
Dual Antiplatelet Therapy: A Concise Review for Clinicians

 , ,
, ,
Abstract
:1. Introduction
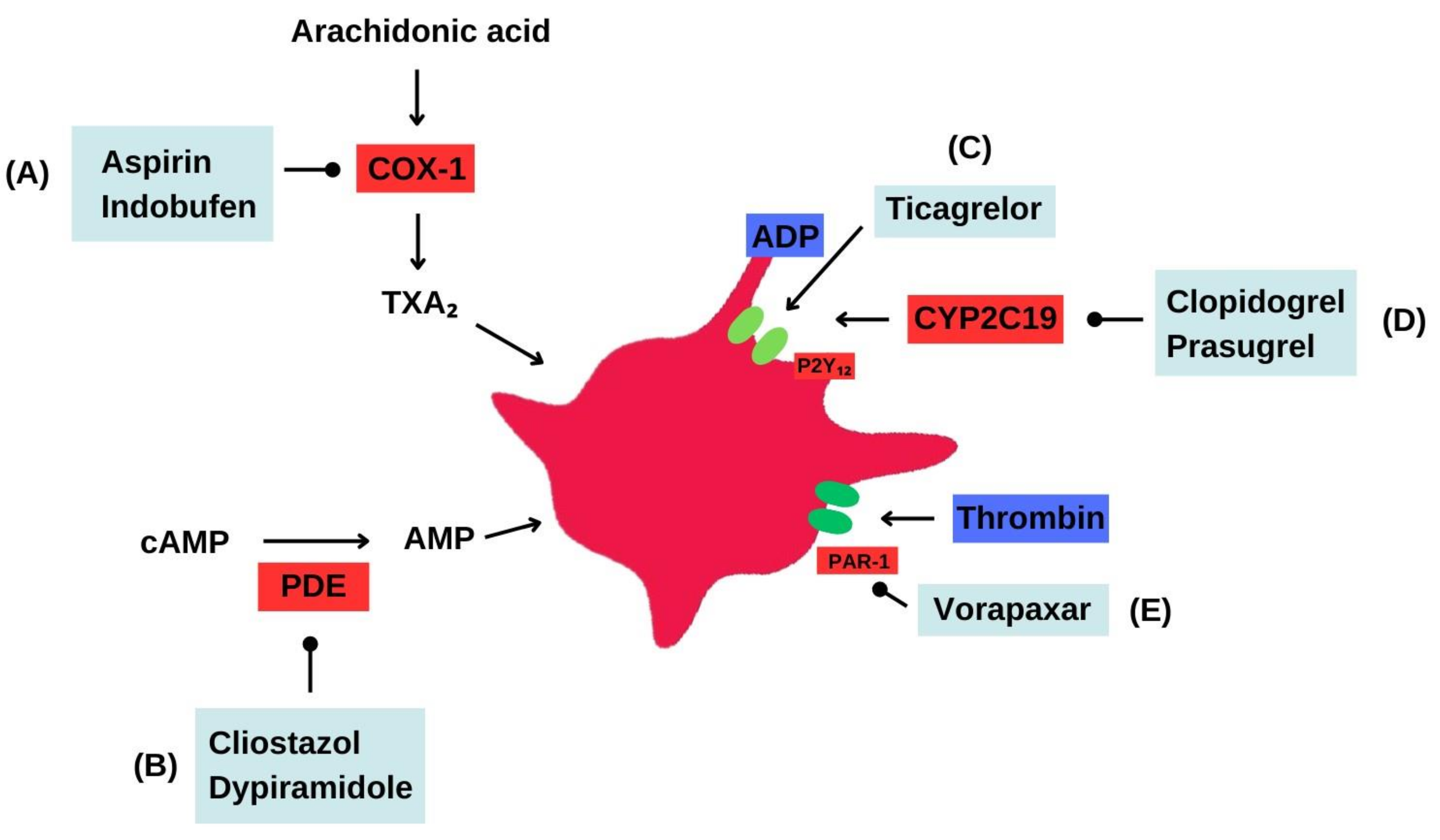
2. Overview of the Antiplatelet Therapies
2.1. Aspirin
2.2. Indobufen
2.3. P2Y12 Receptor Inhibitors
2.4. Clopidogrel
2.5. Prasugrel
2.6. Ticagrelor
2.7. Prasugrel vs. Ticagrelor
2.8. Dipyridamole
2.9. Cilostazol
2.10. Vorapaxar
3. Duration of Antiplatelet Therapy in ACS
3.1. Evidence for Short-Term Dual Antiplatelet Therapy
3.2. Evidence for Extended-Duration Dual Antiplatelet Therapy
4. Duration of Antiplatelet Therapy in Stable CAD
5. Duration of Antiplatelet Therapy in Post-PCI with Atrial Fibrillation in Addition to Anticoagulation
6. Duration of Antiplatelet Therapy in CABG
7. Duration of Antiplatelet Therapy Post TAVI
8. Duration of Antiplatelet Therapy in PAD
9. Duration of Antiplatelet Therapy in PAD Post-Peripheral Stent
10. Duration of Antiplatelet Therapy in Carotid Artery Disease
11. Duration of Antiplatelet Therapy in Carotid Artery Disease Post-Carotid Stent
12. Duration of Antiplatelet Therapy in Myocardial Infarction with Non-Obstructive Coronary Arteries
13. Duration of Antiplatelet Therapy in Spontaneous Coronary Artery Dissection
14. Resistance to Antiplatelet Agents
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jourdi, G.; Lordkipanidzé, M.; Philippe, A.; Bachelot-Loza, C.; Gaussem, P. Current and Novel Antiplatelet Therapies for the Treatment of Cardiovascular Diseases. Int. J. Mol. Sci. 2021, 22, 13079. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [PubMed]
- Urban, P.; Mehran, R.; Colleran, R.; Angiolillo, D.J.; Byrne, R.A.; Capodanno, D.; Cuisset, T.; Cutlip, D.; Eerdmans, P.; Eikelboom, J.; et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: A consensus document from the Academic Research Consortium for High Bleeding Risk. Eur. Heart J. 2019, 40, 2632–2653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biasco, L.; Montrasio, G.; Moccetti, M.; Pedrazzini, G. Current trends in dual antiplatelet therapy: A 2017 update. Cardiovasc. Med. 2017, 20, 169–175. [Google Scholar]
- Cairns, J.A.; Gent, M.; Singer, J.; Finnie, K.J.; Froggatt, G.M.; Holder, D.A.; Jablonsky, G.; Kostuk, W.J.; Melendez, L.J.; Myers, M.G.; et al. Aspirin, Sulfinpyrazone, or Both in Unstable Angina. N. Engl. J. Med. 1985, 313, 1369–1375. [Google Scholar] [CrossRef]
- Jones, W.S.; Mulder, H.; Wruck, L.M.; Pencina, M.J.; Kripalani, S.; Muñoz, D.; Crenshaw, D.L.; Effron, M.B.; Re, R.N.; Gupta, K.; et al. Comparative Effectiveness of Aspirin Dosing in Cardiovascular Disease. N. Engl. J. Med. 2021, 384, 1981–1990. [Google Scholar] [CrossRef]
- Byrne, R.A.; Colleran, R. Aspirin for secondary prevention of cardiovascular disease. Lancet 2020, 395, 1462–1463. [Google Scholar] [CrossRef]
- Patrono, C.; Baigent, C. Role of aspirin in primary prevention of cardiovascular disease. Nat. Rev. Cardiol. 2019, 16, 675–686. [Google Scholar] [CrossRef]
- Pan, Y.; Meng, X.; Chen, W.; Jing, J.; Lin, J.; Jiang, Y.; Johnston, S.C.; Bath, P.M.; Dong, Q.; Xu, A.-D.; et al. Indobufen versus aspirin in acute ischaemic stroke (INSURE): Rationale and design of a multicentre randomised trial. Stroke Vasc. Neurol. 2022, 7, e001480. [Google Scholar] [CrossRef]
- Bhana, N.; McClellan, K.J. Indobufen. Drugs Aging 2001, 18, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Xu, L.; Zhao, X.; Zhang, H.; Cheng, K.; Wang, X.; Chen, M.; Li, G.; Huang, J.; Lan, J.; et al. Indobufen or Aspirin on Top of Clopidogrel After Coronary Drug-Eluting Stent Implantation (OPTION): A Randomized, Open-Label, End Point–Blinded, Noninferiority Trial. Circulation 2023, 147, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Paciaroni, M.; Ince, B.; Hu, B.; Jeng, J.-S.; Kutluk, K.; Liu, L.; Lou, M.; Parfenov, V.; Wong, K.S.L.; Zamani, B.; et al. Benefits and Risks of Clopidogrel vs. Aspirin Monotherapy after Recent Ischemic Stroke: A Systematic Review and Meta-Analysis. Cardiovasc. Ther. 2019, 2019, 1607181. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [PubMed] [Green Version]
- Niitsu, Y.; Jakubowski, J.A.; Sugidachi, A.; Asai, F. Pharmacology of CS-747 (prasugrel, LY640315), a Novel, Potent Antiplatelet Agent with in Vivo P2Y12 Receptor Antagonist Activity. Semin. Thromb. Hemost. 2005, 31, 184–194. [Google Scholar] [CrossRef]
- Pradhan, A.; Tiwari, A.; Caminiti, G.; Salimei, C.; Muscoli, S.; Sethi, R.; Perrone, M.A. Ideal P2Y12 Inhibitor in Acute Coronary Syndrome: A Review and Current Status. Int. J. Environ. Res. Public Health 2022, 19, 8977. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.D.; Williams, A.K.; Lee, C.R.; Cavallari, L.H. Pharmacogenetics of P2Y12 receptor inhibitors. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2023, 43, 158–175. [Google Scholar] [CrossRef]
- Triska, J.; Maitra, N.; Deshotels, M.R.; Haddadin, F.; Angiolillo, D.J.; Vilahur, G.; Jneid, H.; Atar, D.; Birnbaum, Y. A Comprehensive Review of the Pleiotropic Effects of Ticagrelor. Cardiovasc. Drugs Ther. 2022, 1–23. [Google Scholar] [CrossRef]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Montalescot, G.; Van’t Hof, A.W.; Lapostolle, F.; Silvain, J.; Lassen, J.F.; Bolognese, L.; Cantor, W.J.; Cequier, Á.; Chettibi, M.; Goodman, S.G.; et al. Prehospital Ticagrelor in ST-Segment Elevation Myocardial Infarction. N. Engl. J. Med. 2014, 371, 1016–1027. [Google Scholar] [CrossRef] [Green Version]
- Schüpke, S.; Neumann, F.J.; Menichelli, M.; Mayer, K.; Bernlochner, I.; Wöhrle, J.; Richardt, G.; Liebetrau, C.; Witzenbichler, B.; Antoniucci, D.; et al. Ticagrelor or Prasugrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2019, 381, 1524–1534. [Google Scholar] [CrossRef]
- Aytekin, A.; Ndrepepa, G.; Neumann, F.-J.; Menichelli, M.; Mayer, K.; Wöhrle, J.; Bernlochner, I.; Lahu, S.; Richardt, G.; Witzenbichler, B.; et al. Ticagrelor or Prasugrel in Patients with ST-Segment–Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. Circulation 2020, 142, 2329–2337. [Google Scholar] [CrossRef] [PubMed]
- Belviso, N.; Aronow, H.D.; Wyss, R.; Barbour, M.; Zhang, Y.; Wen, X.; Kogut, S. Comparative effectiveness and safety of prasugrel versus ticagrelor following percutaneous coronary intervention: An observational study. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2021, 41, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Venetsanos, D.; Träff, E.; Erlinge, D.; Hagström, E.; Nilsson, J.; Desta, L.; Lindahl, B.; Mellbin, L.; Omerovic, E.; Szummer, K.E.; et al. Prasugrel versus ticagrelor in patients with myocardial infarction undergoing percutaneous coronary intervention. Heart 2021, 107, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Allahham, M.; Lerman, A.; Atar, D.; Birnbaum, Y. Why Not Dipyridamole: A Review of Current Guidelines and Re-evaluation of Utility in the Modern Era. Cardiovasc. Drugs Ther. 2021, 36, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Harker, L.A.; Kadatz, R.A. Mechanism of action of dipyridamole. Thromb. Res. Suppl. 1983, 29, 39–46. [Google Scholar] [CrossRef]
- Verro, P.; Gorelick, P.B.; Nguyen, D. Aspirin plus dipyridamole versus aspirin for prevention of vascular events after stroke or TIA: A meta-analysis. Stroke 2008, 39, 1358–1363. [Google Scholar] [CrossRef]
- Berger, J.S.; Krantz, M.J.; Kittelson, J.M.; Hiatt, W.R. Aspirin for the prevention of cardiovascular events in patients with peripheral artery disease: A meta-analysis of randomized trials. JAMA 2009, 301, 1909–1919. [Google Scholar] [CrossRef]
- Cilostazol: A Review of Basic Mechanisms and Clinical Uses-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/33860901/ (accessed on 21 April 2023).
- Kim, S.M.; Jung, J.M.; Kim, B.J.; Lee, J.S.; Kwon, S.U. Cilostazol Mono and Combination Treatments in Ischemic Stroke: An Updated Systematic Review and Meta-Analysis. Stroke 2019, 50, 3503–3511. [Google Scholar] [CrossRef]
- Matsumoto, M. Cilostazol in secondary prevention of stroke: Impact of the Cilostazol Stroke Prevention Study. Atheroscler. Suppl. 2005, 6, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, Y.; Katayama, Y.; Uchiyama, S.; Yamaguchi, T.; Handa, S.; Matsuoka, K.; Ohashi, Y.; Tanahashi, N.; Yamamoto, H.; Genka, C.; et al. Cilostazol for prevention of secondary stroke (CSPS 2): An aspirin-controlled, double-blind, randomised non-inferiority trial. Lancet Neurol. 2010, 9, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Reilly, M.; Mohler, E.R.; Mohler, I.E.R. Cilostazol: Treatment of Intermittent Claudication. Ann. Pharmacother. 2001, 35, 48–56. [Google Scholar] [CrossRef]
- Scirica, B.M.; Bonaca, M.P.; Braunwald, E.; De Ferrari, G.M.; Isaza, D.; Lewis, B.S.; Mehrhof, F.; Merlini, P.A.; Murphy, S.A.; Sabatine, M.S.; et al. Vorapaxar for secondary prevention of thrombotic events for patients with previous myocardial infarction: A prespecified subgroup analysis of the TRA 2°P-TIMI 50 trial. Lancet 2012, 380, 1317–1324. [Google Scholar] [CrossRef]
- Morrow, D.A.; Braunwald, E.; Bonaca, M.P.; Ameriso, S.F.; Dalby, A.J.; Fish, M.P.; Fox, K.A.A.; Lipka, L.J.; Liu, X.; Nicolau, J.C.; et al. Vorapaxar in the Secondary Prevention of Atherothrombotic Events. N. Engl. J. Med. 2012, 366, 1404–1413. [Google Scholar] [CrossRef]
- Tricoci, P.; Huang, Z.; Held, C.; Moliterno, D.J.; Armstrong, P.W.; Van de Werf, F.; White, H.D.; Aylward, P.E.; Wallentin, L.; Chen, E.; et al. Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary Syndromes. N. Engl. J. Med. 2012, 366, 20–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnani, G.; Bonaca, M.P.; Braunwald, E.; Dalby, A.J.; Fox, K.A.A.; Murphy, S.A.; Nicolau, J.C.; Ophuis, T.O.; Scirica, B.M.; Spinar, J.; et al. Efficacy and Safety of Vorapaxar as Approved for Clinical Use in the United States. J. Am. Heart Assoc. 2015, 4, e001505. Available online: https://www.ahajournals.org/doi/abs/10.1161/JAHA.114.001505 (accessed on 21 April 2023). [CrossRef] [Green Version]
- Misumida, N.; Abo-Aly, M.; Kim, S.M.; Ogunbayo, G.O.; Abdel-Latif, A.; Ziada, K.M. Efficacy and safety of short-term dual antiplatelet therapy (≤6 months) after percutaneous coronary intervention for acute coronary syndrome: A systematic review and meta-analysis of randomized controlled trials. Clin. Cardiol. 2018, 41, 1455–1462. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, H.; Morimoto, T.; Natsuaki, M.; Yamamoto, K.; Obayashi, Y.; Ogita, M.; Suwa, S.; Isawa, T.; Domei, T.; Yamaji, K.; et al. Comparison of Clopidogrel Monotherapy After 1 to 2 Months of Dual Antiplatelet Therapy with 12 Months of Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome: The STOPDAPT-2 ACS Randomized Clinical Trial. JAMA Cardiol. 2022, 7, 407–417. [Google Scholar] [CrossRef]
- Kuno, T.; Ueyama, H.; Takagi, H.; Fox, J.; Bangalore, S. Optimal Duration of Dual Antiplatelet Therapy After Percutaneous Coronary Intervention in Patients with Acute Coronary Syndrome: Insights from a Network Meta-Analysis of Randomized Trials. Cardiovasc. Revasc. Med. 2020, 28, 50–56. [Google Scholar] [CrossRef]
- Lee, S.Y.; Hong, M.K.; Palmerini, T.; Kim, H.S.; Valgimigli, M.; Feres, F.; Colombo, A.; Gilard, M.; Shin, D.H.; Kim, J.S.; et al. Short-Term Versus Long-Term Dual Antiplatelet Therapy After Drug-Eluting Stent Implantation in Elderly Patients. JACC Cardiovasc. Interv. 2018, 11, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Ki, Y.-J.; Kang, J.; Park, J.; Han, J.-K.; Yang, H.-M.; Park, K.W.; Kang, H.-J.; Koo, B.-K.; Kim, H.-S. Efficacy and Safety of Long-Term and Short-Term Dual Antiplatelet Therapy: A Meta-Analysis of Comparison between Asians and Non-Asians. J. Clin. Med. 2020, 9, 652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdoia, M.; Suryapranata, H.; Damen, S.; Camaro, C.; Benit, E.; Barbieri, L.; Rasoul, S.; Liew, H.B.; Polad, J.; Ahmad, W.A.W.; et al. Gender differences with short-term vs. 12 months dual antiplatelet therapy in patients with acute coronary syndrome treated with the COMBO dual therapy stent: 2-years follow-up results of the REDUCE trial. J. Thromb. Thrombolysis 2021, 52, 797–807. [Google Scholar] [CrossRef]
- Hahn, J.Y.; Song, Y.B.; Oh, J.H.; Chun, W.J.; Park, Y.H.; Jang, W.J.; Im, E.S.; Jeong, J.O.; Cho, B.R.; Oh, S.K.; et al. Effect of P2Y12 Inhibitor Monotherapy vs. Dual Antiplatelet Therapy on Cardiovascular Events in Patients Undergoing Percutaneous Coronary Intervention: The SMART-CHOICE Randomized Clinical Trial. JAMA 2019, 321, 2428–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E.; Ganiats, T.G.; Holmes, D.R.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non–ST-Elevation Acute Coronary Syndromes. Circulation 2014, 130, e344–e426. [Google Scholar] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.-L.T.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef] [Green Version]
- Koo, B.-K.; Kang, J.; Park, K.W.; Rhee, T.-M.; Yang, H.-M.; Won, K.-B.; Rha, S.-W.; Bae, J.-W.; Lee, N.H.; Hur, S.-H.; et al. Aspirin versus clopidogrel for chronic maintenance monotherapy after percutaneous coronary intervention (HOST-EXAM): An investigator-initiated, prospective, randomised, open-label, multicentre trial. Lancet 2021, 397, 2487–2496. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Fox, K.A.; Hacke, W.; Berger, P.B.; Black, H.R.; Boden, W.E.; Cacoub, P.; Cohen, E.A.; Creager, M.A.; Easton, J.D.; et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. Am. J. Ophthalmol. 2006, 142, 366. [Google Scholar] [CrossRef] [Green Version]
- Steg, P.G.; Bhatt, D.L.; Simon, T.; Fox, K.; Mehta, S.R.; Harrington, R.A.; Held, C.; Andersson, M.; Himmelmann, A.; Ridderstråle, W.; et al. Ticagrelor in Patients with Stable Coronary Disease and Diabetes. N. Engl. J. Med. 2019, 381, 1309–1320. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, D.L.; Steg, P.G.; Mehta, S.R.; Leiter, L.A.; Simon, T.; Fox, K.; Held, C.; Andersson, M.; Himmelmann, A.; Ridderstråle, W.; et al. Ticagrelor in patients with diabetes and stable coronary artery disease with a history of previous percutaneous coronary intervention (THEMIS-PCI): A phase 3, placebo-controlled, randomised trial. Lancet 2019, 394, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs. aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: A multicentre, open-label, randomised superiority trial. Lancet 2018, 392, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 151–226. [Google Scholar] [CrossRef] [Green Version]
- Members, W.C.; Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar]
- Lip, G.Y.H.; Collet, J.-P.; Haude, M.; Byrne, R.; Chung, E.H.; Fauchier, L.; Halvorsen, S.; Lau, D.; Lopez-Cabanillas, N.; Lettino, M.; et al. 2018 Joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions: A joint consensus document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA). EP Eur. 2018, 21, 192–193. [Google Scholar] [CrossRef]
- Davidson, L.J.; Davidson, C.J. Transcatheter Treatment of Valvular Heart Disease: A Review. JAMA 2021, 325, 2480–2494. [Google Scholar] [CrossRef]
- Saito, Y.; Nazif, T.; Baumbach, A.; Tchétché, D.; Latib, A.; Kaple, R.; Forrest, J.; Prendergast, B.; Lansky, A. Adjunctive Antithrombotic Therapy for Patients with Aortic Stenosis Undergoing Transcatheter Aortic Valve Replacement. JAMA Cardiol. 2020, 5, 92. [Google Scholar] [CrossRef]
- Kuno, T.; Yokoyama, Y.; Briasoulis, A.; Mori, M.; Iwagami, M.; Ando, T.; Takagi, H.; Bangalore, S. Duration of Antiplatelet Therapy Following Transcatheter Aortic Valve Replacement: Systematic Review and Network Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e019490. [Google Scholar] [CrossRef]
- Kobari, Y.; Inohara, T.; Saito, T.; Yoshijima, N.; Tanaka, M.; Tsuruta, H.; Yashima, F.; Shimizu, H.; Fukuda, K.; Naganuma, T.; et al. Aspirin Versus Clopidogrel as Single Antithrombotic Therapy After Transcatheter Aortic Valve Replacement: Insight from the OCEAN-TAVI Registry. Circ. Cardiovasc. Interv. 2021, 14, e010097. [Google Scholar] [CrossRef]
- Ambler, G.K.; Waldron, C.; Contractor, U.B.; Hinchliffe, R.J.; Twine, C.P. Umbrella review and meta-analysis of antiplatelet therapy for peripheral artery disease. Br. J. Surg. 2020, 107, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Gutierrez, J.A.; Creager, M.A.; Scirica, B.M.; Olin, J.; Murphy, S.A.; Braunwald, E.; Morrow, D.A. Vorapaxar in Patients with Peripheral Artery Disease. Circulation 2016, 133, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Zimet, R.; Forbes, W.P.; Zhang, P. Meta-analysis of results from eight randomized, placebo-controlled trials on the effect of cilostazol on patients with intermittent claudication. Am. J. Cardiol. 2002, 90, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Pande, R.L.; Hiatt, W.R.; Zhang, P.; Hittel, N.; Creager, M.A. A pooled analysis of the durability and predictors of treatment response of cilostazol in patients with intermittent claudication. Vasc. Med. 2010, 15, 181–188. [Google Scholar] [CrossRef]
- Stevens, J.W.; Simpson, E.; Harnan, S.; Squires, H.; Meng, Y.; Thomas, S.; Michaels, J.; Stansby, G. Systematic review of the efficacy of cilostazol, naftidrofuryl oxalate and pentoxifylline for the treatment of intermittent claudication. Br. J. Surg. 2012, 99, 1630–1638. [Google Scholar] [CrossRef] [PubMed]
- Bedenis, R.; Stewart, M.; Cleanthis, M.; Robless, P.; Mikhailidis, D.P.; Stansby, G. Cilostazol for intermittent claudication. Cochrane Database Syst. Rev. 2014, 2014, CD003748. [Google Scholar] [CrossRef]
- Balsano, F.; Violi, F. Effect of picotamide on the clinical progression of peripheral vascular disease. A double-blind placebo-controlled study. The ADEP Group. Circulation 1993, 87, 1563–1569. [Google Scholar] [CrossRef] [Green Version]
- Arcan, J.; Blanchard, J.; Boissel, J.; Destors, J.; Panak, E. Multicenter Double-Blind Study of Ticlopidine in the Treatment of Intermittent Claudication and the Prevention of its Complications. Angiology 1988, 39, 802–811. [Google Scholar] [CrossRef]
- Aukland, A.; Hurlow, R.A.; George, A.J.; Stuart, J. Platelet inhibition with Ticlopidine in atherosclerotic intermittent claudication. J. Clin. Pathol. 1982, 35, 740–743. [Google Scholar] [CrossRef] [Green Version]
- Blanchard, J.; Carreras, L.O.; Kindermans, M. Results of EMATAP: A double-blind placebo-controlled multicentre trial of ticlopidine in patients with peripheral arterial disease. Nouv. Rev. Fr. Hematol. 1994, 35, 523–528. [Google Scholar]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e686–e725. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [PubMed] [Green Version]
- Strobl, F.F.; Brechtel, K.; Schmehl, J.; Zeller, T.; Reiser, M.F.; Claussen, C.D.; Tepe, G. Twelve-Month Results of a Randomized Trial Comparing Mono with Dual Antiplatelet Therapy in Endovascularly Treated Patients with Peripheral Artery Disease. J. Endovasc. Ther. 2013, 20, 699–706. [Google Scholar] [CrossRef]
- Tepe, G.; Bantleon, R.; Brechtel, K.; Schmehl, J.; Zeller, T.; Claussen, C.D.; Strobl, F.F. Management of peripheral arterial interventions with mono or dual antiplatelet therapy—The MIRROR study: A randomised and double-blinded clinical trial. Eur. Radiol. 2012, 22, 1998–2006. [Google Scholar] [CrossRef] [PubMed]
- Markus, H.S.; Droste, D.W.; Kaps, M.; Larrue, V.; Lees, K.R.; Siebler, M.; Ringelstein, E.B. Dual Antiplatelet Therapy with Clopidogrel and Aspirin in Symptomatic Carotid Stenosis Evaluated Using Doppler Embolic Signal Detection. Circulation 2005, 111, 2233–2240. [Google Scholar] [CrossRef] [PubMed]
- Paciaroni, M.; Bogousslavsky, J. Antithrombotic Therapy in Carotid Artery Stenosis: An Update. Eur. Neurol. 2015, 73, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.S.L.; Chen, C.; Fu, J.; Chang, H.M.; Suwanwela, N.C.; Huang, Y.N.; Han, Z.; Tan, K.S.; Ratanakorn, D.; Chollate, P.; et al. Clopidogrel plus aspirin versus aspirin alone for reducing embolisation in patients with acute symptomatic cerebral or carotid artery stenosis (CLAIR study): A randomised, open-label, blinded-endpoint trial. Lancet Neurol. 2010, 9, 489–497. [Google Scholar] [CrossRef]
- Naylor, R.; Rantner, B.; Ancetti, S.; de Borst, G.J.; De Carlo, M.; Halliday, A.; Kakkos, S.K.; Markus, H.S.; McCabe, D.J.; Sillesen, H.; et al. Editor’s Choice–European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on the Management of Atherosclerotic Carotid and Vertebral Artery Disease. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 7–111. [Google Scholar] [CrossRef]
- Dalainas, I.; Nano, G.; Bianchi, P.; Stegher, S.; Malacrida, G.; Tealdi, D.G. Dual Antiplatelet Regime Versus Acetyl-acetic Acid for Carotid Artery Stenting. Cardiovasc. Interv. Radiol. 2006, 29, 519–521. [Google Scholar] [CrossRef]
- McKevitt, F.; Randall, M.; Cleveland, T.; Gaines, P.; Tan, K.; Venables, G. The Benefits of Combined Anti-platelet Treatment in Carotid Artery Stenting. Eur. J. Vasc. Endovasc. Surg. 2005, 29, 522–527. [Google Scholar] [CrossRef] [Green Version]
- Abdu, F.A.; Mohammed, A.-Q.; Liu, L.; Xu, Y.; Che, W. Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): A Review of the Current Position. Cardiology 2020, 145, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Bossard, M.; Gao, P.; Boden, W.; Steg, G.; Tanguay, J.F.; Joyner, C.; Granger, C.B.; Kastrati, A.; Faxon, D.; Budaj, A.; et al. Antiplatelet therapy in patients with myocardial infarction without obstructive coronary artery disease. Heart 2021, 107, 1739–1747. [Google Scholar] [CrossRef]
- Lindahl, B.; Baron, T.; Erlinge, D.; Hadziosmanovic, N.; Nordenskjöld, A.; Gard, A.; Jernberg, T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients with Myocardial Infarction with Nonobstructive Coronary Artery Disease. Circulation 2017, 135, 1481–1489. [Google Scholar] [CrossRef]
- Abdu, F.A.; Liu, L.; Mohammed, A.-Q.; Xu, B.; Yin, G.; Xu, S.; Xu, Y.; Che, W. Effect of Secondary Prevention Medication on the Prognosis in Patients with Myocardial Infarction with Nonobstructive Coronary Artery Disease. J. Cardiovasc. Pharmacol. 2020, 76, 678–683. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Saturi, G.; D’Angelo, E.C.; Magnani, I.; Toniolo, S.; Stefanizzi, A.; Rinaldi, A.; Bartoli, L.; Angeli, F.; et al. Secondary Prevention Medical Therapy and Outcomes in Patients with Myocardial Infarction with Non-Obstructive Coronary Artery Disease. Front. Pharmacol. 2019, 10, 1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciliberti, G.; Verdoia, M.; Merlo, M.; Zilio, F.; Vatrano, M.; Bianco, F.; Mancone, M.; Zaffalon, D.; Bonci, A.; Boscutti, A.; et al. Pharmacological therapy for the prevention of cardiovascular events in patients with myocardial infarction with non-obstructed coronary arteries (MINOCA): Insights from a multicentre national registry. Int. J. Cardiol. 2021, 327, 9–14. [Google Scholar] [CrossRef]
- Kim, E.S.H. Spontaneous Coronary-Artery Dissection. N. Engl. J. Med. 2020, 383, 2358–2370. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Starovoytov, A.; Humphries, K.; Sheth, T.; So, D.; Minhas, K.; Brass, N.; Lavoie, A.; Bishop, H.; Lavi, S.; et al. Canadian spontaneous coronary artery dissection cohort study: In-hospital and 30-day outcomes. Eur. Heart J. 2019, 40, 1188–1197. [Google Scholar] [CrossRef] [Green Version]
- Adlam, D.; Alfonso, F.; Maas, A.; Vrints, C.; Writing Committee. European Society of Cardiology, acute cardiovascular care association, SCAD study group: A position paper on spontaneous coronary artery dissection. Eur. Heart J. 2018, 39, 3353–3368. [Google Scholar] [CrossRef]
- Cerrato, E.; Giacobbe, F.; Quadri, G.; Macaya, F.; Bianco, M.; Mori, R.; Biolè, C.A.; Boi, A.; Bettari, L.; Rolfo, C.; et al. Antiplatelet therapy in patients with conservatively managed spontaneous coronary artery dissection from the multicentre DISCO registry. Eur. Heart J. 2021, 42, 3161–3171. [Google Scholar] [CrossRef]
- Hayes, S.N.; Kim, E.S.; Saw, J.; Adlam, D.; Arslanian-Engoren, C.; Economy, K.E.; Ganesh, S.K.; Gulati, R.; Lindsay, M.E.; Mieres, J.H.; et al. Spontaneous Coronary Artery Dissection: Current State of the Science: A Scientific Statement from the American Heart Association. Circulation 2018, 137, e523–e557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breet, N.J.; van Werkum, J.W.; Bouman, H.J.; Kelder, J.C.; Ruven, H.J.T.; Bal, E.T.; Deneer, V.H.; Harmsze, A.M.; van der Heyden, J.A.S.; Rensing, B.J.W.M.; et al. Comparison of Platelet Function Tests in Predicting Clinical Outcome in Patients Undergoing Coronary Stent Implantation. JAMA 2010, 303, 754–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michelson, A.D.; Cattaneo, M.; Eikelboom, J.W.; Gurbel, P.; Kunicki, T.J.; Pulcinelli, F.M.; Cerletti, C.; Rao, A.K.; Kottke-Marchant, K. Aspirin resistance: Position paper of the Working Group on Aspirin Resistance. J. Thromb. Haemost. 2005, 3, 1309–1311. [Google Scholar] [CrossRef]
- Chen, W.-H.; Cheng, X.; Lee, P.-Y.; Ng, W.; Kwok, J.Y.-Y.; Tse, H.-F.; Lau, C.-P. Aspirin Resistance and Adverse Clinical Events in Patients with Coronary Artery Disease. Am. J. Med. 2007, 120, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Gum, P.A.; Kottke-Marchant, K.; Welsh, P.A.; White, J.; Topol, E.J. A prospective, blinded determination of the natural history of aspirin resistance among stable patients with cardiovascular disease. J. Am. Coll. Cardiol. 2003, 41, 961–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garabedian, T.; Alam, S. High residual platelet reactivity on clopidogrel: Its significance and therapeutic challenges overcoming clopidogrel resistance. Cardiovasc. Diagn. Ther. 2013, 3, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Bonello, L.; Tantry, U.S.; Marcucci, R.; Blindt, R.; Angiolillo, D.J.; Becker, R.; Bhatt, D.L.; Cattaneo, M.; Collet, J.P.; Cuisset, T.; et al. Consensus and Future Directions on the Definition of High On-Treatment Platelet Reactivity to Adenosine Diphosphate. J. Am. Coll. Cardiol. 2010, 56, 919–933. [Google Scholar] [CrossRef] [Green Version]
- Gurbel, P.A.; Bliden, K.P.; Hiatt, B.L.; O’connor, C.M. Clopidogrel for Coronary Stenting. Circulation 2003, 107, 2908–2913. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Medication | Properties | Dose | Adverse Effects | Contraindications |
|---|---|---|---|---|
| Inhibitor of the enzyme cyclooxygenase-1 (COX-1) | ||||
| Aspirin | Antiplatelet, analgesic, antipyretic | 75–325 mg/day | Bleeding, gastrointestinal ulcers, tinnitus, Reye’s syndrome | Hypersensitivity, active bleeding, history of bleeding disorders, recent surgery |
| Indobufen | Antiplatelet | 200–300 mg/day | Bleeding, gastrointestinal ulcers, dyspepsia | Hypersensitivity, active bleeding, history of bleeding disorders |
| P2Y12 receptor inhibitors | ||||
| Clopidogrel | Antiplatelet | 75 mg/day | Bleeding, gastrointestinal ulcers, thrombotic thrombocytopenic purpura | Hypersensitivity, active bleeding, history of bleeding disorders |
| Prasugrel | Antiplatelet | 10 mg/day | Bleeding, gastrointestinal ulcers | Hypersensitivity, active bleeding, history of bleeding disorders, previous stroke or transient ischemic attack |
| Ticagrelor | Antiplatelet | 90 mg/twice daily | Bleeding, gastrointestinal ulcers, dyspnea | Hypersensitivity, active bleeding, history of bleeding disorders |
| Phosphodiesterase inhibitors | ||||
| Dipyridamole | Antiplatelet, vasodilator | 200–400 mg/day | Headache, gastrointestinal upset, hypotension | Hypersensitivity, active bleeding, history of bleeding disorders |
| Cilostazol | Antiplatelet, vasodilator | 100 mg/twice daily | Headache, gastrointestinal upset, hypotension | Heart failure, bleeding disorders, recent myocardial infarction |
| Protease-activated receptor-1 antagonists | ||||
| Vorapaxar | Antiplatelet | 2.08 mg/day | Bleeding, gastrointestinal ulcers, intracranial hemorrhage | History of stroke, transient ischemic attack, bleeding disorders |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virk, H.U.H.; Escobar, J.; Rodriguez, M.; Bates, E.R.; Khalid, U.; Jneid, H.; Birnbaum, Y.; Levine, G.N.; Smith, S.C., Jr.; Krittanawong, C. Dual Antiplatelet Therapy: A Concise Review for Clinicians. Life 2023, 13, 1580. https://doi.org/10.3390/life13071580
Virk HUH, Escobar J, Rodriguez M, Bates ER, Khalid U, Jneid H, Birnbaum Y, Levine GN, Smith SC Jr., Krittanawong C. Dual Antiplatelet Therapy: A Concise Review for Clinicians. Life. 2023; 13(7):1580. https://doi.org/10.3390/life13071580
Chicago/Turabian StyleVirk, Hafeez Ul Hassan, Johao Escobar, Mario Rodriguez, Eric R. Bates, Umair Khalid, Hani Jneid, Yochai Birnbaum, Glenn N. Levine, Sidney C. Smith, Jr., and Chayakrit Krittanawong. 2023. "Dual Antiplatelet Therapy: A Concise Review for Clinicians" Life 13, no. 7: 1580. https://doi.org/10.3390/life13071580