
Severe COVID-19 in Hospitalized Carriers of Single CFTR Pathogenic Variants

 , , ,
, , ,  ,
,  , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Cohort Patients
3.2. Identified CFTR Pathogenic Variants
3.3. Demographics and Clinical Characteristics of CF Carriers
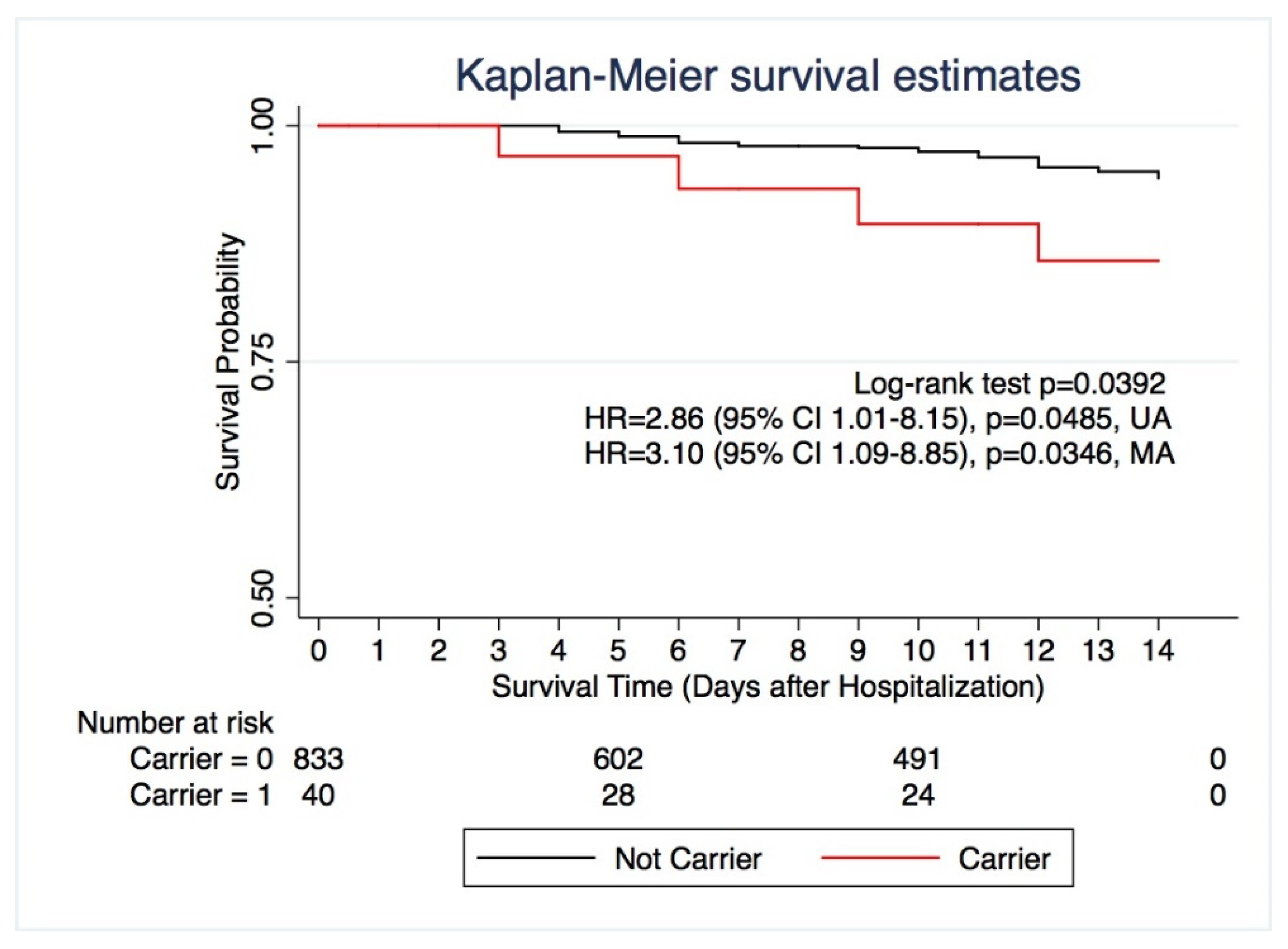
3.4. Mortality in Carriers of CF-Causing Variants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Lopes-Pacheco, M.; Silva, P.L.; Cruz, F.F.; Battaglini, D.; Robba, C.; Pelosi, P.; Morales, M.M.; Caruso Neves, C.; Rocco, P.R.M. Pathogenesis of Multiple Organ Injury in COVID-19 and Potential Therapeutic Strategies. Front. Physiol. 2021, 12, 1–23. [Google Scholar] [CrossRef]
- WHO Coronavirus Disease 2019 (COVID-19) Situation Report. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 12 June 2021).
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020, M20-3012. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19). JAMA 2020, 324, 782. [Google Scholar] [CrossRef] [PubMed]
- Mahmudpour, M.; Roozbeh, J.; Keshavarz, M.; Farrokhi, S.; Nabipour, I. COVID-19 cytokine storm: The anger of inflammation. Cytokine 2020, 133, 155151. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, S.; Liu, H.; Li, W.; Lin, F.; Jiang, L.; Li, X.; Xu, P.; Zhang, L.; Zhao, L.; et al. SARS-CoV-2 infection of the liver directly contributes to hepatic impairment in patients with COVID-19. J. Hepatol. 2020, 73, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wang, H.; Fan, J.; Zhang, Y.; Wang, H.; Zhao, Q. Pancreatic Injury Patterns in Patients With Coronavirus Disease 19 Pneumonia. Gastroenterology 2020, 159, 367–370. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (Lond. Engl.) 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Severe Covid-19 GWAS Group; Ellinghaus, D.; Degenhardt, F.; Bujanda, L.; Buti, M.; Albillos, A.; Invernizzi, P.; Fernández, J.; Prati, D.; Baselli, G.; et al. Genomewide Association Study of Severe Covid-19 with Respiratory Failure. N. Engl. J. Med. 2020, 383, 1522–1534. [Google Scholar] [CrossRef]
- Vietzen, H.; Zoufaly, A.; Traugott, M.; Aberle, J.; Aberle, S.W.; Puchhammer-Stöckl, E. Deletion of the NKG2C receptor encoding KLRC2 gene and HLA-E variants are risk factors for severe COVID-19. Genet. Med. 2021, 1–5. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, Z.; Moncada-Velez, M.; Chen, J.; Ogishi, M.; Bigio, B.; Yang, R.; Arias, A.A.; Zhou, Q.; Han, J.E.; et al. Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science 2020, 370. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Host Genetics Initiative. The COVID-19 Host Genetics Initiative, a global initiative to elucidate the role of host genetic factors in susceptibility and severity of the SARS-CoV-2 virus pandemic. Eur. J. Hum. Genet. 2020, 28, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Benetti, E.; Giliberti, A.; Emiliozzi, A.; Valentino, F.; Bergantini, L.; Fallerini, C.; Anedda, F.; Amitrano, S.; Conticini, E.; Tita, R.; et al. Clinical and molecular characterization of COVID-19 hospitalized patients. PLoS ONE 2020, 15, e0242534. [Google Scholar] [CrossRef]
- Benetti, E.; Tita, R.; Spiga, O.; Ciolfi, A.; Birolo, G.; Bruselles, A.; Doddato, G.; Giliberti, A.; Marconi, C.; Musacchia, F.; et al. ACE2 gene variants may underlie interindividual variability and susceptibility to COVID-19 in the Italian population. Eur. J. Hum. Genet. 2020, 28, 1602–1614. [Google Scholar] [CrossRef] [PubMed]
- Pairo-Castineira, E.; Clohisey, S.; Klaric, L.; Bretherick, A.D.; Rawlik, K.; Pasko, D.; Walker, S.; Parkinson, N.; Fourman, M.H.; Russell, C.D.; et al. Genetic mechanisms of critical illness in Covid-19. Nature 2020. [Google Scholar] [CrossRef]
- Daga, S.; Fallerini, C.; Baldassarri, M.; Fava, F.; Valentino, F.; Doddato, G.; Benetti, E.; Furini, S.; Giliberti, A.; Tita, R.; et al. Employing a systematic approach to biobanking and analyzing clinical and genetic data for advancing COVID-19 research. Eur. J. Hum. Genet. 2021. [Google Scholar] [CrossRef]
- Baldassarri, M.; Picchiotti, N.; Fava, F.; Fallerini, C.; Benetti, E.; Daga, S.; Valentino, F.; Doddato, G.; Furini, S.; Giliberti, A.; et al. Shorter androgen receptor polyQ alleles protect against life-threatening COVID-19 disease in European males. EBioMedicine 2021, 65. [Google Scholar] [CrossRef]
- Fallerini, C.; Daga, S.; Mantovani, S.; Benetti, E.; Picchiotti, N.; Francisci, D.; Paciosi, F.; Schiaroli, E.; Baldassarri, M.; Fava, F.; et al. Association of toll-like receptor 7 variants with life-threatening COVID-19 disease in males: Findings from a nested case-control study. Elife 2021, 10. [Google Scholar] [CrossRef]
- Elborn, J.S. Cystic fibrosis. Lancet 2016, 388, 2519–2531. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Roesch, E.A.; Nichols, D.P.; Chmiel, J.F. Inflammation in cystic fibrosis: An update. Pediatr. Pulmonol. 2018, 53, S30–S50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, A.C.; Comellas, A.P.; Hornick, D.B.; Stoltz, D.A.; Cavanaugh, J.E.; Gerke, A.K.; Welsh, M.J.; Zabner, J.; Polgreen, P.M. Cystic fibrosis carriers are at increased risk for a wide range of cystic fibrosis-related conditions. Proc. Natl. Acad. Sci. USA 2020, 117, 1621–1627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polgreen, P.M.; Brown, G.D.; Hornick, D.B.; Ahmad, F.; London, B.; Stoltz, D.A.; Comellas, A.P. CFTR heterozygotes are at increased risk of respiratory infections: A population-based study. Open Forum Infect. Dis. 2018, 5, 1–7. [Google Scholar] [CrossRef] [Green Version]
- WHO R&D Blueprint novel Coronavirus COVID-19 Therapeutic Trial Synopsis. 2020. Available online: https://www.who.int/publications/i/item/covid-19-therapeutic-trial-synopsis (accessed on 23 May 2021).
- Freeman, G.H.; Halton, J.H. Note on an Exact Treatment of Contingency, Goodness of Fit and Other Problems of Significance. Biometrika 1951, 38, 141. [Google Scholar] [CrossRef] [PubMed]
- Groman, J.D.; Hefferon, T.W.; Casals, T.; Bassas, L.; Estivill, X.; Des Georges, M.; Guittard, C.; Koudova, M.; Fallin, M.D.; Nemeth, K.; et al. Variation in a Repeat Sequence Determines Whether a Common Variant of the Cystic Fibrosis Transmembrane Conductance Regulator Gene Is Pathogenic or Benign. Am. J. Hum. Genet. 2004, 74, 176–179. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, S.E.; Brigman, K.N.; Koller, B.H.; Boucher, R.C.; Stutts, M.J. Cystic fibrosis heterozygote resistance to cholera toxin in the cystic fibrosis mouse model. Science 1994, 266, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Trapnell, B.C.; Chu, C.S.; Paakko, P.K.; Banks, T.C.; Yoshimura, K.; Ferrans, V.J.; Chernick, M.S.; Crystal, R.G. Expression of the cystic fibrosis transmembrane conductance regulator gene in the respiratory tract of normal individuals and individuals with cystic fibrosis. Proc. Natl. Acad. Sci. USA. 1991, 88, 6565–6569. [Google Scholar] [CrossRef] [Green Version]
- Cohn, J.A.; Friedman, K.J.; Noone, P.G.; Knowles, M.R.; Silverman, L.M.; Jowell, P.S. Relation between Mutations of the Cystic Fibrosis Gene and Idiopathic Pancreatitis. N. Engl. J. Med. 1998, 339, 653–658. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11. [Google Scholar] [CrossRef]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Saksena, S.; Sadri-Ardekani, H. ACE2 receptor expression in testes: Implications in coronavirus disease 2019 pathogenesis. Biol. Reprod. 2020, 103, 449–451. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W.; et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat. Med. 2005, 11, 875–879. [Google Scholar] [CrossRef] [PubMed]
- McNabb-Baltar, J.; Jin, D.X.; Grover, A.S.; Redd, W.D.; Zhou, J.C.; Hathorn, K.E.; McCarty, T.R.; Bazarbashi, A.N.; Shen, L.; Chan, W.W. Lipase Elevation in Patients With COVID-19. Am. J. Gastroenterol. 2020, 115, 1286–1288. [Google Scholar] [CrossRef] [PubMed]
- Sarantis, P.; Koustas, E.; Papavassiliou, A.G.; Karamouzis, M.V. Are cystic fibrosis mutation carriers a potentially highly vulnerable group to COVID-19? J. Cell. Mol. Med. 2020, 24, 13542–13545. [Google Scholar] [CrossRef]
- Shah, V.S.; Ernst, S.; Tang, X.X.; Karp, P.H.; Parker, C.P.; Ostedgaard, L.S.; Welsh, M.J. Relationships among CFTR expression, HCO3- secretion, and host defense may inform gene- and cell-based cystic fibrosis therapies. Proc. Natl. Acad. Sci. USA 2016, 113, 5382–5387. [Google Scholar] [CrossRef] [Green Version]
- Bezzerri, V.; Lucca, F.; Volpi, S.; Cipolli, M. Does cystic fibrosis constitute an advantage in COVID-19 infection? Ital. J. Pediatr. 2020, 46, 1–3. [Google Scholar] [CrossRef]
- Colombo, C.; Burgel, P.-R.; Gartner, S.; van Koningsbruggen-Rietschel, S.; Naehrlich, L.; Sermet-Gaudelus, I.; Southern, K.W. Impact of COVID-19 on people with cystic fibrosis. Lancet. Respir. Med. 2020, 8, e35–e36. [Google Scholar] [CrossRef]
- Cosgriff, R.; Ahern, S.; Bell, S.C.; Brownlee, K.; Burgel, P.-R.; Byrnes, C.; Corvol, H.; Cheng, S.Y.; Elbert, A.; Faro, A.; et al. A multinational report to characterise SARS-CoV-2 infection in people with cystic fibrosis. J. Cyst. Fibros. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Shaw, D.M.; Petty, L.E.; Graff, M.; Bohlender, R.J.; Polikowsky, H.G.; Zhong, X.; Kim, D.; Buchanan, V.L.; Preuss, M.H.; et al. Host genetic effects in pneumonia. Am. J. Hum. Genet. 2020, 1–8. [Google Scholar] [CrossRef]
- Chen, R.; Liang, W.; Jiang, M.; Guan, W.; Zhan, C.; Wang, T.; Tang, C.; Sang, L.; Liu, J.; Ni, Z.; et al. Risk Factors of Fatal Outcome in Hospitalized Subjects With Coronavirus Disease 2019 From a Nationwide Analysis in China. Chest 2020, 158, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Price-Haywood, E.G.; Burton, J.; Fort, D.; Seoane, L. Hospitalization and Mortality among Black Patients and White Patients with Covid-19. N. Engl. J. Med. 2020, 382, 2534–2543. [Google Scholar] [CrossRef] [PubMed]
- Castellani, C.; Massie, J.; Sontag, M.; Southern, K.W. Newborn screening for cystic fibrosis. Lancet Respir. Med. 2016, 4, 653–661. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Whole Cohort (n = 874) | Female (n = 377, 43.13%) | Male (n = 496, 56.75%) | |
|---|---|---|---|
| Age, mean ± SD (year) | 59.9 ± 15.64 | 59.78 ± 14.89 | 59.99 ± 16.6 |
| Cat. 1 (Death) | 75.73 ± 10.98 § | 77.4 ± 12.50 | 74.33 ± 9.53 |
| Cat. 2 (Invasive mechanical ventilation) | 60.53 ± 12.19 § | 60 ± 13.86 | 60.71 ± 11.69 |
| Cat. 3 (CPAP/BiPAP) | 63.62 ± 12.46 § | 66.91 ± 13.53 | 62.24 ± 11.79 ° |
| Cat. 4 (Hospitalized with low flow oxygen) | 65.50 ± 14.4 § | 68.08 ± 14.75 | 63.77 ± 13.93 ° |
| Cat. 5 (Hospitalized without oxygen) | 55.74 ± 15.89 § | 54.9 ± 16.85 | 56.5 ± 15.06 |
| Cat. 6 (Not hospitalized) | 47.68 ± 12.01 | 48.38 ± 10.74 | 46.64 ± 13.66 |
| COVID-19 Outcome Scale, No. (%) | |||
| Cat. 1 (Death) | 55 (6.29) | 25 (45.45) | 30 (54.55) * |
| Cat. 2 (Invasive mechanical ventilation) | 70 (8.01) | 18 (25.71) | 52 (74.29) ** |
| Cat. 3 (CPAP/BiPAP) | 146 (16.7) | 43 (29.45) | 103 (70.55) ** |
| Cat. 4 (Hospitalized with low flow oxygen) | 276 (31.58) | 111 (40.22) | 165 (59.64) ** |
| Cat. 5 (Hospitalized without oxygen) | 122 (13.96) | 58 (47-54) | 64 (52.46) * |
| Cat. 6 (Not hospitalized) | 205 (23.45) | 122 (59.51) | 83 (40.49) |
| Chronic Conditions, No. (%) | |||
| Hypertension | 243 (27.8) | 93 (38.27) | 150 (61.63) |
| Diabetes | 105 (12.22) | 44 (41.9) | 61 (58.1) |
| Asthma and COPD | 72 (8.64) | 33 (45.83) | 39 (54.17) |
| CHF and CAD | 68 (8) | 21 (31.34) | 47 (69.11) ° |
| Malignancy | 65 (7.24) | 35 (53.85) | 30 (46.15) |
| Hypothyroidism | 42 (4.8) | 29 (69.05) °° | 13 (30.95) |
| Obesity | 29 (3.35) | 13 (44.83) | 16 (55.17) |
| Total Cohort | Age < 50 years (n = 225) | Age ≥ 50 years (n = 648) | |
|---|---|---|---|
| Total Carriers, No. | 40 | 16 | 24 |
| Carriers by COVID-19 Outcome Scale, No. (%) | |||
| Cat. 1 (Death; n = 55) | 4 (7.1) | 0 | 4 (7.1) |
| Cat. 2 (Invasive mechanical ventilation; n = 70) | 6 (8.7) * | 3 (25) ** | 3 (5.3) |
| Cat. 3 (CPAP/BiPAP; n = 146) | 8 (5.5) | 2 (10) | 6 (4.8) |
| Cat. 4 (Hospitalized, with low flow oxygen; n = 275) | 7 (2.5) | 2 (5.9) | 5 (2.1) |
| Cat. 5 (Hospitalized, without oxygen; n = 122) | 5 (4.1) | 2 (4.7) | 3 (3.8) |
| Cat. 6 (Not hospitalized; n = 205) | 10 (4.9) | 7 (6) | 3 (3.4) |
| Not Carriers (n = 833) | Carriers (n = 40) | |
|---|---|---|
| Age, mean ± SD | ||
| All | 60.09 ± 15.51 | 55.85 ± 17.88 |
| Female | 59.73 ± 16.66 | 61 ± 15.32 |
| Male | 60.37 ± 14.57 | 53.08 ± 18.8 § |
| Cat. 1 (Death) | 75.67 ± 11.13 | 76.5 ± 10.38 |
| Cat. 2 (Invasive mechanical ventilation) | 61.42 ± 10.99 | 51.00 ± 20.21 * |
| Cat. 3 (CPAP/BiPAP) | 63.64 ± 12.08 | 63.25 ± 19 |
| Cat. 4 (Hospitalized with low flow oxygen) | 65.77 ± 14.28 | 57.28 ± 17.74 |
| Cat. 5 (Hospitalized without supplemental oxygen) | 55.75 ± 16.13 ° | 55.40 ± 9.55 # |
| Cat. 6 (Not hospitalized) | 47.88 ± 11.95 °° | 43.80 ± 13.19 ## |
| Outcome | Level | RR | 95% CI |
|---|---|---|---|
| PaO2/FIO2 ratio | ≤250 | 1.54 * | 0.99–1.76 |
| Invasive mechanical ventilation/CPAP/BiPAP | yes vs no | 1.50 | 0.97–2.07 |
| C-reactive protein level (mg/dL) | ≥20 | 1.69 ** | 1.06–2.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldassarri, M.; Fava, F.; Fallerini, C.; Daga, S.; Benetti, E.; Zguro, K.; Amitrano, S.; Valentino, F.; Doddato, G.; Giliberti, A.; et al. Severe COVID-19 in Hospitalized Carriers of Single CFTR Pathogenic Variants. J. Pers. Med. 2021, 11, 558. https://doi.org/10.3390/jpm11060558
Baldassarri M, Fava F, Fallerini C, Daga S, Benetti E, Zguro K, Amitrano S, Valentino F, Doddato G, Giliberti A, et al. Severe COVID-19 in Hospitalized Carriers of Single CFTR Pathogenic Variants. Journal of Personalized Medicine. 2021; 11(6):558. https://doi.org/10.3390/jpm11060558
Chicago/Turabian StyleBaldassarri, Margherita, Francesca Fava, Chiara Fallerini, Sergio Daga, Elisa Benetti, Kristina Zguro, Sara Amitrano, Floriana Valentino, Gabriella Doddato, Annarita Giliberti, and et al. 2021. "Severe COVID-19 in Hospitalized Carriers of Single CFTR Pathogenic Variants" Journal of Personalized Medicine 11, no. 6: 558. https://doi.org/10.3390/jpm11060558
APA StyleBaldassarri, M., Fava, F., Fallerini, C., Daga, S., Benetti, E., Zguro, K., Amitrano, S., Valentino, F., Doddato, G., Giliberti, A., Di Sarno, L., Palmieri, M., Carriero, M. L., Alaverdian, D., Beligni, G., Iuso, N., Castelli, F., Quiros-Roldan, E., Mondelli, M. U., ... on behalf of the GEN-COVID Multicenter Study. (2021). Severe COVID-19 in Hospitalized Carriers of Single CFTR Pathogenic Variants. Journal of Personalized Medicine, 11(6), 558. https://doi.org/10.3390/jpm11060558