Comparing the Japanese Version of the Ocular Surface Disease Index and Dry Eye-Related Quality-of-Life Score for Dry Eye Symptom Assessment

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Inclusion and Exclusion Criteria
2.3. Environmental Conditions
2.4. Dry Eye Symptom Assessment by the Questionnaires
2.5. Dry Eye Disease Diagnosis and Classification
2.6. Clinical Assessments
2.7. Sample Size Calculation
2.8. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Scores of the J-OSDI and DEQS (Frequency and Degree)
3.3. Correlation between the J-OSDI and DEQS
3.4. Comparison of the J-OSDI Total Score and DEQS (Frequency and Degree)
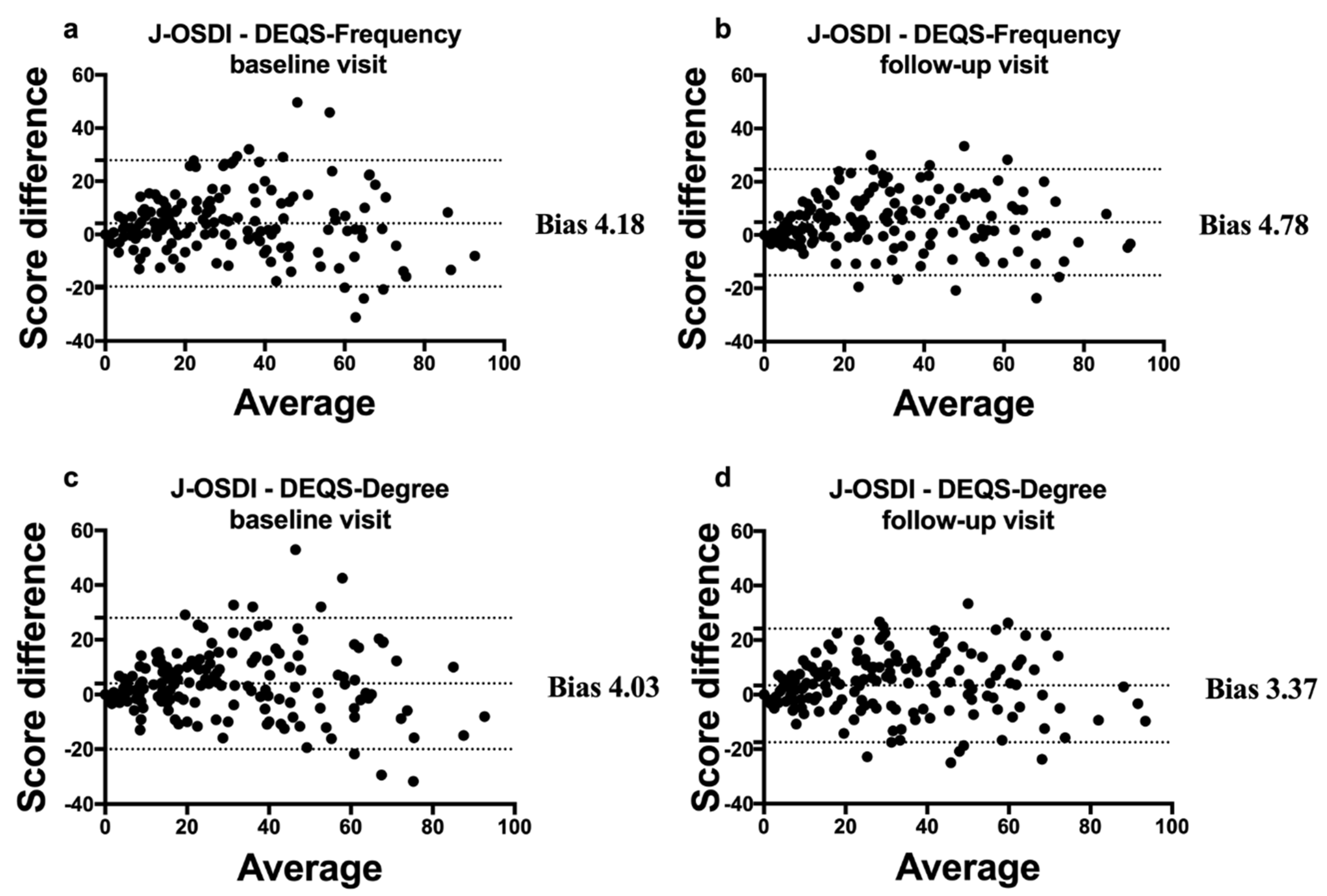
3.5. Bland–Altman Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef]
- Ding, J.; Sullivan, D.A. Aging and dry eye disease. Exp. Gerontol. 2012, 47, 483–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inomata, T.; Shiang, T.; Iwagami, M.; Sakemi, F.; Fujimoto, K.; Okumura, Y.; Ohno, M.; Murakami, A. Changes in Distribution of Dry Eye Disease by the New 2016 Diagnostic Criteria from the Asia Dry Eye Society. Sci. Rep. 2018, 8, 1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inomata, T.; Nakamura, M.; Iwagami, M.; Shiang, T.; Yoshimura, Y.; Fujimoto, K.; Okumura, Y.; Eguchi, A.; Iwata, N.; Miura, M.; et al. Risk Factors for Severe Dry Eye Disease: Crowdsourced Research Using DryEyeRhythm. Ophthalmology 2019, 126, 766–768. [Google Scholar] [CrossRef] [PubMed]
- Inomata, T.; Iwagami, M.; Nakamura, M.; Shiang, T.; Yoshimura, Y.; Fujimoto, K.; Okumura, Y.; Eguchi, A.; Iwata, N.; Miura, M.; et al. Characteristics and Risk Factors Associated With Diagnosed and Undiagnosed Symptomatic Dry Eye Using a Smartphone Application. JAMA Ophthalmol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Inomata, T.; Iwagami, M.; Nakamura, M.; Shiang, T.; Fujimoto, K.; Okumura, Y.; Iwata, N.; Fujio, K.; Hiratsuka, Y.; Hori, S.; et al. Association between Dry Eye and Depressive Symptoms: Large-Scale Crowdsourced Research Using the DryEyeRhythm iPhone Application. Ocul. Surf. 2020. [Google Scholar] [CrossRef] [PubMed]
- Goto, E.; Yagi, Y.; Matsumoto, Y.; Tsubota, K. Impaired functional visual acuity of dry eye patients. Am. J. Ophthalmol. 2002, 133, 181–186. [Google Scholar] [CrossRef]
- Kaido, M.; Ishida, R.; Dogru, M.; Tsubota, K. The relation of functional visual acuity measurement methodology to tear functions and ocular surface status. Jpn. J. Ophthalmol. 2011, 55, 451–459. [Google Scholar] [CrossRef]
- Heidari, M.; Noorizadeh, F.; Wu, K.; Inomata, T.; Mashaghi, A. Dry Eye Disease: Emerging Approaches to Disease Analysis and Therapy. J. Clin. Med. 2019, 8, 1439. [Google Scholar] [CrossRef] [Green Version]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Tsubota, K.; Yokoi, N.; Shimazaki, J.; Watanabe, H.; Dogru, M.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. New Perspectives on Dry Eye Definition and Diagnosis: A Consensus Report by the Asia Dry Eye Society. Ocul. Surf. 2017, 15, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Sakane, Y.; Yamaguchi, M.; Yokoi, N.; Uchino, M.; Dogru, M.; Oishi, T.; Ohashi, Y.; Ohashi, Y. Development and validation of the Dry Eye-Related Quality-of-Life Score questionnaire. JAMA Ophthalmol. 2013, 131, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Ngo, W.; Situ, P.; Keir, N.; Korb, D.; Blackie, C.; Simpson, T. Psychometric properties and validation of the Standard Patient Evaluation of Eye Dryness questionnaire. Cornea 2013, 32, 1204–1210. [Google Scholar] [CrossRef]
- Nichols, K.K.; Nichols, J.J.; Mitchell, G.L. The reliability and validity of McMonnies Dry Eye Index. Cornea 2004, 23, 365–371. [Google Scholar] [CrossRef]
- Midorikawa-Inomata, A.; Inomata, T.; Nojiri, S.; Nakamura, M.; Iwagami, M.; Fujimoto, K.; Okumura, Y.; Iwata, N.; Eguchi, A.; Hasegawa, H.; et al. Reliability and validity of the Japanese version of the Ocular Surface Disease Index for dry eye disease. BMJ Open 2019, 9, e033940. [Google Scholar] [CrossRef] [Green Version]
- Healthcare Engineering Association of Japan Standard Working Group. The Guideline for Design and Operation of Hospital HVAC Systems; Healthcare Engineering Association of Japan: Tokyo, Japan, 2013. [Google Scholar]
- Miller, K.L.; Walt, J.G.; Mink, D.R.; Satram-Hoang, S.; Wilson, S.E.; Perry, H.D.; Asbell, P.A.; Pflugfelder, S.C. Minimal clinically important difference for the ocular surface disease index. Arch. Ophthalmol. 2010, 128, 94–101. [Google Scholar] [CrossRef]
- Inomata, T.; Iwagami, M.; Hiratsuka, Y.; Fujimoto, K.; Okumura, Y.; Shiang, T.; Murakami, A. Maximum blink interval is associated with tear film breakup time: A new simple, screening test for dry eye disease. Sci. Rep. 2018, 8, 13443. [Google Scholar] [CrossRef] [Green Version]
- Van Bijsterveld, O.P. Diagnostic tests in the Sicca syndrome. Arch. Ophthalmol. 1969, 82, 10–14. [Google Scholar] [CrossRef]
- Hulley, S.B.; Browner, W.S.; Grady, D.; Newman, T.B. Designing Clinical Research: An Epidemiologic Approach, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; p. 79. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Lopez, A.D.; Murray, C.C. The global burden of disease, 1990–2020. Nat. Med. 1998, 4, 1241–1243. [Google Scholar] [CrossRef] [PubMed]
- Parasuraman, S.; Sam, A.T.; Yee, S.W.K.; Chuon, B.L.C.; Ren, L.Y. Smartphone usage and increased risk of mobile phone addiction: A concurrent study. Int. J. Pharm. Investig. 2017, 7, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, D.A.; Uchino, M.; Christen, W.G.; Semba, R.D.; Buring, J.E.; Li, J.Z. Patient reported differences in dry eye disease between men and women: Impact, management, and patient satisfaction. PLoS ONE 2013, 8, e76121. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Baseline | Follow-up | p Value |
|---|---|---|---|
| n = 169 | n = 169 | ||
| Age, years ± SD | 61.7 ± 14.1 | - | |
| Sex, female (%) | 143 (84.6) | - | |
| BCVA, logMAR ± SD | −0.066 ± 0.025 | −0.062 ± 0.031 | ** 0.004 |
| IOP, mmHg ± SD | 13.9 ± 2.9 | 13.5 ± 2.7 | 0.085 |
| TFBUT, second ± SD | 1.6 ± 1.6 | 1.6 ± 1.1 | 0.716 |
| CFS, 0–9 ± SD | 3.3 ± 2.6 | 3.5 ± 2.8 | 0.180 |
| Schirmer’s test I, mm ± SD | 4.8 ± 5.3 | 4.0 ± 4.9 | 0.785 |
| MBI, second ± SD | 11.4 ± 7.1 | 11.5 ± 7.1 | 0.866 |
| Baseline | Follow-up | |||
|---|---|---|---|---|
| DEQS | ||||
| J-OSDI, 0–100 | Frequency | Degree | Frequency | Degree |
| Normal (0–12) | 0.662 | 0.688 | 0.606 | 0.531 |
| Mild to moderate (13–32) | 0.665 | 0.462 | 0.358 | 0.378 |
| Severe (33–100) | 0.628 | 0.609 | 0.785 | 0.749 |
| J-OSDI | DEQS | |
|---|---|---|
| Purpose | Symptoms of ocular irritation consistent with DED and their impact on vision-related functioning | Symptoms and their effect on daily life |
| Development, year | 2000 | 2013 |
| Questions, number | 12 | 30 (Frequency and Degree) |
| Score | 0–100 | 0–100 |
| Cut-off value, score | ≥ 13 | > 15 |
| Severity classification | + | − |
| Validation in Japanese | + | + |
| Validation in English | + | − |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inomata, T.; Nakamura, M.; Iwagami, M.; Midorikawa-Inomata, A.; Okumura, Y.; Fujimoto, K.; Iwata, N.; Eguchi, A.; Shokirova, H.; Miura, M.; et al. Comparing the Japanese Version of the Ocular Surface Disease Index and Dry Eye-Related Quality-of-Life Score for Dry Eye Symptom Assessment. Diagnostics 2020, 10, 203. https://doi.org/10.3390/diagnostics10040203
Inomata T, Nakamura M, Iwagami M, Midorikawa-Inomata A, Okumura Y, Fujimoto K, Iwata N, Eguchi A, Shokirova H, Miura M, et al. Comparing the Japanese Version of the Ocular Surface Disease Index and Dry Eye-Related Quality-of-Life Score for Dry Eye Symptom Assessment. Diagnostics. 2020; 10(4):203. https://doi.org/10.3390/diagnostics10040203
Chicago/Turabian StyleInomata, Takenori, Masahiro Nakamura, Masao Iwagami, Akie Midorikawa-Inomata, Yuichi Okumura, Keiichi Fujimoto, Nanami Iwata, Atsuko Eguchi, Hurramhon Shokirova, Maria Miura, and et al. 2020. "Comparing the Japanese Version of the Ocular Surface Disease Index and Dry Eye-Related Quality-of-Life Score for Dry Eye Symptom Assessment" Diagnostics 10, no. 4: 203. https://doi.org/10.3390/diagnostics10040203