
HLA Typing and Celiac Disease in Moroccans

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population Sample
2.2. DNA Extraction and CD-Associated HLA Class II Polymorphism
2.3. Statistical Analysis
3. Results
3.1. DQ2 and DQ8 genotypes in CD
3.2. Risk Groups and Risk Gradient for CD
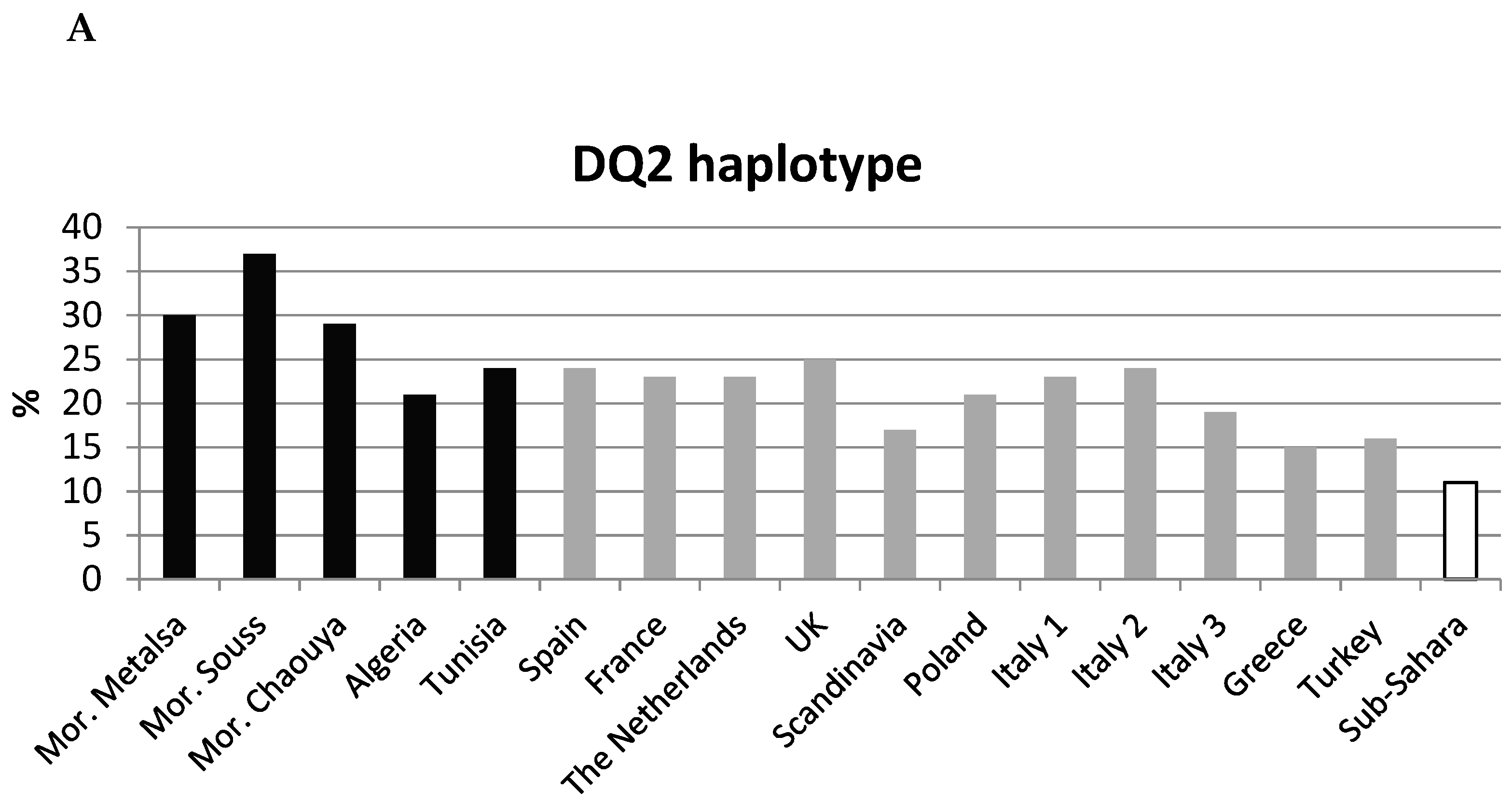
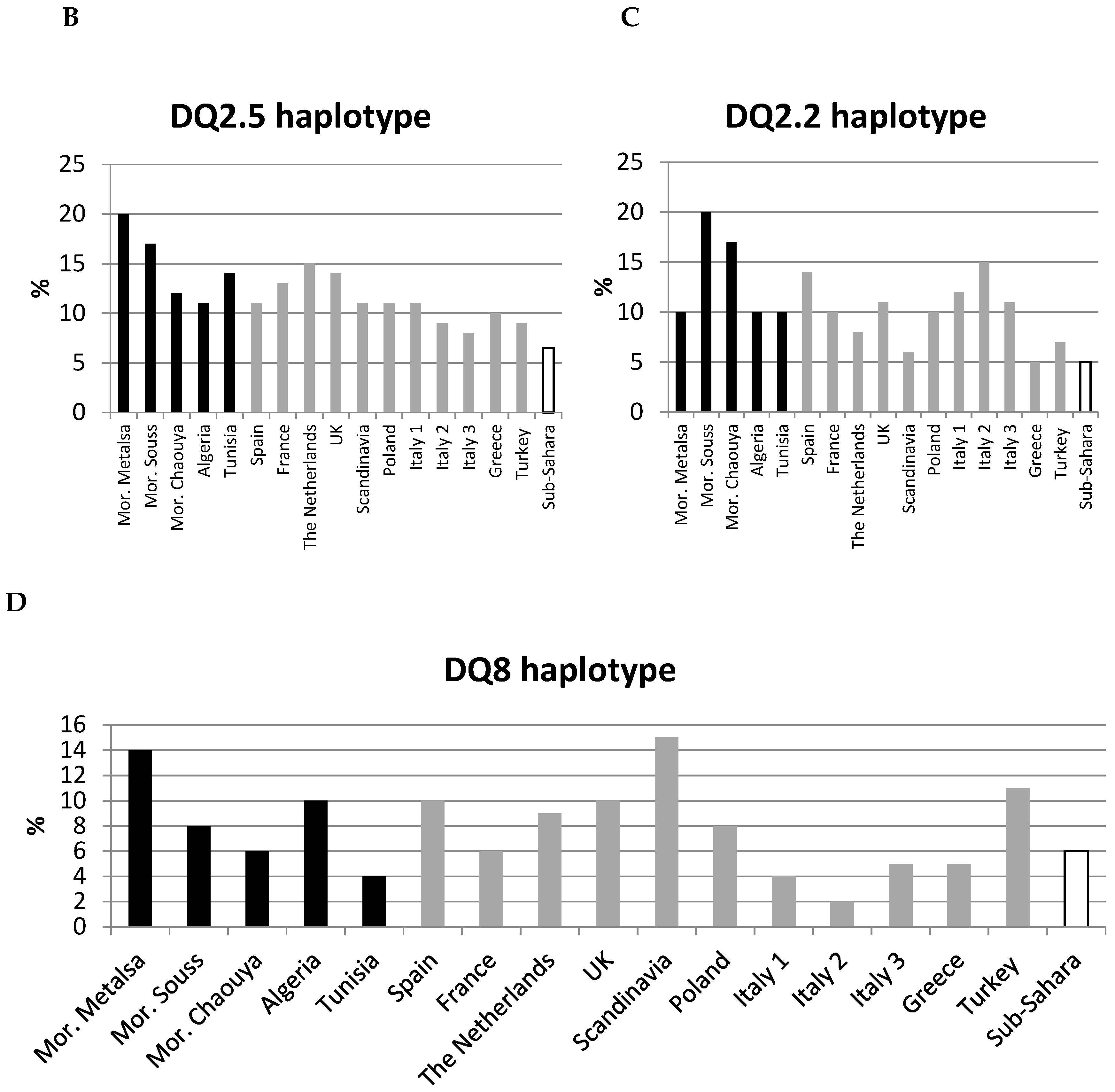
3.3. HLA-DQA1-DQB1-DRB1 haplotypes in populations and in CD
4. Discussion
4.1. CD Prevalence and Geographic Area
4.2. Genetic Test and DQ2 Homozygosity
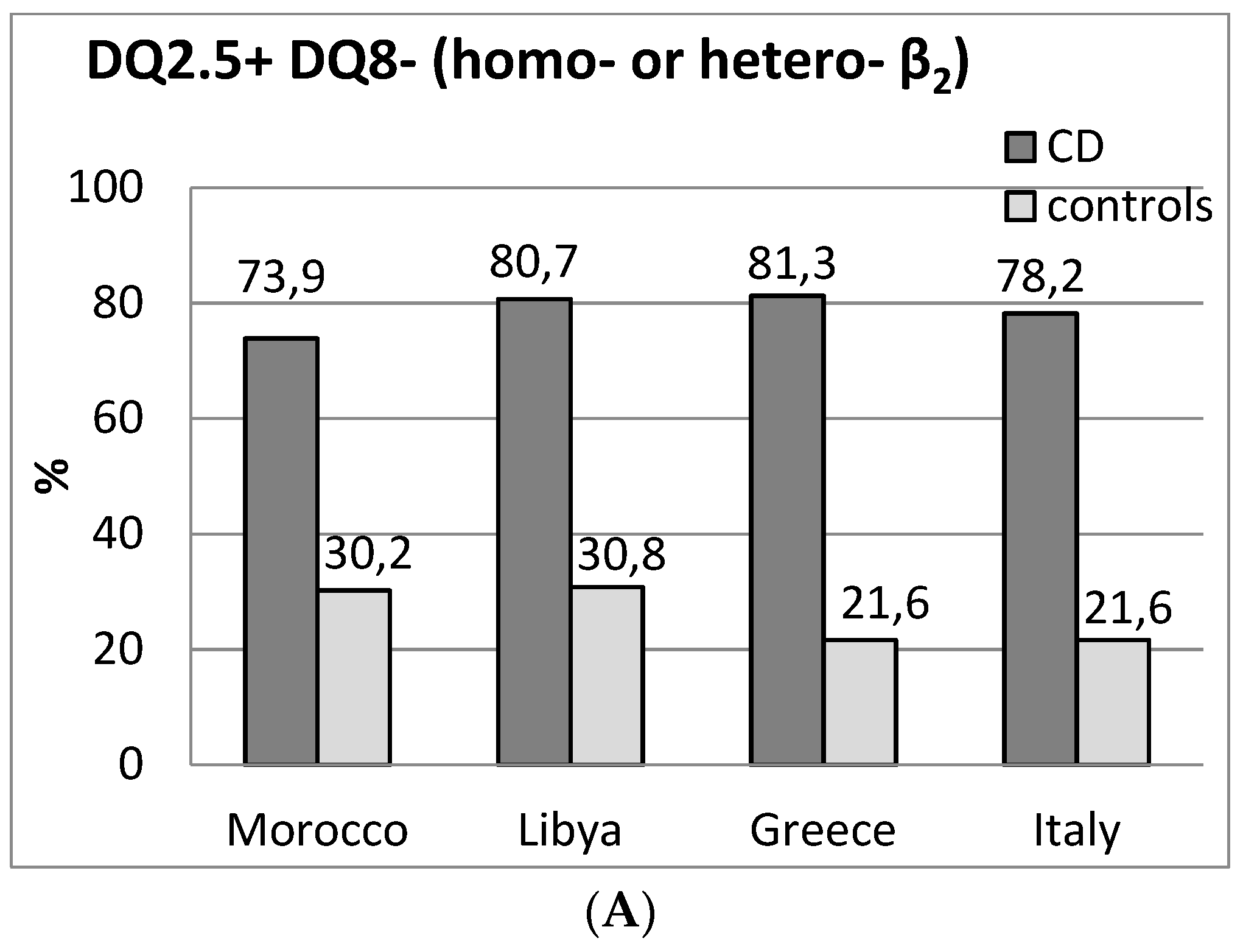
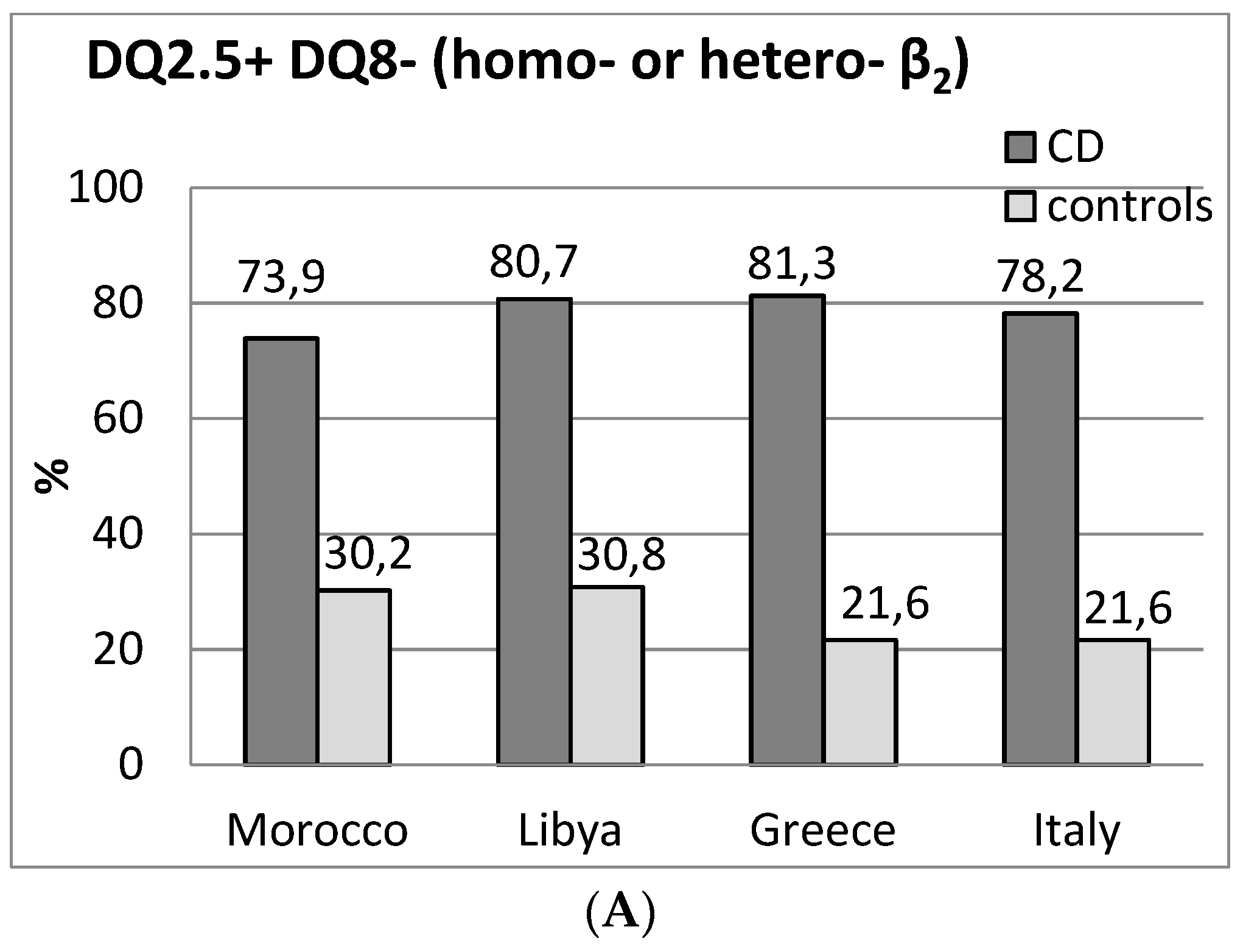
4.3. HLA-DQ2.5 Homozygosity
4.4. DQ8
4.5. Environmental Factors and CD-Associated Genotypes
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Greco, L.; Timpone, L.; Abkari, A.; Abu-Zekry, M.; Attard, T.; Bouguerrà, F.; Cullufi, P.; Kansu, A.; Micetic-Turk, D.; Mišak, Z.; et al. Burden of celiac disease in the Mediterranean area. World J. Gastroenterol. 2011, 17, 4971–4978. [Google Scholar] [CrossRef] [PubMed]
- Piancatelli, D.; Canossi, A.; Aureli, A.; Oumhani, K.; del Beato, T.; Di Rocco, M.; Liberatore, G.; Tessitore, A.; Witter, K.; El Aouad, R.; et al. Human leukocyte antigen-A, -B, and -Cw polymorphism in a Berber population from North Morocco using sequence-based typing. Tissue Antigens 2004, 63, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Nunes, J.M.; Buhler, S.; Roessli, D.; Sanchez-Mazas, A.; The HLA-net 2013 Collaboration. The HLA-net GENE[RATE] pipeline for effective HLA data analysis and its application to 145 population samples from Europe and neighbouring areas. Tissue Antigens 2014, 83, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ghandri, N.; Piancatelli, D.; Adams, S.; Chen, D.; Robbins, F.; Wang, E.; Monaco, A.; Selleri, S.; Bouaouina, N.; et al. Associations between HLA Class I alleles and the prevalence of nasopharyngeal carcinoma (NPC) among Tunisians. J. Transl. Med. 2007, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Brick, C.; Atouf, O.; Bouayad, A.; Essakalli, M. Moroccan study of HLA (-A, -B, -C, -DR, -DQ) polymorphism in 647 unrelated controls. Updating data. Mol. Cell. Probes 2015, 29, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Cataldo, F.; Montalto, G. Celiac disease in the developing countries: A new and challenging public health problem. World J. Gastroenterol. 2007, 13, 2153–2159. [Google Scholar] [CrossRef] [PubMed]
- Megiorni, F.; Mora, B.; Bonamico, M.; Nenna, R.; Di Pierro, M.; Catassi, C.; Drago, S.; Mazzilli, M.C. A rapid and sensitive method to detect specific human lymphocyte antigen (HLA) class II alleles associated with celiac disease. Clin. Chem. Lab. Med. 2008, 46, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Margaritte-Jeannin, P.; Babron, M.C.; Bourgey, M.; Louka, A.S.; Clot, F.; Percopo, S.; Coto, I.; Hugot, J.P.; Ascher, H.; Sollid, L.M.; et al. HLA-DQ relative risks for coeliac disease in European populations: A study of the European Genetics Cluster on Coeliac Disease. Tissue Antigens 2004, 63, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Megiorni, F.; Mora, B.; Bonamico, M.; Barbato, M.; Nenna, R.; Maiella, G.; Lulli, P.; Mazzilli, M.C. HLA-DQ and risk gradient for celiac disease. Hum. Immunol. 2009, 70, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Excoffier, L.; Lischer, H.E.L. Arlequin suite ver 3.5: A new series of programs to perform population genetics analyses under Linux and Windows. Mol. Ecol. Resour. 2010, 10, 564–567. [Google Scholar] [CrossRef] [PubMed]
- Alarida, K.; Harown, J.; Di Pierro, M.R.; Drago, S.; Catassi, C. HLA-DQ2 and -DQ8 genotypes in celiac and healthy Libyan children. Dig. Liver Dis. 2010, 42, 425–427. [Google Scholar] [CrossRef] [PubMed]
- Krini, M.; Chouliaras, G.; Kanariou, M.; Varela, I.; Spanou, K.; Panayiotou, J.; Roma, E.; Constantinidou, N. HLA class II high-resolution genotyping in Greek children with celiac disease and impact on disease susceptibility. Pediatr. Res. 2012, 72, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Charro, B.; Donat, E.; Miner, I.; Aranburu, E.; Sánchez-Valverde, F.; Ramos-Arroyo, M.A. Modifying effect of HLA haplotypes located trans to DQB1*02-DRB1*03 in celiac patients of Southern Europe. Tissue Antigens 2008, 71, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ortiz, E.; Montraveta, M.; Cabré, E.; Herrero-Mata, M.J.; Pujol-Borrell, R.; Palou, E.; Faner, R. HLA-DQ2/DQ8 and HLA-DQB1*02 homozygosity typing by real-time polymerase chain reaction for the assessment of celiac disease genetic risk: Evaluation of a Spanish celiac population. Tissue Antigens 2014, 84, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Galarza, F.F.; Takeshita, L.Y.; Santos, E.J.; Kempson, F.; Maia, M.H.; Silva, A.L.; Silva, A.L.; Ghattaoraya, G.S.; Alfirevic, A.; Jones, A.R.; et al. Allele frequency net 2015 update: New features for HLA epitopes, KIR and disease and HLA adverse drug reaction associations. Nucleic Acid Res. 2015, 28, D784–D788. [Google Scholar] [CrossRef] [PubMed]
- Bourgey, M.; Calcagno, G.; Tinto, N; Gennarelli, D.; Margaritte-Jeannin, P.; Greco, L.; Limongelli, M.G.; Oscar Esposito, O.; Marano, C.; Troncone, R.; et al. HLA related genetic risk for coeliac disease. Gut 2007, 56, 1054–1059. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Achury, J.; Zhernakova, A.; Pulit, S.L.; Trynka, G.; Hunt, K.A.; Romanos, J.; Raychaudhuri, S.; van Heel, D.A.; Wijmenga, C.; de Bakker, P.I. Fine mapping in the MHC region accounts for 18% additional genetic risk for celiac disease. Nat. Genet. 2015, 47, 577–578. [Google Scholar] [CrossRef] [PubMed]
- Barada, K.; Bitar, A.; Mokadem, M.A.; Hashash, J.G.; Green, P. Celiac disease in Middle Eastern and North African countries: A new burden? World J. Gastroenterol. 2010, 16, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Cataldo, F.; Lio, D.; Simpore, J.; Musumeci, S. Consumpion of wheat foodstuffs not a risk for celiac disease occurrence in Burkina Faso. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Cataldo, F.; Pitarresi, N.; Accomando, S.; Greco, L.; SIGENP; GLNBI Working Group on Coeliac Disease. Epidemiological and clinical features in immigrant children with coeliac disease: An Italian multicentre study. Dig. Liver Dis. 2004, 36, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.A.; Moore, S.B.; van Dyke, C.T.; Lahr, B.D.; Dierkhising, R.A.; Zinsmeister, A.R.; Melton, L.J., 3rd; Kroning, C.M.; El-Yousseff, M.; Czaja, A.J. HLA DQ gene dosage and risk and severity of celiac disease. Clin. Gastroenterol. Hepatol. 2007, 5, 1406–1412. [Google Scholar] [CrossRef] [PubMed]
- Vader, W.; Stepniak, D.; Kooy, Y.; Mearin, L.; Thompson, A.; van Rood, J.J.; Spaenij, L.; Koning, F. The HLA-DQ2 gene dose effect in celiac disease is directly related to the magnitude and breadth of gluten-specific T cell responses. Proc. Natl. Acad. Sci. USA 2003, 100, 12390–12395. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Vattiato, C.; Marchese, A.; Trotta, L.; Badulli, C.; de Silvestri, A.; Martinetti, M.; Corazza, G.R. Influence of HLA-DQ2 and DQ8 on severity in celiac disease. J. Clin. Gastroenterol. 2012, 46, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Bergseng, E.; Dørum, S.; Arntzen, M.Ø.; Nielsen, M.; Nygård, S.; Buus, S.; de Souza, G.A.; Sollid, L.M. Different binding motifs of the celiac disease-associated HLA molecules DQ2.5, DQ2.2, and DQ7.5 revealed by relative quantitative proteomics of endogenous peptide repertoires. Immunogenetics 2015, 67, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietzak, M.M.; Schofield, T.C.; McGinniss, M.J.; Nakamura, R.M. Stratifying risk for celiac disease in a large at-risk United States population by using HLA alleles. Clin. Gastroenterol. Hepatol. 2009, 7, 966–971. [Google Scholar] [CrossRef] [PubMed]
- Pisapia, L.; Camarca, A.; Picascia, S.; Bassi, V.; Barba, P.; del Pozzo, G.; Gianfrani, C. HLA-DQ2.5 genes associated with celiac disease risk are preferentially expressed with respect to non-predisposing HLA genes: Implication for anti-gluten T cell response. J. Autoimmun. 2016, 70, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Karinen, H.; Kärkkäinen, P.; Pihlajamäki, J.; Janatuinen, E.; Heikkinen, M.; Julkunen, R.; Kosma, V.M.; Naukkarinen, A.; Laakso, M. Gene dose effect of the DQB1*0201 allele contributes to severity of coeliac disease. Scand. J. Gastroenterol. 2006, 41, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Goerres, M.S.; Meijer, J.W.; Peña, A.S.; Crusius, J.B.; Mulder, C.J. Human leukocyte antigen-DQ2 homozygosity and the development of refractory celiac disease and enteropathy-associated T-cell lymphoma. Clin. Gastroenterol. Hepatol. 2006, 4, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Henderson, K.N.; Tye-Din, J.A.; Reid, H.H.; Chen, Z.; Borg, N.A.; Beissbarth, T.; Tatham, A.; Mannering, S.I.; Purcell, A.W.; Dudek, N.L.; et al. A structural and immunological basis for the role of human leukocyte antigen DQ8 in celiac disease. Immunity 2007, 27, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Schirru, E.; Jores, R.D.; Cicotto, L.; Frau, F.; de Virgiliis, S.; Rossino, R.; Macis, M.D.; Lampis, R.; Congia, M. High frequency of low-risk human leukocyte antigen class II genotypes in latent celiac disease. Hum. Immunol. 2011, 72, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Valarini, N.; Maciel, S.M.; Moura, S.K.; Poli-Frederico, R.C. Association of Dental Caries with HLA Class II Allele in Brazilian Adolescents. Caries Res. 2012, 46, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Cicerone, C.; Nenna, R.; Pontone, S. Th17, intestinal microbiota and the abnormal immune response in the pathogenesis of celiac disease. Gastroenterol. Hepatol. Bed Bench 2015, 8, 117–122. [Google Scholar] [PubMed]
- Olivares, M.; Neef, A.; Castillejo, G.; Palma, G.D.; Varea, V.; Capilla, A.; Palau, F.; Nova, E.; Marcos, A.; Polanco, I.; et al. The HLA-DQ2 genotype selects for early intestinal microbiota composition in infants at high risk of developing coeliac disease. Gut 2015, 64, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, E.; Castellaneta, S.; Francavilla, R.; Pulvirenti, A.; Tonutti, E.; Amarri, S.; Barbato, M.; Barbera, C.; Barera, G.; Bellantoni, A.; et al. Introduction of gluten; HLA status; and the risk of celiac disease in children. N. Engl. J. Med. 2014, 371, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.; Lee, H.S.; Aronsson, C.A.; Hagopian, W.A.; Koletzko, S.; Rewers, M.J.; Eisenbarth, G.S.; Bingley, P.J.; Bonifacio, E.; Simell, V.; et al. Risk of Pediatric Celiac Disease According to HLA Haplotype and Country. N. Engl. J. Med. 2014, 371, 42–49. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HLA Class II Haplotypes 1 | DQB1*02 (α5β2 cis/trans heterodimer) | Risk Group 2 | Risk Group 3 | Morocco CD | Morocco Controls | CD Risk 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DQ heterodimer | DQA1 | DQB1 | DRB1 | DR-DQ | n | % | n | % | Morocco | Italy [9] | Spain [14] | ||||
| 2DQ2 (DQ2.5) CM5: 45,2% Risk 1:14 | 05 | 02 | 03 | DR3-DQ2 | Homozygous | DQ2, DQB1*02/02 | 1 | 22 | 19.1 | 3 | 3.1 | 1:14 | 1:10 | 1:12 | |
| 05 | 02 | 03 | |||||||||||||
| 05 | 02 | 03 | DR3-DQ2 | Homozygous | 30 | 26.1 | 3 | 3.1 | |||||||
| 0201 | 02 | 07 | DR7-DQ2 | ||||||||||||
| DQ2 (DQ2.5) CM5: 28.8% Risk 1:80 | 0201 | 02 | 07 | DR7-DQ2 | One (α5β2 trans) | DQ2, DQB1*02/X | 2 | 11 | 9.6 | 1 | 1.0 | 1:10 | 1:35 | 1:64 | |
| 05 | 0301/04 | 11/12 | DR11/12-DQ7 | ||||||||||||
| 05 | 02 | 03 | DR3-DQ2 | Two (α5β2 cis + trans) | 3 | 8 | 7.0 | 4 | 4.2 | 1:60 | 1:83 | ||||
| 05 | 0301/04 | 11/12 | DR11/12-DQ7 | ||||||||||||
| 05 | 02 | 03 | DR3-DQ2 | One (α5β2 cis) | 14 | 12.2 | 18 | 18.8 | 1:150 | ||||||
| other | other | other | other | ||||||||||||
| DQ2 + DQ8 (DQ2.5 + DQ8) CM5: 4.3% Risk 1:170 | 05 | 02 | 03 | DR3-DQ2 | One (α5β 2 cis) | DQ2 and DQ8 | 3 | 5 | 4.3 | 7 | 7.3 | 1:170 | 1:7 | 1:22 | |
| 03 | 0302 | 04 | DR4-DQ8 | ||||||||||||
| DQ8 CM5: 8.7% Risk 1:190 | 0201 | 02 | 07 | DR7-DQ2.2 | DQ8, DQB1*02+ | 4 | 2 | 1.7 | 2 | 2.1 | 1:120 | 1:24 | 1:22 | ||
| 03 | 0302 | 04 | DR4-DQ8 | ||||||||||||
| 03 | 0302 | 04 | DR4-DQ8 | DQ8, DQB1*02− | 4/5 | 8 | 7.0 | 14 | 14.6 | 1:200 | 1:89 | 1:265 | |||
| other | other | other | |||||||||||||
| DQ2.2 (half DQ2) CM5: 7.8% Risk 1:200 | 0201 | 02 | 07 | DR7-DQ2.2 | Homozygous | β2, DQB1*02/02 | 4 | 2 | 1.7 | 1 | 1.0 | 1:59 | 1:26 | 1:1063 | |
| 0201 | 02 | 07 | |||||||||||||
| 0201 | 02 | 07 | DR7-DQ2.2 | β2, DQB1*02/X | 5 | 7 | 6.1 | 12 | 12.5 | 1:205 | 1:210 | ||||
| other | other | other | |||||||||||||
| Other4 CM5: 5.2% Risk > 1:200 | 05 | 0301/04 | 11/12 | DR11/12-DQ7 | α5 (DQA1*05) | 5 | 4 | 3.5 | 7 | 7.3 | 1:209 | 1:1842 | - | ||
| other | other | other | |||||||||||||
| 05 | other | other | 2 | 1.7 | 2 | 2.1 | 1:124 | ||||||||
| other | other | other | |||||||||||||
| other | other | other | 0 | 0 | 22 | 22.9 | - | 1:2518 | - | ||||||
| other | other | other | |||||||||||||
| Total | 115 | 100 | 96 | 100 | |||||||||||
| Controls (2n = 192) | Celiac Disease (2n = 230) | |||
|---|---|---|---|---|
| DQA1-DQB1-DRB1 | Frequency (n) | Frequency (n) | p | |
| DQ2 | *05-*02-*03 (DQ2.5) | 0.20 (38) | 0.44 (101) | pc < 0.0000 |
| OR: 3.17 | ||||
| CI: 2.04–4.93 | ||||
| *02-*02-*07 (DQ2.2) | 0.10 (20) | 0.24 (54) | pc = 0.003 | |
| O.R. = 2.64 | ||||
| CI: 1.52–4.59 | ||||
| DQ8 | *x-*03:02-*04 | 0.14 (26) | 0.06 (15) | ns |
| *05-*03:01-*11/12 | 0.06 (12) | 0.10 (23) | ns | |
| *05-*x-*x, *x-*x-*x 1 | 0.50 (96) | 0.16 (37) | pc < 0.0000 | |
| OR: 0.19 | ||||
| CI: 0.12–0.30. | ||||
| DQA1-DQB1-DRB1 | Morocco [present study] | Spain [17] | Greece [12] | Italy [17] | UK [17] | The Netherlands [17] | Poland [17] | |
|---|---|---|---|---|---|---|---|---|
| DQ2 | *05-*02-*03 | 0.44 | 0.45 | 0.40 | 0.32 | 0.52 | 0.54 | 0.39 |
| (DQ2.5) | ||||||||
| *02-*02-*07 | 0.24 | 0.23 | 0.20 | 0.28 | 0.16 | 0.13 | 0.19 | |
| (DQ2.2) | ||||||||
| DQ8 | *x-*03:02-*04 | 0.06 | 0.06 | 0.08 | 0.05 | 0.06 | 0.06 | 0.07 |
| *05-*03:01-*11/12 | 0.10 | 0.09 | 0.16 | 0.18 | 0.03 | 0.05 | 0.10 | |
| *05-*x-*x, *x-*x-*x 1 | 0.16 | 0.17 | 0.15 | 0.17 | 0.23 | 0.22 | 0.25 | |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piancatelli, D.; Ben El Barhdadi, I.; Oumhani, K.; Sebastiani, P.; Colanardi, A.; Essaid, A. HLA Typing and Celiac Disease in Moroccans. Med. Sci. 2017, 5, 2. https://doi.org/10.3390/medsci5010002
Piancatelli D, Ben El Barhdadi I, Oumhani K, Sebastiani P, Colanardi A, Essaid A. HLA Typing and Celiac Disease in Moroccans. Medical Sciences. 2017; 5(1):2. https://doi.org/10.3390/medsci5010002
Chicago/Turabian StylePiancatelli, Daniela, Imane Ben El Barhdadi, Khadija Oumhani, Pierluigi Sebastiani, Alessia Colanardi, and Abdellah Essaid. 2017. "HLA Typing and Celiac Disease in Moroccans" Medical Sciences 5, no. 1: 2. https://doi.org/10.3390/medsci5010002