1. Introduction
The criteria of systemic inflammatory response syndrome (SIRS) are an easy-to-apply set of clinical parameters that aid clinicians in identifying potential patients with systemic infection [
1,
2,
3]. Clinicians frequently rely on fever as a criterion for initiating infection surveys in the emergency department (ED). Patients with fever accompanied by signs of severe infection, such as a change in mental status or low blood pressure, can aid physicians in tentatively diagnosing bacteremia [
4]. However, patients with bacteremia might present to the ED without evidence of fever. Delays in diagnosis and treatment might occur in these patients. Previous studies have identified that afebrile bacteremia has a distinct presentation in the elderly or patients with an immunosuppressed status [
5,
6,
7,
8,
9]. According to a previous retrospective cohort study, the authors found that 14.9% (140/937) of patients with episodes of afebrile bacteremia during the one-year study period had a high mortality rate reaching 45% [
9]. In a study, Lin et al. revealed that age > 64 years, liver cirrhosis, malignancy, use of alcohol, polymicrobial bacteremia, anemia, and sepsis were independent positive predictors of short-term mortality in ED bacteremic patients [
10]. In a case–control study, the ED patients with polymicrobial bacteremia had a higher mortality rate than those with monomicrobial bacteremia [
11]. Several studies reported that the cause of higher mortality rates partly attributed to afebrile bacteremia with lowered level warnings by the clinicians. This cause may be related to a delayed or absent response to antimicrobial therapy in many patients within 24 h of admission [
12,
13,
14,
15]. Another possibility for a terrible prognosis in patients with afebrile bacteremia is the development of a poor immune response to bacterial invasion, putting the patient at risk of impediment and death [
16].
In the literature review, there is no research on afebrile bacteremia on specific factitive microorganisms to assess the association of different pathogens on clinical outcomes. In this study, we analyzed the clinical characteristics and laboratory data of 600 afebrile adult patients visiting the ED with bacteremia caused by monomicrobial gram-negative bacteria (GNB) during a 10-year study period. Our goal is to clarify specific risk factors and various scoring systems, in order to predict the mortality risk of bacteremia caused by monomicrobial GNB in afebrile adult patients.
4. Discussion
The main findings of this study were as follows: (1) Age ≥ 75 years and malignancy were the comorbid conditions most associated with afebrile monomicrobial GNB; (2) The mortality rate in ED patients with afebrile bacteremia caused by monomicrobial GNB was as high as 50.17% and, exceptionally, reached 68.52% in patients with liver cirrhosis; (3) The gram-negative bacterial pathogens were similar in both the survivor and non-survivor groups. E. coli was the leading pathogen; (4) Several risk factors were associated with mortality, including male gender, liver cirrhosis, malignancy, and septic shock. The increased levels of RDW, high serum lactate, and low serum albumin had the highest association with death probability, so we used them as parameters for revising scoring systems; (5) The original MEDS, revised MEDS, revised qSOFA, and revised NEWS were valuable tools for predicting the mortality risk in patients with afebrile bacteremia caused by monomicrobial GNB.
The reported literature described afebrile bacteremia as having a distinct presentation in the elderly and patients with an immunosuppressed status [
5,
6,
7,
8,
9]. Yo et al. further reported that the oldest group (age ≥ 85 years) and solid malignancy were the comorbidities that were most apt to obtain afebrile bacteremia [
9]. In this study, we also found that afebrile bacteremia of monomicrobial GNB most frequently occurred in those aged ≥75 years (42.66%, 256 of 600) and in patients with malignancy (53.83%, 323 of 600). We found a certain proportion of adult patients aged between 18 and 64 years old (36.66%, 220 of 600) in this study. Our study revealed a higher mortality rate of 50.17% in patients with afebrile bacteremia of monomicrobial GNB. In the subgroup of patients with liver cirrhosis, we found an extremely high mortality rate of up to 68.52%.
Yo et al. reported that
E. coli infection was an independent negative predictor of afebrile bacteremia [
9]. However,
E. coli is the predominant causative pathogen (42.83%, 257 of 600) in this series of patients with afebrile bacteremia of monomicrobial GNB. The bacteriology was similar in both groups and other gram-negative pathogens, including
Klebsiella spp. (20%),
Salmonella spp. (6%), and
Pseudomonas spp. (5%) were present. Previous research on GNB reported that
E. coli is the most common pathogen in patients with community-acquired bacteremia, occurring in 26.6% of patients, and this is the second most common bacteria within hospital-acquired infection, occurring in 21.3% of patients.
Klebsiella pneumoniae is the third most common pathogen for both community- and hospital-acquired bacteremia, responsible for 7.2% and 8.8% of patients, respectively.
Pseudomonas aeruginosa is the fourth most prevalent pathogen of hospital-acquired bacteremia (7.4% of patients) and ranked the fifth most common pathogen causing community-acquired bacteremia (7.3% of patients) [
17,
18,
19]. In our series of patients, specific causative pathogens, such as
E. coli,
Klebsiella spp.,
Salmonella spp., and
Pseudomonas spp., were not associated with increased mortality in patients with afebrile bacteremia caused by monomicrobial GNB.
The following factors were associated with in-hospital mortality, including male gender, liver cirrhosis, malignancy, and septic shock in this study of patients with afebrile bacteremia of monomicrobial GNB. Our findings were consistent with previous studies that reported a mortality risk associated with sepsis. At an older age, immunosuppressive diseases, and DM are well-established risk factors relating to a patient’s susceptibility to be infected and becoming victim to different organ failures [
20]. Some epidemiological studies have revealed a lower prevalence of sepsis in women than in men [
21,
22]. However, the evidence on how gender influences clinical outcomes in sepsis was changeable from previous retrospective studies, and there is no precise evidence on how gender impacts the outcomes in sepsis [
23,
24]. In this series of patients, we found that men had significantly higher in-hospital mortality rates than women (67.10% vs. 32.89%,
p < 0.001) among those with afebrile bacteremia of monomicrobial GNB.
Patients with liver cirrhosis, complicating the bacterial infection, frequently have atypical manifestations, such as an afebrile state [
25]. Chen et al. described that ED patients with afebrile bacteremia showed a higher rate of inappropriate antibiotic administration. They also had a higher 30-day mortality rate than the febrile group (40% vs. 18.4%) [
26]. We found that cirrhotic patients with afebrile bacteremia of microbial GNB had an extremely high mortality rate of 68.52% (74 of 108). On the univariate logistic regression modeling, liver cirrhosis associated with a higher OR of2.541 (
p < 0.001) was a positive predictor of the mortality risk.
In this study, hyperlipidemic patients with afebrile bacteremia of monomicrobial GNB had a lower OR of 0.458 (
p < 0.001) associated with death. In an animal study, Morin et al. reported that higher high-density lipoprotein (HDL) cholesterol levels were related to a lower mortality risk of sepsis [
27]. Furthermore, in a prospective cohort study, Chien et al. found that a lower low-density lipoprotein (LDL) cholesterol level on day 1 of severe sepsis had a higher mortality rate and grave outcomes [
28]. Hyperlipidemia may be a protective factor in patients with afebrile bacteremia of monomicrobial GNB. However, lipid profiles, including HDL and LDL of cholesterol, were not routinely assessed in the ED. Further studies are required to gain evidence on how hyperlipidemia influences the clinical outcomes of bacteremia.
The authors developed various easy-to-apply scoring systems based on clinical parameters, in order to aid physicians in identifying potentially critical conditions early and quickly stratify patients in the ED or intensive care units (ICU) [
29,
30,
31,
32,
33]. Shapiro et al. first developed the MEDS score in 2003, including nine parameters (age, nursing home residence, terminal disease, respiratory difficulty, lower respiratory infection, septic shock, platelet, band proportion, and altered mental status). Due to its ready availability, ED clinicians could use the MEDS score to evaluate the mortality risk during the patient’s presentation [
29]. This score accurately predicts mortality in ED patients with suspected infection [
34,
35]. Smith et al. first published the NEWS in 2012, which demonstrated outstanding ability and a high maximum AUC of the ROC in predicting risk in patients with cardiac arrest, unplanned ICU admission, or death within 24 h [
30,
36]. Physicians performed the NEWS, including body temperature, heart rate, respiratory rate, systolic blood pressure, oxygen saturation, the necessity of oxygen supply, and consciousness level, to measure the scores during the ED course. As a rapid and more simplified ED sepsis screening tool, the qSOFA consists of three items, including altered mental status (GCS < 15), respiratory rate ≥ 22/min, and systolic blood pressure ≤ 100 mmHg [
4,
35]. Although the qSOFA may be a tool to predict sepsis-related mortality, some studies suggested it performs poorly in predicting severe sepsis and mortality [
37,
38,
39].
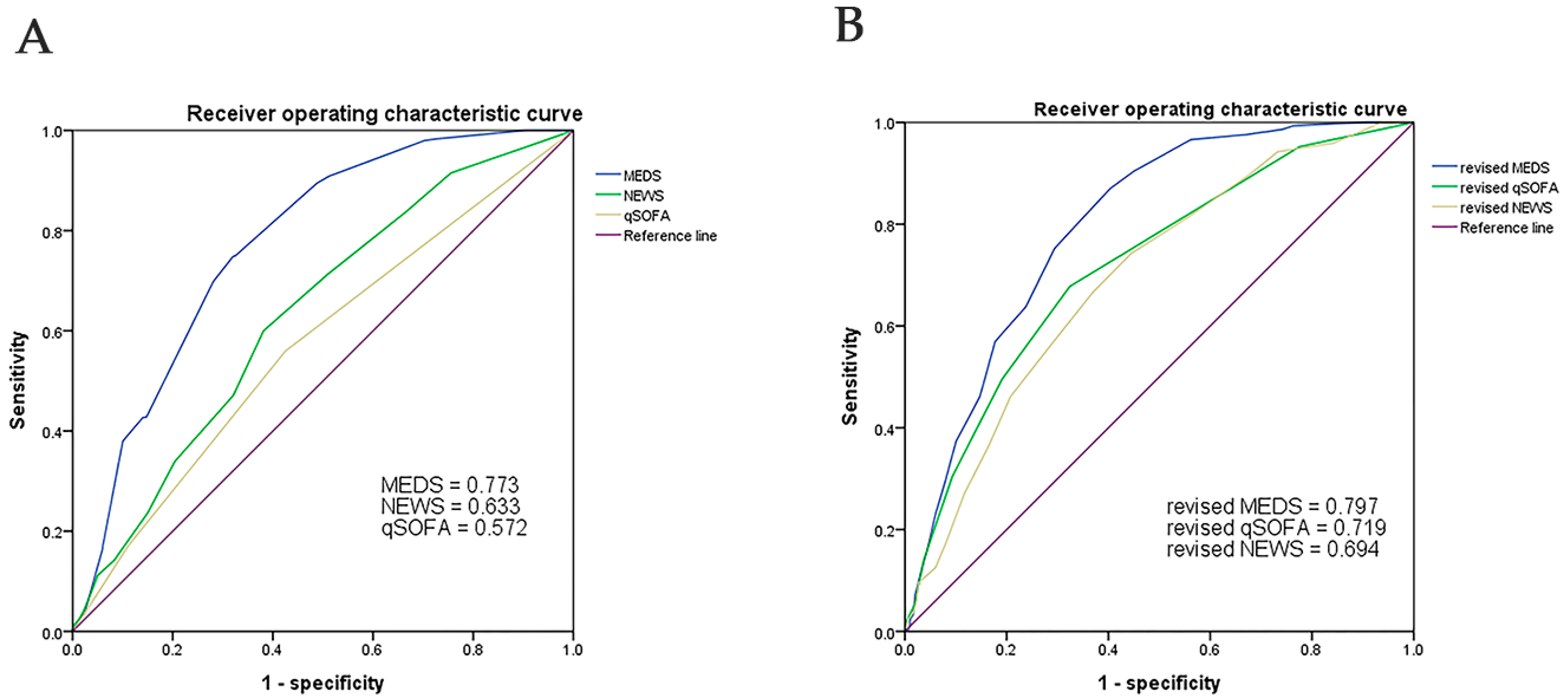
In this single-center retrospective study, we found that the non-survivors had higher scores of the original MEDS, NEWS, MEWS, qSOFA, and REMS than the survivors, which were associated with a higher risk of death on univariate logistic regression analyses. The original MEDS showed the best performance in predicting the mortality risk of adult patients with afebrile bacteremia caused by monomicrobial GNB. The AUC of the ROC of MEDS was 0.773 at a cut-off point of 11, with a sensitivity of 75% and a specificity of 68%. The qSOFA and NEWS demonstrated an acceptable performance in predicting the mortality risk, with the AUCs of the ROC of 0.633 and 0.572, respectively (
Figure 1).
Based on the univariate and multivariate analytic results of laboratory variables, we found that increased levels of RDW, high serum lactate, and low serum albumin were highly associated with the mortality rate (
Table 5 and
Table 6). Some studies suggested that RDW could be a risk variable in patients with sepsis and septic shock [
40,
41]. Serum lactate, acidosis, and hypoalbuminemia had clarified positive associations with the mortality rate in severe sepsis cases [
37,
42,
43,
44]. All these parameters were in the form of readily available data within 2 h during the ED workup. Therefore, we applied revisions of the original MEDS, qSOFA, and NEWS by adding scores of RDW (RDW > 16.5%, score = 1; RDW > 19.9%, score = 2), albumin (albumin < 3.0 g/dL, score = 1; albumin < 2.4 g/dL, score = 2), and lactate (lactate > 21 mg/dL, score = 1; lactate > 48 mg/dL, score = 2) to get a better performance than that of the original scoring systems. The revised MEDS (cut-off point of 11) remained the best performance in predicting mortality, with an AUC of the ROC of 0.797, a sensitivity of 87%, and a specificity of 60%. The revised qSOFA (cut-off point of 3) and NEWS (cut-off point of 6) simultaneously showed a superior performance than the original systems, with the AUCs of the ROC of 0.719 and 0.694, respectively. Our findings suggested that the original MEDS, revised MEDS, revised qSOFA, and revised NEWS were valuable tools for predicting the mortality risk in patients with afebrile bacteremia of monomicrobial GNB.





{kind=link}
{kind=link}
{kind=link}