9 Nm vs. 146.8 ± 40.8 Nm from our study) and lower HEXT (146.7 ± 56.7 Nm vs. 199.8 ± 52.6 Nm from our study). Furthermore, HADD:HABD ratio of ~103% from bilateral measurement and HFLX:HEXT ratio of ~75% from unilateral measurement is in agreement with previous studies using the GroinBar device on football players [13,15], while measured HIR:HER ratio of ~96% from unilateral and 124% from bilateral measurement in our study is comparable to bilaterally measured the HIR:HER ratio of 108% from the study by Desmyttere et al. (2019) [15]. In addition, peak torques during the NHE showed high intra-session reliability, which is comparable to other similar devices for measuring forces during the NHE—namely, Opar et al. (2015) [19], who tested the NordBord device, and Lodge et al. (2020) [20], who recently tested the Hamstring Solo Elite device. This is a particularly important measurement characteristic of dynamometers since eccentric strength of the hamstrings (measured during the NHE but not on the isokinetic dynamometer) [21,22] is a significant risk factor for the occurrence of hamstring strain injuries [23]. Another important measurement characteristic of the device in the context of prevention/rehabilitation of hamstring injuries is the ability to measure forces for each limb separately since inter-limb strength asymmetry during the NHE is another risk factor for hamstring injuries [24].
We observed high to excellent intra- and inter-session reliability for bilateral tests of HADD, HABD, HIR, and HER and moderate to good intra-session reliability results for unilateral tests of HFLX and HEXT. This is comparable to the results of the study by Desmyttere et al. (2019) [15], in which they used the GroinBar device, a similar externally fixated dynamometer. Results are similar despite the following differences in body positions and lever arm lengths: HFLX was measured in 90° hip flexion with short lever arm compared to our measurement of HFLX in neutral position with long lever arm; HEXT in prone position in 4-point support and 90° knee flexion with short lever arm compared to prone lying position with neutral knee position and with long lever arm; HADD and HABD in supine position with 45° knee and hip flexion with short lever arm compared to supine position and neutral position in hip and knee joint with long lever arm; and HIR and HER in supine position with hip and knee in 90° flexion compared to prone position in 4-point support. Furthermore, Ryan et al. (2018) [14] found similar low within-individual variation (CV < 10%) and excellent reliability using the GroinBar device for bilateral HADD peak force compared with results from our study. In addition, hip strength measurements using hand-held dynamometry displayed comparable (moderate to excellent) reliability [25,26,27]. Based on the abovementioned findings, it can be concluded that the externally fixated dynamometer MuscleBoard® analyzed in our study could be a reliable alternative for assessing hip and lower limb strength compared to hand-held dynamometry, as it is not dependent on examiner’s strength. Additionally, handling this dynamometer requires less knowledge and experience compared to hand-held dynamometry.
When measuring HADD, HABD, HIR, and HER, bilateral contractions had systematically better (good to excellent) intra- and inter-session test-retest reliability compared with unilateral contractions. There could be two main reasons that made maximal voluntary isometric contractions (more) difficult to perform during unilateral contractions: (i) lack of stabilization/fixation of body position and (ii) participants’ division of attention. Participants were instructed to abduct or rotate the non-measured leg outside of sensor braces and to maintain this position during unilateral measurements in addition to generating maximal isometric torque with the measured leg. This seemed even more difficult during unilateral abduction and adduction in the supine position, as the peak torque generated with the measured leg was partly dependent on strong fixation of the trunk, upper body, and non-measured leg. Thus, in our case, participants resisted with the non-measured leg at the outer edge of the dynamometer to improve stabilization during unilateral adduction. During unilateral abduction, participants tried to stabilize themselves by pushing the non-measured leg into the ground, which occasionally caused a slight movement of the dynamometer in the direction of abduction of the measured leg. To prevent this movement, the examiner had to provide additional external stabilization (by holding the dynamometer in place). Moreover, the absence of bilateral deficit (reduction of the produced force from a single leg during maximal bilateral contraction) could be explained by the same two factors (lack of body position stabilization/fixation and division of attention during unilateral measurements). The sum of peak torques for the unilaterally measured left and right leg was lower than peak torques for the bilaterally measured test in all three sessions (e.g., for the adduction in the first session: 2.09 Nm/kg for bilateral test, >0.77 Nm/kg for the right leg, + 0.77 Nm/kg for the left leg). To our knowledge, this is the first study in which both the reliability of bilateral and unilateral contractions was tested on this type of externally fixated dynamometer. It would be interesting to see if the participants would achieve comparable results in terms of bilateral deficit on similarly designed dynamometers (e.g., GroinBar device).
An advantage of the MuscleBoard® compared to other recently introduced portable, externally fixed dynamometers, is its ability to measure the strength of knee extensors and plantarflexors. Specifically, knee extension strength has been repeatedly shown to be essential in monitoring the rehabilitation process following anterior cruciate ligament reconstruction [28,29], while plantarflexor strength is associated with mid-portion Achilles tendinopathy [30]. The current study showed moderate to high intra- and inter-session reliability of testing strength of these muscle groups, suggesting that MuscleBoard® has the potential to be used in clinical settings related to knee and Achilles tendon injuries.
Inter-session reliability was generally lower compared with intra-session reliability, with a higher number of measured parameters showing a statistically significant systematic bias. This was particularly evident for the NHE and HFLX tests. The reasons could be in participants’ motor learning and task/measurement procedure familiarization, as they had already performed six repetitions before third measurement session started. It is, therefore, suggested that each participant perform one familiarization session before the first official measurement of these muscle groups with the MuscleBoard® device.
Some limitations of the present study need to be acknowledged. The measurement for each muscle group was performed in only one body position. Different body positions could significantly influence produced peak torques or the reliability of the measurements. For example, HADD maximal strength can be evaluated with different hip and knee flexion angles, which could have a significant impact on peak HADD torques and peak muscle activity [31]. Further studies are needed to test the reliability of the MuscleBoard® dynamometer for different body positions within the same muscle group. Moreover, a certain degree of learning effect, which could have notably influenced the reliability between the sessions, cannot be ruled out. Hence, a more extensive familiarization (particularly for unilateral test) and, possibly, better stabilization with the arms is warranted when individuals or groups are being tested with a MuscleBoard® device for the first time.
5. Conclusions
Our results indicate a high to excellent intra- and inter-session reliability of the new, portable, and externally fixated dynamometer MuscleBoard® for assessing bilateral hip and lower limb muscle strength and agonist:antagonist strength ratios. Lower (i.e., moderate to good) intra- and inter-session reliability was generally shown for unilateral hip and lower limb muscle strength. These findings can be a good basis for further use of the described dynamometer in research- and clinical-based environments, where objective, easy to use, and reliable measurement of hip and lower limb strength is both important and necessary. Future studies are needed to evaluate the MuscleBoard® device in sports and clinical settings.
Author Contributions
Conceptualization, N.Š. and G.M.; methodology, J.M., N.Š. and G.M.; software, N.Š.; validation, J.M., N.Š. and G.M.; formal analysis, J.M.; investigation, J.M.; resources, N.Š.; data curation, J.M. and G.M.; writing—original draft preparation, J.M.; writing—review and editing, J.M., G.M. and N.Š.; visualization, N.Š.; supervision, N.Š.; funding acquisition, N.Š. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Slovenian Research Agency through the programme “Kinesiology of monostructural, polystructural and conventional sports” [P5-0147 (B)] and the project TELASI-PREVENT [L5-1845] (Body asymmetries as a risk factor in musculoskeletal injury development: studying aetiological mechanisms and designing corrective interventions for primary and tertiary preventive care).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the National Medical Ethics Committee of Slovenia (approval number 0120-690/2017/8).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent to publish this paper was obtained from the patient(s).
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
G.M. and N.Š. are co-owners of the company that developed MuscleBoard® and is planning its commercialization. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Suchomel, T.J.; Nimphius, S.; Stone, M.H. The Importance of Muscular Strength in Athletic Performance. Sport. Med. 2016, 46, 1419–1449. [Google Scholar] [CrossRef]
- Timmins, R.G.; Bourne, M.N.; Shield, A.J.; Williams, M.D.; Lorenzen, C.; Opar, D.A. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): A prospective cohort study. Br. J. Sports Med. 2016, 50, 1524–1535. [Google Scholar] [CrossRef]
- Ryan, J.; Deburca, N.; Creesh, K.M. Risk factors for groin / hip injuries in field-based sports: A systematic review. Br. J. Sports Med. 2014, 48, 1–8. [Google Scholar] [CrossRef]
- Mosler, A.B.; Agricola, R.; Weir, A.; Hölmich, P.; Crossley, K.M. Which factors differentiate athletes with hip / groin pain from those without? A systematic review with. Br. J. Sports Med. 2015, 49, 810. [Google Scholar] [CrossRef]
- Opar, D.A.; Williams, M.D.; Shield, A.J. Hamstring strain injuries: Factors that Lead to injury and re-Injury. Sport. Med. 2012, 42, 209–226. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Tanaka, M.; Shida, M. Intrinsic Risk Factors of Lateral Ankle Sprain: A Systematic Review and Meta-analysis. Sports Health 2016, 8, 190–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, S.C.; Goodheart, G.J. On the reliability and validity of manual muscle testing: A literature review. Chiropr. Osteopat. 2007, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, T.; Walker, B.; Phillips, J.K.; Fejer, R.; Beck, R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM R 2011, 3, 472–479. [Google Scholar] [CrossRef]
- Thorborg, K.; Bandholm, T.; Schick, M.; Jensen, J.; Hölmich, P. Hip strength assessment using handheld dynamometry is subject to intertester bias when testers are of different sex and strength. Scand. J. Med. Sci. Sport. 2013, 23, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Thorborg, K.; Bandholm, T.; Hölmich, P. Hip- and knee-strength assessments using a hand-held dynamometer with external belt-fixation are inter-tester reliable. Knee Surg. Sport. Traumatol. Arthrosc. 2013, 21, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Krause, D.A.; Schlagel, S.J.; Stember, B.M.; Zoetewey, J.E.; Hollman, J.H. Influence of Lever Arm and Stabilization on Measures of Hip Abduction and Adduction Torque Obtained by Hand-Held Dynamometry. Arch. Phys. Med. Rehabil. 2007, 88, 37–42. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.; Bourne, M.; Heerey, J.; Timmins, R.G.; Pizzari, T. A novel device to assess hip strength: Concurrent validity and normative values in male athletes. Phys. Ther. Sport 2019, 35, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, S.; Kempton, T.; Pacecca, E.; Coutts, A.J. Measurement Properties of an Adductor Strength Assessment System in Professional Australian Footballers. Int. J. Sports Physiol. Perform. 2018, 14, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Desmyttere, G.; Gaudet, S.; Begon, M. Test-retest reliability of a hip strength assessment system in varsity soccer players. Phys. Ther. Sport 2019, 37, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Markovic, G.; Šarabon, N.; Pausic, J.; Hadžić, V. Adductor muscles strength and strength asymmetry as risk factors for groin injuries among professional soccer players: A prospective study. Int. J. Environ. Res. Public Health 2020, 17, 4946. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 1988. [Google Scholar]
- Tourville, T.W.; Smith, H.C.; Shultz, S.J.; Vacek, P.M.; Slauterbeck, J.R.; Johnson, R.J.; Beynnon, B.D. Reliability of a New Stabilized Dynamometer System for the Evaluation of Hip Strength. Sports Health 2013, 5, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Opar, D.A.; Piatkowski, T.; Williams, M.D.; Shield, A.J. A novel device using the nordic hamstring exercise to assess eccentric knee flexor strength: A reliability and retrospective injury study. J. Orthop. Sports Phys. Ther. 2013, 43, 636–640. [Google Scholar] [CrossRef] [Green Version]
- Lodge, C.; Tobin, D.; O’Rourke, B.; Thorborg, K. Reliability and Validity of a New Eccentric Hamstring Strength Measurement Device. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100034. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; Bourne, M.N.; Pizzari, T. Isokinetic strength assessment offers limited predictive validity for detecting risk of future hamstring strain in sport: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 329–336. [Google Scholar] [CrossRef] [PubMed]
- van Dyk, N.; Witvrouw, E.; Bahr, R. Interseason variability in isokinetic strength and poor correlation with Nordic hamstring eccentric strength in football players. Scand. J. Med. Sci. Sport. 2018, 28, 1878–1887. [Google Scholar] [CrossRef] [Green Version]
- Van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef] [Green Version]
- Bourne, M.N.; Opar, D.A.; Williams, M.D.; Shield, A.J. Eccentric knee flexor strength and risk of hamstring injuries in rugby union. Am. J. Sports Med. 2015, 43, 2663–2670. [Google Scholar] [CrossRef]
- Thorborg, K.; Petersen, J.; Magnusson, S.P.; Hölmich, P. Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand. J. Med. Sci. Sport. 2010, 20, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Charlton, P.C.; Mentiplay, B.F.; Grimaldi, A.; Pua, Y.H.; Clark, R.A. The reliability of a maximal isometric hip strength and simultaneous surface EMG screening protocol in elite, junior rugby league athletes. J. Sci. Med. Sport 2017, 20, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.A.; Bond, E.Q.; Sisto, S.A.; Nadler, S.F. The intra- and interrater reliability of hip muscle strength assessments using a handheld versus a portable dynamometer anchoring station. Arch. Phys. Med. Rehabil. 2004, 85, 598–603. [Google Scholar] [CrossRef]
- Van Melick, N.; Van Cingel, R.E.H.; Brooijmans, F.; Neeter, C.; Van Tienen, T.; Hullegie, W.; Nijhuis-Van Der Sanden, M.W.G. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flagg, K.Y.; Karavatas, S.G.; Thompson Jr, S.; Bennett, C. Current criteria for return to play after anterior cruciate ligament reconstruction: An evidence-based literature review. Ann. Transl. Med. 2019, 7, S252. [Google Scholar] [CrossRef]
- O’Neill, S.; Barry, S.; Watson, P. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: The role of soleus. Phys. Ther. Sport 2019, 37, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Delahunt, E.; Kennelly, C.; McEntee, B.L.; Coughlan, G.F.; Green, B.S. The thigh adductor squeeze test: 45° of hip flexion as the optimal test position for eliciting adductor muscle activity and maximum pressure values. Man. Ther. 2011, 16, 476–480. [Google Scholar] [CrossRef]
Figure 1.
Portable dynamometer MuscleBoard®. (A) = the device from above: measurement scales, tablet with software; (B) = sensor braces with load cells in position for measuring horizontal movement (left or right); (C) = sensor braces with load cells in position for measuring vertical movement (up or down).
Figure 1.
Portable dynamometer MuscleBoard®. (A) = the device from above: measurement scales, tablet with software; (B) = sensor braces with load cells in position for measuring horizontal movement (left or right); (C) = sensor braces with load cells in position for measuring vertical movement (up or down).

Figure 2.
Test positions for measuring peak torque in hip, knee or ankle. (A) = hip flexion, abduction, and adduction; (B) = hip extension; (C) = hip internal and external rotation; (D) = knee extension; (E) = ankle plantarflexion; (F) = Nordic hamstring exercise.
Figure 2.
Test positions for measuring peak torque in hip, knee or ankle. (A) = hip flexion, abduction, and adduction; (B) = hip extension; (C) = hip internal and external rotation; (D) = knee extension; (E) = ankle plantarflexion; (F) = Nordic hamstring exercise.

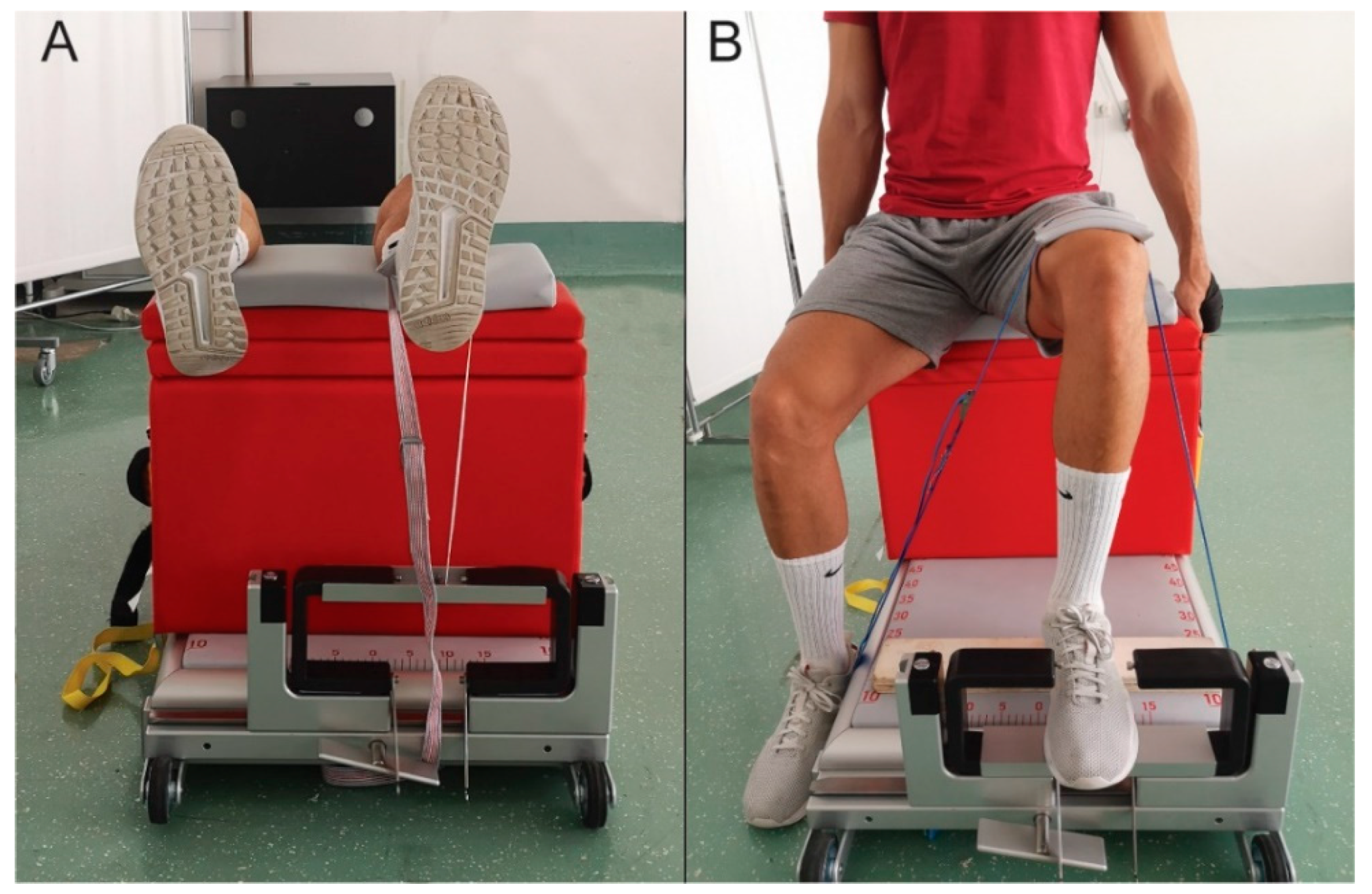
Figure 3.
Knee extension (A) and ankle plantarflexion (B) strength measurements using MuscleBoard®. Knee extension isometric strength was measured using non-elastic strap that connected participant’s lower leg with a rigid rod mounted on both sensor braces on the superior part. Ankle plantarflexion isometric strength was measured using a rigid rod that was mounted on both sensor braces on the inferior part. For both tests, sum of forces from both load cells presented one unilateral measurement.
Figure 3.
Knee extension (A) and ankle plantarflexion (B) strength measurements using MuscleBoard®. Knee extension isometric strength was measured using non-elastic strap that connected participant’s lower leg with a rigid rod mounted on both sensor braces on the superior part. Ankle plantarflexion isometric strength was measured using a rigid rod that was mounted on both sensor braces on the inferior part. For both tests, sum of forces from both load cells presented one unilateral measurement.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Description of the tests.
| Task | Body Position | Sensor & Lower Leg Contact |
|---|---|---|
| HIP FLX HIP ADD HIP ABD | seated position; hip in ~45° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee locked in full extension; ankle in slight dorsiflexion and neutral in other planes; hands placed on the floor behind the device for support; non-elastic strap placed across the pelvis on the anterior side for stabilization | anterior (for FLX), medial (for ADD), or lateral (for ABD) side of the lower leg in contact with superior (for FLX), medial (for ADD), or lateral (for ABD) part of sensor brace; 5 cm proximal to the medial malleoli |
| HIP EXT | prone position; hip in neutral position in all planes (0° flexion/extension; 0° abduction/adduction; 0° external/internal rotation); knee locked in full extension and placed slightly above the surface (to further emphasize hip extension movement and to avoid any knee flexion during contraction); ankle in slight dorsiflexion and neutral in other planes; elbows placed on the padded mat on the floor behind the device for support; non-elastic strap placed across the pelvis on the posterior side for stabilization | posterior side of the lower leg in contact with superior part of sensor brace; 5 cm proximal to the medial malleoli |
| HIP IR HIP ER | 4-point support on the dynamometer (on hands and knees); hip in 90° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee in 90° flexion and neutral in transversal plane (0° internal/external rotation); ankle in slight dorsiflexion and neutral in other planes, no stabilization strap was used | lateral (for IR) or medial (for ER) side of the lower leg in contact with lateral (for IR) or medial (for ER) part of sensor brace; 5 cm proximal to the medial malleoli |
| KNEE EXT | supine position, hip in 90° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee in 90° flexion and neutral in transverse plane (0° internal/external rotation); ankle in slight dorsiflexion and neutral in other planes; posterior side of lower leg was placed on the box, which was fixated on the dynamometer with non-elastic strap (yellow strap, shown in Figure 2D); posterior side of thigh in contact with the box; for stabilization, participant held the straps attached to the box (black strap, shown in Figure 2D) | the measurement was performed using non-elastic strap that connected participant’s lower leg on the anterior side (5 cm proximal to medial malleoli) with a rigid rod mounted on both sensor braces on the superior part (shown in Figure 3A) |
| ANKLE PFLX | seated position, hip in 90° flexion and neutral in other planes (0° abduction/adduction; 0° external/internal rotation); knee in 90° flexion and neutral in transverse plane (0° internal/external rotation); ankle in neutral position in all planes (0° plantar/dorsal flexion, 0° inversion/eversion); non-elastic strap that enabled isometric plantar flexion was placed across the thigh proximal to the knee; for stabilization, the participant held the straps attached to the box (black strap, shown in Figure 2E) | the measurement was performed using a rigid rod that was mounted on both sensor braces on the inferior part; metatarso-phalangeal joints were placed on the middle of the rigid rod (shown in Figure 3B) |
| NHE | kneeling position; lower leg placed on the padded mat distally to the patella (to allow free movement of the patella during the descend); participant slowly descended in 3–5 s (eccentric contraction of knee flexors) while maintaining straight knee-hip-shoulder line | posterior side of the lower leg in contact with superior part of sensor brace; 5 cm proximal to the medial malleoli |
ADD = adduction, ABD = abduction, FLX = flexion, EXT = extension, IR = internal rotation, ER = external rotation, PFLX = plantar flexion, NHE = Nordic hamstring exercise.
Table 2.
Intra-session reliability-peak torque (Nm/kg).
| Task | Parameter | S1 Mean (SD) | S1 95% CI | S2 Mean (SD) | S2 95% CI | %CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | ||||||||
| HIP ADD | R AVG | 0.77 (0.2) | 0.69–0.85 | 0.76 (0.23) | 0.67–0.85 | 6.0 | 0.90 | 0.37 | 0.55 | 0.05 |
| L AVG | 0.77 (0.21) | 0.69–0.85 | 0.75 (0.21) | 0.66–0.84 | 5.4 | 0.92 | 0.25 | 0.62 | 0.10 | |
| B AVG | 2.09 (0.5) | 1.89–2.29 | 2.02 (0.49) | 1.82–2.22 | 3.6 | 0.94 | 0.59 | 0.45 | 0.14 | |
| R MAX | 0.83 (0.2) | 0.75–0.91 | 0.82 (0.25) | 0.72–0.92 | 6.0 | 0.90 | 0.04 | 0.85 | 0.04 | |
| L MAX | 0.84 (0.25) | 0.74–0.94 | 0.8 (0.22) | 0.71–0.89 | 7.0 | 0.90 | 1.59 | 0.22 | 0.17 | |
| B MAX | 2.17 (0.51) | 1.97–2.37 | 2.11 (0.5) | 1.91–2.31 | 3.5 | 0.94 | 0.41 | 0.53 | 0.12 | |
| HIP ABD | R AVG | 0.74 (0.14) | 0.68–0.8 | 0.7 (0.16) | 0.64–0.76 | 7.1 | 0.84 | 2.08 | 0.16 | 0.27 |
| L AVG | 0.69 (0.12) | 0.64–0.74 | 0.68 (0.14) | 0.62–0.74 | 7.8 | 0.77 | 0.12 | 0.73 | 0.08 | |
| B AVG | 2.04 (0.38) | 1.89–2.19 | 1.99 (0.39) | 1.83–2.15 | 7.8 | 0.87 | 0.12 | 0.73 | 0.13 | |
| R MAX | 0.78 (0.15) | 0.72–0.84 | 0.74 (0.18) | 0.67–0.81 | 6.00 | 0.81 | 0.93 | 0.35 | 0.24 | |
| L MAX | 0.74 (0.13) | 0.69–0.79 | 0.73 (0.15) | 0.67–0.79 | 8.5 | 0.76 | 1.47 | 0.24 | 0.07 | |
| B MAX | 2.12 (0.4) | 1.96–2.28 | 2.05 (0.4) | 1.89–2.21 | 8.6 | 0.86 | 0.10 | 0.76 | 0.18 | |
| HIP IR | R AVG | 0.7 (0.15) | 0.64–0.76 | 0.73 (0.17) | 0.66–0.8 | 17.4 | 0.61 | 1.00 | 0.33 | 0.19 |
| L AVG | 0.67 (0.19) | 0.59–0.75 | 0.74 (0.17) | 0.67–0.81 | 9.3 | 0.82 | 8.53 | 0.01 | 0.39 | |
| B AVG | 2.2 (0.53) | 1.99–2.41 | 2.15 (0.49) | 1.95–2.35 | 6.6 | 0.86 | 0.44 | 0.52 | 0.10 | |
| R MAX | 0.75 (0.17) | 0.68–0.82 | 0.78 (0.17) | 0.71–0.85 | 18.7 | 0.54 | 0.84 | 0.37 | 0.18 | |
| L MAX | 0.74 (0.19) | 0.66–0.82 | 0.8 (0.19) | 0.72–0.88 | 9.4 | 0.79 | 3.77 | 0.06 | 0.32 | |
| B MAX | 2.32 (0.51) | 2.12–2.52 | 2.25 (0.5) | 2.05–2.45 | 5.0 | 0.88 | 1.04 | 0.32 | 0.14 | |
| HIP ER | R AVG | 0.76 (0.16) | 0.69–0.83 | 0.73 (0.14) | 0.67–0.79 | 9.9 | 0.67 | 1.01 | 0.33 | 0.20 |
| L AVG | 0.74 (0.18) | 0.67–0.81 | 0.7 (0.13) | 0.65–0.75 | 6.2 | 0.86 | 2.66 | 0.12 | 0.25 | |
| B AVG | 1.81 (0.32) | 1.68–1.94 | 1.74 (0.34) | 1.6–1.88 | 2.1 | 0.95 | 5.31 | 0.03 | 0.21 | |
| R MAX | 0.83 (0.19) | 0.75–0.91 | 0.79 (0.17) | 0.72–0.86 | 11.1 | 0.67 | 1.46 | 0.24 | 0.22 | |
| L MAX | 0.8 (0.21) | 0.72–0.88 | 0.76 (0.14) | 0.7–0.82 | 8.4 | 0.81 | 1.87 | 0.18 | 0.22 | |
| B MAX | 1.88 (0.34) | 1.74–2.02 | 1.82 (0.34) | 1.68–1.96 | 2.2 | 0.94 | 5.50 | 0.03 | 0.18 | |
| HIP EXT | R AVG | 2.71 (0.48) | 2.51–2.91 | 2.65 (0.5) | 2.45–2.85 | 6.4 | 0.69 | 0.03 | 0.88 | 0.12 |
| L AVG | 2.63 (0.55) | 2.4–2.86 | 2.55 (0.49) | 2.35–2.75 | 5.9 | 0.75 | 0.28 | 0.60 | 0.15 | |
| R MAX | 2.87 (0.4) | 2.7–3.04 | 2.83 (0.56) | 2.61–3.05 | 6.4 | 0.71 | 0.06 | 0.82 | 0.08 | |
| L MAX | 2.77 (0.53) | 2.55–2.99 | 2.69 (0.48) | 2.5–2.88 | 3.9 | 0.81 | 0.34 | 0.57 | 0.16 | |
| HIP FLX | R AVG | 1.94 (0.41) | 1.78–2.1 | 2.04 (0.45) | 1.86–2.22 | 7.5 | 0.69 | 2.01 | 0.17 | 0.23 |
| L AVG | 1.89 (0.35) | 1.75–2.03 | 2.04 (0.45) | 1.86–2.22 | 8.2 | 0.60 | 4.43 | 0.05 | 0.37 | |
| R MAX | 2.03 (0.42) | 1.86–2.2 | 2.14 (0.46) | 1.96–2.32 | 7.3 | 0.68 | 2.19 | 0.15 | 0.25 | |
| L MAX | 1.97 (0.36) | 1.83–2.11 | 2.16 (0.46) | 1.98–2.34 | 8.0 | 0.63 | 7.56 | 0.01 | 0.46 | |
| KNEE EXT | R AVG | 6.59 (1.81) | 5.87–7.31 | 6.06 (1.69) | 5.38–6.74 | 10.0 | 0.67 | 3.65 | 0.07 | 0.30 |
| L AVG | 6.24 (1.72) | 5.55–6.93 | 6.25 (1.91) | 5.49–7.01 | 6.4 | 0.83 | 0.00 | 0.97 | 0.01 | |
| R MAX | 6.91 (1.92) | 6.14–7.68 | 6.47 (1.77) | 5.76–7.18 | 9.7 | 0.70 | 2.40 | 0.14 | 0.24 | |
| L MAX | 6.59 (1.79) | 5.87–7.31 | 6.58 (1.97) | 5.79–7.37 | 5.6 | 0.84 | 0.00 | 0.98 | 0.01 | |
| ANKLE PFLX | R AVG | 4.86 (0.6) | 4.61–5.11 | 4.83 (0.62) | 4.57–5.1 | 6.7 | 0.54 | 0.04 | 0.85 | 0.04 |
| L AVG | 4.61 (0.5) | 4.4–4.82 | 4.75 (0.85) | 4.39–5.11 | 6.3 | 0.43 | 0.66 | 0.43 | 0.20 | |
| R MAX | 5.19 (0.59) | 4.94–5.44 | 5.18 (0.75) | 4.86–5.49 | 5.8 | 0.68 | 0.01 | 0.91 | 0.02 | |
| L MAX | 4.85 (0.54) | 4.62–5.08 | 4.94 (0.91) | 4.55–5.32 | 6.4 | 0.44 | 0.24 | 0.63 | 0.12 | |
| NHE | R AVG | 1.97 (0.44) | 1.79–2.15 | 1.98 (0.38) | 1.83–2.13 | 2.5 | 0.91 | 0.17 | 0.68 | 0.02 |
| L AVG | 1.92 (0.42) | 1.75–2.09 | 1.94 (0.39) | 1.78–2.1 | 3.0 | 0.90 | 0.45 | 0.51 | 0.05 | |
| B AVG | 3.88 (0.84) | 3.54–4.22 | 3.92 (0.76) | 3.62–4.22 | 2.6 | 0.91 | 0.34 | 0.56 | 0.05 | |
| R MAX | 2.06 (0.45) | 1.88–2.24 | 2.07 (0.36) | 1.93–2.21 | 3.0 | 0.90 | 0.14 | 0.72 | 0.02 | |
| L MAX | 1.98 (0.43) | 1.81–2.15 | 2.03 (0.36) | 1.89–2.17 | 4.7 | 0.83 | 1.04 | 0.32 | 0.13 | |
| B MAX | 4.03 (0.84) | 3.69–4.37 | 4.09 (0.7) | 3.81–4.37 | 3.6 | 0.87 | 0.71 | 0.41 | 0.08 | |
ADD = adduction, ABD = abduction; IR = internal rotation; ER = external rotation; EXT = extension; FLX = flexion, PFLX = plantar flexion; NHE = Nordic hamstring exercise; AVG = average of 3 repetitions; MAX = highest of 3 repetitions; R = right leg; L = left leg; S1 = session 1; S2 = session 2; CI = confidence interval; TEM = typical error of measurement; CV = coefficient of variance; ICC = interclass coefficient; d = effect size—Cohen’s d.
Table 3.
Intra-session reliability-peak torque hip agonist:antagonist ratio (%).
| Parameter | S1 Mean (SD) | S1 95% CI | S2 Mean (SD) | S2 95% CI | % CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | |||||||
| ADD:ABD UNI R | 105.74 (24.58) | 95.91–115.57 | 110.29 (30) | 98.03–122.55 | 19.3 | 0.55 | 0.17 | 0.68 | 0.17 |
| ADD:ABD UNI L | 112.13 (24.5) | 102.33–121.93 | 114.39 (27.85) | 103.01–125.77 | 12.6 | 0.65 | 0.06 | 0.81 | 0.09 |
| ADD:ABD BI R | 102.03 (17.51) | 93.32–110.4 | 101.83 (15.74) | 94.09–108.94 | 9.4 | 0.71 | 0.00 | 0.95 | 0.01 |
| ADD:ABD BI L | 103.19 (19.66) | 92.89–111.99 | 102.63 (15.86) | 94.77–109.79 | 11.9 | 0.66 | 0.01 | 0.94 | 0.03 |
| IR:ER UNI R | 97.08 (24.47) | 86.85–107.31 | 102.4 (25.74) | 92.1–112.7 | 22.5 | 0.39 | 1.08 | 0.31 | 0.21 |
| IR:ER UNI L | 95.14 (28.38) | 83.79–106.49 | 108.36 (25.86) | 98.01–118.71 | 11.3 | 0.78 | 9.95 | 0.00 | 0.49 |
| IR:ER BI R | 125.85 (32.20) | 109.87–138.97 | 128.15 (27.68) | 114.67–141.09 | 9.9 | 0.76 | 0.18 | 0.68 | 0.08 |
| IR:ER BI L | 122.04 (26.94) | 109.79–133.06 | 123.44 (26.37) | 111.78–135.91 | 8.1 | 0.83 | 0.11 | 0.74 | 0.05 |
| FLX:EXT UNI R | 74.8 (15.67) | 68.25–81.35 | 78.53 (17.71) | 71.44–85.62 | 7.5 | 0.8 | 0.95 | 0.34 | 0.22 |
| FLX:EXT UNI L | 74.89 (14.43) | 68.86–80.92 | 81.1 (16.17) | 74.63–87.57 | 8.1 | 0.75 | 4.68 | 0.04 | 0.40 |
ADD = adduction, ABD = abduction; IR = internal rotation; ER = external rotation; EXT = extension; FLX = flexion; UNI = ratio, calculated from unilateral contractions; BI = ratio, calculated from bilateral contractions; R = right leg; L = left leg; S1 = session 1; S2 = session 2; CI = confidence interval; CV = coefficient of variance; ICC = interclass coefficient; d = effect size—Cohen’s d.
Table 4.
Inter-session reliability–peak torque (Nm/kg).
| Task | Parameter | S1 Mean (SD) | S1 95% CI | S3 Mean (SD) | S3 95% CI | % CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | ||||||||
| HIP ADD | R AVG | 0.77 (0.2) | 0.69–0.85 | 0.77 (0.18) | 0.7–0.84 | 8.8 | 0.8 | 0 | 0.96 | 0.00 |
| L AVG | 0.77 (0.21) | 0.69–0.85 | 0.8 (0.21) | 0.72–0.88 | 14.7 | 0.7 | 0.72 | 0.41 | 0.14 | |
| B AVG | 2.09 (0.5) | 1.89–2.29 | 2.09 (0.47) | 1.9–2.28 | 2.3 | 0.96 | 0.01 | 0.94 | 0.00 | |
| R MAX | 0.83 (0.2) | 0.75–0.91 | 0.85 (0.18) | 0.78–0.92 | 9.1 | 0.78 | 0.29 | 0.59 | 0.11 | |
| L MAX | 0.84 (0.25) | 0.74–0.94 | 0.87 (0.21) | 0.79–0.95 | 14.8 | 0.74 | 0.5 | 0.49 | 0.13 | |
| B MAX | 2.17 (0.51) | 1.97–2.37 | 2.18 (0.46) | 2–2.36 | 1.9 | 0.97 | 0.02 | 0.88 | 0.02 | |
| HIP ABD | R AVG | 0.74 (0.14) | 0.68–0.8 | 0.74 (0.15) | 0.68–0.8 | 13.6 | 0.66 | 0 | 0.97 | 0.00 |
| L AVG | 0.69 (0.12) | 0.64–0.74 | 0.73 (0.15) | 0.67–0.79 | 10.1 | 0.68 | 2.2 | 0.15 | 0.29 | |
| B AVG | 2.04 (0.38) | 1.89–2.19 | 2.03 (0.4) | 1.87–2.19 | 2.7 | 0.94 | 0.06 | 0.81 | 0.03 | |
| R MAX | 0.78 (0.15) | 0.72–0.84 | 0.78 (0.15) | 0.72–0.84 | 13.8 | 0.61 | 0.05 | 0.83 | 0.00 | |
| L MAX | 0.74 (0.13) | 0.69–0.79 | 0.78 (0.16) | 0.72–0.84 | 9.4 | 0.73 | 2.08 | 0.16 | 0.27 | |
| B MAX | 2.12 (0.4) | 1.96–2.28 | 2.1 (0.41) | 1.94–2.26 | 2.7 | 0.94 | 0.27 | 0.61 | 0.05 | |
| HIP IR | R AVG | 0.7 (0.15) | 0.64–0.76 | 0.75 (0.18) | 0.68–0.82 | 8.6 | 0.82 | 1.92 | 0.18 | 0.30 |
| L AVG | 0.67 (0.19) | 0.59–0.75 | 0.74 (0.2) | 0.66–0.82 | 17.2 | 0.66 | 3.64 | 0.07 | 0.36 | |
| B AVG | 2.2 (0.53) | 1.99–2.41 | 2.1 (0.49) | 1.9–2.3 | 6.7 | 0.86 | 2.25 | 0.15 | 0.20 | |
| R MAX | 0.75 (0.17) | 0.68–0.82 | 0.81 (0.19) | 0.73–0.89 | 10.0 | 0.79 | 2.38 | 0.14 | 0.33 | |
| L MAX | 0.74 (0.19) | 0.66–0.82 | 0.81 (0.22) | 0.72–0.9 | 12.8 | 0.71 | 2.81 | 0.11 | 0.34 | |
| B MAX | 2.32 (0.51) | 2.12–2.52 | 2.19 (0.48) | 2–2.38 | 5.5 | 0.87 | 3.88 | 0.06 | 0.26 | |
| HIP ER | R AVG | 0.76 (0.16) | 0.69–0.83 | 0.78 (0.16) | 0.72–0.84 | 12.0 | 0.63 | 0.2 | 0.66 | 0.13 |
| L AVG | 0.74 (0.18) | 0.67–0.81 | 0.83 (0.19) | 0.75–0.91 | 13.0 | 0.68 | 7.56 | 0.01 | 0.49 | |
| B AVG | 1.81 (0.32) | 1.68–1.94 | 1.8 (0.35) | 1.66–1.94 | 2.4 | 0.94 | 0.07 | 0.8 | 0.03 | |
| R MAX | 0.83 (0.19) | 0.75–0.91 | 0.83 (0.18) | 0.76–0.9 | 10.0 | 0.72 | 0.06 | 0.81 | 0.00 | |
| L MAX | 0.8 (0.21) | 0.72–0.88 | 0.91 (0.23) | 0.82–1 | 12.6 | 0.76 | 8.44 | 0.01 | 0.50 | |
| B MAX | 1.88 (0.34) | 1.74–2.02 | 1.87 (0.36) | 1.73–2.01 | 2.2 | 0.95 | 0.27 | 0.61 | 0.03 | |
| HIP EXT | R AVG | 2.71 (0.48) | 2.51–2.91 | 2.63 (0.49) | 2.43–2.83 | 8.5 | 0.78 | 0.12 | 0.73 | 0.16 |
| L AVG | 2.63 (0.55) | 2.4–2.86 | 2.5 (0.52) | 2.29–2.71 | 4.5 | 0.86 | 1.07 | 0.31 | 0.24 | |
| R MAX | 2.87 (0.4) | 2.7–3.04 | 2.81 (0.51) | 2.61–3.01 | 6.7 | 0.77 | 0.05 | 0.83 | 0.13 | |
| L MAX | 2.77 (0.53) | 2.55–2.99 | 2.7 (0.53) | 2.49–2.91 | 5.2 | 0.85 | 0.09 | 0.77 | 0.13 | |
| HIP FLX | R AVG | 1.94 (0.41) | 1.78–2.1 | 2.13 (0.41) | 1.97–2.29 | 7.7 | 0.81 | 10.1 | 0 | 0.46 |
| L AVG | 1.89 (0.35) | 1.75–2.03 | 2.18 (0.41) | 2.02–2.34 | 14.7 | 0.58 | 15.3 | 0 | 0.76 | |
| R MAX | 2.03 (0.42) | 1.86–2.2 | 2.22 (0.43) | 2.05–2.39 | 7.4 | 0.81 | 9.12 | 0.01 | 0.45 | |
| L MAX | 1.97 (0.36) | 1.83–2.11 | 2.25 (0.43) | 2.08–2.42 | 14.6 | 0.58 | 12.3 | 0 | 0.71 | |
| KNEE EXT | R AVG | 6.59 (1.81) | 5.87–7.31 | 6.44 (2.02) | 5.63–7.25 | 6.5 | 0.9 | 0.4 | 0.53 | 0.08 |
| L AVG | 6.24 (1.72) | 5.55–6.93 | 6.25 (2.33) | 5.32–7.18 | 7.8 | 0.9 | 0 | 0.95 | 0.00 | |
| R MAX | 6.91 (1.92) | 6.14–7.68 | 6.86 (2.16) | 6–7.72 | 6.2 | 0.9 | 0.04 | 0.84 | 0.02 | |
| L MAX | 6.59 (1.79) | 5.87–7.31 | 6.55 (2.33) | 5.62–7.48 | 5.4 | 0.92 | 0.03 | 0.86 | 0.02 | |
| ANKLE PFLX | R AVG | 4.86 (0.6) | 4.61–5.11 | 5.24 (0.88) | 4.87–5.62 | 7.2 | 0.57 | 5.51 | 0.03 | 0.51 |
| L AVG | 4.61 (0.5) | 4.4–4.82 | 4.87 (0.76) | 4.55–5.19 | 5.4 | 0.44 | 2.82 | 0.11 | 0.41 | |
| R MAX | 5.19 (0.59) | 4.94–5.44 | 5.51 (0.79) | 5.18–5.84 | 7.2 | 0.68 | 5.84 | 0.02 | 0.46 | |
| L MAX | 4.85 (0.54) | 4.62–5.08 | 5.15 (0.79) | 4.81–5.48 | 5.6 | 0.44 | 3.29 | 0.08 | 0.44 | |
| NHE | R AVG | 1.97 (0.44) | 1.79–2.15 | 2.06 (0.33) | 1.93–2.19 | 5.6 | 0.88 | 3.6 | 0.07 | 0.23 |
| L AVG | 1.92 (0.42) | 1.75–2.09 | 2.03 (0.33) | 1.9–2.16 | 5.5 | 0.88 | 6.14 | 0.02 | 0.29 | |
| B AVG | 3.88 (0.84) | 3.54–4.22 | 4.1 (0.65) | 3.84–4.36 | 5.4 | 0.88 | 5.15 | 0.03 | 0.29 | |
| R MAX | 2.06 (0.45) | 1.88–2.24 | 2.13 (0.33) | 2–2.26 | 6.1 | 0.85 | 1.47 | 0.24 | 0.18 | |
| L MAX | 1.98 (0.43) | 1.81–2.15 | 2.1 (0.33) | 1.97–2.23 | 5.8 | 0.87 | 5.51 | 0.03 | 0.31 | |
| B MAX | 4.03 (0.84) | 3.69–4.37 | 4.22 (0.65) | 3.96–4.48 | 5.9 | 0.86 | 3.34 | 0.08 | 0.25 | |
ADD = adduction, ABD = abduction; IR = internal rotation; ER = external rotation; EXT = extension; FLX = flexion, PFLX = plantar flexion; NHE = Nordic hamstring exercise; AVG = average of 3 repetitions; MAX = highest of 3 repetitions; R = right leg; L = left leg; S1 = session 1; S3 = session 3; CI = confidence interval; TEM = typical error of measurement; CV = coefficient of variance; ICC = interclass coefficient; d = effect size—Cohen’s d.
Table 5.
Inter-session reliability-peak torque hip agonist:antagonist ratio (%).
| Parameter | S1 Mean (SD) | S1 95% CI | S3 Mean (SD) | S3 95% CI | % CV | ICC2.k | Bias | ||
|---|---|---|---|---|---|---|---|---|---|
| F | sig | d | |||||||
| ADD:ABD UNI R | 105.74 (24.58) | 95.91–115.57 | 105.8 (25.25) | 95.7–115.9 | 12.4 | 0.68 | 0 | 0.99 | 0.00 |
| ADD:ABD UNI L | 112.13 (24.5) | 102.33–121.93 | 112.72 (34.35) | 98.98–126.46 | 25.6 | 0.30 | 0.01 | 0.94 | 0.02 |
| ADD:ABD BI R | 102.03 (17.51) | 93.32–110.4 | 102.55 (17.35) | 93.96–110.89 | 3.2 | 0.92 | 0.07 | 0.79 | 0.03 |
| ADD:ABD BI L | 103.19 (19.66) | 92.89–111.99 | 103.72 (13.43) | 97.03–109.81 | 4.4 | 0.89 | 0.06 | 0.81 | 0.03 |
| IR:ER UNI R | 97.08 (24.47) | 86.85–107.31 | 97.62 (26.62) | 86.97–108.27 | 11.9 | 0.78 | 0.06 | 0.81 | 0.02 |
| IR:ER UNI L | 95.14 (28.38) | 83.79–106.49 | 91.94 (26.26) | 81.43–102.45 | 12.0 | 0.73 | 0.38 | 0.54 | 0.12 |
| IR:ER BI R | 125.85 (32.2) | 109.87–138.97 | 121.94 (28.93) | 108.21–135.89 | 16.2 | 0.58 | 0.33 | 0.57 | 0.13 |
| IR:ER BI L | 122.04 (26.94) | 109.79–133.06 | 114.37 (23.85) | 103.02–125.12 | 12.5 | 0.67 | 2.25 | 0.15 | 0.30 |
| FLX:EXT UNI R | 74.8 (15.67) | 68.25–81.35 | 82.38 (16.34) | 75.84–88.92 | 18.1 | 0.55 | 4.02 | 0.06 | 0.47 |
| FLX:EXT UNI L | 74.89 (14.43) | 68.86–80.92 | 88.92 (13.96) | 83.33–94.51 | 12.6 | 0.53 | 19.18 | 0.00 | 0.99 |
ADD = adduction, ABD = abduction; IR = internal rotation; ER = external rotation; EXT = extension; FLX = flexion; UNI = ratio, calculated from unilateral contractions; BI = ratio, calculated from bilateral contractions; R = right leg; L = left leg; S1 = session 1; S3 = session 3; CI = confidence interval; CV = coefficient of variance; ICC = interclass coefficient; d = effect size—Cohen’s d.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marušič, J.; Marković, G.; Šarabon, N. Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength. Appl. Sci. 2021, 11, 3391. https://doi.org/10.3390/app11083391
AMA Style
Marušič J, Marković G, Šarabon N. Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength. Applied Sciences. 2021; 11(8):3391. https://doi.org/10.3390/app11083391
Chicago/Turabian StyleMarušič, Jan, Goran Marković, and Nejc Šarabon. 2021. "Reliability of a New Portable Dynamometer for Assessing Hip and Lower Limb Strength" Applied Sciences 11, no. 8: 3391. https://doi.org/10.3390/app11083391
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.