1. Introduction
Salmonella is one of the top bacterial pathogens to cause illnesses, hospitalizations and deaths annually. Centers for disease control and prevention (CDC) estimate about 23,000 hospitalizations in the United States and 155,000 of deaths per year globally due to salmonellosis diseases specifically gastroenteritis disease [
1]. To date, over 2600
Salmonella serotypes were identified and the majority of these serotypes cause human infections. Infected individuals with
Salmonella develop diarrhea, fever and abdominal cramps after 12 to 72 h of infection. The illness usually lasts for 10 days or less [
2].
Considering that
Salmonella species are pathogenic, it comes to no surprise that they are the top food- and waterborne bacterial pathogens responsible for food spoilage and a variety of infections in humans. The ability of
Salmonella to be transmitted through a fecal-oral route of infection makes it one of the major worldwide public health concerns [
3]. Nowadays,
Salmonella outbreaks mainly occur among vulnerable populations such as infants and young children due to the consumption of powdered infant formula. Powdered infant formula manufacturing is one of the most high-risk types of food manufacturing [
2]. The risk of contamination of the manufacture environments may occur as a result of poor operational practices, inadequate hygiene, improper maintenance, substandard facility and equipment design [
1]. Also, the inadequate ingredient control is one of the risk factors for
Salmonella contamination. The ability of
Salmonella to survive and remain stable for a long time in processed and dried (low water activity of 0.2 at 22 °C) products like powdered infant milk has been previously reported [
4]. Moreover, infants are more likely to experience
Salmonella infections due to their less well-developed immune system and their lack of competing intestinal microflora [
5].
The increase in bacterial diseases worldwide is accounted for to a large extent by a parallel global prevalence of multidrug resistant bacteria, such as extended-spectrum beta-lactamases (ESBLs) pathogens. These pathogens including
Salmonella are associated with high rates of mortality and morbidity, which poses a serious threat to the health sectors in many countries. A rapid continuous increase in bacterial diseases has led to the increase in numbers of death among the different age groups in Bahrain [
6]. Among 11,886 Enterobacteriaceae species isolated from hospitals in Bahrain during 2005–2006, 2695 (22.6%) were ESBL producers.
Overall, the prevalence of bacterial diseases including salmonellosis was noticeable worldwide mainly in infants and children below the age of five years. According to the World Health Organization (WHO) data [
5], 550 million people fall ill each year, including 220 million children under the age of five years from diarrheal diseases, with
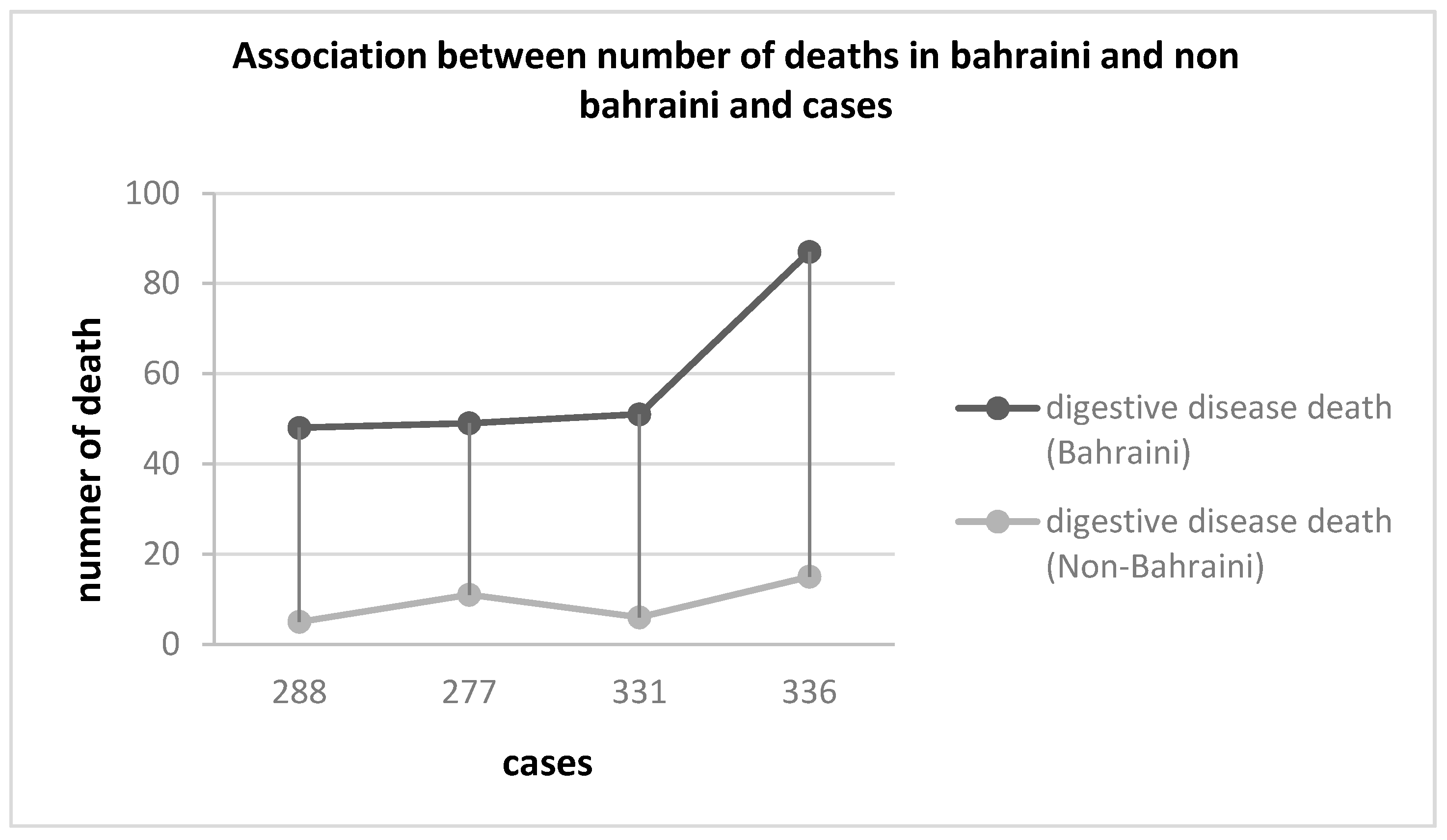
Salmonella being one of the four major causes of diarrheal diseases globally. This has prompted the global health community to alert the public about this disease. For instance, the Ministry of Health in Bahrain has taken a number of initiatives to educate the public about salmonellosis disease in order to prevent it and reduce its ratio in terms of cases to the total population. In this regard, the Ministry of Health in Bahrain started documenting the number of cases in each hospital and health centers. According to the records and statistics data, there was an increase in salmonellosis within the past few years specifically from 2012 to 2015 where it reached its highest number of cases (288 cases to 336 cases, respectively) [
6].
The objectives of this study were to (1) determine whether there was any association between Salmonella infections and geographical region, (2) detect any possible correlation of Salmonella infections with ethnic groups in the Kingdom of Bahrain, (3) determine whether water and birth weight were possible factors for salmonellosis and (4) detect if a relationship existed between gastrointestinal disease-related deaths and salmonellosis.
2. Methods
2.1. Ethical Issues
The study was approved by the Ministry of Health Research Committees reviews.
This decision was made as the obtained data were completely anonymized with no possibility of being linked directly or indirectly to human subjects.
2.2. Data Source
Salmaniya Medical Complex is the main public hospital and the only medical complex in the Kingdom of Bahrain that was established in 1957. The cases of salmonellosis were recorded in this hospital as well as in other private hospitals via laboratory examinations. Biochemical tests were done to confirm the diagnosis by isolating Salmonella from clinical specimens (stool or blood). The specimens were plated on several selective agar media (MacConkey agar, eosin-methylene blue) as well as into an enrichment broth such as tetrathionate. The biochemical reactions of suspicious colonies were then determined on triple sugar iron agar and lysine-iron agar, and a presumptive identification was made. The biochemical identification of Salmonella was achieved using the matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry (MS) that enabled the rapid testing of 10–20 different biochemical parameters simultaneously.
Recorded cases included patients (with information such as age, gender and location) who attended hospitals in Bahrain during 2012–2016. The statistical data was obtained from the Ministry of Health, Bahrain, and is the only data regarding salmonellosis cases in Bahrain. The total population in Bahrain during 2012–2016 was based on the published statistics of the Bahrain Central Informatics Organization.
We analyzed data from 2012–2016 for the age group 0–5 years old and for both genders. In addition, we analyzed the data for all regions (Capital, Muharraq, Northern and Southern governorates). However, the central region was excluded from further analysis because of the lack of data due to its merger with other governorates.
2.3. Statistical Analysis
Statistical analysis was performed using the SPSS version 21 (IBM).12 Descriptive statistics (N, % and mean ± standard deviation (SD) were calculated to assess the number of cases, nationalities, gender, and serotype. Incidence rates (IR) of salmonellosis cases were calculated per 100,000 population per year. The independent t test was applied to test the difference between prevalence rates compared to the category of water (safe versus unsafe) and birth weight (under weight versus normal weight).
4. Discussion
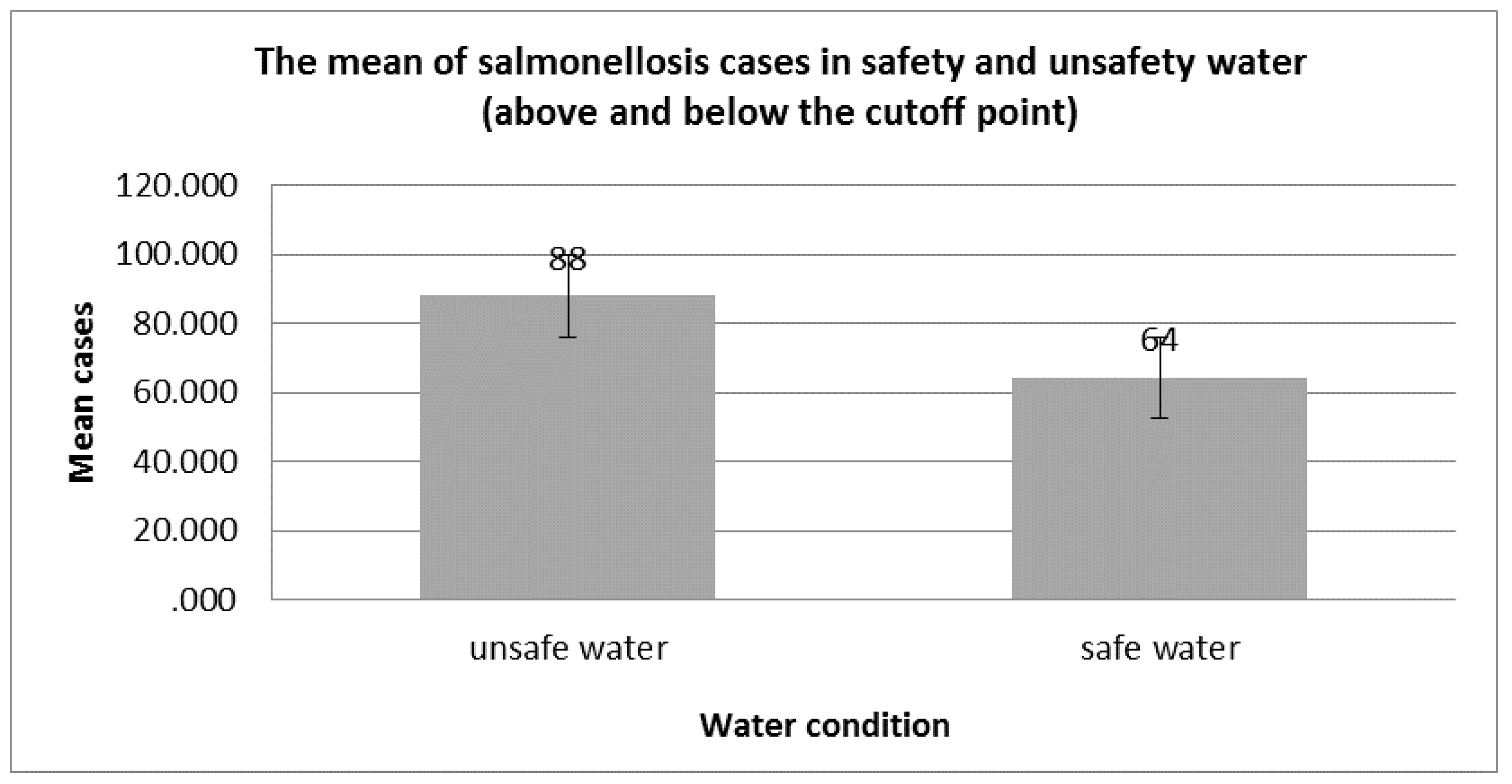
This study, the first of its kind in Bahrain, reports on the cases of salmonellosis in Bahrain, specifically in children below five years of age. The results showed that children between 0–5 years old were susceptible to salmonellosis ranging from 21.050 to 26.675 cases in 100,000 persons. Data on possible risk factors was evaluated as the second outcome of this present study. One possible risk factor was the contamination of the water supply with
Salmonella and other bacterial pathogens (representing 2.14% of the total sample analyzed), in which the mean number of cases from unsafe water reached 88. This is not completely surprising given that Bahrain depends principally on groundwater extraction to meet its irrigation and domestic needs. Moreover, a study on the contamination of potable water in Al-Ahsa region of neighboring Saudi Arabia found that the underground water supplied to the consumers via water vehicles was not suitable for drinking [
7]. For this reason, further studies and investigation on the potability of water supplies in Bahrain are recommended.
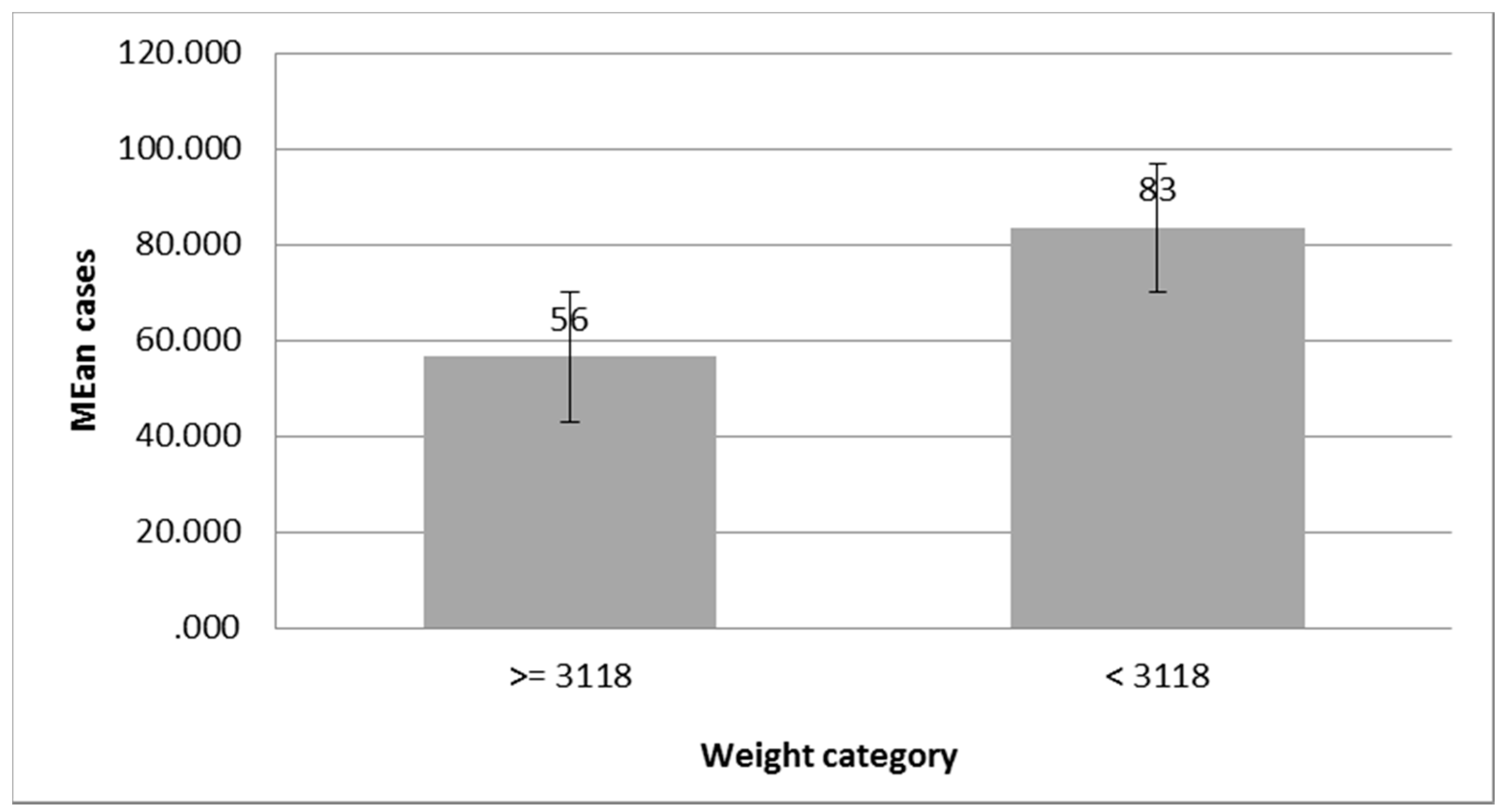
The study also identified low birth weight as a predictor of risk for salmonellosis. In a previous study by Hamadeh et al. [
8] to determine the incidence rate of foodborne climate-related disease and their seasonal variation, the authors found that a relationship existed between
Salmonella cases and climate change. However, their study did not consider salmonellosis and no other possible risk factors were identified.
In a recent similar epidemiological study carried out in the neighboring Gulf country of Qatar, it was reported that the incidence of non-typhoidal salmonellosis decreased during the study period of 2004 to 2016 [
9]. The authors attributed this to the improvement in the food chain and sanitation in the country. Similarly, there was a decline in salmonellosis cases in Bahrain from 331 cases to 300 cases during the study period (2012–2016) due to the improvement in food hygiene standards and surveillance system. For instance, an international outbreak of
Salmonella was linked to a contaminated shipment of sprouted chia seed powder that was distributed globally including Bahrain in 2013–2014. The food recall warnings issued by the local health authorities ensured the removal of the contaminated sprouted chia seed powder products from the marketplace [
10]. Another example was the successful recall and disposal of
Salmonella-contaminated milk that was imported to Bahrain from France [
11]. Despite the decline in the number of salmonellosis cases in Bahrain as a result of the implementation of international standards for food safety and hygiene and the maintenance of a surveillance system for imported foods, the incidence rate in 2012 was high at 23.21 per 100,000 persons. Lower rates were reported in Qatar with 18.1 cases per 100,000 habitants [
9].
One of the novel approaches to identify the epidemiological characteristics of
Salmonella was demonstrated by Boore et al. [
12]. In their study, the authors reported that the number of salmonellosis cases in the United States was 15 per 100,000 persons. In comparison, the number of cases was higher in Bahrain with 26.68 cases per 100,000 inhabitants. The high rate of salmonellosis cases in Bahrain may be attributed to the wide distribution of
Salmonella-contaminated foods. In fact, a salmonellosis outbreak was associated with a local restaurant in 2014 [
11]. Another possible explanation could be the omnipresent source like water as our study results indicated. It must be mentioned, however, that the weakness regarding this data is related to a lack in terms of water contamination microorganisms in overall samples of unsafety water.
In terms of geographical location, our study showed that salmonellosis cases were high in both the Capital (32%) and Northern (26%) regions, however they were in the same low range in the Muharraq (13%), Southern (11%) and Central (18%) regions. This is in agreement with the study of Boore et al. [
12] which reported an approximately equal low number of salmonellosis cases in—several US states while other states had a higher number of cases. Moreover, the similar rate of salmonellosis cases in the different regions may suggest a homogenous source or a relatively even geographic distribution source such as nationally distributed food products. In contrast, the higher cases of salmonellosis in specific regions could be due to the natural restricted reservoir in specific local habits or food products.
On the other hand, the same US study [
12] reported similar findings to our study with regard to the higher number of salmonellosis cases observed in females compared to males. The possible exposure to fresh produce and the food handling practices might explain these results. In addition, the variation in traditional food exposures, including the home-prepared foods sold on the street by unlicensed Bahraini retailers could explain the significant differences in salmonellosis cases and digestive disease-related deaths between Bahrainis and non-Bahrainis.
Furthermore, the highest salmonellosis cases in our study occurred in children below five years of age, which was similar to that of Boore et al. [
12]. This is probably due to the fact that this age group is more likely to seek healthcare, thereby resulting in lower numbers of unreported cases in comparison to the other age groups. Adding to that, the probable link between low-birth weight and immunocompromised infants and the increased incidence of salmonellosis cases [
13].
This study is a basic fundamental for the Bahrain Vision of 2030. Bahrain will be a leading centre for modern medicine, offering high-quality and financially sustainable health care in the region.
Salmonellosis remains an important human disease in Bahrain and presents many challenges to the food and agriculture industries and those charged with the protection of public health. Infection rates will only be reduced if there is the closest possible working relationship between all those involved with food production and the government agencies with responsibility for food safety.
In conclusion, this study identifies unsafe water supplies, low-birth weight, nationality, gender, age, geographical region and gastrointestinal diseases as possible major risk factors to salmonellosis infections, either directly or indirectly. Nevertheless, further clinical and experimental studies are needed to fully explore other possible risk factors of salmonellosis in Bahrain.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}