
Anxious-Withdrawal and Sleep Problems during Adolescence: The Moderating Role of Peer Difficulties

1
Department of Psychology, University at Buffalo, The State University of New York, Buffalo, NY 14260-4110, USA
2
Department of Human Development and Quantitative Methodology, University of Maryland, College Park, MD 20742, USA
*
Author to whom correspondence should be addressed.
Behav. Sci. 2023, 13(9), 740; https://doi.org/10.3390/bs13090740
Submission received: 25 July 2023
/
Revised: 29 August 2023
/
Accepted: 1 September 2023
/
Published: 5 September 2023
(This article belongs to the Special Issue The Developmental Trajectory of Children's Social Behaviors and Their Cognitive Neural Mechanisms)
Abstract
:Anxious-withdrawal is a well-established individual risk factor for psychosocial difficulties during adolescence. It is unknown, however, whether it also places youth at increased risk for physical health problems, such as sleep difficulties. This study examines the concurrent and prospective associations between anxious-withdrawal and six types of sleep difficulties (i.e., sleeping too much, sleeping too little, talking/walking in sleep, being overtired, nightmares, and general trouble sleeping). We further evaluate whether these associations differ for adolescents who are high versus low in exclusion and victimization. The participants were 395 adolescents (Mage = 13.61 years; 35% ethnic minority) who completed peer nominations of anxious-withdrawal, exclusion, and victimization at Time 1 (T1). Their mothers completed reports of sleep difficulties at T1 and at Time 2 (T2). Path analyses revealed unique associations between anxious-withdrawal and several types of sleep difficulties (e.g., sleeping too much) at T1. Analyses also revealed a significant interaction effect between T1 anxious-withdrawal and exclusion/victimization such that anxious-withdrawal was prospectively associated with trouble sleeping only for those young adolescents who are highly excluded/victimized. Our findings are the first to link anxious-withdrawal to a physical health outcome in adolescence and point to the need for future research to not only examine anxious-withdrawal and physical health but also to include assessments of peer difficulties.
1. Introduction
While most youth desire to engage with their peers, some youth regularly withdraw behaviorally when in the company of their peers [1]. When this behavioral tendency is rooted in social anxieties and fears, it is referred to as anxious-withdrawal (closely related constructs include anxious-solitude, social withdrawal, shyness–sensitivity, e.g., [2]). Understanding anxious-withdrawal is important, because it is related to a broad range of significant psychological difficulties, including anxiety, depressive symptoms, and loneliness [3,4]. Anxious-withdrawal during childhood and adolescence is also associated with numerous peer problems, such as peer exclusion (i.e., being left out of group activities) and victimization (i.e., being subjected to repeated peer abuse), which in turn explain why many anxiously-withdrawn youth suffer psychologically [2,3].
While the negative psychological and peer concomitants of anxious-withdrawal are well-established, less is known about potential related physical health problems. In recent years, it has become clear that peer difficulties during adolescence can foster physical health problems, including numerous types of sleep difficulties (e.g., poor sleep quality [5,6,7]). In general, the majority of Americans do not get the recommended amount of daily sleep, and this is especially the case for adolescents (10–18 years) [8]. Sleep complications are significant at any age because they are related to other types of physical and psychological health difficulties (e.g., anxiety, loneliness, obesity [9,10,11]). However, during adolescence, sleep difficulties also interfere with important developmental tasks, including those in the academic domain (e.g., studying, academic performance), and thus can lead to cascading negative developmental consequences [12,13]).
Anxiously-withdrawn youth are shy and anxious; they also experience problematic peer relations [14]. These intra- and interpersonal difficulties may independently, or interactively, predict sleep difficulties, a novel hypothesis evaluated for the first time in the current investigation. Once we better understand the many different types of health difficulties associated with anxious-withdrawal, we can use this knowledge to develop strategies that help anxiously-withdrawn youth cope with their difficulties and learn to more often approach, rather than avoid, their social worlds.
1.1. Anxious-Withdrawal and Sleep
Most published studies on anxious-withdrawal (and related constructs) have not evaluated the occurrence or development of sleep difficulties. There are several relevant lines of inquiry, however, suggesting that anxious-withdrawal might be related to sleep difficulties. First, it is well-established that anxiety contributes to the development of sleep difficulties during adolescence. Of note, in the extant literature, sleep difficulties can be indexed in numerous ways, including sleeping too much, sleeping too little, talking/walking in sleep, nightmares, general trouble sleeping, sleep quality or sleep efficiency (or percent time in bed sleeping), insomnia, nighttime awakenings, and daytime sleepiness. Anxiety during adolescence has been linked to all of these indices of sleep difficulty (e.g., [5,11]). Although there is some variability across different informants, recent research indicates positive associations between both self- and parent-reports of anxiety and self- and parent-reports of sleep difficulties during adolescence [15].
When clinical samples are considered, sleep problems are found to be extremely common in youth with diagnosed anxiety disorders. For instance, approximately 88 percent of youth with anxiety disorders report at least one type of sleep difficulty, and more than half report greater than three different types of sleep difficulties [16]. In addition, clinically elevated levels of anxiety in early childhood have been found to predict insomnia in middle adulthood [17]. Anxiety is strongly linked with a variety of sleep disturbances due to the heightened physical arousal associated with anxiety as well as the rumination and biased information processing in which many anxious youth engage [7]. Of course, not all anxiously-withdrawn youth report clinically elevated levels of anxiety, but all do withdraw from their peers due to (at least small-to-moderate levels of) social anxieties and fears [18].
Second, there is growing evidence that loneliness, or dissatisfaction with and perceived inadequacy in social relationships, is associated with numerous types of sleep difficulties [19]. For instance, lonely adults report poorer sleep efficiency than do non-lonely adults, such that they experience more restless sleep and spend more time awake after sleep onset [20]. Loneliness is also associated with longer sleep latency, more nighttime awakenings, and lower perceived sleep quality during emerging adulthood [21]. Similarly, in young adults, loneliness has been robustly related to lower sleep quality [22]. Although less commonly studied with samples of adolescents, there is some indication that loneliness similarly interferes with sleep quality during adolescence [23]. Thus, at all ages, loneliness appears to “invade the nights” [20] (p. 364), likely because it promotes such negative social cognitions as hypervigilance to social threats, which keep the individual physically aroused and alert and thus unable to fall and stay asleep [19]. Although anxiously-withdrawn youth actively avoid their peers, they also very much desire to be with them, and as a result, report strong feelings of loneliness [3,24].
Third, there is some indication that social isolation leads to sleep difficulties. In this area of research, social isolation is typically indexed by self-reports of few social interactions, small network sizes, and the lack of social support [25,26]. In addition, these indices have been related positively to several types of sleep difficulties, including insomnia, longer sleep latency, and poor sleep quality [25,26,27]. For instance, in a sample of young adults, individuals who rated themselves as socially isolated reported poor sleep quality, long sleep latencies, and high levels of daytime dysfunction [28].
The evidence for links between social isolation and sleep difficulties is most robust in studies of adults. However, several recent studies have revealed associations between social isolation and sleep difficulties during adolescence [26,29]. At any age, social isolation may act as an interpersonal stressor that promotes rumination and interferes with sleep. It is also plausible that the lack of social stimulation interferes with the extent to which individuals are appropriately exhausted and ready for nighttime sleep. By definition, anxiously-withdrawn youth spend considerable time alone and on the periphery of the social scene and thus are usually also socially isolated. That said, there are many youth who are socially isolated who are not also anxiously-withdrawn (e.g., many aggressive youth).
We were not able to locate a single study in which anxious-withdrawal during adolescence was examined as it related to sleep difficulties. However, several studies have shown significant associations between shyness and sleep difficulties during adulthood (e.g., [30]). Conceptually, the constructs of shyness and anxious-withdrawal are related with the shared anxiety and fear of negative evaluation; the difference between these phenomena, however, is that not all shy individuals are socially withdrawn [1]. Nevertheless, the available evidence suggests that anxious-withdrawal may be a risk factor for sleep difficulties during adolescence. The present study is novel in the evaluation of this possibility with the consideration of six types of sleep difficulties: sleeping too much, sleeping too little, talking/walking in sleep, being overtired, nightmares, and general trouble sleeping.
1.2. The Role of Peer Difficulties
The present study also considers the possibility that peer difficulties, in the form of peer victimization and exclusion, may moderate the prospective associations between anxious-withdrawal and sleep difficulties. As noted previously, it is well-established that anxious-withdrawal is associated with and predictive of peer difficulties [31]. This is likely because anxious-withdrawn behaviors are judged to be non-normative and atypical, especially during childhood and adolescence when peer interaction and relationship involvement is expected and valued [32]. It has also been posited that anxiously-withdrawn youth are likely judged to be “easy targets” for peer victimization who are unlikely to retaliate and/or fight back [33].
To our knowledge, no past research has considered anxious-withdrawal and peer problems in relation to sleep difficulties, but peer problems alone have been linked concurrently and prospectively with sleep difficulties during adolescence [34,35,36]. Moreover, it has been found that peer victimization moderates the associations between loneliness and sleep difficulties, such that loneliness is most strongly associated with sleep difficulties for those who are highly victimized by peers [22]. In this study [22], it was suggested that peer difficulties are an interpersonal stressor that likely exacerbates the sleep difficulties associated with the individual/intrapersonal risk factors of loneliness.
Thus, in the present study, we considered not only whether anxious-withdrawal might represent an intrapersonal behavioral risk factor for sleep difficulties but also whether interpersonal difficulties with peers might enhance the risk for developing increased sleep difficulties. This suggestion seems plausible if both intra- and interpersonal difficulties conspire by increasing intrapersonal stress, rumination, and negatively biased cognitions. Furthermore, this suggested developmental process may be especially likely to occur during early adolescence (10–14 years) when getting along with peers increases in importance, rumination tendencies first begin to develop and become resistant to change, and sleep becomes increasingly disrupted [37].
1.3. The Present Study
In summary, the present study extends past research with its novel consideration of the concurrent and prospective associations between anxious-withdrawal and six types of sleep difficulties (i.e., sleeping too much, sleeping too little, talking/walking in sleep, being overtired, nightmares, and general trouble sleeping). Peer difficulties in the form of peer exclusion and victimization were also evaluated as a moderator of the prospective associations between anxious-withdrawal and sleep difficulties. Due to the dearth of research in this area, hypotheses were tentative and not specific to different types of sleep difficulties. Instead, it was generally expected that anxious-withdrawal would be related significantly to sleep difficulties (Hypothesis #1) and that anxious-withdrawal in combination with peer exclusion and victimization would predict increases in sleep difficulties over time (Hypothesis #2). To evaluate these hypotheses, we utilized a longitudinal sample of young adolescents and multi-method assessments (maternal-reports of sleep, peer nominations of anxious-withdrawal and peer exclusion and victimization).
2. Materials and Methods
2.1. Participants and Procedures
Participants were 395 (Mage = 13.61 years (SD = 0.54) at the start of the study; 139 boys, Mage = 13.67 years (SD = 0.52); 256 girls, Mage = 13.56 years (SD = 0.55)) young adolescents in the Greater Washington, DC metropolitan area selected from a larger longitudinal project on peer relationships (see [14,33]). These participants (and their mothers) completed measures in Grade 5 and/or Grade 6 and also when they were in Grade 8 (described in more detail below). The sample was racially diverse, with 35% belonging to a racial or ethnic minority group (with 11% African American, 17% Asian, and 5% Hispanic/Latino). In terms of parental education, 66% of the participants’ mothers (59% of the fathers) had an undergraduate or advanced graduate university degree, 19% had some college education (12% of the fathers), and 6% had high school or vocational education (12% of the fathers). Comparisons of participants who were included in this study versus those who were not included from the larger project did not reveal any significant differences in the study variables (output available by request).
In the larger project, principals of public elementary and middle schools were first contacted and agreed to participate in the study, and then all students in their schools were invited to participate. Youth with signed parental consent and adolescent assent forms then completed paper-and-pencil peer nomination measures in their schools during the spring of Grade 5 (the final year of elementary school) and/or Grade 6 (the first year of middle school; 70% consent rate; University of Maryland, Institutional Review Board #00475). All participating Grade 5 and 6 youth and their parents (392/395 or 99% of these parents were mothers) were next invited to complete additional measures in the laboratory (where they provided additional signed parent consent and adolescent assent).
The school and laboratory measures collected during Grade 5/Grade 6 are referred to as occurring at Time 1 (T1). Most (75% of the sample) of the T1 data were collected from participants and their mothers when the participants were in Grade 6. There were no significant grade (Grade 5 versus Grade 6) differences, however, in any of the T1 study variables (ps > 0.12). Also of note, when participants completed school and laboratory measures in both Grades 5 and 6, only their Grade 6 data were used. Participants and their parents also completed measures in the laboratory or at home when they were in Grade 8 (Time 2; T2; the final year of middle school). In addition to the measures described next, participants completed additional measures, such as a nomination measure of friendship at the T1 school visits and a social information processing measure at the T1 laboratory visits; these were not of interest in this investigation. Participants received gift cards for completing the laboratory measures at each time point.
2.2. Measures
2.2.1. School Measures (T1)
Anxious-withdrawal and peer exclusion/victimization. Participants (and their classmates) completed a 30-item peer nomination measure that included four items descriptive of anxious-withdrawal (e.g., “very shy”, “gets nervous about participating in group discussions” [14,33]). Four items descriptive of peer victimization and exclusion were also included (e.g., “gets hit/kicked”, “left out of group activities”). In Grade 5, participants selected one same- and one other-sex peer from their classroom and grade who were most like these items from rosters; in Grade 6, due to school schedules that involved numerous classroom changes throughout the day, participants wrote names for up to three same- and other-sex grade-mates without a roster. Self-nominations were permitted but not considered. For each item, the nominations received were summed, proportionalized, and then standardized within sex and school (to adjust for differences across schools in the number of possible nominations received [38]). Mean scores were calculated with higher scores reflecting greater anxious-withdrawal (α = 0.84) and peer exclusion/victimization (α = 0.90). Previous psychometric work with the Grade 5 and Grade 6 peer nomination data revealed identical and separate anxious-withdrawal and peer exclusion/victimization factors in each grade [14].
2.2.2. Laboratory Measures (T1, T2)
Sleep problems. Sleep problems at T1 and T2 were measured with the same six items drawn from the parent-reported Child Behavior Checklist (CBCL; [39]) (“nightmares”, “sleep less than most kids”, “sleep more than most kids”, “talks/walks in sleep”, “overtired”, “trouble sleeping”; for other published studies of 6-to-17-year-old youth that utilized the CBCL to assess sleep, see [15]). At both time points, items were scored on a three-point scale (ranging from 0 = not true to 2 = very/often true). Items were analyzed individually rather than with composite/mean scores due to poor internal consistencies at each time point (αs < 0.50). Self-reports of five of these sleep difficulties (“nightmares”, “sleep less than most kids”, “sleep more than most kids”, “overtired”, “trouble sleeping”; with the Youth Self-Report; YSR [40]) were also available, but at T2 only. Therefore, primary models utilized the CBCL data, but an exploratory model was also evaluated with the T2 YSR self-report data utilized.
2.3. Data Analysis
Means and standard deviations for, and zero-order correlations among, the study variables were first examined and are presented in Table 1. To evaluate the primary study objective and hypotheses, Mplus version 6.12 [41] was used to estimate a path model with full information maximum likelihood estimation with robust standard errors. Missing data were minimal, and full information maximum likelihood estimation is appropriate to handle missing data. The path model is depicted in Figure 1 with the main effect from anxious-withdrawal to sleep difficulties included as a test of Hypothesis #1. The stability paths (from T1 to T2) between the sleep variables were also estimated, as were the paths from the interaction term between the centered T1 anxious-withdrawal and exclusion/victimization variables and the T2 sleep problem variables (with the interaction effect included to test Hypothesis #2). Although not shown in the figure, covariances between exogenous variables (each T1 maternal-reported sleep problem variable, T1 anxious-withdrawal, T1 exclusion/victimization) were estimated, as were the covariances between the endogenous variables (each T2 maternal-reported sleep problem variable). Model fit was assessed with chi-square goodness-of-fit and the root-mean-square error of approximation (RMSEA; 0.08 or less), standardized root-mean-square residual (SRMR; 0.09 or less), and comparative fit index (CFI; 0.95 or greater). Only significant effects are described.
3. Results
3.1. Preliminary Analyses
In the correlational analyses, anxious-withdrawal at T1 was related positively to T1 exclusion/victimization, T1 maternal-reports of nightmares, T1 and T2 maternal-reports of sleeping more than other kids, and T1 and T2 maternal-reports of trouble sleeping. A series of exploratory t-tests did not reveal any significant sex differences in any of the study variables (ps > 0.05).
3.2. Primary Analyses
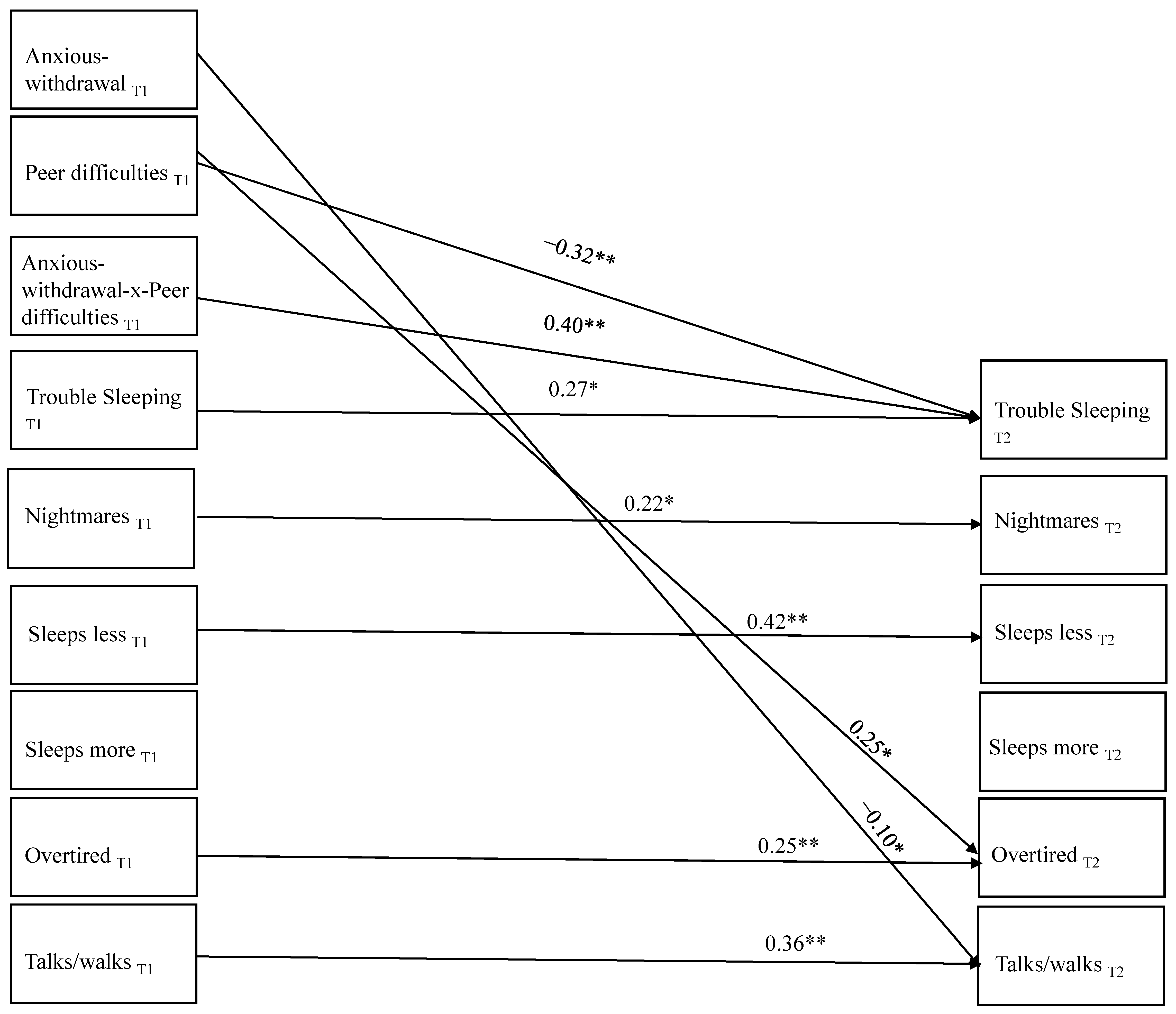
There was a good fit of the model to the data: χ2 (30) = 40.50, p = 0.096, RMSEA = 0.03, 90% CI [0.000, 0.051], SRMR = 0.048, CFI = 0.94; thus, no post hoc model fitting was performed. As is evident in Figure 2, significant stability was found over time for each type of sleep problem, with the exception of reports of sleeping more than other kids. In terms of additional prospective associations, T1 exclusion/victimization predicted increases in maternal-reports of being overtired and decreases in trouble sleeping over time. T1 anxious-withdrawal predicted decreases in maternal-reports of talking/walking in sleep from T1 to T2. In addition, the interaction between T1 anxious-withdrawal and T1 exclusion/victimization when predicting T2 maternal-reports of trouble sleeping was significant. Simple slope analyses showed that T1 anxious-withdrawal predicted increases in maternal-reports of trouble sleeping (β = 0.34, p = 0.001) at high levels of T1 exclusion/victimization but not at low levels (β = −0.15, p = 0.18).
Not shown in the figure for ease of communication were numerous unique within-time significant associations. For example, T1 anxious-withdrawal and T1 victimization/exclusion were significantly related (β = 0.31, p = 0.001). T1 anxious-withdrawal was also related uniquely to T1 maternal-reports of sleeping more than other kids (β = 0.16, p = 0.02) and trouble sleeping (β = 0.18, p = 0.01). T1 exclusion/victimization was associated uniquely with T1 maternal-reports of trouble sleeping (β = 0.16, p = 0.05) but was not related significantly with any other types of sleep difficulties at T1.
Within-time unique associations among the sleep difficulties also emerged. At T1, maternal-reports of nightmares were related uniquely to maternal reports of being overtired (β = 0.12, p = 0.04), sleeping less than other kids (β = 0.11, p = 0.05), sleeping more than other kids (β = 0.13, p = 0.04), talking/walking in sleep (β = 0.17, p = 0.007), and trouble sleeping (β = 0.29, p = 0.001). At T1, maternal-reports of sleeping less than other kids were also correlated with maternal-reports of being overtired (β = 0.26, p = 0.001), and maternal-reports of trouble sleeping were associated uniquely with maternal-reports of being overtired (β = 0.21, p = 0.004), sleeping less than other kids (β = 0.31, p = 0.004), and talking in sleep (β = 0.18, p = 0.03).
At T2, maternal-reports of nightmares were associated uniquely with maternal-reports of being overtired (β = 0.23, p = 0.044), talking/walking in sleep (β = 0.27, p = 0.01), and trouble sleeping (β = 0.31, p = 0.003). T2 maternal-reports of sleeping less than other kids were also related uniquely to maternal-reports of being overtired (β = 0.19, p = 0.037) and so were maternal-reports of sleeping more than other kids (β = 0.40, p = 0.001). T2 maternal-reports of sleeping less than other kids, however, were also related uniquely and negatively with T2 maternal-reports of talking/walking in sleep. Finally, T2 maternal-reports of trouble sleeping were associated uniquely with maternal-reports of being overtired (β = 0.43, p = 0.001) and sleeping less than other kids (β = 0.33, p = 0.006).
3.3. Exploratory Analyses
3.3.1. Evaluation of Sex Differences
We next explored, without any a priori predictions, whether sex moderated the proposed associations with a multiple group analysis in which a fully unconstrained model (all paths and covariances freely estimated for both sexes) was compared to a fully constrained model (all regression paths and covariances set equal for both sexes). A significant χ2 difference test between the constrained and free-to-vary models indicated no differences across sex, Δχ2 (37) = 46.406, p = 0.13.
3.3.2. Youth Self-Reports of Sleep Difficulties
We then evaluated the fit of an exploratory model identical to the primary model with one notable difference: T2 sleep variables were reported by the adolescent. Adolescent self-reported sleep data were not available at T1, and so we controlled for T1 maternal-reports in these models. There was one other difference: the YSR does not ask youth about the extent to which they are talking/walking in their sleep, and so this model included five (as opposed to six) T1 and T2 sleep variables. Table 2 shows the zero-order correlations between the study variables included in this model.
There was adequate fit to the data for this model: χ2 (20) = 40.77, p = 0.004, RMSEA = 0.05, 90% CI [0.028, 0.074], SRMR = 0.047, CFI =0.85, and no post hoc model fitting was performed. Of note, in this model, maternal-reports of nightmares at T1 predictively positively self-reports of nightmares at T2 (β = 0.19, p = 0.03). Similar prospective effects were found for T1 maternal-reports of trouble sleeping and T2 self-reports of trouble sleeping (β = 0.18, p = 0.02). Surprisingly, T1 maternal-reports of sleeping more than other kids were related negatively to T2 self-reports of sleeping more than other kids (β = −0.12, p = 0.04).
In terms of main effects, T1 exclusion/victimization was related positively to T2 self-reports of nightmares (β = 0.26, p = 0.02). Moreover, the interaction between T1 anxious-withdrawal and T1 exclusion/victimization significantly predicted T2 trouble sleeping (β = −0.19, p = 0.02). Simple slope analyses revealed that T1 anxious-withdrawal was a negative predictor of T2 trouble sleeping at high levels of peer exclusion/victimization (β = −0.18, p = 0.051) but was not a significant predictor at low levels of peer exclusion/victimization (β = 0.045, p = 0.36).
4. Discussion
Anxious-withdrawal during childhood and adolescence has been associated concurrently and prospectively with a host of psychological difficulties, including anxiety, depressive symptoms, and loneliness [1]. There is also evidence that anxiously-withdrawn behaviors interfere with positive peer interactions and relationships and instead promote such negative peer difficulties as peer exclusion and peer victimization [31]. However, researchers have yet to investigate whether anxiously-withdrawn behavioral tendencies also place youth at risk for physical health difficulties. The present study aimed to extend previous research by examining, for the first time, whether anxious-withdrawal during early adolescence is related concurrently and prospectively with six different types of sleep problems (nightmares, talking/walking in sleep, sleeping more than other kids, sleeping less than other kids, being overtired, and general trouble sleeping), as well as whether peer difficulties (in the form of peer victimization and exclusion) moderate these associations.
Consistent with expectations (Hypothesis #1), peer-nominated anxious-withdrawal was associated concurrently with several types of maternal-reported sleep problems, including nightmares and sleeping too much, in the zero-order correlational analyses. In path models, anxious-withdrawal was also related uniquely to T1 maternal-reports of sleeping more than other kids and trouble sleeping. Taken together, these findings suggest, for the first time, that adolescents who regularly withdraw from their peers due to social fears and anxieties during the daytime hours also experience difficulties in the nighttime. Although these findings will require replication, they may point to the need for a “24-h approach” in future research to fully understand the multitude of health difficulties associated with anxious-withdrawal. Such approaches, which track social interaction and activities continuously for 24 h, are becoming increasingly common in other areas of developmental and clinical psychology research (e.g., obesity research [42], personality disorder research [43]) but have not yet been utilized in studies of anxious-withdrawal. In fact, most studies of anxious-withdrawal not only neglect functioning and well-being during the nighttime hours but also neglect how anxiously-withdrawn youth fare when they are awake and not in school (or before and after school hours).
Young adolescents who are anxiously-withdrawn may experience sleep difficulties due to their nervous and negatively-biased social information processing and cognition tendencies (e.g., rejection-sensitivity, internal blame attributions [44]). Similar to those who are anxious as well as lonely and socially isolated, these negative cognitive styles may interfere with several aspects of the sleep process, such as falling asleep at the start of bedtime. Significantly, the findings from this study suggest that anxious-withdrawal may be related to some, but not all, types of sleep difficulties. As one example, anxious-withdrawal at T1 was related uniquely to T1 sleeping more than other kids and having trouble sleeping; anxious-withdrawal was not associated with T1 reports of sleeping less than other kids and talking/walking in sleep. This may point to the possibility that anxiously-withdrawn young adolescents struggle most with initially falling asleep and not staying asleep. Additional work with more nuanced assessments of sleep (e.g., physiological assessments of sleep), however, is needed to evaluate this hypothesis.
As shown in previous research, peer-nominated peer victimization and exclusion in this study was related concurrently to several types of sleep problems, including being overtired. Novel to this research, however, was the prospective and interactive effect of anxious-withdrawal and these peer problems on reports of trouble sleeping. Specifically, and consistent with Hypothesis #2, the results showed that anxious-withdrawal at T1 predicted increased maternal-reports of trouble sleeping at T2 for young adolescents who were highly excluded and victimized by their peers at school. The longitudinal relation between anxious-withdrawal and trouble sleeping was not significant for young adolescents who were low in peer victimization and exclusion. It is possible that these findings reflect increased worry, anxieties, and negative social cognitions experienced by anxiously-withdrawn young adolescents who also struggle in their relationships with their peers [45]. It seems that such cognitions and affect may, in turn, interfere with sleep. Past research has shown that youth with the intrapersonal risk factor of anxious-withdrawal suffer the most psychologically when they also struggle interpersonally with their peers [2,3,45]. The present findings, however, are the first to show similar intra- and interpersonal interactive effects as they pertain to a physical health outcome. The findings of the present study may suggest that anxiously-withdrawn young adolescents might benefit from explicit instruction on sleep hygiene. Peer problems can be difficult to change, especially without school-wide intervention efforts, but there is growing evidence to support the efficacy of cognitive–behavioral sleep interventions for not only adults but also adolescents [46,47,48]. Such therapies might not solve anxiously-withdrawn adolescents’ psychological and peer difficulties, but they might help them to be better rested when dealing with them.
Several limitations of this study should be acknowledged. First, even with longitudinal analyses, the present study does not provide evidence about causality. In addition, the conceptualization and analyses for our study were informed by other areas of research which assume that individual risk factors (e.g., anxiety) lead to the development of sleep difficulties over time [49,50]. However, it is certainly plausible that sleep difficulties, and the daytime exhaustion related to many of them, might lead some youth to not have the energy and positive affect necessary to engage with peers. Such direction of effects could not be examined in this study but should be evaluated in future research.
Second, the present study focused on peer victimization and exclusion, the two most commonly considered types of peer difficulties in research on anxious-withdrawal [31]. Although oftentimes discussed as conclusive, the evidence linking anxious-withdrawal and peer rejection (or active dislike) is actually quite mixed, especially in the few studies published on anxious-withdrawal and peer rejection with adolescent samples [31]. Nevertheless, future research on anxious-withdrawal and sleep should explore the potential contributions of peer rejection and other types of peer difficulties, including those involving friends (e.g., friendship instability, dissolution, and betrayal), which may also increase anxiously-withdrawn young adolescents’ distress and interfere with their sleep. In such research, measures of anxiety and negative cognitions should also be included to evaluate the proposed mechanisms of influence in this study [50,51]. The lack of such assessments in this study is another significant limitation.
Third, this study was further limited by its reliance on maternal-reports of sleep difficulties. We did explore self-reports of sleep difficulties at T2, but we are cautious to interpret such findings given the lack of T1 self-reports of sleep difficulties. That said, the results did differ somewhat from those with the maternal-reports of sleep difficulties, which we think may point to the importance of multiple informants in future research in this area of research [52,53]. Perhaps multiple informant assessments might help make sense of several unexpected findings found in this study, such as why T1 exclusion/victimization predicted decreases in maternal-reports of trouble sleeping over time and T1 anxious-withdrawal predicted decreases in maternal-reports of talking/walking in sleep from T1 to T2; these effects were also not found when T2 self-reports of sleep difficulties were considered.
5. Conclusions
Despite these limitations, the present study extends past research with its consideration of anxious-withdrawal in relation to physical health difficulty. The findings linking anxious-withdrawal concurrently and prospectively to sleep difficulties are novel and should set the stage for future research on anxious-withdrawal that conceptualizes adjustment difficulties more broadly to include physical health difficulties. Also noteworthy was the interaction effect between anxious-withdrawal and peer exclusion/victimization in the prediction of trouble sleeping. This result is the first to show that anxiously-withdrawn young adolescents’ peer difficulties contribute to physical heath difficulties (just as they contribute to their social and psychological health difficulties). Thus, we hope this latter finding helps to further highlight the importance of considering peer difficulties in the study of anxious-withdrawal, and perhaps after replication, informs intervention and prevention efforts with youth who regularly withdraw from their peers due to social fears and anxieties.
Author Contributions
Conceptualization: J.C.B., J.N.G., C.L.R. and K.H.R.; methodology: J.C.B. and K.H.R.; software: J.C.B.; analysis: J.C.B. and J.N.G.; writing—original draft: J.C.B., J.N.G., C.L.R. and K.H.R.; writing—reviewing and editing: J.C.B., J.N.G., C.L.R. and K.H.R.; project administration: J.C.B. and K.H.R.; funding acquisition: K.H.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by National Institute of Mental Health Grant 1R01MH58116 to Kenneth H. Rubin.
Institutional Review Board Statement
All participants and their parents gave their signed informed consent before they participated in this study. This study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Institutional Review Board at the University of Maryland (#00475).
Informed Consent Statement
Written informed consent was obtained from all participants and their parents involved in the study.
Data Availability Statement
De-identified data and code will be made available upon reasonable request to the first author.
Acknowledgments
The authors graciously acknowledge and thank the adolescents and their families who participated in this study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Rubin, K.H.; Chronis-Tuscano, A. Perspectives on social withdrawal in childhood: Past, present, and prospects. Child Dev. Perspect. 2021, 15, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Gazelle, H.; Ladd, G.W. Anxious solitude and peer exclusion: A diathesis-stress model of internalizing trajectories in childhood. Child Dev. 2003, 74, 257–278. [Google Scholar] [CrossRef] [PubMed]
- Boivin, M.; Hymel, S.; Bukowski, W.M. The roles of social withdrawal, peer rejection, and victimization by peers in predicting loneliness and depressed mood in childhood. Dev. Psychopathol. 1995, 7, 765–785. [Google Scholar] [CrossRef]
- Rubin, K.H.; Chen, X.; McDougall, P.; Bowker, A.; McKinnon, J. The Waterloo Longitudinal Project: Predicting adolescent internalizing and externalizing problems from early and mid-childhood. Dev. Psychopathol. 1995, 7, 751–764. [Google Scholar] [CrossRef]
- Alfano, C.A.; Zakem, A.H.; Costa, N.M.; Taylor, L.K.; Weems, C.F. Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depress. Anxiety 2009, 26, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.J.; Zeringue, M.M.; El-Sheikh, M. Adolescents’ sleep and adjustment: Reciprocal effects. Child Dev. 2021, 93, 540–555. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.A.; Oosterhoff, B.; Bower, J.L.; Kaplow, J.B.; Alfano, C.A. Associations among adolescent sleep problems, emotion regulation, and affective disorders: Findings from a nationally representative sample. J. Psychiatr. Res. 2018, 96, 1–8. [Google Scholar] [CrossRef]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth risk behavior surveillance—United States, 2017. MMWR Surveill. Summ. 2018, 67, 1–114. [Google Scholar] [CrossRef]
- Dikeos, D.; Georgantopoulos, G. Medical comorbidity of sleep disorders. Curr. Opin. Psychiatry 2011, 24, 346–354. [Google Scholar] [CrossRef]
- Freeman, D.; Sheaves, B.; Waite, F.; Harvey, A.G.; Harrison, P.J. Sleep disturbance and psychiatric disorders. Lancet Psychiatry 2020, 7, 628–637. [Google Scholar] [CrossRef]
- Orchard, F.; Gregory, A.M.; Gradisar, M.; Reynolds, S. Self-reported sleep patterns and quality amongst adolescents: Cross-sectional and prospective associations with anxiety and depression. J. Child Psychol. Psychiatry 2020, 61, 1126–1137. [Google Scholar] [CrossRef]
- Berger, R.H.; Diaz, A.; Valiente, C.; Eisenberg, N.; Sprinrad, T.L.; Thompson, M.S.; Hernandez, M.M.; VanSchyndel, S.K.; Southworth, J. Sleep duration moderates the association between children’s temperament and academic achievement. Early Educ. Dev. 2018, 29, 624–640. [Google Scholar] [CrossRef] [PubMed]
- Simola, P.; Liukkonen, K.; Pitkaranta, A.; Pirinen, T.; Aronen, E.T. Psychosocial and somatic outcomes of sleep problems in children: A 4-year follow-up study. Child Care Health Dev. 2012, 40, 60–67. [Google Scholar] [CrossRef]
- Oh, W.; Rubin, K.H.; Bowker, J.C.; Booth-LaForce, C.L.; Rose-Krasnor, L.; Laursen, B. Trajectories of social withdrawal from middle childhood to early adolescence. J. Abnorm. Child Psychol. 2008, 36, 553–556. [Google Scholar] [CrossRef]
- Lamoureux, V.A.; Glenn, A.L.; Ling, S.; Raine, A.; Ang, R.P.; Fung, D. The role of anxiety and callous-unemotional traits in the relationship between externalizing behaviors and sleep problems in clinic-referred youth. Clin. Child Psychol. Psychiatry 2023, 28, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.A.; Ginsburg, G.S.; Kingery, J.N. Sleep-related problems among children and adolescents with anxiety disorder. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 224–232. [Google Scholar] [CrossRef]
- McMakin, D.L.; Alfano, C.A. Sleep and anxiety in late childhood and early adolescence. Curr. Opin. Psychiatry 2015, 28, 483–489. [Google Scholar] [CrossRef]
- Gazelle, H.; Workman, J.O.; Allan, W. Anxious solitude and clinical disorder in middle childhood: Bridging developmental and clinical approaches to childhood social anxiety. J. Abnorm. Child Psychol. 2010, 38, 1–17. [Google Scholar] [CrossRef]
- Hom, M.A.; Chu, C.; Rogers, M.L.; Joiner, T.E. A meta-analysis of the relationship between sleep problems and loneliness. Clin. Psychol. Sci. 2020, 8, 799–824. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C.; Berntson, G.G.; Ernst, J.M.; Gibbs, A.C.; Stickgold, R.; Hobson, J.A. Do lonely days invade the nights? Potential social modulation of sleep efficiency. Psychol. Sci. 2002, 13, 384–387. [Google Scholar] [CrossRef]
- Peng, A.; Tang, Y.; He, S.; Ji, S.; Dong, B.; Chen, L. Association between loneliness, sleep behavior and quality: A propensity-score-matched case-control study. Sleep Med. 2021, 86, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Matthews, T.; Danese, A.; Gregory, A.M.; Caspi, A.; Moffitt, T.E.; Arseneault, L. Sleeping with one eye open: Loneliness and sleep quality in young adults. Psychol. Med. 2017, 47, 2177–2186. [Google Scholar] [CrossRef] [PubMed]
- Eccles, A.M.; Qualter, P.; Madsen, K.R.; Holstein, B.E. Loneliness in the lives of Danish adolescents: Associations with health and sleep. Scand. J. Public Health 2020, 48, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Markovic, A.; Bowker, J.C. Friends also matter: Examining friendship adjustment indices as moderators of anxious-withdrawal and trajectories of change in psychological maladjustment. Dev. Psychol. 2017, 53, 1462. [Google Scholar] [CrossRef] [PubMed]
- Azizi-Zeinalhajlou, A.; Mirghafourvand, M.; Nadrian, H.; Sis, S.S.; Matlabi, H. The contribution of social isolation and loneliness to sleep disturbances among older adults: A systematic review. Sleep Biol. Rhythm. 2022, 20, 153–163. [Google Scholar] [CrossRef]
- Richardson, C.; Oar, E.; Fardouly, J.; Magson, N.; Johnco, C.; Forbes, M.; Rapee, R. The moderating role of sleep in the relationship between social isolation and internalising problems in adolescence. Child Psychiatry Hum. Dev. 2019, 50, 1011–1020. [Google Scholar] [CrossRef]
- Pilcher, J.J.; Dorsey, L.L.; Galloway, S.M.; Erikson, D.N. Social isolation and sleep: Manifestation during COVID-19 quarantines. Front. Psychol. 2022, 12, 6476. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C. Social isolation and health, with an emphasis on underlying mechanisms. Perspect. Biol. Med. 2003, 46, S39–S52. [Google Scholar] [CrossRef]
- Palmer, C.A.; Powell, S.L.; Deutchman, D.R.; Tintzman, C.; Poppler, A.; Oosterhoff, B. Sleepy and secluded: Sleep disturbances are associated with connectedness in early adolescent social networks. J. Res. Adolesc. 2022, 32, 756–768. [Google Scholar] [CrossRef]
- Weissbluth, M. Sleep-loss stress and temperamental difficultness: Psychobiological processes and practical considerations. In Temperament in Childhood; Kohnstamm, G.A., Bates, J.E., Rothbart, M.K., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 1989; pp. 357–375. [Google Scholar]
- Bowker, J.C.; White, H.I. Studying peers in research on social withdrawal: Why broader assessments of peers are needed. Child Dev. Perspect. 2021, 15, 90–95. [Google Scholar] [CrossRef]
- Bowker, J.C.; Ooi, L.L.; Coplan, R.J.; Etkin, R.G. When is it okay to be alone? Gender differences in normative beliefs about social withdrawal in emerging adulthood. Sex Roles 2020, 82, 482–492. [Google Scholar] [CrossRef]
- Rubin, K.H.; Wojslawowicz, J.C.; Rose-Krasnor, L.; Booth-LaForce, C.; Burgess, K.B. The best friendships of shy/withdrawn children: Prevalence, stability, and relationship quality. J. Abnorm. Child Psychol. 2006, 34, 139–153. [Google Scholar] [CrossRef] [PubMed]
- De Lise, F.; Bacaro, V.; Crocetti, E. The social side of sleep: A systematic review of the longitudinal associations between peer relationships and sleep quality. Int. J. Environ. Res. Public Health 2023, 20, 2017. [Google Scholar] [CrossRef] [PubMed]
- Tu, K.M.; Spencer, C.W.; El-Sheikh, M.; Erath, S.A. Peer victimization predicts sleep problems in early adolescence. J. Early Adolesc. 2019, 39, 67–80. [Google Scholar] [CrossRef]
- Van Geel, M.; Goemans, A.; Vedder, P.H. The relation between peer victimization and sleeping problems: A meta-analysis. Sleep Med. Rev. 2016, 27, 89–95. [Google Scholar] [CrossRef]
- LaFontana, K.M.; Cillessen, A.H. Developmental changes in the priority of perceived status in childhood and adolescence. Soc. Dev. 2010, 19, 130–147. [Google Scholar] [CrossRef]
- Cillessen, A.H.N. Sociometric methods. In Handbook of Peer Interactions, Relationships, and Groups; Rubin, K.H., Bukowski, W.M., Laursen, B., Eds.; The Guilford Press: New York, NY, USA, 2009; pp. 82–99. [Google Scholar]
- Achenbach, T.M. Manual for Child Behavior Checklist/4–18 and 1991 Profile; University of Vermont Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 6th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2010. [Google Scholar]
- Rosenberger, M.E.; Fulton, J.E.; Buman, M.P.; Troiano, R.P.; Grandner, M.A.; Buchner, D.M.; Haskell, W.L. The 24-hour activity cycle: A new paradigm for physical activity. Med. Sci. Sports Exerc. 2019, 51, 454. [Google Scholar] [CrossRef]
- McGowan, N.M.; Saunders, K.E. The emerging circadian phenotype of borderline personality disorder: Mechanisms, opportunities and future directions. Curr. Psychiatry Rep. 2021, 23, 30. [Google Scholar] [CrossRef]
- Kingsbury, M.; Coplan, R.J.; Rose-Krasnor, L. Shy but getting by? An examination of the complex links among shyness, coping, and socioemotional functioning in childhood. Soc. Dev. 2013, 22, 126–145. [Google Scholar] [CrossRef]
- Gazelle, H.; Rudolph, K.D. Moving toward and away from the world: Social approach and avoidance trajectories in anxious solitary youth. Child Dev. 2004, 75, 829–849. [Google Scholar] [CrossRef]
- Blake, M.J.; Sheeber, L.B.; Youssef, G.J.; Raniti, M.B.; Allen, N.B. Systematic review and meta-analysis of adolescent cognitive–behavioral sleep interventions. Clin. Child Fam. Psychol. Rev. 2017, 20, 227–249. [Google Scholar] [CrossRef]
- Hendricks, M.C.; Ward, C.M.; Grodin, L.K.; Slifer, K.J. Multicomponent cognitive-behavioural intervention to improve sleep in adolescents: A multiple baseline design. Behav. Cogn. Psychother. 2014, 42, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Kodsi, A.; Bullock, B.; Kennedy, G.A.; Tirlea, L. Psychological interventions to improve sleep in young adults: A systematic review and meta-analysis of randomized controlled trials. Behav. Sleep Med. 2022, 20, 125–142. [Google Scholar] [CrossRef]
- Nguyen, V.V.; Zainal, N.H.; Newman, M.G. Why sleep is key: Poor sleep quality is a mechanism for the bidirectional relationship between major depressive disorder and generalized anxiety disorder across 18 years. J. Anxiety Disord. 2022, 90, 102601. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Sznajder, K.; Cui, C.; Yang, Y.; Li, Y.; Yang, X. Anxiety and its relationship with sleep disturbance and problematic smartphone use among Chinese medical students during COVID-19 home confinement—A structural equation model analysis. J. Affect. Disord. 2022, 296, 315–321. [Google Scholar] [CrossRef]
- Chellappa, S.L.; Aeschbach, D. Sleep and anxiety: From mechanisms to interventions. Sleep Med. Rev. 2022, 61, 101583. [Google Scholar] [CrossRef]
- Kim, H.; Kim, S.H.; Jang, S.I.; Park, E.C. Association between sleep quality and anxiety in Korean adolescents. J. Prev. Med. Public Health 2022, 55, 173. [Google Scholar] [CrossRef]
- Chen, Y.; Zhu, J. Longitudinal associations between cybervictimization and adolescent sleep problems: The role of anxiety and depressive symptoms. J. Interpers. Violence 2023, 38, 2806–2827. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Model Evaluated in the Primary Analyses Predicting Time 2 Sleep Difficulties.
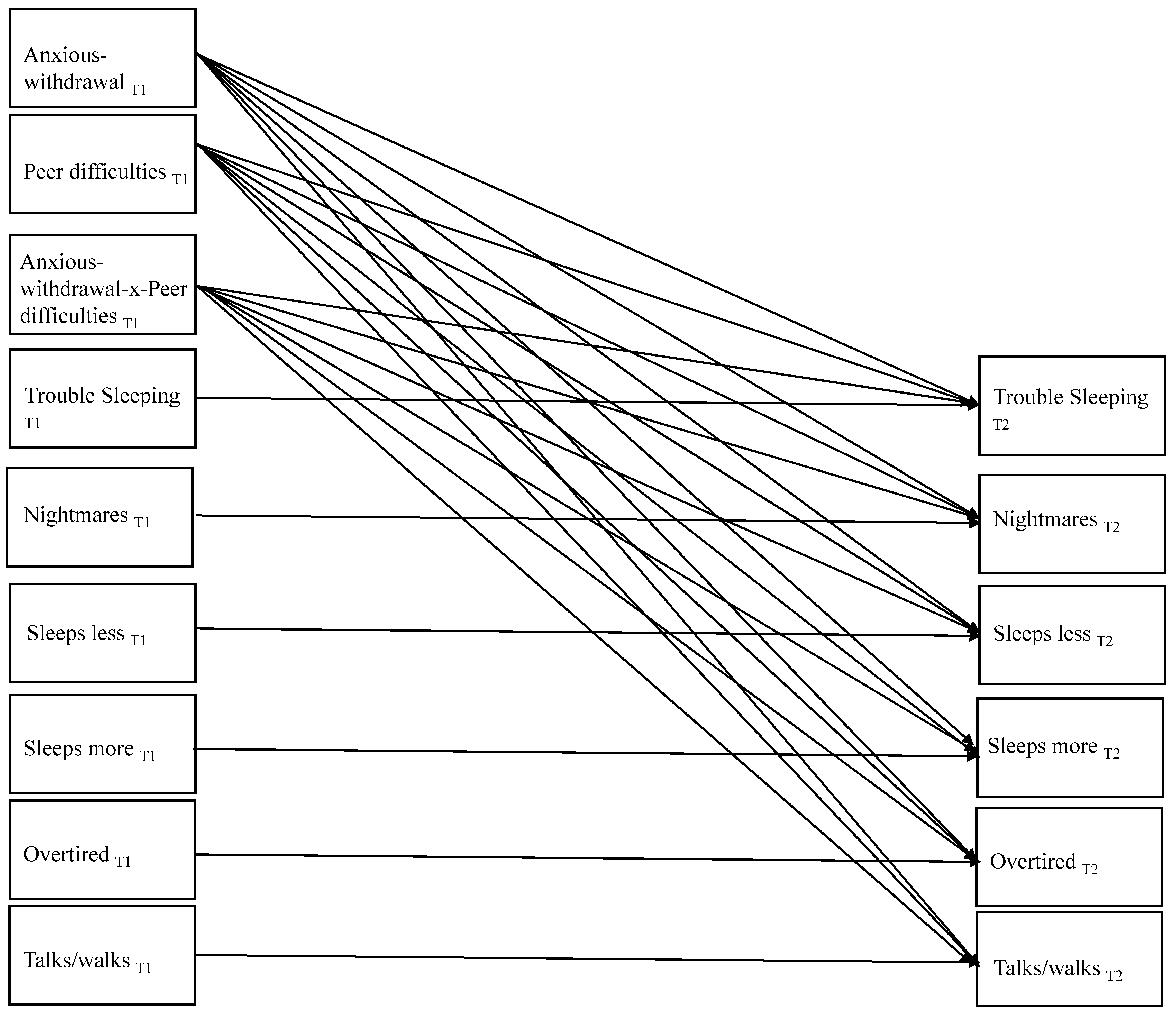
Figure 2.
Significant Paths in the Primary Model Predicting Time 2 Sleep Difficulties; * p < 0.05, ** p < 0.001.
Figure 2.
Significant Paths in the Primary Model Predicting Time 2 Sleep Difficulties; * p < 0.05, ** p < 0.001.

{kind=link}
{kind=link}
Table 1.
Zero-order Correlations and Descriptive Statistics.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Anxious-withdrawal T1 | ||||||||||||||
| 2. Exclusion/Victimization T1 | 0.320 ** | |||||||||||||
| 3. Nightmares T1 | 0.122 * | 0.127 * | ||||||||||||
| 4. Overtired T1 | 0.101 | 0.071 | 0.119 * | |||||||||||
| 5. Sleeps less T1 | 0.039 | 0.037 | 0.112 * | 0.262 ** | ||||||||||
| 6. Sleeps more T1 | 0.175 ** | 0.055 | 0.134 ** | 0.104 * | 0.013 | |||||||||
| 7. Talks/walks T1 | −0.052 | −0.054 | 0.173 ** | 0.034 | −0.005 | 0.082 | ||||||||
| 8. Trouble sleeping T1 | 0.198 ** | 0.175 ** | 0.288 ** | 0.210 ** | 0.301 ** | 0.08 | 0.181 ** | |||||||
| 9. Nightmares T2 | 0.089 | 0.068 | 0.244 ** | 0.057 | −0.059 | 0.004 | 0.186 * | 0.053 | ||||||
| 10. Overtired T2 | 0.1 | 0.275 ** | 0.232 ** | 0.300 ** | 0.15 | 0.097 | 0.021 | 0.212 ** | 0.261 ** | |||||
| 11. Sleeps less T2 | 0.008 | 0.008 | 0.015 | 0.007 | 0.436 ** | 0.026 | −0.074 | 0.128 | 0.036 | 0.187 * | ||||
| 12. Sleeps more T2 | 0.194 * | 0.081 | 0.023 | −0.002 | 0.048 | 0.202 ** | 0.018 | 0.245 ** | 0.066 | 0.388 ** | 0.272 ** | |||
| 13. Talks/walks T2 | −0.145 | −0.115 | 0.011 | −0.006 | −0.055 | 0.008 | 0.433 ** | −0.028 | 0.297 ** | 0.054 | −0.142 | 0.071 | ||
| 14. Trouble sleeping T2 | 0.225 * | 0.247 ** | 0.178 * | 0.208 ** | 0.222 ** | 0.15 | 0.074 | 0.374 ** | 0.311 ** | 0.451 ** | 0.307 ** | 0.163 * | −0.019 | |
| M | −0.016 | −0.005 | 0.168 | 0.223 | 0.168 | 0.097 | 0.112 | 0.125 | 0.138 | 0.204 | 0.174 | 0.078 | 0.133 | 0.156 |
| SD | 0.837 | 0.605 | 0.381 | 0.463 | 0.425 | 0.344 | 0.34 | 0.394 | 0.379 | 0.446 | 0.439 | 0.29 | 0.374 | 0.38 |
Note. Sleep variables were mother-reported, anxious-withdrawal and victimization/exclusion were based on peer nominations; T1 = Time 1 or Grade 5/6; T2 = Time 2 or Grade 8; * p < 0.05; ** p < 0.001.
Table 2.
Zero-order Correlations and Descriptive Statistics for Maternal-reported (T1) and Self-reported (T2) Sleep Difficulties.
Table 2.
Zero-order Correlations and Descriptive Statistics for Maternal-reported (T1) and Self-reported (T2) Sleep Difficulties.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Anxious-withdrawal T1 | ||||||||||||
| 2. Exclusion/Victimization T1 | 0.320 ** | |||||||||||
| 3. Nightmares T1 | 0.122 * | 0.127 * | ||||||||||
| 4. Overtired T1 | 0.101 | 0.071 | 0.119 * | |||||||||
| 5. Sleeps less T1 | 0.039 | 0.037 | 0.112 * | 0.262 * | ||||||||
| 6. Sleeps more T1 | 0.175 ** | 0.055 | 0.134 ** | 0.104 * | 0.013 | |||||||
| 7. Trouble sleeping T1 | 0.198 ** | 0.175 ** | 0.288 ** | 0.210 ** | 0.301 ** | 0.08 | ||||||
| 8. Nightmares T2 | 0.019 | 0.166 | 0.167 * | 0.043 | 0.026 | −0.023 | −0.042 | |||||
| 9. Overtired T2 | 0.009 | 0.088 | −0.006 | 0.067 | 0.095 | 0.197 ** | 0.065 | 0.231 ** | ||||
| 10. Sleeps less T2 | −0.106 | −0.09 | −0.088 | 0.027 | 0.162 * | −0.047 | −0.007 | 0.092 | 0.206 ** | |||
| 11. Sleeps more T2 | −0.042 | 0.017 | −0.122 | −0.076 | −0.114 | 0.008 | −0.067 | −0.019 | 0.065 | −0.053 | ||
| 12. Trouble sleeping T2 | −0.08 | −0.084 | 0.022 | 0.038 | 0.211 ** | 0.089 | 0.116 | 0.171 * | 0.429 ** | 0.408 ** | −0.089 | |
| M | −0.016 | −0.005 | 0.168 | 0.223 | 0.168 | 0.097 | 0.125 | 0.477 | 0.465 | 0.465 | 0.269 | 0.374 |
| SD | 0.837 | 0.605 | 0.381 | 0.463 | 0.425 | 0.344 | 0.394 | 0.577 | 0.652 | 0.643 | 0.562 | 0.614 |
Note. All T1 sleep variables were maternal-reported, and all T2 sleep variables were self-reported, and T1 anxious-withdrawal and victimization/exclusion were based on peer-nominations; T1 = Time 1 or Grade 5/6; T2 = Time 2 or Grade 8; * p < 0.05; ** p < 0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bowker, J.C.; Gurbacki, J.N.; Richard, C.L.; Rubin, K.H. Anxious-Withdrawal and Sleep Problems during Adolescence: The Moderating Role of Peer Difficulties. Behav. Sci. 2023, 13, 740. https://doi.org/10.3390/bs13090740
AMA Style
Bowker JC, Gurbacki JN, Richard CL, Rubin KH. Anxious-Withdrawal and Sleep Problems during Adolescence: The Moderating Role of Peer Difficulties. Behavioral Sciences. 2023; 13(9):740. https://doi.org/10.3390/bs13090740
Chicago/Turabian StyleBowker, Julie C., Jessica N. Gurbacki, Chloe L. Richard, and Kenneth H. Rubin. 2023. "Anxious-Withdrawal and Sleep Problems during Adolescence: The Moderating Role of Peer Difficulties" Behavioral Sciences 13, no. 9: 740. https://doi.org/10.3390/bs13090740
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.