
Goal-Directed Resilience in Training (GRIT): A Biopsychosocial Model of Self-Regulation, Executive Functions, and Personal Growth (Eudaimonia) in Evocative Contexts of PTSD, Obesity, and Chronic Pain

Abstract
:The experiences of camp life show that man does have a choice of action…become a plaything of circumstances…or striv(e) and struggl(e) for a worthwhile goal…Viktor E. Frankl
1. Introduction
1.1. Approach/Engagement versus Withdrawal/Defense
1.1.1. Motivational Models: Approach-Avoidance
1.1.2. Emotional Models: Approach-Avoidance
1.1.3. Action Models: Intention-Based versus Stimulus-Based Responding
1.1.4. Attention Models: Goal-Directed versus Stimulus-Driven
1.1.5. Brain Functions: Predictive and Reactive Biobehavioral Programs
1.1.6. Clinically Relevant Concepts
1.1.6.1. Well-Being: Eudaimonia versus Hedonia
1.1.6.2. Goal-Relevant Motivational Constructs and PTSD
1.1.7. Beyond Dualities
1.1.8. Summary: Engagement and Withdrawal
1.2. Goal-Directed and Stimulus-Based Responding in Clinical Practice
1.2.1. Not all Extreme Experiences Result in Trauma
1.2.2. New Wave Therapies
1.3. Resilience
1.3.1. Resilience Training as Primary Prevention
1.3.1.1. Resilience Prevention Programs with Children
1.3.1.2. Resilience Prevention in the Armed Forces
1.3.2. Resilience Training as Secondary Intervention
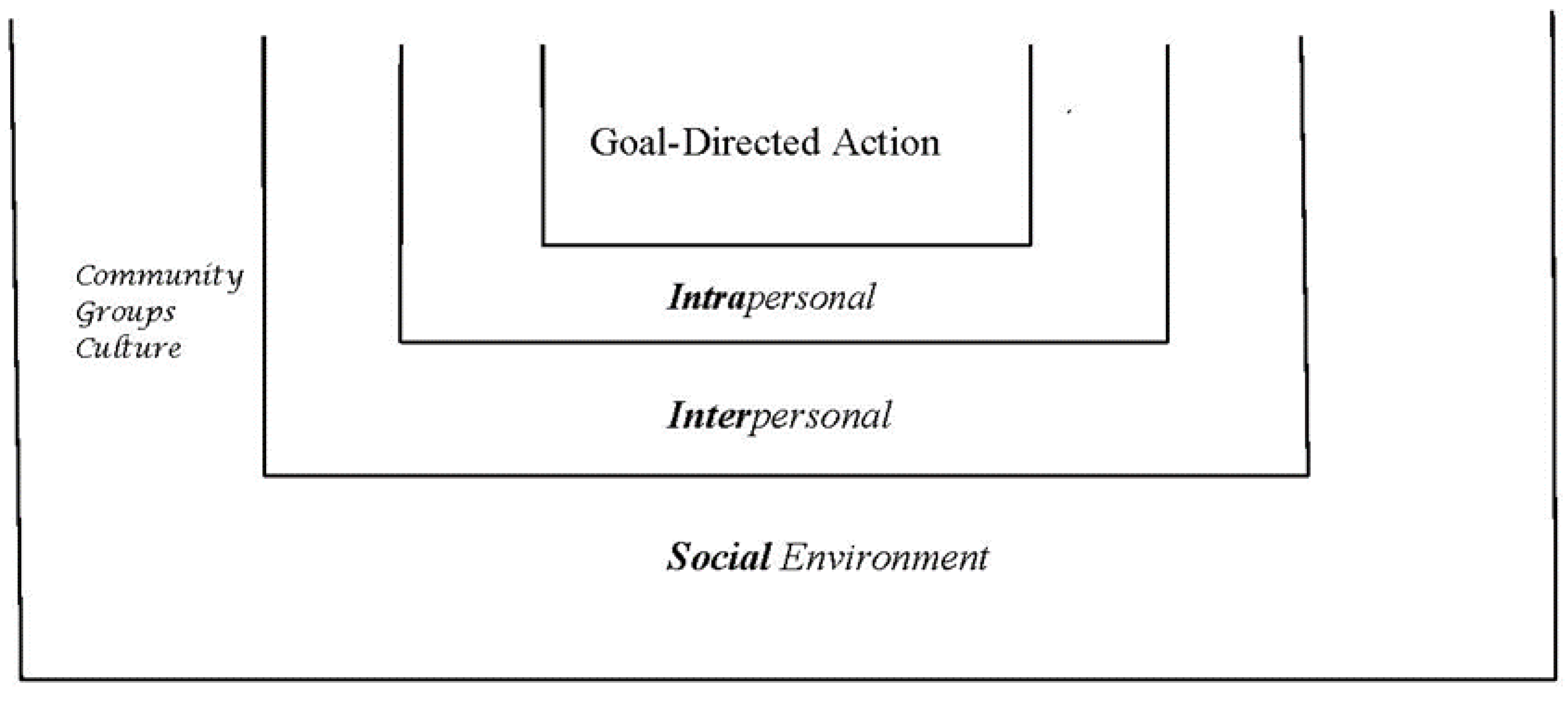
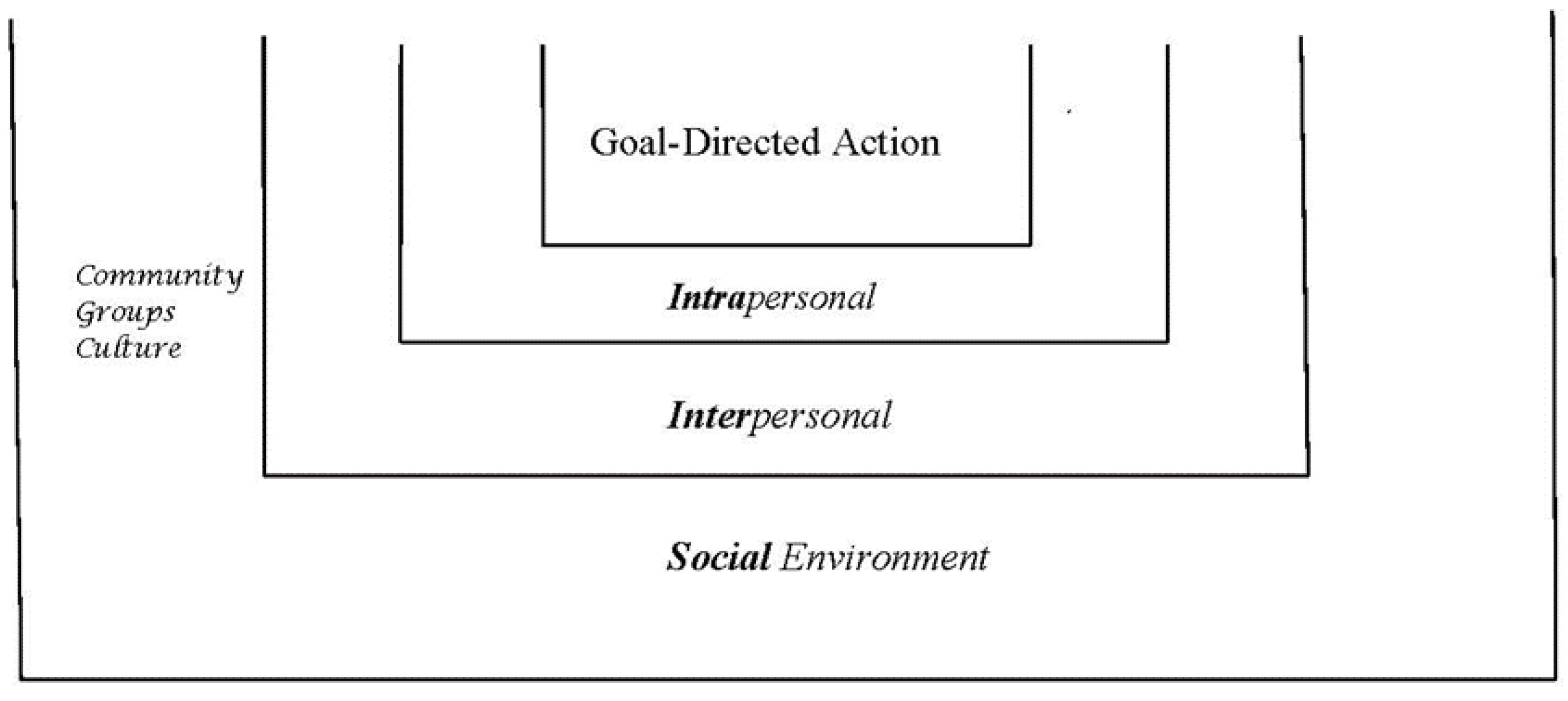
1.3.3. Resilience Training as Restoring and Training Goal-Directed Skills: A Model
- (1)
- Goal-directedness: The actions in the examples of engagement and the social relatedness examples were goal-directed. As reviewed earlier, the ideomotor theory defined goals as rooted in responses made to the effects or consequences of actions. Poetry chanting by Eugenia Ginzburg, a Russian journalist who became a political prisoner for 18 years in the Gulag, exemplifies this well. One line of poetry anticipates and has as its goal the chanting of the next line. Parenthetically, it can be noted that skilled performance is goal-directed.
- (2)
- Emotional valence: The actions of survivors were ones they valued and were accompanied by a certain emotional intensity, even passion.
- (3)
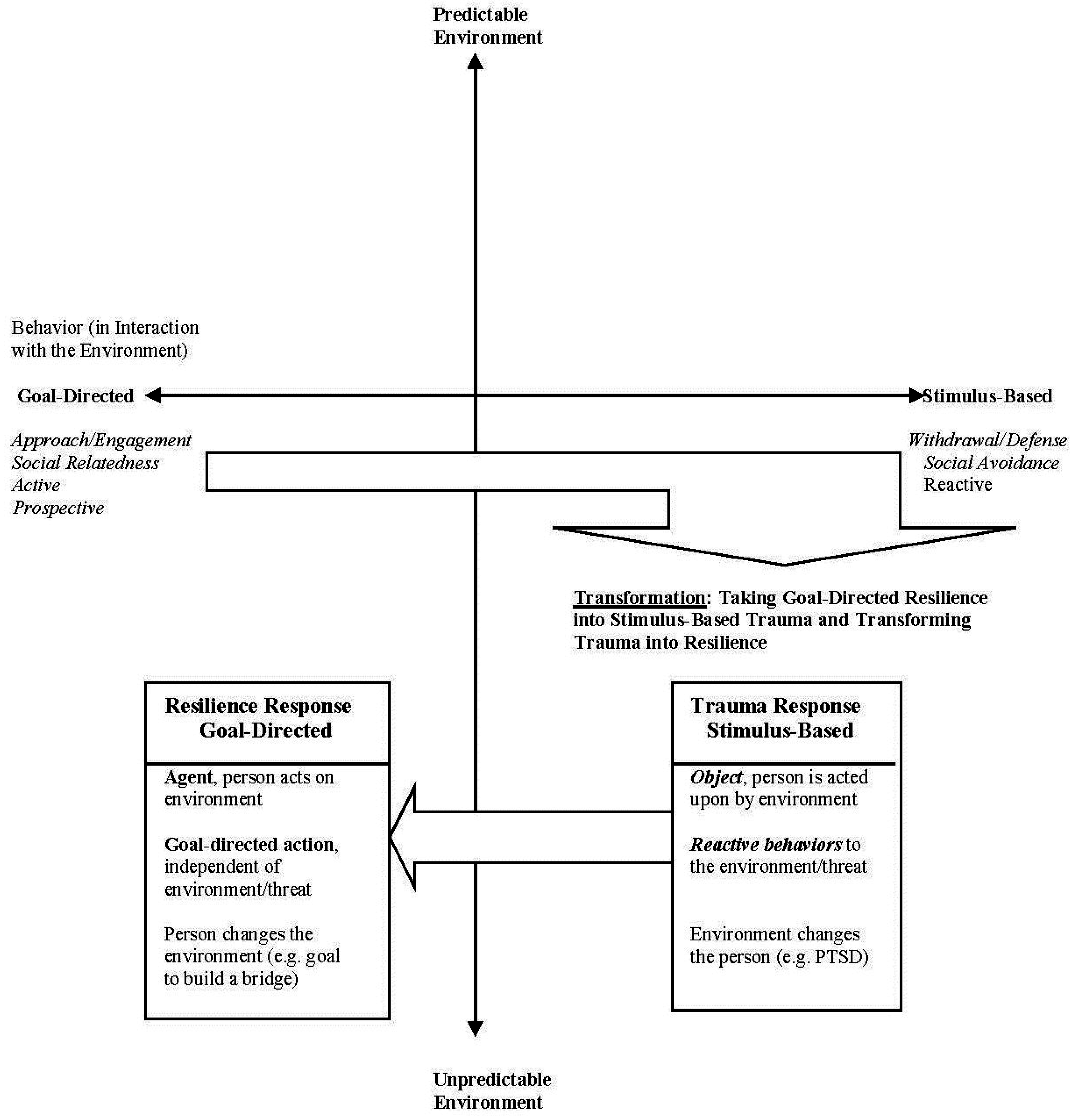
- Context independence: These actions were independent of the threatening context. This independence came as a result of the actors responding to the consequences of their actions rather than to the threatening environmental stimuli. This feature is easily missed and is so central that it requires to be underscored as a particularly adaptive element.
- (4)
- Altered environment: These goal-directed actions changed the environment or experiences of the environment whereas merely reacting to threat, or reactivity, changed the person.
- (5)
- Engagement/Social relatedness: Finally, the actions of engagement as expressed in interest, curiosity, or appreciation and social relatedness of empathy, compassion, or helping become resilience skills and life-preserving abilities when expressed in adverse contexts. They become the focal activity that holds its ground and prevails in the face of adversity.
1.3.4. Iconic Exemplars of Resilient Action
1.3.4.1. Approach/Engagement
1.3.4.2. Social Relatedness
1.3.5. Simulation of Goal-Directed Resilience
1.3.6. Summary of Survivor Themes
2. Method
2.1. Background
2.1.1. Simulation
2.1.2. Grounding New Skills in Sensation
2.2. Goal-Directed Resilience in Training (GRIT): A Model
- (1)
- Preparation. To allow participants to do the work of the program, a readily available calming response is required. Participants are asked to set traumatic experiences aside and find an episode from childhood or early adult years in which they are cherished and loved, or they cherish and love someone or something else. When stressed during the intervention, they are to return to this episode rather than remain stressed. Experiences of secure attachment restore feelings of safety even during high threat conditions and aid in healing trauma even when mobilized symbolically [117].
- (2)
- The elements. Participants identify approach/engagement and social relatedness experiences from childhood and early adulthood. Since these experiences are not novel but are already biologically established, they facilitate the re-experiencing of goal-directed responding and ground these in sensations. The view of memory as a construction made up of fragments of the past [118] is particularly compatible with the ‘simulated constructive’ approach of the program. Participants have an opportunity to find relevant past fragments and fashion new themes out of them.
- (3)
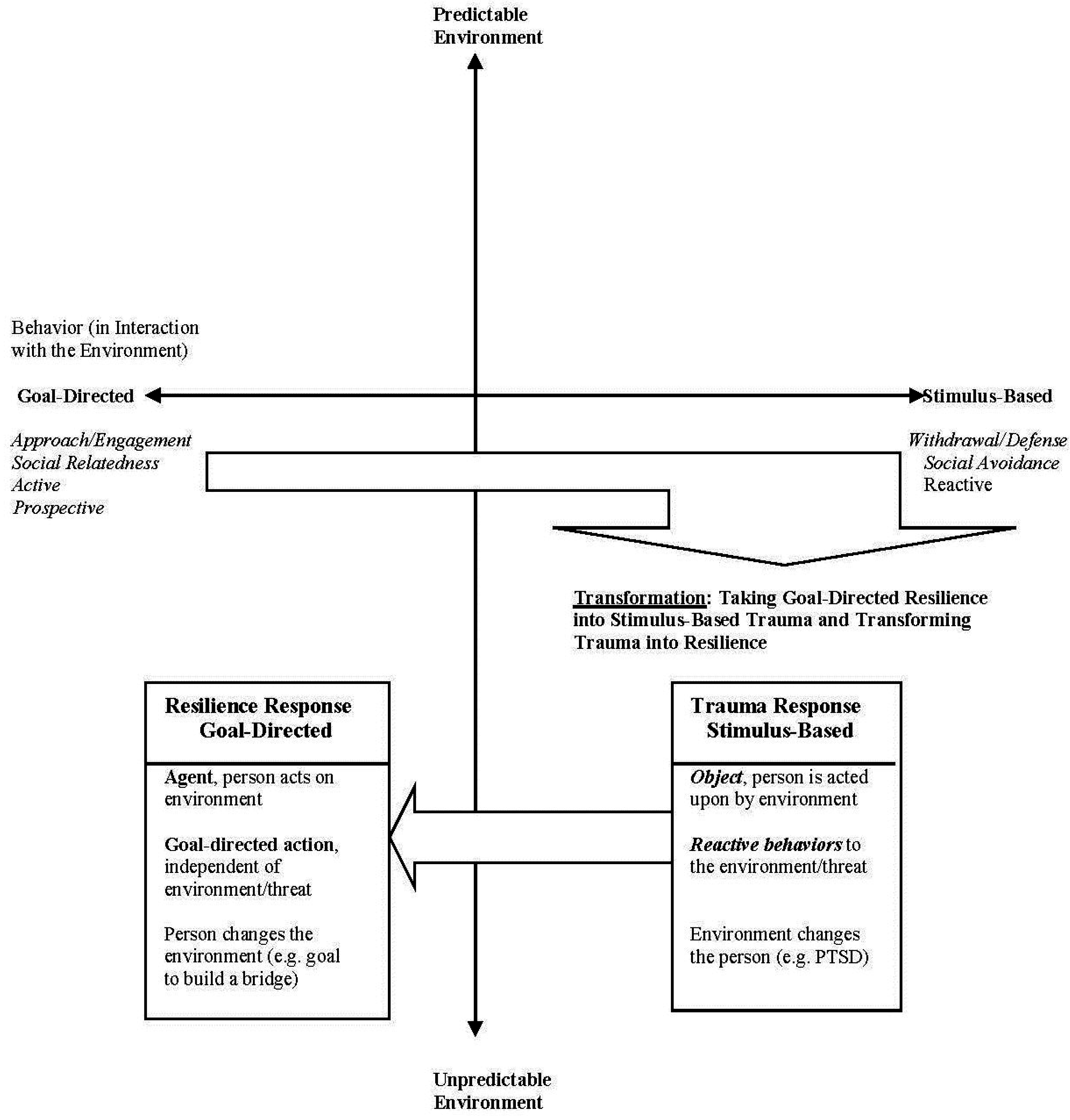
- Transformation. Approach/engagement and social relatedness episodes are used in a return to traumatic events. As noted earlier, engagement activities of interest or curiosity and social activities in themselves are relatively pleasant and innocuous. However, they become tools for transformation when facing challenges, thereby demonstrating adaptive action and ‘resilience’. A case example of transformation from past trials of the intervention comes from a Vietnam-era veteran who returned to a battle scene in his narrative with the activity and sensations of holding his first frog in his hands when he was five years old. The battle scene felt like the wiggling magical creature in his hands. Another case: a veteran returned to Baghdad as the boy fixing his toys and selling them on the sidewalk in Cleveland. The veteran described the sensations of the Cleveland sidewalk sale in Baghdad, the humid air of Ohio in Baghdad. The bombing in the Baghdad market took on a different feel and perspective. In this constructive approach to memory and sensation, the past is rearranged into a recombined memory with goal-directed action that is grounded in sensation and a prospective direction to the future.
- (4)
- The future. The goal-directed approach/engagement and social relatedness are applied to designing a good life with resilient responses to possible future challenges. Participants’ futures contain their own goals and interests and pathways to achieving them. Goal-directed engagement and relatedness are essential for flexible anticipatory adaptation capable of transforming reactivity. This process enables participants to create a new, resilient, and more integrated narrative of their lives that is rooted in their experiences and sensations.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Introduction | Introduction and Psychoeducation:
|
| Module I | Approach/Engagement:
|
| Module II | Social relatedness:
|
| Module III | Transformation: Simulation is used to integrate the newly re-established engagement and relatedness experiences of Modules I and II with an evocative context such as a stressful life event. Challenging experiences are revisited in a graded manner with the above practiced engagement and social relatedness experiences.
|
| Module IV | Building a Good Life: Participants will be asked to identify the key characteristics of a life well lived.
|
2.3. A Model for Goal-Directed Resilience Training in Evocative Contexts
- Physiological Features
- (1)
- Stress and dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis in PTSD and chronic pain.
- (2)
- Changes in cortical circuits that include PFC dysregulation and changes in the reward circuitry in all three conditions. Dysregulation of reward circuits.
- (3)
- Change in energy regulation and sleep.
- Environment as Precipitant
- (1)
- Environmental precipitants that include childhood trauma and adult trauma.
- (2)
- Hyperresponsivity to environmental stimuli, salience of threat or reward stimuli.
- Behavioral Features
- (1)
- Interference in social functions.
- (2)
- Interference in daily activities and work roles.
- (3)
- Change in reward system such that normal rewards from valued activities and social relationships are no longer rewarding and are replaced by avoidance of threat, seeking cessation of pain, overeating.
- Cognition
- (1)
- Attention is automatic and reflexive, with a negativity bias in PTSD and pain, reward salience in obesity, salience of threat and pain in PTSD and chronic pain, hypervigilance in PTSD.
- (2)
- Dysregulation of executive functions in all three conditions evident in the reduced ability to inhibit responses and pursue goal-directed action in order to realize future goals.
- (3)
- Learning is rapid and implemented by principles of conditioning, rather than slow learning, as in the learning of skills.
- Chronicity
- (1)
- All three conditions are chronic and are difficult to terminate or reverse.
- (2)
- All three curtail new experiences, new learning, and personal growth.
- (3)
- The results are a constricted range of experiences and an impoverished life.
2.4. A Model for Testing the Efficacy of Goal-Directed Resilience Training
- (1)
- (2)
- (3)
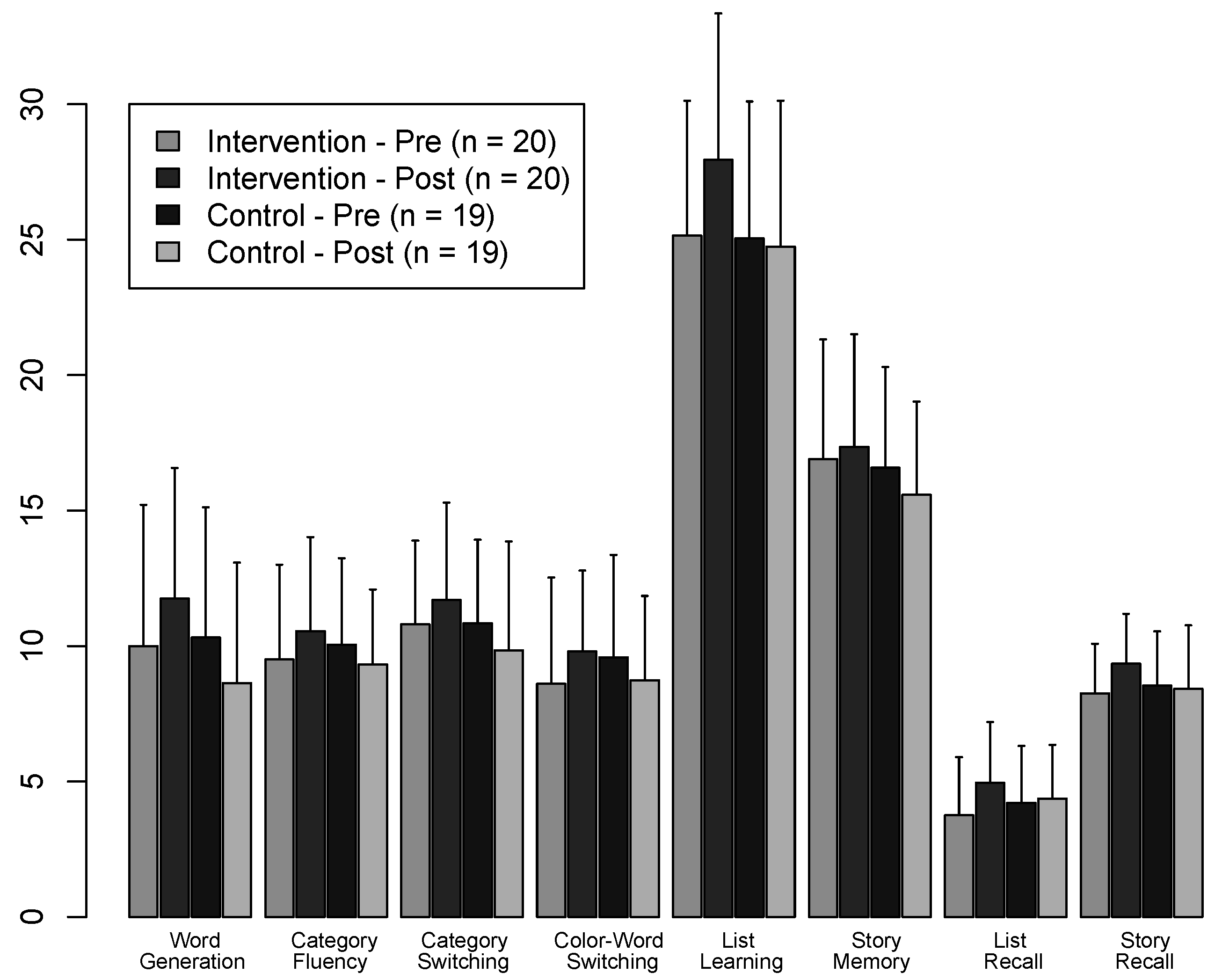
- Neuropsychological tests: Executive functions assessed with the Word Generation subtest of the Neuropsychological Assessment Battery [135], the Category Fluency, Category Switching, and Color-Word Switching subtests of the Delis-Kaplan executive Function System [136], Repeatable Battery for the Assessment of Neuropsychological Status [137] subtests assessed working memory and episodic memory. Alternative versions of all cognitive tests were employed at pre- and post-assessment.
- (4)
- Physiological/endocrine measures: We explored the feasibility of assessing cortisol changes with salivary cortisol and evaluated several devices for ease of use and reliability to assess heart rate variability.
3. Results Supporting the Model for Goal-Directed Resilience Training
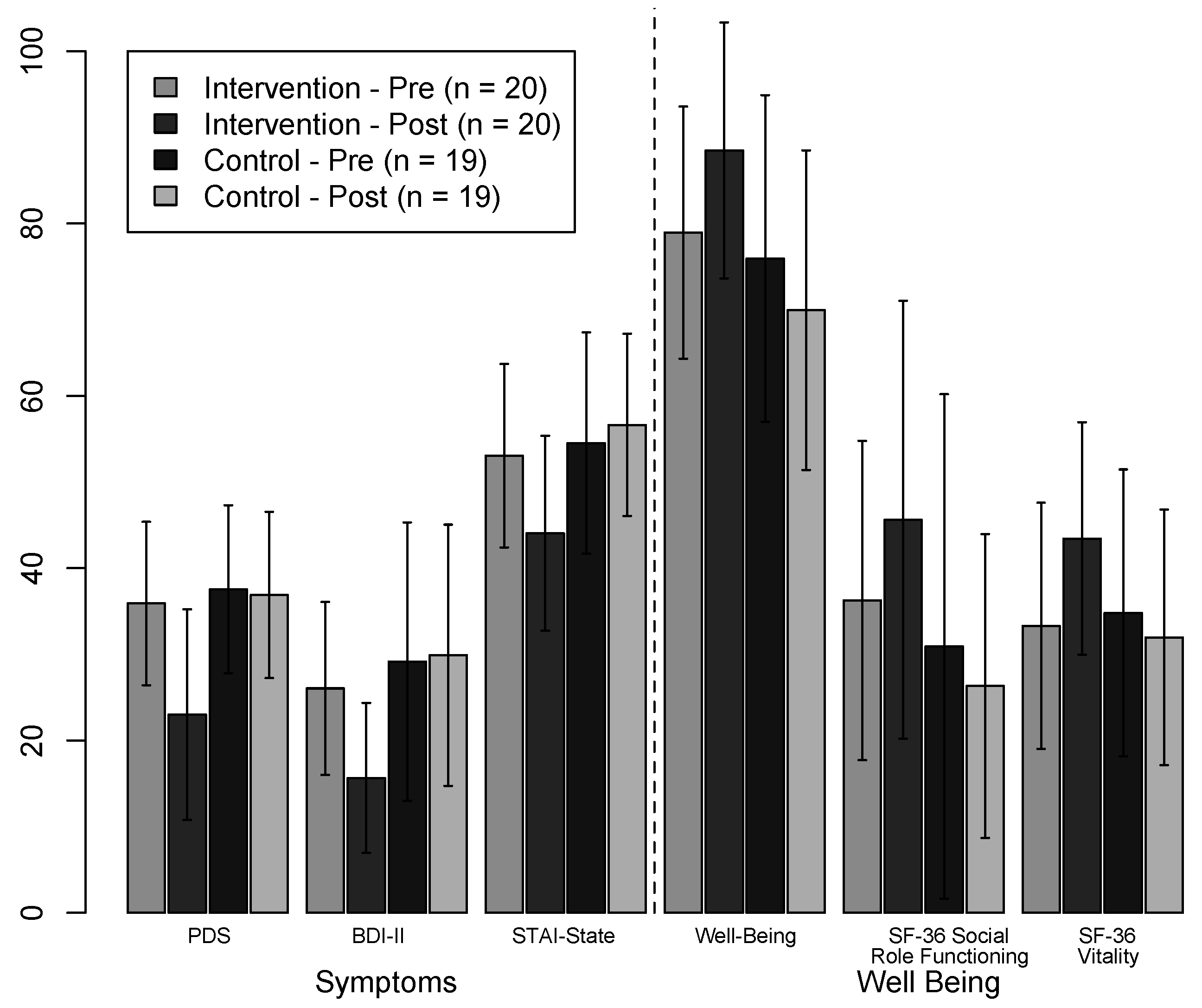
3.1. Posttraumatic Stress Disorder (PTSD)


3.2. Obesity
3.3. Chronic Pain
4. Discussion
4.1. Innovations of the Goal-Directed Resilience Training Model
- (1)
- Theory and model. We identify goal-directed action as the main element that needs to be restored in chronic evocative contexts in which stimulus-based reactivity has resulted in maladaptive conditions such as PTSD or obesity. Our model posits a reciprocal relationship between prospective and reactive responding that accounts for both adaptive and maladaptive behaviors, rather than just focusing on a theory that accounts for symptoms.
- (2)
- Method. Simulation is used in a step-by-step approach that includes re-experience of goal-directed elements that are then taken into a challenging situation, thereby simulating a resilient response. Our approach draws on personal experience and sensation to change bottom-up brain functions that have downstream effects that, in turn, help to restore top-down cognitive and affective processes through goal-directed action and positive affect, as are exemplified in engagement and social relatedness. The simulation includes repeated practice; special attention to sensation and expanding sensation beyond those felt in trauma, obesity, or pain; and special attention paid to the retention and generalization of gains.
- (3)
- Efficacy. Multiple functions are assessed with a multi-method approach for testing efficacy. Effectiveness of the intervention assesses not only symptoms but also well-being, effects on cortical functions as assessed by neuropsychological measures, and effects on biological functions as assessed with endocrine measures of cortisol, leptin and adeponectin.
- (4)
- Retention and generalization. Exercises allowed participants to apply concepts to their own lives, such as in “Life on Three Stages”. We sought to devise methods that incorporated the new knowledge gained from the intervention into participants’ lives. One approach was to have participants design a ‘good life’ with goals and a future they could look forward to, that could apply new learning that is generalized to other areas of their lives.
4.2. Limitations of the Goal-Directed Resilience Training Model
- (1)
- At the level of theory and model building, numerous details need to be developed. Examples are the adjustments and additional techniques in the intervention method for conditions that have unique characteristics beyond the evocative commonality, such as features unique to each of PTSD, obesity, pain, and others.
- (2)
- Simulation can be enhanced by applications developed for new technologies.
- (3)
- The multi-modal tests of efficacy do not yet include a wider array of endocrine functions and functional imaging. In addition, there is as yet no single scale that tests the main elements of the model, notably the predictability of the environment, approach-engagement, and social relatedness and how these three are affected by the intervention. So far we have used a patchwork of subscales from a variety of standardized tests, such as the SF-36 or Ryff’s Psychological Well-Being Scale. We are attempting to rectify this for chronic pain by developing a scale that will specifically test the main elements of the intervention.
- (4)
- The extent to which gains are retained and generalized need to be evaluated over time.
4.3. Future Directions of Goal-Directed Resilience Training
4.4. Conclusion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cannon, W.B. The Wisdom of the Body; Norton: New York, NY, USA, 1963. [Google Scholar]
- Kent, M.; Davis, M.C.; Reich, J.W. (Eds.) The Resilience Handbook: Approaches to Stress and Trauma; Routledge: New York, NY, USA, 2014.
- Dickinson, A.; Balleine, B. Motivational control of goal-directed action. Anim. Learn Behav. 1994, 22, 1–18. [Google Scholar] [CrossRef]
- Kenward, B.; Folke, S.; Holmberg, J.; Johansson, A.; Gredebäck, G. Goal directedness and decision making in infants. Dev. Psychol. 2009, 45, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Polak, A.R.; Witteveen, A.B.; Reitsma, J.B.; Olff, M. The role of executive function in posttraumatic stress disorder: A systematic review. J. Affect. Disorders 2012, 141, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Olff, M.; Polak, A.R.; Witteveen, A.B.; Denys, D. Executive function in posttraumatic stress disorder (PTSD) and the influence of comorbid depression. Neurobiol. Learn. Mem. 2014, 112, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Rivers, C.; Zautra, A.J.; Davis, M.C. Resilience. To appear in; In The Encyclopedia of Mental Health, 2nd ed.; Friedman, H., Ed.; Elsevier: New York, NY, USA, 2015; in press. [Google Scholar]
- Garmezy, N. Vulnerability research and the issue of primary prevention. Am. J. Orthopsychiat. 1971, 41, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M. Protective factors in children’s response to stress and disadvantage. In Primary Prevention of Psychopathology: Social Competence in Children; Kent, M.W., Rolf, J.E., Eds.; University Press of New England: Hanover, NH, USA, 1979; Volume 3, pp. 49–74. [Google Scholar]
- Bonanno, G.A.; Diminich, E.D. Annual Research Review: Positive adjustment to adversity-trajectories of minimal–impact resilience and emergent resilience. J. Child Psychol. Psyc. 2013, 54, 378–401. [Google Scholar] [CrossRef] [PubMed]
- Rivers, C. Role of Cognitive Shift in Resilient Adaptation to Difficult Events (UMI No. 1555827). Master’s thesis, Arizona State University, Tempe, 2014. [Google Scholar]
- Zautra, A.J.; Arewasikporn, A.; Davis, M.C. Resilience: Promoting well-being through recovery, sustainability, and growth. Res. Hum. Dev. 2010, 7, 221–238. [Google Scholar] [CrossRef]
- Kent, M. From neuron to social context: Restoring resilience as a capacity for good survival. In The Social Ecology of Resilience: A Handbook of Theory and Practice; Ungar, M., Ed.; Springer: New York, NY, USA, 2012; pp. 111–125. [Google Scholar]
- Elliot, A.J. The hierarchical model of approach-avoidance motivation. Motiv. Emot. 2006, 30, 111–116. [Google Scholar] [CrossRef]
- Haggard, P. Human volition: Towards a neuroscience of will. Nat. Rev. Neurosci. 2008, 9, 934–946. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, M.; Shulman, G.L. Control of goal-directed and stimulus-driven attention in the brain. Nat. Rev. Neurosci. 2002, 3, 201–218. [Google Scholar] [CrossRef] [PubMed]
- Vittersø, J.; Søholt, Y.; Hetland, A.; Thoresen, I.A.; Røysamb, E. Was Hercules happy? Some answers from a functional model of human well-being. Social Indic. Res. 2010, 95, 1–18. [Google Scholar]
- Rotter, J.B. Generalized expectancies and internal versus external control of reinforcement. Psychol. Monogr. 1966, 80, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Tops, M.; Luu, P.; Boksem, M.A.S.; Tucker, D.M. The roles of predictive and reactive biobehavioral programs in resilience. In The Resilience Handbook: Approaches to Stress and Trauma, 1st ed.; Kent, M., Davis, M.C., Reich, J.W., Eds.; Routledge: New York, NY, USA, 2014; pp. 15–32. [Google Scholar]
- Tops, M.; Boksem, M.A.S.; Quirin, M.; Ijzerman, H.; Koole, S.L. Internally directed cognition and mindfulness: An integrative perspective derived from predictive and reactive control systems theory. FPSYG 2014, 5, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tops, M.; Koole, S.L.; Ijzerman, H.; Buisman-Pijlman, F.T.A. Why social attachment and oxytocin protect against addiction and stress: Insights from the dynamics between ventral and dorsal corticostriatal systems. Pharmacol. Biochem. Behav. 2014, 119, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Jilka, S.R.; Scott, G.; Ham, T.; Pickering, A.; Bonnelle, V.; Braga, R.M.; Leech, R.; Sharp, D.J. Damage to the salience network and interactions with the default mode network. J. Neursci. 2014, 34, 10798–10807. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L.; Grewen, K.M.; Coffey, K.A.; Algoe, S.B.; Firestine, A.M.; Arevalo, J.M.G.; Ma, J.; Cole, S.W. A functional genomic perspective on human well-being. Proc. Natl. Acad. Sci. USA. 2013, 110, 13684–13689. [Google Scholar] [CrossRef] [PubMed]
- Gentsch, A.; Synofzik, M. Affective coding: The emotional dimension of agency. FNHUM 2014, 8, 1–7. [Google Scholar]
- Elliot, A.J. (Ed.) Approach and avoidance motivation. In Handbook of Approach and Avoidance Motivation; Psychology Press: New York, NY, USA; pp. 3–14.
- Lewin, K. A Dynamic Theory of Personality; McGraw-Hill: New York, NY, USA, 1935. [Google Scholar]
- Hull, C.L. The goal-gradient hypothesis applied to some “field-force” problems in the behavior of young children. Psychol. Rev. 1938, 45, 271–299. [Google Scholar] [CrossRef]
- Miller, N.E. Liberalization of basic S-R concepts: Extensions to conflict behavior and social learning. In Psychology: A Study of a Science; Koch, S., Ed.; McGraw-Hill: New York, NY, USA, 1959; Volume 2, pp. 431–465. [Google Scholar]
- Dollard, J.; Miller, N.E. Personality and Psychotherapy; McGraw-Hill: New York, NY, USA, 1950. [Google Scholar]
- Freud, S. The unconscious (1915). In General Psychological Theory: Papers on Metapsychology; Rieff, P., Ed.; Touchstone/Simon & Shuster: New York, NY, USA, 1991. [Google Scholar]
- James, W. The Principles of Psychology; Henry Holt & Co.: New York, NY, USA, 1890; Volume 2. [Google Scholar]
- Elliot, A.J.; Eder, A.B.; Harmon-Jones, E. Approach-avoidance motivation in emotion: Convergence and divergence. Emot. Rev. 2013, 5, 308–311. [Google Scholar] [CrossRef]
- Schneirla, T.C. An evolutionary and developmental theory of biphasic processes underlying approach and withdrawal. In Nebraska Symposium on Motivation; Jones, M.R., Schneirla, T.C., Eds.; University of Nebraska Press: Lincoln, NB, USA, 1959; Volume 7, pp. 1–42. [Google Scholar]
- Rolls, E.E. What are emotional states and why do we have them? Emot. Rev. 2013, 5, 241–247. [Google Scholar] [CrossRef]
- Aarts, H.; Elliot, A.J. (Eds.) Goal-Directed Behavior; Psychology Press/Taylor & Francis: New York, NY, USA, 2012.
- Moskowitz, B.B.; Grant, H. (Eds.) The Psychology of Goals; Guilford Press: New York, NY, USA, 2009.
- Ekman, P. Cross-cultural studies of facial expression. In Darwin and Facial Expression: A Century of Research in Review; Ekman, P., Ed.; Academic Press: New York, NY, USA, 1973; pp. 169–222. [Google Scholar]
- Russell, J.A. A circumplex model of affect. J. Pers. Soc. Psychol. 1980, 39, 1161–1178. [Google Scholar] [CrossRef]
- Watson, D.; Tellege, A. Toward a consensual structure of mood. Psychol. Bull. 1985, 98, 219–235. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A. Affective space is bipolar. J. Pers. Soc. Psychol. 1979, 37, 345–356. [Google Scholar] [CrossRef]
- Russell, J.A.; Feldman Barrett, L. Core affect, prototypical emotional episodes, and other things called emotion: Dissecting the elephant. J. Pers. Soc. Psychol. 1999, 76, 805–819. [Google Scholar] [CrossRef] [PubMed]
- Reich, J.W.; Zautra, A.J.; Davis, M.C. Dimensions of affect relationships: Models and their integrative implications. Rev. Gen. Psychol. 2003, 7, 66–83. [Google Scholar] [CrossRef]
- Gray, J.A. A critique of Eysenck’s theory of personality. In A Model for Personality; Eysenck, H.J., Ed.; Springer Verlag: Berlin, Germany, 1981; pp. 246–276. [Google Scholar]
- Gray, J.A. The Neuropsychology of Anxiety: An Enquiry into the Functions of the Septo-Hippocampal System; Oxford University Press: New York, NY, USA, 1982. [Google Scholar]
- Sutton, S.K.; Davidson, R.J. Prefrontal brain asymmetry: A biological substrate of the behavioral approach and inhibition system. Psychol. Sci. 1997, 8, 204–210. [Google Scholar] [CrossRef]
- Prinz, W. Perception and action planning. Eur. J. Cogn. Psychol. 1997, 9, 129–154. [Google Scholar] [CrossRef]
- Hommel, B.; Muesseler, J.; Aschersleben, G.; Prinz, W. The theory of event coding (TEC): A framework for perception and action planning. Behav. Brain. Sci. 2001, 24, 849–878. [Google Scholar] [CrossRef] [PubMed]
- Hommel, B. Ideomotor action control: On the perceptual grounding of voluntary actions and agents. In Action Science: Foundations of an Emerging Discipline; Prinz, W., Beisert, M., Herwig, A., Eds.; MIT Press: Cambridge, MA, USA, 2013; pp. 113–136. [Google Scholar]
- Eder, A.B.; Hommel, B. Anticipatory control of approach and avoidance: An ideomotor approach. Emot. Rev. 2013, 5, 275–279. [Google Scholar] [CrossRef]
- Herwig, A.; Waszak, F. Action-effect bindings and ideomotor learning in intention- and stimulus-based actions. FPSYG 2012, 3, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Waszak, F.; Wascher, E.; Keller, P.; Koch, I.; Aschersleben, G.; Rosenbaum, D.A.; Prinz, W. Intention-based and stimulus-based mechanisms in action selection. Exp. Brain Res. 2005, 162, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Haggard, P.; Clarke, S. Intentional action: Conscious experience and neural prediction. Conscious Cogn. 2003, 12, 695–707. [Google Scholar] [CrossRef]
- Corbetta, M.; Patel, P.; Shulman, G.L. The reorienting system of the human brain: From environment to theory of mind. Neuron 2008, 58, 306–324. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B. There is no such thing as attention. FPSYG 2011, 2, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Morey, R.A.; Dolcos, F.; Petty, C.M.; Cooper, D.A.; Hayes, J.P.; LaBar, K.S.; McCarthy, G. The role of trauma-related distractors on neural systems for working memory and emotion processing in posttraumatic stress disorder. J. Psychiat. Res. 2008, 43, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Astor-Jack, T.; Haggard, P. Intention and reactivity. In Attention in Action: Advances from Cognitive Neuroscience; Humphreys, G.W., Riddoch, M.J., Eds.; Psychology Press/Taylor & Francis: New York, NY, USA, 2005; pp. 131–149. [Google Scholar]
- Hannus, A.; Neggers, S.F.W.; Cornelissen, F.W.; Bekkering, H. Selective attention for action: New evidence from visual search studies. In Attention in Action: Advances from Cognitive Neuroscience; Humphreys, G.W., Riddoch, M.J., Eds.; Psychology Press/Taylor & Francis: New York, NY, USA, 2005; pp. 109–120. [Google Scholar]
- Tops, M. Slow life history strategies and slow updating of internal models: The examples of conscientiousness and obsessive-compulsive disorder. Psychol. Inq. 2014, 25, 376–384. [Google Scholar] [CrossRef]
- Quirin, M.; Kent, M.; Boksem, M.A.S.; Tops, M. Integration of negative experiences: A neuropsychological framework for human resilience. Behav. Brain Sci. 2014, in press. [Google Scholar]
- Kalisch, R.; Müller, M.B.; Tüscher, O. A conceptual framework for the neurobiological study of resilience. Behav. Brain Sci. 2014, 1–49. [Google Scholar] [CrossRef] [PubMed]
- Copleston, F. A History of Philosophy: Greece and Rome; Doubleday: New York, NY, USA, 2003; Volume 1. [Google Scholar]
- Aristotle. In Nicomachean Ethics; Irwin, T., Translator; Hackett: Indianapolis, IN, USA, 1985.
- Annas, J. The Morality of Happiness; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Vittersø, J.; Oelmann, H.I.; Wang, A.L. Life satisfaction is not a balanced stimator of the good life: Evidence from reaction time measures and self-reported emotions. J. Happiness Stud. 2009, 10, 1–17. [Google Scholar] [CrossRef]
- Karlsen, E.; Dybdahl, R.; Vittersø, J. The possible benefits of difficulty: How stress can increase and decrease subjective well-being. Scand. J. Psychol. 2006, 47, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Simmen-Janevska, K.; Brandstätter, V.; Maercker, A. The overlooked relationship between motivational abilities and posttraumatic stress: A review. Eur. J. Psychotraumatol. 2012, 3, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFarlane, A.C. Resilience, vulnerability, and the course of posttraumatic reactions. In Traumatic Stress: The Effects of Overwhelming Experience of Mind, Body, and Society; van der Kolk, B.A., McFarlane, A.C., Weisaeth, L., Eds.; Guilford Press: New York, NY, USA, 1996; pp. 155–181. [Google Scholar]
- Levin, A. PTSD not sufficient to explain responses to trauma. Psychiatric News. 18 August 2006. Available online: http://psychnews.psychiatryonline.org/newsarticle.aspx?articleid=110242 (accessed on 20 April 2015).
- Smith, T. 1 Month since the bombings, signs of progress in Boston. 15 May 2013. Retrieved 20 April 2015. Available online: http://www.npr.org/2013/05/15/184132974/1-month-since-the-bombings-signs-of-progress-in-boston (accessed on 20 April 2015).
- Hayes, S.C. Acceptance and commitment therapy and the new behavior therapies: Mindfulness, acceptance, and relationship. In Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition; Hayes, S.C., Follette, V.M., Linehan, M.M., Eds.; Guilford Press: New York, NY, USA, 2004; pp. 1–29. [Google Scholar]
- Linehan, M.M. Cognitive Behavioral Treatment for Borderline Personality Disorder; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Cloitre, M.; Cohen, L.R.; Koenen, K.C. Treating Survivors of Childhood Abuse: Psychotherapy for the Interrupted Life; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Najavits, L.M. Seeking Safety: A Treatment Manual for PTSD and Substance AAbuse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Lewinsohn, P.M. The behavioral study and treatment of depression. In Progress in Behavior Modification; Hersen, M., Eisler, R.M., Miller, P.M., Eds.; Academic Press: New York, NY, USA, 1975; pp. 19–65. [Google Scholar]
- Jacobson, N.S.; Martell, C.R.; Dimidjian, S. Behavioral activation for depression: Returning to contextual roots. Clin. Psychol. Sci. Pract. 2001, 8, 255–270. [Google Scholar] [CrossRef]
- Dichter, G.S.; Smoski, M.; Henderson, R.K.; Dimidjian, S. Behavioral activation as a treatment for depression: Theory, neurobiologic effects, and potential linkages to resilience. In The Resilience Handbook: Approaches to Stress and Trauma, 1st ed.; Kent, M., Davis, M.C., Reich, J.W., Eds.; Routledge: New York, NY, USA, 2014; pp. 211–226. [Google Scholar]
- Fava, G.A.; Ruini, C. Development and characteristics of a well-being enhancing psychotherapeutic strategy: Well-being therapy. J. Behav. Ther. Exp. Psychiatry 2003, 34, 45–63. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B. The contours of positive human health. Psychol. Inq. 1998, 9, 1–28. [Google Scholar] [CrossRef]
- Teasdale, J.D.; Segal, Z.V.; Williams, J.M.G.; Ridgeway, V.A.; Soulsby, J.M.; Lau, M.A. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. J. Consult. Clin. Psychol. 2000, 68, 615–623. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis: A Mmethods Sourcebook, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Durlak, J.A.; Wells, A.M. Primary prevention mental health programs for children and adolescents: A meta-analytic review. Am. J. Commun. Psychol. 1997, 25, 115–152. [Google Scholar]
- Johnson, D.L. The Houston Parent-Child Development Center Project. Prev. Hum. Serv. 1990, 7, 89–108. [Google Scholar] [CrossRef]
- Wolchik, S.A.; Sandler, I.N.; Millsap, R.E.; Plummer, B.A.; Greene, S.M.; Anderson, E.R.; Dawson-McClure, S.R.; Hipke, K.; Haine, R.A. Six-year follow-up of preventive interventions for children of divorce: A randomized controlled trial. JAMA 2002, 288, 874–1881. [Google Scholar] [CrossRef]
- Nash, W.P.; Krantz, L.; Stein, N.; Westphal, R.J.; Litz, B. Comprehensive soldier fitness, battlemind, and the stress continuum model: Military organizational approaches to prevention. In Caring for Veterans with Deployment-Related Stress Disorders; Ruzek, J.I., Schnurr, P.P., Vasterling, J.J., Friedman, M.J., Eds.; American Psychological Association: Washington, DC, USA, 2011; pp. 193–214. [Google Scholar]
- Cigrang, J.A.; Wayne Talcott, G.; Tatum, J.; Baker, M.; Cassidy, D.; Sonnek, S.; Smith Slep, A.M. Impact of combat deployment on psychological and relationship health: A longitudinal study. J. Trauma Stress 2014, 27, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Sayer, N.A.; Carlson, K.F.; Frazier, P.A. Reintegration challenges in U.S. service members and veterans following combat deployment. Soc. Issues Policy Rev. 2014, 8, 33–73. [Google Scholar] [CrossRef]
- Adler, A.B.; Castro, C.A.; McGurk, D. Time-Driven Battlemind Psychological Debriefing: A group-level early intervention in combat. Mil. Med. 2009, 174, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Southwick, S.M.; Litz, B.T.; Charney, D.; Friedman, M.J. (Eds.) Resilience and Mental Health: Challenges across the Lifespan, 1st ed.; Cambridge University Press: New York, NY, USA, 2011.
- Ungar, M. (Ed.) The Social Ecology of Resilience: A Handbook of Theory and Practice; Springer: New York, NY, USA, 2012.
- Sinclair, R.R.; Britt, T.W. (Eds.) Building Psychological Resilience in Military Personnel: Theory and Practice; American Psychological Association: Washington, DC, USA, 2013.
- Kreuter, E.A. Fostering Resilience for Loss and Irrelevance; Springer: New York, NY, USA, 2012. [Google Scholar]
- Rodin, J. The Resilience Dividend: Being Strong in a World Where Things Go Wrong; Rockefeller Foundation: New York, NY, USA, 2014. [Google Scholar]
- Resnick, B.; Gwyther, L.P. (Eds.) Resilience in Aging: Concepts, Research, and Outcomes; Springer: New York, NY, USA, 2010.
- Reich, J.W.; Zautra, A.J.; Hall, J.S. (Eds.) Handbook of Adult Resilience; Guilford Press: New York, NY, USA, 2010.
- Masten, A.S.; Best, K.M.; Garmezy, N. Resilience and development: Contributions from the study of children who overcame adversity. Dev. Psychopathol. 1990, 2, 425–444. [Google Scholar] [CrossRef]
- Luthar, S.S. Resilience in development: A synthesis of research across five decades. In Developmental Psychopathology, 2nd ed.; Cohen, D.J., Cicchetti, D., Eds.; Wiley: Hoboke, NJ, USA, 2006; pp. 739–795. [Google Scholar]
- Judd, G. This Emotional Life; Nova/WGBH Science Unit & Vulcan Productions. Film produced by Kunhardt McGee Productions: Seattle, WA, USA, 2010. [Google Scholar]
- Ginzburg, E.S. Journey into the Whirlwind; Stevenson, P.; Hayward, M., Translators; Harcourt Brace Jovanovich: New York, NY, USA, 1967; pp. 220–221. [Google Scholar]
- Ginzburg, E. Within the Whirlwind; Boland, I., Translator; Harcourt, Brace, Jovanovich: New York, NY, USA, 1981. [Google Scholar]
- Leet, M.; Phoenix, AZ, USA. Personal Communication, 1984.
- Terr, L.C. Children of Chowchilla: A study of psychic trauma. Psychoanal. Stud. Chil. 1979, 34, 547–623. [Google Scholar]
- Ritchie, G.G.; Sherrill, E. Return from Tomorrow; Baker Book House: Grand Rapids, MI, USA, 1978. [Google Scholar]
- Levi, P. Survival in Auschwitz; Collier Books/Macmillan Publishing Co.: New York, NY, USA, 1959; p. 58. [Google Scholar]
- Delbo, C. Auschwitz and after; Lamont, R.C., Translator; Yale University Press: New Haven, MA, USA, 1995; p. 63. [Google Scholar]
- Decety, J.; Grèzes, J. The power of simulation: Imagining one’s own and other’s behavior. Brain Res. 2006, 1079, 4–14. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; Mulder, T. Motor imagery and stroke rehabilitation: A critical discussion. J. Rehabil. Med. 2007, 39, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Ticini, L.F.; Schütz-Bosbach, S.; Weiss, C.; Casile, A.; Waszak, F. When sounds become actions: Higher-order representation of newly learned action sounds in the human motor system. J. Cogn. Neurosci. 2012, 24, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Hauk, O.; Johnsrude, I.; Pulvermüller, F. Somatotopic representation of action words in human motor and premotor cortex. Neuron 2004, 41, 301–307. [Google Scholar] [CrossRef]
- Keysers, C.; Wicker, B.; Gazzola, V.; Anton, J.L.; Fogassi, L.; Gallese, V. A Touching sight: SII/PV activation during the observation and experience of touch. Neuron 2004, 42, 335–346. [Google Scholar] [CrossRef]
- Kent, M.; Davis, M.C.; Stark, S.L.; Stewart, L.A. A resilience-oriented treatment for posttraumatic stress disorder: Results of a preliminary randomized clinical trial. J. Trauma Stress 2011, 24, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Aupperle, R.L.; Melrose, A.J.; Stein, M.B.; Paulus, M.P. Executive function and PTSD: Disengaging from trauma. Neuropharmacolog 2011, 62, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Svensson, H.; Morse, A.F.; Ziemke, T. Neural pathways of embodied simulation. In ABiALS, LNAI; Pezzulo, G., Butz, M.V., Sigaud, O., Baldassarre, G., Eds.; Springer Verlag: Berlin, Germany, 2009; Volume 5499, pp. 95–114. [Google Scholar]
- Mikulincer, M.; Shaver, P.R.; Horesh, N. Attachment bases of emotion regulation and posttraumatic adjustment. In Emotion Regulation in Couples and Families: Pathways to Dysfunction and Health; Snyder, D.K., Simpson, J.A., Huges, J.N., Eds.; American Psychological Association: Washington, DC, USA, 2006; pp. 77–99. [Google Scholar]
- Schacter, D.L.; Addis, D.R. The cognitive neuroscience of constructive memory: Remembering the past and imagining the future. Phil. Trans. Roy. Soc. Lond. B Biol. Sci. 2007, 362, 773–786. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.E.; Schneider, S.K. Coping and the simulation of events. Soc. Cogn. 1989, 7, 174–194. [Google Scholar]
- Shakespeare, W. The Complete Works of William Shakespeare; Craig, W.J., Ed.; Oxford University Press: London, UK, 1916. [Google Scholar]
- Insel, T.; Cuthbert, B.; Garvey, M.; Heinssen, R.; Pine, D.S.; Quinn, K.; et al. Research domain criteria (RDoC): Toward a new classification framework for research on mental disorders. Am. J. Psychiatry 2010, 167, 748–751. [Google Scholar]
- Rassp, R.G. Pain disorders and the new DSM-5. LexisNexis Workers Compensation eNewsletter National Edition 2013, 4. [Google Scholar]
- Marcus, M.D.; Wildes, J.E. Obesity in DSM-5. Psychiat Ann. 2012, 42, 431–435. [Google Scholar] [CrossRef]
- Moriarty, O.; McGuire, B.E.; Finn, D.P. The effect of pain on cognitive function: A review of clinical and preclinical research. Prog. Neurobiol. 2011, 93, 385–404. [Google Scholar] [CrossRef] [PubMed]
- Palyo, S.A.; Beck, J.G. Post-traumatic stress disorder symptoms, pain, and perceived life control: Associations with psychosocial and physical functioning. Pain 2005, 117, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Elias, M.F.; Goodell, A.L.; Waldstein, S.R. Obesity, cognitive functioning and dementia: Back to the future. J. Alzheimers Dis. 2012, 30 (Suppl. 2), S113–S125. [Google Scholar] [PubMed]
- Kent, M. Building Resilience out of Trauma; University of Winnipeg: Winnipeg, MB, Canada, 2005. [Google Scholar]
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a clinician-administered PTSD scale. J. Trauma Stress 1995, 8, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (PCL-5). 2013; Scale available from the National Center for PTSD. Available online: www.ptsd.va.gov (accessed on 23 May 2015). [Google Scholar]
- Beck, A.T.; Brown, G.; Steer, R.A. Beck Depression Inventory II Manual; The Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Ware, J.E.; Kosinski, M.; Keller, S.D. SF-36 Physical and Mental Health Summary Scales: A Users’ Manual. The Health Institute: Boston, MA, USA, 1994. [Google Scholar]
- Ryff, C.D.; Singer, B. Psychological well-being: Meaning, measurement, and implications for psychotherapy research. Psychother. Psychosom. 1996, 65, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Stern, R.A.; White, T. Neuropsychological Assessment Battery (NAB); Psychological Assessment Resources, Inc.: Lutz, FL, USA, 2003. [Google Scholar]
- Delis, D.C.; Kaplan, E.; Kramer, J.H. Delis-Kaplan Executive Function System (D-KEFS) Examiner’s Manual; The Psychological Corporation: San Antonio, TX, USA, 2001. [Google Scholar]
- Randolph, C. Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) Manual; Pearson Clinical Assessment: Bloomington, MN, USA, 2012. [Google Scholar]
- Powers, M.B.; Halpern, J.M.; Ferenschak, M.P.; Gillihan, S.J.; Foa, E.B. A meta-analytic review of prolonged exposure for posttraumatic stress disorder. Clin. Psychol. Rev. 2010, 30, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Schnurr, P.P. The rocks and hard places in psychotherapy outcome research. J. Trauma Stress 2007, 20, 779–792. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. Health, United States, 2006 with Chartbook on Trends in the Health of Americans. National Center for Health Statistics: Hyattsville, MD, USA, 2006. Available online: http://www.cdc.gov/nchs/data/hus/hus06.pdf (accessed on 23 May 2015). [Google Scholar]
- Gentsch, A.; Schütz-Bosbach, S.; Endrass, T.; Kathmann, N. Dysfunctional forward model mechanisms and aberrant sense of agency in obsessive-compulsive disorder. Biol. Psychiat. 2012, 71, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Blakemore, S.; Wolpert, D.M.; Frith, C.D. Abnormalities in the awareness of action. Trends Cogn. Sci. 2002, 6, 237–242. [Google Scholar] [CrossRef]
- Synofzik, M.; Their, P.; Leube, D.T.; Schlotterbeck, P.; Lindner, A. Misattributions of agency in schizophrenia are based on imprecise predictions about the sensory consequences of one’s actions. Brain 2010, 133, 262–271, (First published). [Google Scholar] [CrossRef] [PubMed]
- Alvares, G.A.; Balleine, B.W.; Guastella, A.J. Impairments in goal-directed actions predict treatment response to cognitive-behavioral therapy in social anxiety disorder. PLoS ONE 2014, 9, 1–7. [Google Scholar]
- Griffiths, K.R.; Morris, R.W.; Balleine, B.W. Translational studies of goal-directed action as a framework for classifying deficits across psychiatric disorders. FNSYS 2014, 8, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Starcke, K.; Brand, M. Decision making under stress: A selective review. Neurosci. Biobehav. Rev. 2012, 36, 1228–1248. [Google Scholar] [CrossRef] [PubMed]
- Wrenn, G. Strengthening Resilience in African American Women with Clinically Significant Posttraumatic Stress Symptoms; A proposal submitted to R-CENTER Collaborative Clinical and Translational Pilot Project Program; Morehouse School of Medicine: Atlanta, GA, USA, 2014. [Google Scholar]
- Russo, S.J.; Murrough, J.W.; Han, M.H.; Charney, D.S.; Nestler, E.J. Neurobiology of resilience. Nat. Neurosci. 2012, 15, 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, J. Go Tell it on the Mountain; Random House: New York, NY, USA, 1995. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kent, M.; Rivers, C.T.; Wrenn, G. Goal-Directed Resilience in Training (GRIT): A Biopsychosocial Model of Self-Regulation, Executive Functions, and Personal Growth (Eudaimonia) in Evocative Contexts of PTSD, Obesity, and Chronic Pain. Behav. Sci. 2015, 5, 264-304. https://doi.org/10.3390/bs5020264
Kent M, Rivers CT, Wrenn G. Goal-Directed Resilience in Training (GRIT): A Biopsychosocial Model of Self-Regulation, Executive Functions, and Personal Growth (Eudaimonia) in Evocative Contexts of PTSD, Obesity, and Chronic Pain. Behavioral Sciences. 2015; 5(2):264-304. https://doi.org/10.3390/bs5020264
Chicago/Turabian StyleKent, Martha, Crystal T. Rivers, and Glenda Wrenn. 2015. "Goal-Directed Resilience in Training (GRIT): A Biopsychosocial Model of Self-Regulation, Executive Functions, and Personal Growth (Eudaimonia) in Evocative Contexts of PTSD, Obesity, and Chronic Pain" Behavioral Sciences 5, no. 2: 264-304. https://doi.org/10.3390/bs5020264