Exploiting Inter-Organizational Relationships in Health Care: A Bibliometric Analysis and Literature Review



Abstract
:1. Introduction
- R.Q. 1:
- What are the triggers of inter-organizational relationships in health care?
- R.Q. 2:
- What are the attributes of inter-organizational relationships in health care?
- R.Q. 3:
- What are the main implications of inter-organizational relationships in health care?
2. Methods and Materials
2.1. Study Design
2.2. Data Collection
TITLE-ABS-KEY (“Inter-organi* network” OR “Interorgani* network” OR “Inter-organi* relation*” OR “Interorgani* relation*” OR “Inter-organi* Collab*” OR “Interorgani* Collab*” OR “Inter-organi* Coop*” OR “Interorgani* Coop*”) AND TITLE-ABS-KEY (“health care” OR “healthcare”)
2.3. Data Preparation
2.4. Core Analysis
3. Findings
3.1. Overview of Selected Literature
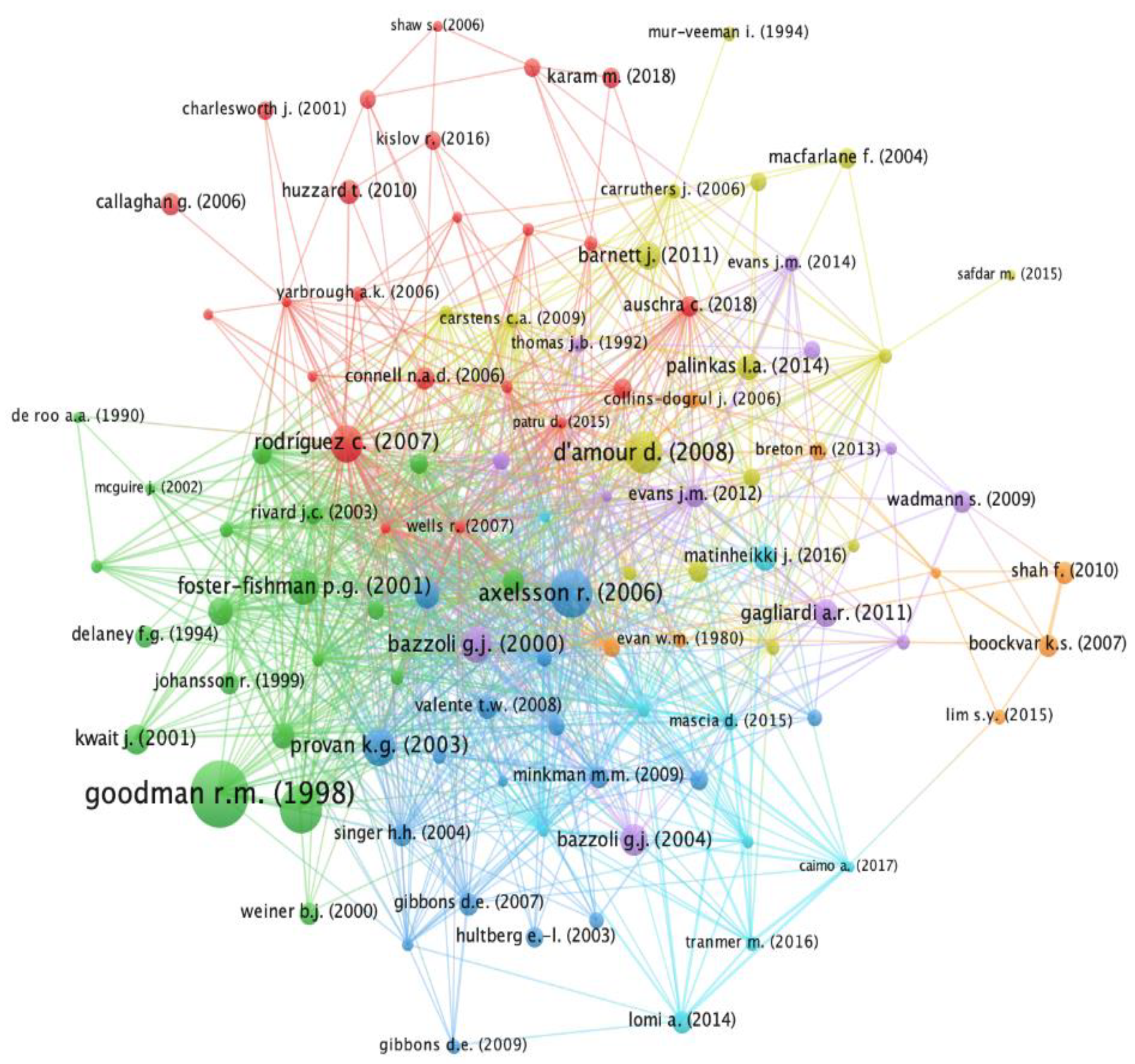
3.2. The “Red” Cluster: The Outer and Inner Triggers of Inter-Organizational Relationships in Health Care
3.3. The “Yellow” Cluster: The Hard and Soft Infrastructures of Inter-Organizational Relationships
3.4. The “Orange” Cluster: The Barriers to Inter-Organizational Relationships
3.5. The “Purple” Cluster: Inter-Organizational Relationships in a Perspective of Integrated Care
3.6. The “Green” Cluster: Organizing an Inter-Organizational Venture
3.7. The “Blue” Cluster: The Implications of Inter-Organizational Relationships
3.8. The “Cyan” Cluster: Looking beyond Cooperation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Agostini, Lara, and Anna Nosella. 2019. Inter-organizational relationships involving SMEs: A bibliographic investigation into the state of the art. Long Range Planning 52: 1–31. [Google Scholar] [CrossRef]
- Ahgren, Bengt, and Runo Axelsson. 2007. Determinants of integrated health care development: Chains of care in Sweden. International Journal of Health Planning and Management 22: 145–57. [Google Scholar] [CrossRef]
- Alexander, Jeffrey A., Arnold D. Kaluzny, and Suann C. Middleton. 1986. Organizational growth, survival and death in the U.S. hospital industry: A population ecology perspective. Social Science & Medicine 22: 303–08. [Google Scholar]
- Auschra, Carolin. 2018. Barriers to the integration of care in inter-organisational settings: A literature review. International Journal of Integrated Care 18: 5–18. [Google Scholar] [CrossRef] [Green Version]
- Axelsson, R., and Susanna Bihari Axelsson. 2006. Integration and collaboration in public health—A conceptual framework. International Journal of Health Planning and Management 21: 75–88. [Google Scholar] [CrossRef]
- Bajwa, Nadia M., Naïke Bochatay, Virginie Muller-Juge, Stéphane Cullati, Katherine S. Blondon, Noëlle Junod Perron, Fabienne Maître, Pierre Chopard, Nu V. Vu, Sara Kim, and et al. 2020. Intra versus interprofessional conflicts: Implications for conflict management training. Journal of Interprofessional Care 34: 259–68. [Google Scholar] [CrossRef]
- Barnett, Julie, Konstantina Vasileiou, Fayika Djemil, Laurence Brooks, and Terry Young. 2011. Understanding innovators’ experiences of barriers and facilitators in implementation and diffusion of healthcare service innovations: A qualitative study. BMC Health Services Research 11: 342–53. [Google Scholar] [CrossRef] [Green Version]
- Bazzoli, Gloria J., Rita Harmata, and Cheeling Chan. 1998. Community-based trauma systems in the United States: An examination of structural development. Social Science & Medicine 46: 1137–49. [Google Scholar]
- Bazzoli, Gloria J., Benjamin Chan, Stephen M. Shortell, and Thomas D’Aunno. 2000. The financial performance of hospitals belonging to health networks and systems. Inquiry 37: 234–52. [Google Scholar]
- Bazzoli, Gloria J., Linda Dynan, Lawton R. Burns, and Clarence Yap. 2004. Two decades of organizational change in health care: What have we learned? Medical Care Research and Review 61: 247–331. [Google Scholar] [CrossRef]
- Boockvar, Kenneth S., and Orah R. Burack. 2007. Organizational relationships between nursing homes and hospitals and quality of care during hospital–nursing home patient transfers. Journal of the American Geriatric Society 55: 1078–84. [Google Scholar] [CrossRef]
- Boyack, Kevin W., and Richard Klavans. 2010. Co-citation analysis, bibliographic coupling, and direct citation: Which citation approach represents the research front most accurately? Journal of the American Society for Information Science and Technology 61: 2389–404. [Google Scholar] [CrossRef]
- Brattström, Anna, and Dries Faems. 2019. Inter-organizational relationships as political battlefields: How fragmentation within organizations shapes relational dynamics between organizations. Academy of Management Journal. Published on-line ahead of print. [Google Scholar] [CrossRef]
- Breton, Mylaine, Raynald Pineault, Jean-Frédéric Levesque, Danièle Roberge, Roxane Borgès Da Silva, and Alexandre Prud’homme. 2013. Reforming healthcare systems on a locally integrated basis: Is there a potential for increasing collaborations in primary healthcare? BMC Health Services Research 13: 262–73. [Google Scholar] [CrossRef] [Green Version]
- Caimo, Alberto, Francesca Pallotti, and Alessandro Lomi. 2017. Bayesian exponential random graph modelling of interhospital patient referral networks. Statistics in Medicine 36: 2902–20. [Google Scholar] [CrossRef]
- Callaghan, Gillian, and Gerald Wistow. 2006. Governance and public involvement in the British national health service: Understanding difficulties and developments. Social Science & Medicine 63: 2289–300. [Google Scholar]
- Carruthers, Janet, Nicholas J. Ashill, and Michel Rod. 2006. Mapping and assessing the key management issues influencing UK public healthcare purchaser-provider cooperation. Qualitative Market Research 9: 86–102. [Google Scholar] [CrossRef]
- Carstens, Carol A., Phyllis C. Panzano, Rick Massatti, Dee Roth, and Helen Anne Sweeney. 2009. A Naturalistic Study of MST Dissemination in 13 Ohio Communities. Journal of Behavioral Health Services and Research 36: 344–60. [Google Scholar] [CrossRef]
- Casey, M. 2008. Partnership—Success factors of interorganizational relationships. Journal of Nursing Management 16: 72–83. [Google Scholar] [CrossRef]
- Chakraborty, Samyadip. 2018. Enablers of co-creation in hospital-supplier relationships: Empirical study in Indian healthcare context. Supply Chain Forum 19: 331–52. [Google Scholar] [CrossRef]
- Charlesworth, Julie. 2001. Negotiating and managing partnership in primary care. Health and Social Care in the Community 9: 279–85. [Google Scholar] [CrossRef] [PubMed]
- Collins-Dogrul, Julie. 2006. Managing US-Mexico "border health": An organizational field approach. Social Science & Medicine 63: 3199–211. [Google Scholar]
- Colvin, Marianna L., Heather M. Thompson, and Morgan E. Cooley. 2020. The ‘cost’ of collaborating and other challenges in inter-organizational child welfare practice: A community-wide perspective. Journal of Public Child Welfare. Published on-line ahead of print. [Google Scholar] [CrossRef]
- Connell, N. A. D., and R. Mannion. 2006. Conceptualisations of trust in the organisational literature: Some indicators from a complementary perspective. Journal of Health Organization and Management 20: 417–33. [Google Scholar] [CrossRef] [PubMed]
- Cote, Jane, and Claire K. Latham. 2006. Trust and commitment: Intangible drivers of interorganizational performance. In Advances in Management Accounting. Edited by Cura di M. J. Epstein and J. Y. Lee. Bingley: Emerald, pp. 293–325. [Google Scholar]
- D’amour, Danielle, Lise Goulet, Jean-François Labadie, Leticia San Martín-Rodriguez, and Raynald Pineault. 2008. A model and typology of collaboration between professionals in healthcare organizations. BMC Health Services Research 8: 188–201. [Google Scholar] [CrossRef] [Green Version]
- Dabić, Marina, Jane Maley, Leo-Paul Dana, Ivan Novak, Massimiliano M. Pellegrini, and Andrea Caputo. 2019. Pathways of SME internationalization: A bibliometric and systematic review. Small Business Economics. Published on-line ahead of print. [Google Scholar] [CrossRef] [Green Version]
- Dainty, Katie N., Damon C. Scales, Tasnim Sinuff, and Merrick Zwarenstein. 2013. Competition in collaborative clothing: A qualitative case study of influences on collaborative quality improvement in the ICU. BMJ Quality and Safety 22: 317–23. [Google Scholar] [CrossRef]
- De Roo, Aad A., and Hans AM Maarse. 1990. Understanding the central-local relationship in health care: A new approach. International Journal of Health Planning and Management 5: 15–25. [Google Scholar] [CrossRef]
- Dearing, James W., Amanda M. Beacom, Stephanie A. Chamberlain, Jingbo Meng, Whitney B. Berta, Janice M. Keefe, Janet E. Squires, Malcolm B. Doupe, Deanne Taylor, Robert Colin Reid, and et al. 2017. Pathways for best practice diffusion: The structure of informal relationships in Canada’s long-term care sector. Implementation Science 12: 11. [Google Scholar] [CrossRef] [Green Version]
- Delaney, Faith G. 1994. Muddling through the middle ground: Theoretical concerns in intersectoral collaboration and health promotion. Health Promotion International 9: 217–25. [Google Scholar] [CrossRef]
- Dickinson, Helen, and Jon Glasby. 2010. ‘Why partnership working doesn’t work’. Pitfalls, problems and possibilities in English health and social care. Public Management Review 12: 811–28. [Google Scholar] [CrossRef]
- Ding, Ying, Ronald Rousseau, and Dietmar Wolfram. 2016. Measuring Scholarly Impact. Cham: Springer. [Google Scholar]
- Dunlop, Judith M., and Michael J. Holosko. 2004. The story behind the story of collaborative networks–relationships do matter! Journal of Health & Social Policy 19: 1–18. [Google Scholar]
- Eden, Colin, and Chris Huxham. 2001. The negotiation of purpose in multi-organizational collaborative groups. Journal of Management Studies 38: 373–91. [Google Scholar] [CrossRef]
- Eiriz, Vasco, Natália Barbosa, and José Figueiredo. 2010. A conceptual framework to analyse hospital competitiveness. Service Industries Journal 30: 437–48. [Google Scholar] [CrossRef]
- Elango, B. 2019. A bibliometric analysis of franchising research (1988–2017). The Journal of Entrepreneurship 28: 223–49. [Google Scholar] [CrossRef]
- Evan, William M., and R. Christopher Klemm. 1980. Interorganizational relations among hospitals: A strategy, structure, and performance model. Human Relations 33: 315–37. [Google Scholar] [CrossRef]
- Evans, Jenna M., G. Ross Baker, Whitney Berta, and Jan Barnsley. 2014. A cognitive perspective on health systems integration: Results of a Canadian Delphi study. BMC Health Services Research 14: 222–34. [Google Scholar] [CrossRef] [Green Version]
- Faust, Victoria, Brian D. Christens, Shannon MA Sparks, and Amy E. Hilgendorf. 2015. Exploring relationships among organizational capacity, collaboration, and network change. Psychological Intervention 24: 125–31. [Google Scholar] [CrossRef] [Green Version]
- Fleury, Marie-Josée. 2006. Integrated service networks: The Quebec case. Health Services Management Research 19: 153–65. [Google Scholar] [CrossRef]
- Fleury, Marie Josée, Céline Mercier, and Jean-Louis Denis. 2002. Regional planning implementation and its impact on integration of a mental health care network. International Journal of Health Planning and Management 17: 315–32. [Google Scholar] [CrossRef]
- Foster-Fishman, Pennie G., Deborah A. Salem, Nicole A. Allen, and Kyle Fahrbach. 2001. Facilitating interorganizational collaboration: The contributions of interorganizational alliances. American Journal of Community Psychology 29: 875–905. [Google Scholar] [CrossRef] [PubMed]
- Franco, Mário, and Heiko Haase. 2015. Inter-organizational cooperation in community health organizations: A competence-based perspective. International Journal of Health Care Quality Assurance 28: 193–210. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, Anna R., Mark J. Dobrow, and Frances C. Wright. 2011. How can we improve cancer care? A review of interprofessional collaboration models and their use in clinical management. Surgical Oncology 20: 146–54. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, Deborah E. 2007. Interorganizational network structures and diffusion of information through a health system. American Journal of Public Health 97: 1684–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibbons, Deborah E., and Subhashish Samaddar. 2009. Designing referral network structures and decision rules to streamline provision of urgent health and human services. Decision Sciences 40: 351–71. [Google Scholar] [CrossRef]
- Gittell, Jody Hoffer, and Leigh Weiss. 2004. Coordination networks within and across organizations: A multi-level framework. Journal of Management Studies 41: 127–53. [Google Scholar] [CrossRef]
- Glänzel, Wolfgang, and Bart Thijs. 2012. Using ‘core documents’ for detecting and labeling new emerging topics. Scientometrics 91: 399–416. [Google Scholar] [CrossRef]
- Goodman, Robert M., Marjorie A. Speers, Kenneth Mcleroy, Stephen Fawcett, Michelle Kegler, Edith Parker, Steven Rathgeb Smith, Terrie D. Sterling, and Nina Wallerstein. 1998. Identifying and Defining the Dimensions of Community Capacity to Provide a Basis for Measurement. Health Education and Behavior 25: 258–78. [Google Scholar] [CrossRef] [Green Version]
- Gramm, Larry D. 1992. Health care markets as interorganizational fields: A conceptual perspective. Health Services Management Research 5: 44–53. [Google Scholar]
- Gray, Barbara. 2004. Strong opposition: Frame-based resistance to collaboration. Journal of Community and Applied Social Psychology 14: 166–76. [Google Scholar] [CrossRef]
- Gray, Barbara. 2009. Intervening to improve inter-organizational partnerships. In The Oxford Handbook of Inter-Organizational Relations. Edited by Cropper Steve, Huxham Chris, Ebers Mark and Peter Smith Ring. Oxford: Oxford University Press. [Google Scholar]
- Hardin, Lauran, Adam Kilian, and Kristin Spykerman. 2017. Competing health care systems and complex patients: An inter-professional collaboration to improve outcomes and reduce health care costs. Journal of Interprofessional Education & Practice 7: 5–10. [Google Scholar]
- Harris, Jenine K., Keith G. Provan, Kimberly J. Johnson, and Scott J. Leischow. 2012. Drawbacks and benefits associated with inter-organizational collaboration along the discovery-development-delivery continuum: A Cancer research network case study. Inplementation Science 7: 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellberg, Ann-Sofie, and Åke Grönlund. 2013. Conflicts in implementing interoperability: Re-operationalizing basic values. Government Information Quarterly 30: 154–62. [Google Scholar] [CrossRef]
- Hervas-Oliver, Jose-Luis, Gregorio Gonzalez, Pedro Caja, and Francisca Sempere-Ripoll. 2015. Clusters and industrial districts: Where is the literature going? Identifying emerging sub-fields of research. European Planning Studies 23: 1827–72. [Google Scholar] [CrossRef]
- Howard, Mickey, Jens K. Roehrich, Michael A. Lewis, and Brian Squire. 2019. Converging and Diverging Governance Mechanisms: The Role of (Dys)Function in Long-term Inter-organizational Relationships. British Journal of Management 30: 624–44. [Google Scholar] [CrossRef]
- Hultberg, Eva-Lisa, Knut Lönnroth, and Peter Allebeck. 2003. Co-financing as a means to improve collaboration between primary health care, social insurance and social service in Sweden. A qualitative study of collaboration experiences among rehabilitation partners. Health Policy 64: 142–52. [Google Scholar] [CrossRef]
- Huo, Baofeng, Min Tian, Yu Tian, and Qiyuan Zhang. 2019. The dilemma of inter-organizational relationships: Dependence, use of power and their impacts on opportunism. International Journal of Operations & Production Management 39: 2–23. [Google Scholar]
- Huxham, Chris, and Siv Vangen. 2013. Managing to Collaborate: The Theory and Practice of Collaborative Advantage. London: Taylor and Francis. [Google Scholar]
- Huzzard, Tony, Beth Maina Ahlberg, and Marianne Ekman. 2010. Constructing interorganizational collaboration: The action researcher as boundary subject. Action Research 8: 293–314. [Google Scholar] [CrossRef]
- Johansson, Roine, and Klas Borell. 1999. Central steering and local networks: Old-age care in Sweden. Public Administration 77: 585–98. [Google Scholar] [CrossRef]
- Karam, Marlène, Isabelle Brault, Thérèse Van Durme, and Jean Macq. 2018. Comparing interprofessional and interorganizational collaboration in healthcare: A systematic review of the qualitative research. International Journal of Nursing Studies 79: 70–83. [Google Scholar] [CrossRef]
- Karlsson, Margareta, Rickard Garvare, Karin Zingmark, and Birgitta Nordström. 2020. Organizing for sustainable inter-organizational collaboration in health care processes. Journal of Interprofessional Care 34: 241–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, Maxwell Mirton. 1963. Bibliographic coupling between scientific papers. Journal of the Association for Information Science and Technology 14: 10–25. [Google Scholar] [CrossRef]
- King, Nelson. 2013. Exploring the impact of operating model choice on the governance of inter-organizational workflow: The U.S. e-prescribing network. European Journal of Information Systems 22: 548–68. [Google Scholar] [CrossRef]
- Kislov, Roman, Damian Hodgson, and Ruth Boaden. 2016. Professionals as Knowledge Brokers: The Limits of Authority in Healthcare Collaboration. Public Administration 94: 472–89. [Google Scholar] [CrossRef]
- Kousgaard, Marius Brostrøm, Anne Sofie Kjær Joensen, and Thorkil Thorsen. 2015. The challenges of boundary spanners in supporting inter-organizational collaboration in primary care—A qualitative study of general practitioners in a new role. BMC Family Practice 16: 17–25. [Google Scholar] [CrossRef] [Green Version]
- Kwait, Jennafer, Thomas W. Valente, and David D. Celentano. 2001. Interorganizational relationships among HIV/AIDS service organizations in Baltimore: A network analysis. Journal of Urban Health 78: 468–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laing, Angus, and Seonaidh Cotton. 1997. Patterns of inter-organizational purchasing: Evolution of consortia-based purchasing amongst GP fundholders. European Journal of Purchasing & Supply Management 3: 83–91. [Google Scholar]
- Leurs, Mariken T. W., Ingrid M. Mur-Veeman, Rosalie van der Sar, Herman P. Schaalma, and Nanne K. de Vries. 2008. Diagnosis of sustainable collaboration in health promotion—A case study. BMC Public Health 8: 382–97. [Google Scholar] [CrossRef]
- Lewis, Jenny M. 2009. The why and how of partnerships: Policy and governance foundations. Australian Journal of Primary Health 15: 225–31. [Google Scholar] [CrossRef]
- Li, Weizi, Aaquib Islam, Kevin Johnson, Priam Lauchande, Xiaopu Shang, and Shen Xu. 2018. Understanding inter-organizational trust among integrated care service provider networks: A perspective on organizational asymmetries. Health Policy 122: 1356–63. [Google Scholar] [CrossRef]
- Lim, Shi Ying, Sirkka L. Jarvenpaa, and Holly J. Lanham. 2015. Barriers to Interorganizational Knowledge Transfer in Post-Hospital Care Transitions: Review and Directions for Information Systems Research. Journal of Management Information Systems 32: 48–74. [Google Scholar] [CrossRef]
- Löfström, Mikael. 2010. Inter-organizational collaboration projects in the public sector: A balance between integration and demarcation. International Journal of Health Planning and Management 25: 136–55. [Google Scholar] [CrossRef] [PubMed]
- Lomi, Alessandro, Daniele Mascia, Duy Quang Vu, Francesca Pallotti, Guido Conaldi, and Theodore J. Iwashyna. 2014. Quality of care and interhospital collaboration: A study of patient transfers in Italy. Medical Care 52: 407–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Fernández, Ma Concepción, Ana Ma Serrano-Bedia, and Marta Pérez-Pérez. 2016. Entrepreneurship and family firm research: A bibliometric analysis of an emerging field. Journal of Small Business Management 54: 622–39. [Google Scholar] [CrossRef]
- Macfarlane, F., T. Greenhalgh, T. Schofield, and T. Desombre. 2004. RCGP quality team development programme: An illuminative evaluation. Quality and Safety in Health Care 13: 356–62. [Google Scholar] [CrossRef] [Green Version]
- Manesh, Mohammad Fakhar, Massimiliano Matteo Pellegrini, Giacomo Marzi, and Marina Dabic. 2020. Knowledge Management in the Fourth Industrial Revolution: Mapping the Literature and Scoping Future Avenues. IEEE Transactions on Engineering Management. Published on-line ahead of print. [Google Scholar] [CrossRef]
- Marín-Idárragaa, Diego Armando, and Luz Ángela Losada da Campos. 2015. Organizational structure and inter-organizational relations: Analysis in health care public institutions in Colombia. Estudios Gerenciales 31: 88–99. [Google Scholar]
- Mascia, Daniele, and Vincenzo Di Fausto. 2013. Dynamics of hospital competition: Social network analysis in the italian national health service. Health Care Management Review 38: 234–47. [Google Scholar] [CrossRef]
- Mascia, Daniele, Federica Angeli, and Fausto Di Vincenzo. 2015. Effect of hospital referral networks on patient readmissions. Social Science & Medicine 132: 113–21. [Google Scholar]
- Matinheikki, Juri, Karlos Artto, Antti Peltokorpi, and Risto Rajala. 2016. Managing inter-organizational networks for value creation in the front-end of projects. International Journal of Project Management 34: 1226–41. [Google Scholar] [CrossRef] [Green Version]
- Maurya, Dayashankar, and Amit Kumar Srivastava. 2019. Managing partner opportunism in public–private partnerships: The dynamics of governance adaptation. Public Management Review 21: 1420–42. [Google Scholar] [CrossRef]
- McCloskey, Rose, Michael Campo, Robert Savage, and SueAnn Mandville-Anstey. 2009. A Conceptual Framework for Understanding Interorganizational Relationships Between Nursing Homes and Emergency Departments: Examples From the Canadian Setting. Policy Politics & Nursing Practice 10: 285–94. [Google Scholar]
- McDonald, Julie, Gawaine Powell Davies, and Mark Fort Harris. 2009. Interorganisational and interprofessional partnership approaches to achieve more coordinated and integrated primary and community health services: The Australian experience. Australian Journal of Primary Health 15: 262–69. [Google Scholar] [CrossRef]
- McGuire, James, Robert Rosenheck, and Craig Burnette. 2002. Expanding service delivery: Does it improve relationships among agencies serving homeless people with mental illness? Administration and Policy in Mental Health 29: 243–56. [Google Scholar] [CrossRef] [PubMed]
- Meijboom, Bert, Jobde Haan, and Piet Verheyen. 2004. Networks for integrated care provision: An economic approach based on opportunism and trust. Health Policy 69: 33–43. [Google Scholar] [CrossRef] [PubMed]
- Mervyn, Kieran, Nii Amoo, and Rebecca Malby. 2019. Challenges and insights in inter-organizational collaborative healthcare networks: An empirical case study of a place-based network. International Journal of Organizational Analysis 27: 875–902. [Google Scholar] [CrossRef]
- Minkman, Mirella M. N., Kees T. B. Ahaus, and Robbert Huijsman. 2009. A four phase development model for integrated care services in the Netherlands. BMC Health Services Research 9: 42–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, Shannon M., and Stephen M. Shortell. 2000. The Governance and Management of Effective Community Health Partnerships: A Typology for Research, Policy, and Practice. Milbank Quarterly 78: 241–89. [Google Scholar] [CrossRef] [Green Version]
- Mohr, Bernard J., and Ezra Dessers. 2019. Designing Integrated Care Ecosystems: A Socio-Technical Perspective. Cham: Springer. [Google Scholar]
- Morrissey, Joseph P., Matthew C. Johnsen, and Michael O. Calloway. 1997. Evaluating performance and change in mental health systems serving children and youth: An interorganizational network approach. Journal of Behavioral Health Services and Research 24: 4–22. [Google Scholar]
- Morrissey, Joseph P., Michael O. Calloway, Neil Thakur, Joseph Cocozza, Henry J. Steadman, Deborah Dennis, and The ACCESS National Evaluation Team. 2002. Integration of service systems for homeless persons with serious mental illness through the ACCESS program. Psychiatric Services 53: 949–57. [Google Scholar] [CrossRef]
- Mur-Veeman, Ingrid, and Arno Van Raak. 1994. Inter-organizational networks on the dutch home health care market. International Journal of Planning and Management 9: 245–58. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, Nuno, and Fabrice Lumineau. 2019. The Dark Side of Interorganizational Relationships: An Integrative Review and Research Agenda. Journal of Management 45: 231–61. [Google Scholar] [CrossRef] [Green Version]
- Oliver, Amalya L., and Mark Ebers. 1998. Networking network studies: An analysis of conceptual configurations in the study of inter-organizational relationships. Organization Studies 19: 549–83. [Google Scholar] [CrossRef]
- Otte-Trojel, Terese, Antoinette de Bont, Marcello Aspria, Samantha Adams, Thomas G. Rundall, Joris van de Klundert, and Marleen de Mul. 2015. Developing patient portals in a fragmented healthcare system. International Journal of Medical Informatics 84: 835–46. [Google Scholar] [CrossRef] [PubMed]
- Otte-Trojel, Terese, Thomas G. Rundall, Antoinette de Bont, and Joris van de Klundert. 2017. Can relational coordination help inter-organizational networks overcome challenges to coordination in patient portals? International Journal of Healthcare Management 10: 75–83. [Google Scholar] [CrossRef]
- Palinkas, Lawrence A., Dahlia Fuentes, Megan Finno, Antonio R. Garcia, Ian W. Holloway, and Patricia Chamberlain. 2014. Inter-organizational collaboration in the implementation of evidence-based practices among public agencies serving abused and neglected youth. Administration and Policy in Mental Health and Mental Health Services Research 41: 74–85. [Google Scholar] [CrossRef]
- Palumbo, Rocco. 2015. Reforming penitentiary health. The transition from ‘cure’ to ‘care’ in Italian prisons. International Journal of Healthcare Management 8: 232–43. [Google Scholar] [CrossRef]
- Palumbo, Rocco. 2016a. Designing health-literate health care organization: A literature review. Health Services Management Research 29: 79–87. [Google Scholar] [CrossRef]
- Palumbo, Rocco. 2016b. Contextualizing co-production of health care: A systematic literature review. International Journal of Public Sector Management 29: 72–90. [Google Scholar] [CrossRef]
- Palumbo, Rocco, and Rosalba Manna. 2018. What if things go wrong in co-producing health services? Exploring the implementation problems of health care co-production. Policy and Society 37: 368–85. [Google Scholar] [CrossRef] [Green Version]
- Palumbo, Rocco, Silvia Cosimato, and Aurelio Tommasetti. 2017. Dream or reality? A recipe for sustainable and innovative health care ecosystems. TQM Journal 29: 847–62. [Google Scholar] [CrossRef]
- Paluzzi, Joan E. 2012. “Dualities of Interest”: The Inter-Organizational Relationships between Disease-Specific Nonprofits and the Pharmaceutical Industry. International Journal of Health Services 42: 323–39. [Google Scholar] [CrossRef] [PubMed]
- Patru, Daniela, Kristina Lauche, Hans van Kranenburg, and Gerrit Willem Ziggers. 2015. Multilateral boundary spanners: Creating virtuous cycles in the development of health care networks. Medical Care and Review 72: 665–86. [Google Scholar] [CrossRef]
- Pellegrini, Massimiliano Matteo, Francesco Ciampi, Giacomo Marzi, and Beatrice Orlando. 2020. The relationship between knowledge management and leadership: Mapping the field and providing future research avenues. Journal of Knowledge Management. Published on-line ahead of print. [Google Scholar] [CrossRef]
- Petrakou, Alexandra. 2009. Integrated care in the daily work: Coordination beyond organisational boundaries. International Journal of Integrated Care 9: e87. [Google Scholar] [CrossRef] [PubMed]
- Provan, Keith G., Juliann G. Sebastian, and H. Brinton Milward. 1996. Interorganizational cooperation in community mental health: A resource-based explanation of referrals and case coordination. Medical Care Research and Review 53: 94–119. [Google Scholar] [CrossRef] [PubMed]
- Provan, Keith G., Leigh Nakama, Mark A. Veazie, Nicolette I. Teufel-Shone, and Carol Huddleston. 2003. Building Community Capacity Around Chronic Disease Services through a Collaborative Interorganizational Network. Health Education & Behavior 30: 646–62. [Google Scholar]
- Retrum, Jessica H., Carrie L. Chapman, and Danielle M. Varda. 2013. Implications of Network Structure on Public Health Collaboratives. Health Education & Behavior 40: 13–23. [Google Scholar]
- Rivard, Jeanne C., and Joseph P. Morrissey. 2003. Factors associated with interagency coordination in a child mental health service system demonstration. Administration and Policy in Mental Health 30: 397–415. [Google Scholar] [CrossRef]
- Rodriguez, Charo, Ann Langley, François Béland, and Jean-Louis Denis. 2007. Governance, power, and mandated collaboration in an interorganizational network. Administration & Society 39: 150–93. [Google Scholar]
- Safdar, Morooj, Greg Richards, and Bijan Raahemi. 2015. A model of effective IT governance for collaborative networked organizations. Paper presented at the Colmar: 12th International Conference on e-Business (ICETE), Alsace, France, July 20–22; Volume 2, pp. 191–202. [Google Scholar]
- Saltman, Richard, Reinhard Busse, and Josep Figueras. 2007. Decentralization In Health Care: Strategies and Outcomes. New York: McGraw Hill. [Google Scholar]
- Schermerhorn, John R., Jr., and Larry E. Shirland. 1981. Hospital administrator felt needs for interorganizational cooperation and actual cooperative outcomes by their hospitals. Decision Sciences 12: 486–501. [Google Scholar] [CrossRef]
- Schmidt, M., T. Plochg, J. Harting, N. S. Klazinga, and K. Stronks. 2009. Micro grants as a stimulus for community action in residential health programmes: A case study. Health Promotion International 24: 234–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schooley, Benjamin, Thomas Horan, and Michael Marich. 2010. Managing IT Collaboration in Multi-Organizational Time-Critical Services. MIS Quarterly Executive 9: 4. [Google Scholar]
- Schumaker, Alice M. 2002. Interorganizational networks: Using a theoretical model to predict effectiveness of rural health care delivery networks. Journal of Health and Human Services Administration 25: 371–406. [Google Scholar] [PubMed]
- Secundo, Giustina, Antonio Toma, Giovanni Schiuma, and Giuseppina Passiante. 2019. Knowledge transfer in open innovation: A classification framework for healthcare ecosystems. Business Process Management Journal 25: 144–63. [Google Scholar] [CrossRef]
- Shah, Faraaz, Orah Burack, and Kenneth S. Boockvar. 2010. Perceived barriers to communication between hospital and nursing home at time of patient transfer. Journal of the American Medical Directors Association 11: 239–45. [Google Scholar] [CrossRef]
- Shaw, Sara, John Ashcroft, and Roland Petchey. 2006. Barriers and opportunities for developing sustainable relationships for health improvement: The case of public health and primary care in the UK. Critical Public Health 16: 73–88. [Google Scholar] [CrossRef]
- Singer, Helen Harber, and Michelle Crozier Kegler. 2004. Assessing interorganizational networks as a dimension of community capacity: Illustrations from a community intervention to prevent lead poisoning. Health Education & Behavior 31: 808–21. [Google Scholar]
- Small, Henry. 2009. Critical thresholds for co-citation clusters and emergence of the giant component. Journal of Informetrics 2: 332–40. [Google Scholar] [CrossRef]
- Stevens, Merieke, John Paul MacDuffie, and Susan Helper. 2015. Reorienting and Recalibrating Inter-organizational Relationships: Strategies for Achieving Optimal Trust. Organization Studies 36: 1237–64. [Google Scholar] [CrossRef] [Green Version]
- Taylor, Maureen, and Marya L. Doerfel. 2005. Another dimension to explicating relationships: Measuring inter-organizational linkages. Public Relations Review 31: 121–29. [Google Scholar] [CrossRef]
- Thomas, James B., David J. Ketchen Jr., Linda Klebe Trevino, and Reuben R. McDaniel Jr. 1992. Developing interorganizational relationships in the health sector: A multicase study. Health Care Management Review 17: 7–20. [Google Scholar] [CrossRef] [PubMed]
- Touati, Nassera, Danièle Roberge, and Jean-Louis Denis. 2006. Clinical leaders at the forefront of change in health-care systems: Advantages and issues. Lessons learned from the evaluation of the implementation of an integrated oncological services network. Health Services Management Research 19: 105–22. [Google Scholar] [CrossRef] [PubMed]
- Tranfield, David, David Denyer, and Palminder Smart. 2003. Towards a methodology for developing evidence—Informed management knowledge by means of systematic review. British Journal of Management 14: 207–22. [Google Scholar] [CrossRef]
- Tranmer, Mark, Francesca Pallotti, and Alessandro Lomi. 2016. The embeddedness of organizational performance: Multiple membership multiple classification models for the analysis of multilevel networks. Social Networks 44: 269–80. [Google Scholar] [CrossRef] [Green Version]
- Valente, Thomas W., Kathryn A. Coronges, Gregory D. Stevens, and Michael R. Cousineau. 2008. Collaboration and competition in a children’s health initiative coalition: A network analysis. Evolution and Programme Planning 31: 392–402. [Google Scholar] [CrossRef]
- Valentijn, Pim P., Inge C. Boesveld, Denise M. van der Klauw, Dirk Ruwaard, Jeroen N. Struijs, Johanna J. W. Molema, Marc A. Bruijnzeels, and Hubertus J. M. Vrijhoef. 2015. Towards a taxonomy for integrated care: A mixed-methods study. International Journal of Integrated Care 15: e003. [Google Scholar] [CrossRef] [Green Version]
- Van Eck, Nees Jan, and Ludo Waltman. 2007. VOS: A new method for visualizing similarities between objects. In Advances in Data Analysis. Edited by di R. Decker and H. J. Lenz. Berlin: Springer, pp. 299–306. [Google Scholar]
- Van Eck, Nees Jan, and Ludo Waltman. 2010. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 84: 523–38. [Google Scholar] [CrossRef] [Green Version]
- van Meerkerk, Ingmar, and Jurian Edelenbos. 2018. Boundary Spanners in Public Management and Governance: An Interdisciplinary Perspective. Northampton: Edward Elgar. [Google Scholar]
- van Rensburg, André Janse, and Pieter Fourie. 2016. Health policy and integrated mental health care in the SADC region: Strategic clarification using the Rainbow Model. International Journal of Integrated Mental Health Systems 10: 49–61. [Google Scholar] [CrossRef] [Green Version]
- Vangen, Siv. 2017. Culturally diverse collaborations: A focus on communication and shared understanding. Public Management Review 19: 305–25. [Google Scholar] [CrossRef]
- Vangen, Siv, and Chris Huxham. 2012. The tangled web: Unraveling the principle of common goals in collaborations. Journal of Public Administration Research and Theory 22: 731–60. [Google Scholar] [CrossRef]
- Wadmann, Sarah, Martin Strandberg-Larsen, and Karsten Vrangbæk. 2009. Coordination between primary and secondary healthcare in Denmark and Sweden. International Journal of Integrated Care 9: e04. [Google Scholar] [CrossRef] [PubMed]
- Walker, Rae. 1992. Inter-organizational linkages as mediating structures community health. Health Promotion International 7: 257–64. [Google Scholar] [CrossRef]
- Weech-Maldonado, Robert, Keith J. Benson, and Larry D. Gamm. 2003. Evaluating the effectiveness of community health partnerships: A stakeholder accountability approach. Journal of Health and Human Services Administration 26: 58–92. [Google Scholar]
- Weiner, Bryan J., Jeffrey A. Alexander, and Howard S. Zuckerman. 2000. Strategies for effective management participation in community health partnerships. Health Care Management Review 25: 48–66. [Google Scholar] [CrossRef]
- Wells, Rebecca, and Bryan J. Weiner. 2007. Adapting a Dynamic Model of Interorganizational Cooperation to the Health Care Sector. Medical Care Research and Review 64: 518–43. [Google Scholar] [CrossRef]
- Wells, Rebecca, Christy Harris Lemak, and Thomas A. D’aunno. 2005. Factors associated with interorganizational relationships among outpatient drug treatment organizations 1990–2000. Health Services Research 40: 1356–78. [Google Scholar] [CrossRef] [Green Version]
- Welsh, Wayne N., Hannah K. Knudsen, Kevin Knight, Lori Ducharme, Jennifer Pankow, Terry Urbine, Adrienne Lindsey, Sami Abdel-Salam, Jennifer Wood, Laura Monico, and et al. 2016. Effects of an organizational linkage intervention on inter-organizational service coordination between probation/parole agencies and community treatment providers. Administration and Policy in Mental Health and Mental Health Services Research 43: 105–21. [Google Scholar] [CrossRef] [Green Version]
- Wendel, Monica L., John D. Prochaska, Heather R. Clark, Shawta Sackett, and Keith Perkins. 2010. Interorganizational network changes among health organizations in the Brazos Valley, Texas. Journal of Primary Prevention 31: 59–68. [Google Scholar] [CrossRef]
- Westra, Daan, Federica Angeli, Martin Carree, and Dirk Ruwaard. 2017a. Coopetition in health care: A multi-level analysis of its individual and organizational determinants. Social Science & Medicine 186: 43–51. [Google Scholar]
- Westra, Daan, Federica Angeli, Martin Carree, and Dirk Ruwaard. 2017b. Understanding competition between healthcare providers: Introducing an intermediary inter-organizational perspective. Health Policy 121: 149–57. [Google Scholar] [CrossRef] [PubMed]
- Willis, Cameron D., Barbara L. Riley, Carol P. Herbert, and Allan Best. 2013. Networks to strengthen health systems for chronic disease prevention. American Journal of Public Health 103: 39–48. [Google Scholar] [CrossRef] [PubMed]
- Willumsen, Elisabeth. 2008. Interprofessional collaboration—A matter of differentiation and integration? Theoretical reflections based in the context of Norwegian childcare. Journal of Interprofessional Care 22: 352–63. [Google Scholar] [CrossRef] [PubMed]
- Wistow, Gerald, Helen Dickinson, Jenna M. Evans, and G. Ross Baker. 2012. Shared mental models of integrated care: Aligning multiple stakeholder perspectives. Journal of Health Organization and Management 26: 713–36. [Google Scholar]
- Yarbrough, Amy K., and Thomas L. Powers. 2006a. A resource-based view of partnership strategies in health care organizations. Journal of Hospital Marketing & Public Relations 17: 45–65. [Google Scholar]
- Yarbrough, Amy K., and Thomas L. Powers. 2006b. The evolution of ruralhospitals viewed through a population ecology framework. Health Marketing Quarterly 23: 33–48. [Google Scholar] [CrossRef]
- Yu, Sui-Hua, and Ming-Yu Chen. 2013. Performance impacts of interorganizational cooperation: A transaction cost perspective. The Service Industry Journal 33: 1223–41. [Google Scholar] [CrossRef]
- Zakus, J. David L. 1998. Resource dependency and community participation in primary health care. Social Science & Medicine 46: 475–94. [Google Scholar]
- Zou, Guanyang, Xiaolin Wei, John D Walley, Jia Yin, and Qiang Sun. 2012. Factors influencing integration of TB services in general hospitals in two regions of China: A qualitative study. BMC Health Services Research 12: 21–31. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Research Question | Cluster | Key Contents |
|---|---|---|
| R.Q. 1: What are the triggers of inter-organizational relationships in health care? | “Red” cluster | Two triggers to inter-organizational relationships can be retrieved. Firstly, they are engendered by the complexity of the external environment and they are solicited by the need of health care organizations to thrive in a continuously evolving institutional, epidemiological, and competitive context. Secondly, they are encouraged by internal triggers. Since partners may be interested to opportunistically participate in networking, trust and commitment to collaboration are key internal determinants of inter-organizational relationships in the health care domain. |
| “Yellow” cluster | Partners have to align external pressures, features of organizational collaborations, and internal attributes to build successful collaborations. Governance models based on centrality and connectivity, formalization of exchanges, trust internalization, and shared goals and values are essential for the effectiveness of inter-organizational collaborations. | |
| “Orange” cluster | Goal conflicts, organizational and operational inconsistencies, and communication barriers amongst partners prevent effective collaboration Such conflicts are triggered by the specificity of partners’ policies, structures, cultures, and practices. | |
| R.Q. 2: What are the attributes of inter-organizational relationships in health care? | “Purple” cluster: | Strategic and operational coordination, holistic and inter-professional networking, integrated financial management systems, and networked IT systems boost the implications of inter-organizational relationships in terms of integrated care. |
| “Green” cluster: | Coordination is facilitated when interorganizational relationships fulfill both the internal agency needs for goal attainment and the external needs for exerting greater control over the larger policy and program environment. A mixture of integration and decentralization determines better results as compared with a fully-fledged centralization of inter-organizational practices. | |
| R.Q. 3: What are the main implications of inter-organizational relationships in health care? | “Blue” cluster | Effective inter-organizational relationships require sound micro, meso, and macro-level interventions. The establishment of larger coalitions (networks of networks) and the participation of the community are essential to sustain the institutional legitimacy of inter-organizational relationships. |
| “Cyan” cluster | Selfish interests may prevent the effectiveness of inter-organizational relationships. They are more likely to arise when leading actors are unable to affirm their centrality, when inter-organizational ties are weak, and when the partners do not perceive an adequate level of trust. This leads to coopetitive behaviors rather than to cooperative practices. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palumbo, R.; Manesh, M.F.; Pellegrini, M.M.; Flamini, G. Exploiting Inter-Organizational Relationships in Health Care: A Bibliometric Analysis and Literature Review. Adm. Sci. 2020, 10, 57. https://doi.org/10.3390/admsci10030057
Palumbo R, Manesh MF, Pellegrini MM, Flamini G. Exploiting Inter-Organizational Relationships in Health Care: A Bibliometric Analysis and Literature Review. Administrative Sciences. 2020; 10(3):57. https://doi.org/10.3390/admsci10030057
Chicago/Turabian StylePalumbo, Rocco, Mohammad Fakhar Manesh, Massimiliano M. Pellegrini, and Giulia Flamini. 2020. "Exploiting Inter-Organizational Relationships in Health Care: A Bibliometric Analysis and Literature Review" Administrative Sciences 10, no. 3: 57. https://doi.org/10.3390/admsci10030057