Adipose Mesenchymal Extracellular Vesicles as Alpha-1-Antitrypsin Physiological Delivery Systems for Lung Regeneration

 ,
,  , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Lyo-Secretome Preparation
2.2.1. Cell Culture and Secretome Collection
2.2.2. MSC-Secretome Concentration, Purification, and Lyophilization
2.2.3. MSC-Secretome Fraction Separation and Freeze-Drying
2.3. Lyo-Secretome and Secretome Fractions Characterization
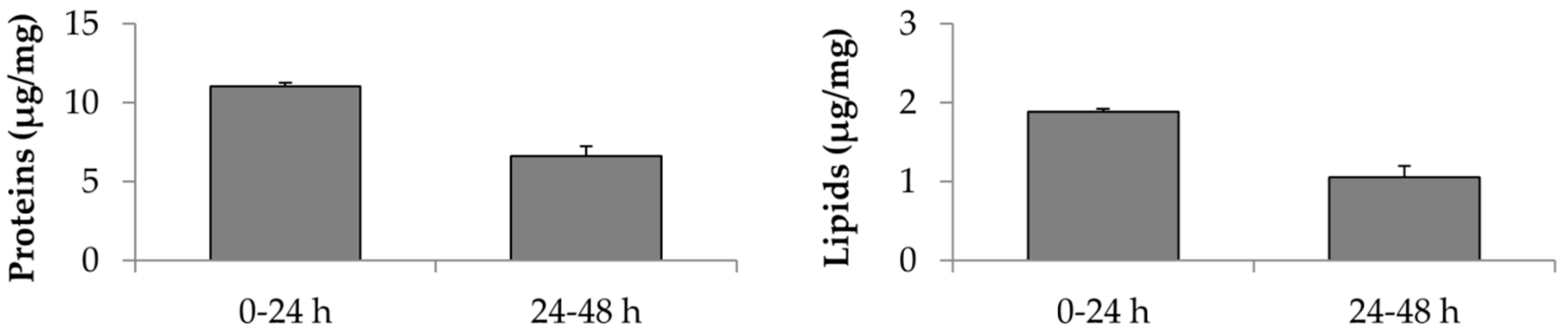
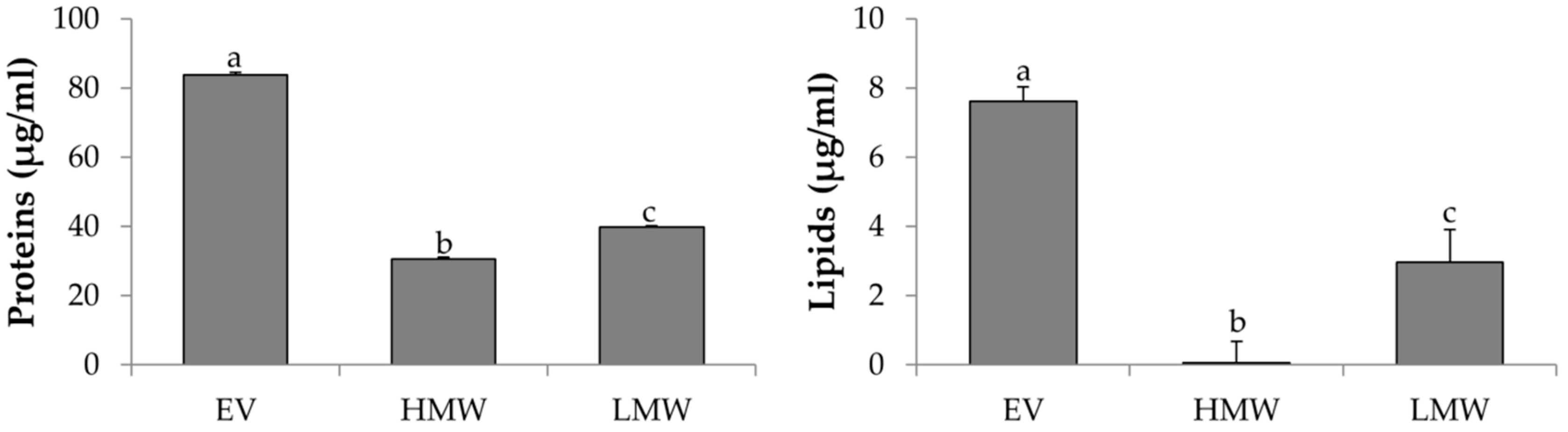
2.3.1. Total Protein Content
2.3.2. Total Lipid Content
2.3.3. Alpha-1-Antitrypsin Dosage
2.3.4. Physical-Chemical Characterization
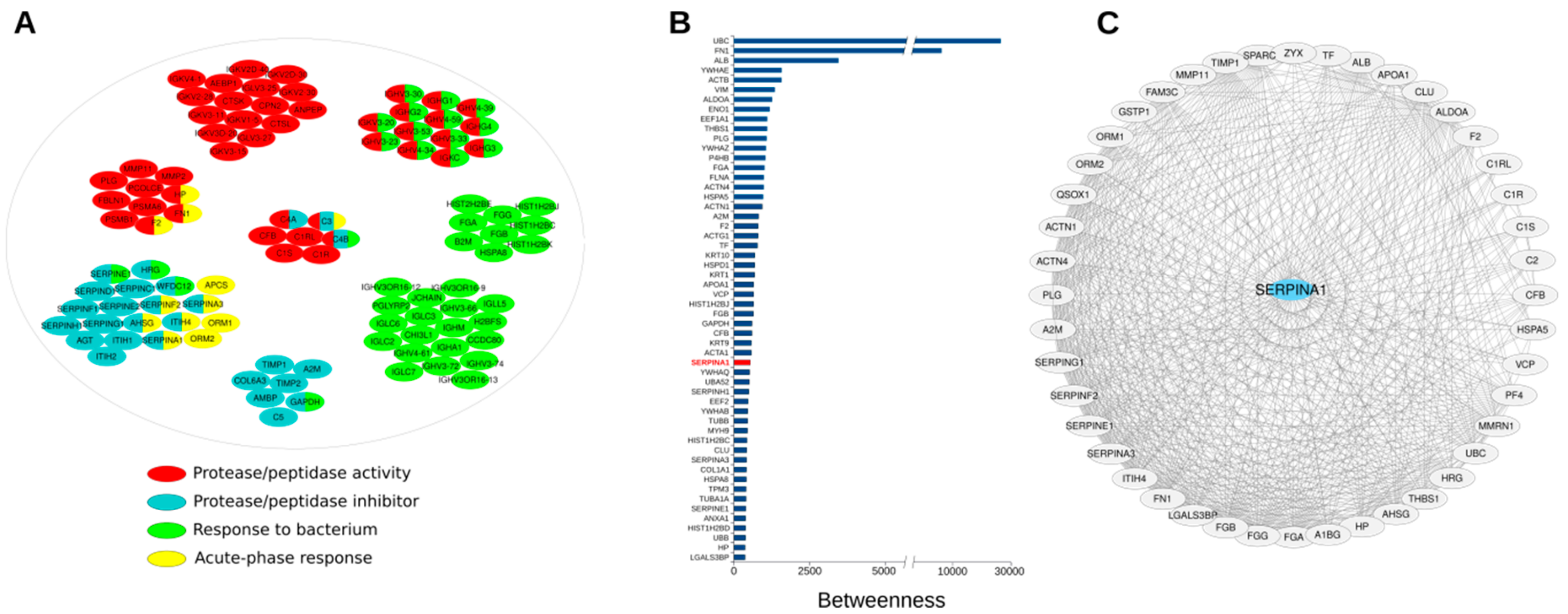
2.3.5. Network Analysis
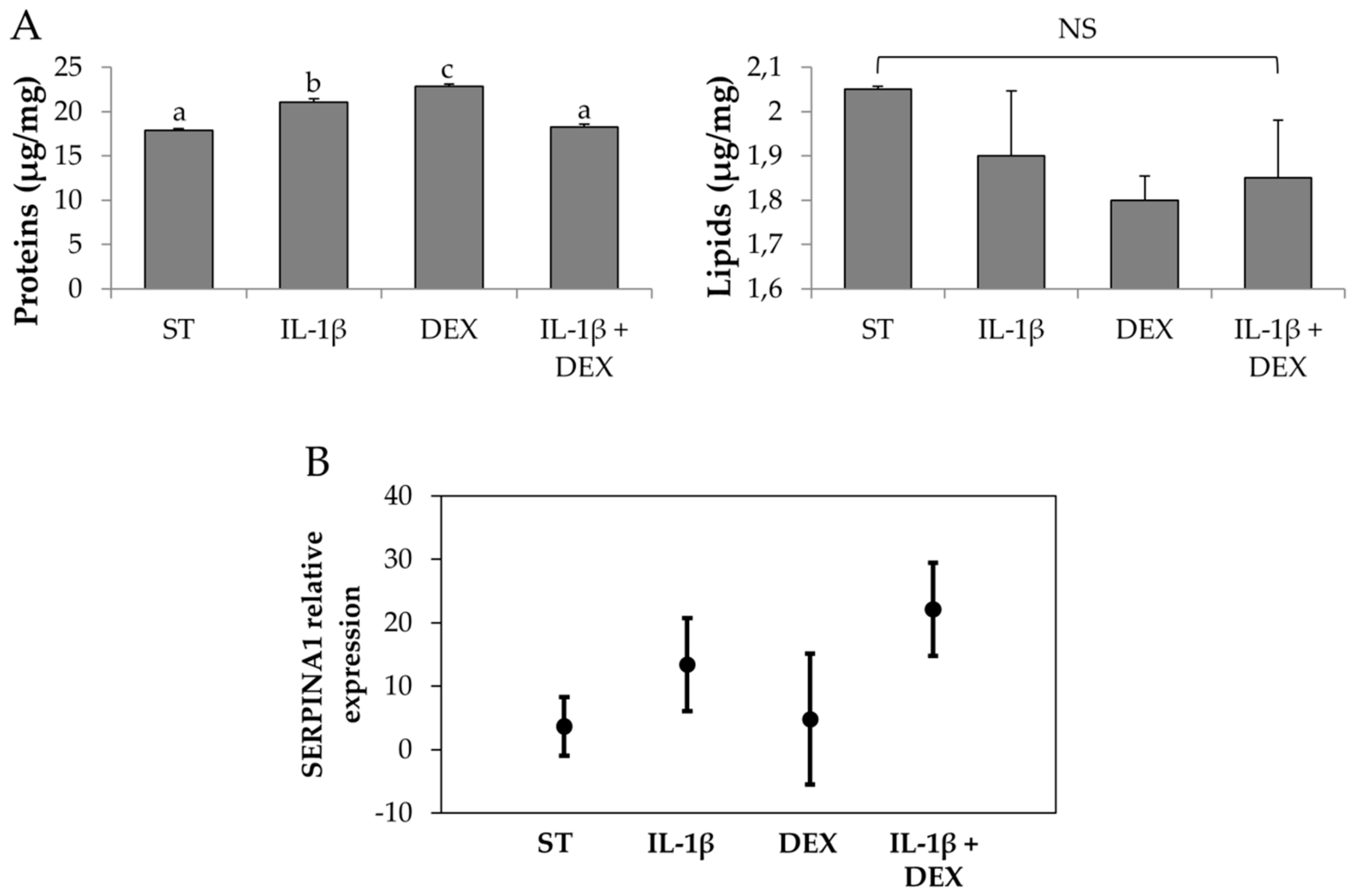
2.4. Stimulated-Secretome Preparation and Characterization
Evaluation of AAT Gene Expression in AD-MSCs
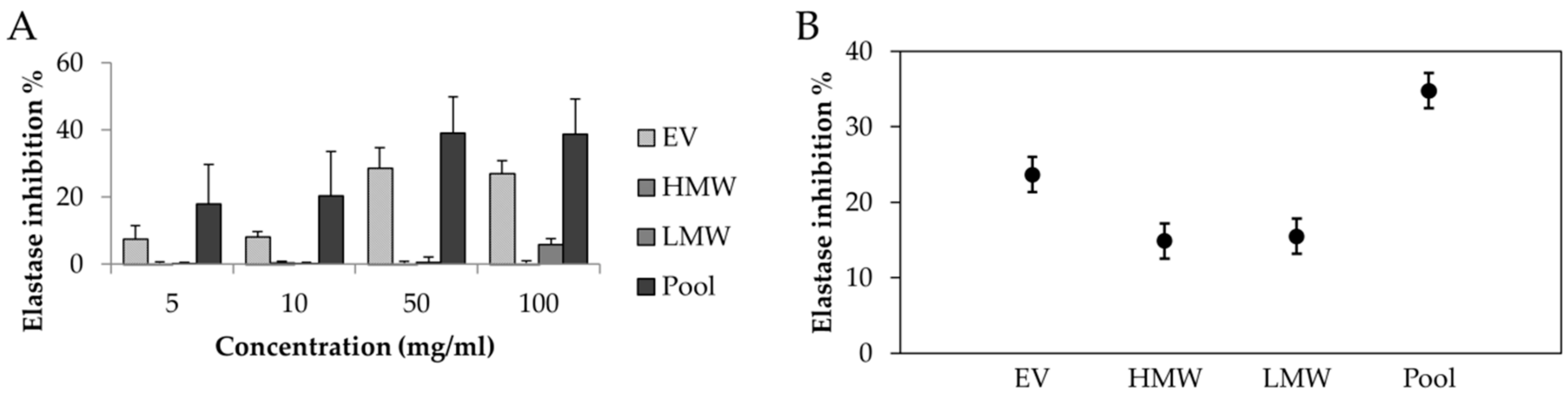
2.5. In Vitro Anti-Elastase Activity
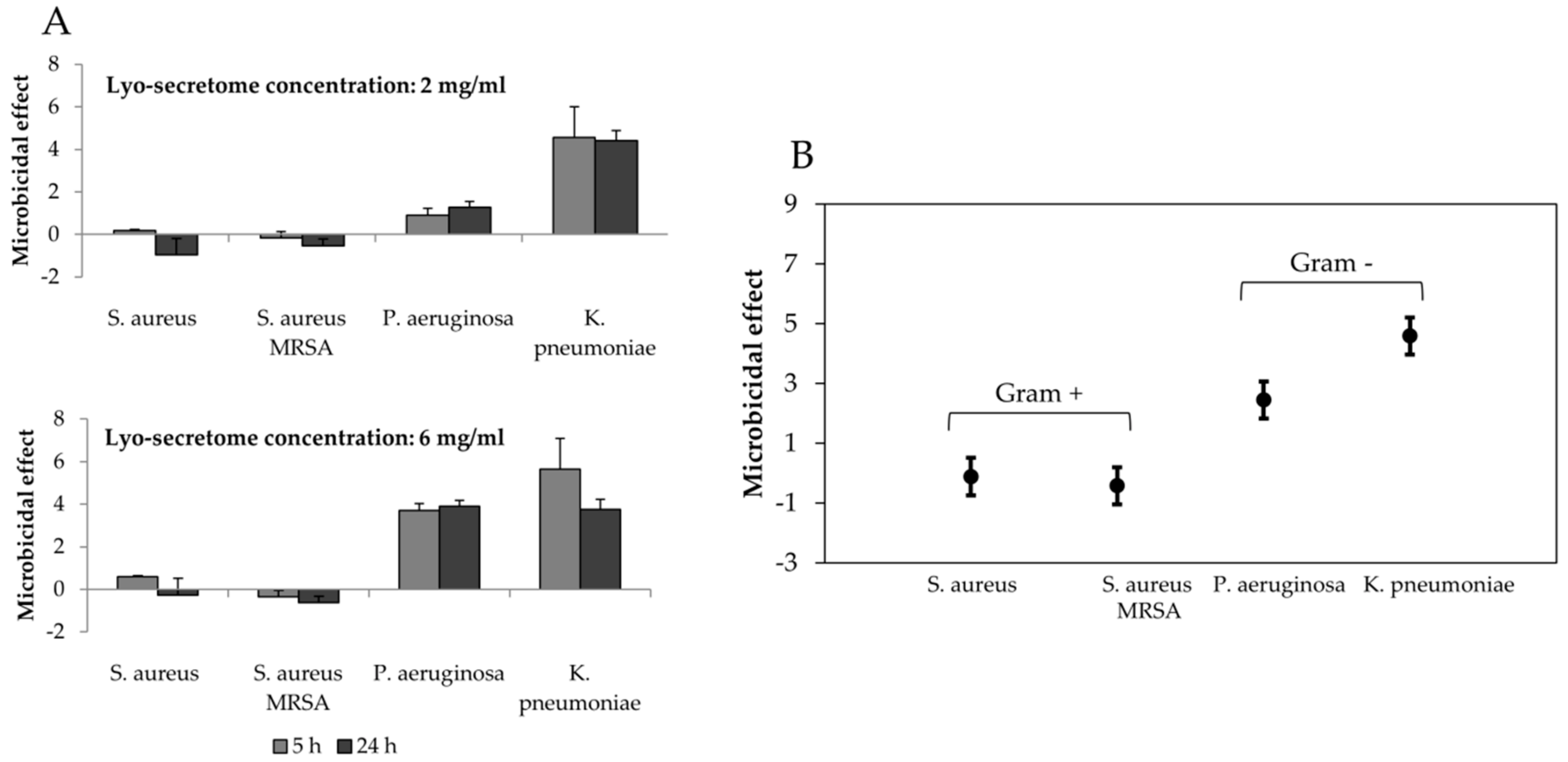
2.6. Antibacterial Activity Measurements
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Phinney, D.G.; Pittenger, M.F. Concise Review: MSC-Derived Exosomes for Cell-Free Therapy. Stem Cells 2017, 35, 851–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Girolamo, L.; Lucarelli, E.; Alessandri, G.; Avanzini, M.A.; Bernardo, M.E.; Biagi, E.; Brini, A.T.; D’Amico, G.; Fagioli, F.; Ferrero, I.; et al. Mesenchymal Stem/Stromal Cells: A New “Cells as Drugs” Paradigm. Efficacy and Critical Aspects in Cell Therapy. Curr. Pharm. Des. 2013, 19, 2459–2473. [Google Scholar] [CrossRef] [PubMed]
- Crivelli, B.; Chlapanidas, T.; Perteghella, S.; Lucarelli, E.; Pascucci, L.; Brini, A.T.; Ferrero, I.; Marazzi, M.; Pessina, A.; Torre, M.L. Mesenchymal stem/stromal cell extracellular vesicles: From active principle to next generation drug delivery system. J. Control. Release 2017, 262, 104–117. [Google Scholar] [CrossRef] [PubMed]
- Bari, E.; Ferrarotti, I.; Torre, M.L.; Corsico, A.G.; Perteghella, S. Mesenchymal stem/stromal cell secretome for lung regeneration: The long way through “pharmaceuticalization” for the best formulation. J. Control. Release 2019, 309, 11–24. [Google Scholar] [CrossRef]
- Giebel, B.; Lambros, K.; Verena, B. Clinical potential of mesenchymal stem/stromal cell-derivedextracellular vesicles. Stem Cell Invest. 2017, 4, 84. [Google Scholar] [CrossRef] [PubMed]
- Gimona, M.; Pachler, K.; Laner-Plamberger, S.; Schallmoser, K.; Rohde, E. Manufacturing of Human Extracellular Vesicle-Based Therapeutics for Clinical Use. Int. J. Mol. Sci. 2017, 18, 1190. [Google Scholar] [CrossRef]
- Bari, E.; Perteghella, S.; Di Silvestre, D.; Sorlini, M.; Catenacci, L.; Sorrenti, M.; Marrubini, G.; Rossi, R.; Tripodo, G.; Mauri, P.; et al. Pilot Production of Mesenchymal Stem/Stromal Freeze-Dried Secretome for Cell-Free Regenerative Nanomedicine: A Validated GMP-Compliant Process. Cells 2018, 7, 190. [Google Scholar] [CrossRef]
- Fregonese, L.; Stolk, J. Hereditary alpha-1-antitrypsin deficiency and its clinical consequences. Orphanet J. Rare Dis. 2008, 3, 16. [Google Scholar] [CrossRef]
- Tonelli, A.R.; Brantly, M.L. Augmentation therapy in alpha-1 antitrypsin deficiency: advances and controversies. Ther. Adv. Respir. Dis. 2010, 4, 289–312. [Google Scholar] [CrossRef]
- Stoller, J.K.; Aboussouan, L.S. alpha 1-antitrypsin deficiency. Lancet 2005, 365, 2225–2236. [Google Scholar] [CrossRef]
- Jonigk, D.; Al-Omari, M.; Maegel, L.; Mueller, M.; Izykowski, N.; Hong, J.; Hong, K.; Kim, S.-H.; Dorsch, M.; Mahadeva, R.; et al. Anti-inflammatory and immunomodulatory properties of alpha 1-antitrypsin without inhibition of elastase. Proc. Natl. Acad. Sci. USA 2013, 110, 15007–15012. [Google Scholar] [PubMed]
- Churg, A.; Wang, X.; Wang, R.D.; Meixner, S.C.; Pryzdial, E.L.G.; Wright, J.L. α1-Antitrypsin Suppresses TNF-α and MMP-12 Production by Cigarette Smoke–Stimulated Macrophages. Am. J. Respir. Cell Mol. Boil. 2007, 37, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Gramegna, A.; Aliberti, S.; Confalonieri, M.; Corsico, A.; Richeldi, L.; Vancheri, C.; Blasi, F. Alpha-1 antitrypsin deficiency as a common treatable mechanism in chronic respiratory disorders and for conditions different from pulmonary emphysema? A commentary on the new European Respiratory Society statement. Mult. Respi. Med. 2018, 13, 39. [Google Scholar] [CrossRef]
- Greene, C.M.; Marciniak, S.J.; Teckman, J.; Ferrarotti, I.; Brantly, M.L.; Lomas, D.A.; Stoller, J.K.; McElvaney, N.G. alpha 1-Antitrypsin deficiency (vol 2, 16051, 2016). Nat. Rev. Dis. Primers 2018, 4. [Google Scholar] [CrossRef]
- Wang, F.; Ni, S.-S.; Liu, H. Pollutional haze and COPD: etiology, epidemiology, pathogenesis, pathology, biological markers and therapy. J. Thorac. Dis. 2016, 8, E20–E30. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.J.; Miedinger, D.; Keidel, D.; Bettschart, R.; Bircher, A.; Bridevaux, P.-O.; Curjuric, I.; Kromhout, H.; Rochat, T.; Rothe, T.; et al. Occupational Exposure to Dusts, Gases, and Fumes and Incidence of Chronic Obstructive Pulmonary Disease in the Swiss Cohort Study on Air Pollution and Lung and Heart Diseases in Adults. Am. J. Respir. Crit. Care Med. 2012, 185, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Stocks, J.M.; Brantly, M.L.; Wang-Smith, L.; Campos, M.A.; Chapman, K.R.; Kueppers, F.; Sandhaus, R.A.; Strange, C.; Turino, G. Pharmacokinetic comparability of Prolastin-C to Prolastin in alpha₁-antitrypsin deficiency: a randomized study. BMC Clin. Pharmacol. 2010, 10, 13. [Google Scholar] [CrossRef]
- Sandhaus, R.A.; Stocks, J.; Rouhani, F.N.; Brantly, M.; Strauss, P. Biochemical Efficacy and Safety of a New, Ready-to-Use, Liquid Alpha-1-Proteinase Inhibitor, GLASSIA (Alpha(1)-Proteinase Inhibitor (Human), Intravenous). Copd-J. Chron. Obst. Pulmon. Dis. 2014, 11, 17–25. [Google Scholar] [CrossRef]
- Stocks, J.M.; Brantly, M.; Pollock, D.; Barker, A.; Kueppers, F.; Strange, C.; Donohue, J.F.; Sandhaus, R. Multi-Center Study: The Biochemical Efficacy, Safety and Tolerability of a New α 1 -Proteinase Inhibitor, Zemaira. COPD: J. Chronic Obstr. Pulm. Dis. 2006, 3, 17–23. [Google Scholar] [CrossRef]
- Mordwinkin, N.M.; Louie, S.G. Aralast: An α1-protease inhibitor for the treatment of α-antitrypsin deficiency. Expert Opin. Pharmacother. 2007, 8, 2609–2614. [Google Scholar] [CrossRef]
- Kolarich, D.; Turecek, P.L.; Weber, A.; Mitterer, A.; Graninger, M.; Matthiessen, P.; Nicolaes, G.A.; Altmann, F.; Schwarz, H.P. Biochemical, molecular characterization, and glycoproteomic analyses of ?1-proteinase inhibitor products used for replacement therapy. Transfusion 2006, 46, 1959–1977. [Google Scholar] [CrossRef] [PubMed]
- Teschler, H. Long-term experience in the treatment of α1-antitrypsin deficiency: 25 years of augmentation therapy. Eur. Respir. Rev. 2015, 24, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Cantin, A.M.; Woods, D.E.; Cloutier, D.; Dufour, E.K.; LeDuc, R. Polyethylene Glycol Conjugation at Cys232Prolongs the Half-Life ofα1 Proteinase Inhibitor. Am. J. Respir. Cell Mol. Boil. 2002, 27, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Flotte, T.R.; Brantly, M.L.; Spencer, L.T.; Byrne, B.J.; Spencer, C.T.; Baker, D.J.; Humphries, M. Phase I Trial of Intramuscular Injection of a Recombinant Adeno-Associated Virus Alpha 1-Antitrypsin (rAAV2-CB-hAAT) Gene Vector to AAT-Deficient Adults. Hum. Gene Ther. 2004, 15, 93–128. [Google Scholar] [PubMed]
- Burrows, J.A.J.; Willis, L.K.; Perlmutter, D.H. Chemical chaperones mediate increased secretion of mutant alpha 1-antitrypsin (alpha 1-AT) Z: A potential pharmacological strategy for prevention of liver injury and emphysema in alpha 1-AT deficiency. Proc. Natl. Acad. Sci. USA 2000, 97, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Marcus, N.Y.; Perlmutter, D.H. Glucosidase and Mannosidase Inhibitors Mediate Increased Secretion of Mutant 1 Antitrypsin Z. J. Boil. Chem. 2000, 275, 1987–1992. [Google Scholar] [CrossRef] [PubMed]
- Sandhaus, R.A. alpha(1)-antitrypsin deficiency center dot 6: New and emerging treatments for alpha(1)-anitrypsin deficiency. Thorax 2004, 59, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Perteghella, S.; Bari, E.; Chlapanidas, T.; Sorlini, M.; De Girolamo, L.; Perucca Orfei, C.; Viganò, M.; Torre, M.L. Process for isolating and lyophilizing extracellular vesicles. WO2018078524 (A1), 28 October 2016. [Google Scholar] [CrossRef]
- Bari, E.; Perteghella, S.; Catenacci, L.; Sorlini, M.; Croce, S.; Mantelli, M.; A Avanzini, M.; Sorrenti, M.; Torre, M.L. Freeze-dried and GMP-compliant pharmaceuticals containing exosomes for acellular mesenchymal stromal cell immunomodulant therapy. Nanomedicine 2019, 14, 753–765. [Google Scholar] [CrossRef]
- Faustini, M.; Bucco, M.; Chlapanidas, T.; Lucconi, G.; Marazzi, M.; Tosca, M.C.; Gaetani, P.; Klinger, M.; Villani, S.; Ferretti, V.V.; et al. Nonexpanded Mesenchymal Stem Cells for Regenerative Medicine: Yield in Stromal Vascular Fraction from Adipose Tissues. Tissue Eng. Part C: Methods 2010, 16, 1515–1521. [Google Scholar] [CrossRef]
- Gaetani, P.; Torre, M.L.; Klinger, M.; Faustini, M.; Crovato, F.; Bucco, M.; Marazzi, M.; Chlapanidas, T.; Levi, D.; Tancioni, F.; et al. Adipose-Derived Stem Cell Therapy for Intervertebral Disc Regeneration: An In Vitro Reconstructed Tissue in Alginate Capsules. Tissue Eng. Part A 2008, 14, 1415–1423. [Google Scholar] [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Krause, D.S.; Deans, R.J.; Keating, A.; Prockop, D.J.; Horwitz, E.M. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Ferrarotti, I.; Scabini, R.; Campo, I.; Ottaviani, S.; Zorzetto, M.; Gorrini, M.; Luisetti, M. Laboratory diagnosis of alpha1-antitrypsin deficiency. Transl. Res. 2007, 150, 267–274. [Google Scholar] [CrossRef]
- Sinden, N.J.; Koura, F.; Stockley, R.A. The significance of the F variant of alpha-1-antitrypsin and unique case report of a PiFF homozygote. BMC Pulm. Med. 2014, 14, 132. [Google Scholar] [CrossRef]
- Bari, E.; Arciola, C.R.; Vigani, B.; Crivelli, B.; Moro, P.; Marrubini, G.; Sorrenti, M.; Catenacci, L.; Bruni, G.; Chlapanidas, T.; et al. In Vitro Effectiveness of Microspheres Based on Silk Sericin and Chlorella vulgaris or Arthrospira platensis for Wound Healing Applications. Materials 2017, 10, 983. [Google Scholar] [CrossRef]
- Gorrini, M.; Ferrarotti, I.; Lupi, A.; Bosoni, T.; Mazzola, P.; Scabini, R.; Campo, I.; Zorzetto, M.; Novazi, F.; Luisetti, M. Validation of a Rapid, Simple Method to Measure 1-Antitrypsin in Human Dried Blood Spots. Clin. Chem. 2006, 52, 899–901. [Google Scholar] [CrossRef]
- Saito, R.; E Smoot, M.; Ono, K.; Ruscheinski, J.; Wang, P.-L.; Lotia, S.; Pico, A.R.; Bader, G.D.; Ideker, T. A travel guide to Cytoscape plugins. Nat. Methods 2012, 9, 1069–1076. [Google Scholar] [CrossRef] [Green Version]
- Doncheva, N.T.; Morris, J.H.; Gorodkin, J.; Jensen, L.J. Cytoscape StringApp: Network Analysis and Visualization of Proteomics Data. J. Proteome Res. 2019, 18, 623–632. [Google Scholar] [CrossRef]
- Scardoni, G.; Tosadori, G.; Pratap, S.; Spoto, F.; Laudanna, C. Finding the shortest path with PesCa: a tool for network reconstruction. F1000Research 2015, 4, 484. [Google Scholar] [CrossRef] [Green Version]
- Maere, S.; Heymans, K.; Kuiper, M. BiNGO: A Cytoscape plugin to assess overrepresentation of Gene Ontology categories in Biological Networks. Bioinformatics 2005, 21, 3448–3449. [Google Scholar] [CrossRef]
- Scardoni, G.; Petterlini, M.; Laudanna, C. Analyzing biological network parameters with CentiScaPe. Bioinformatics 2009, 25, 2857–2859. [Google Scholar] [CrossRef] [Green Version]
- Lara, B.; Martinez, M.T.; Blanco, I.; Hernández-Moro, C.; Velasco, E.A.; Ferrarotti, I.; Rodriguez-Frias, F.; Perez, L.; Vázquez, I.; Alonso, J.; et al. Severe alpha-1 antitrypsin deficiency in composite heterozygotes inheriting a new splicing mutation QOMadrid. Respir. Res. 2014, 15, 4344. [Google Scholar] [CrossRef]
- Chlapanidas, T.; Faragò, S.; Lucconi, G.; Perteghella, S.; Galuzzi, M.; Mantelli, M.; Avanzini, M.A.; Tosca, M.C.; Marazzi, M.; Vigo, D.; et al. Sericins exhibit ROS-scavenging, anti-tyrosinase, anti-elastase, and in vitro immunomodulatory activities. Int. J. Boil. Macromol. 2013, 58, 47–56. [Google Scholar] [CrossRef]
- Anon, B.S. EN 13697: 2001, Chemical Disinfectants and Antiseptics. Quantitative Non-Porous Surface Test for the Evaluation of Bacterial and/or Fungicidal Activity of Chemical Disinfectants Used in Food, Industrial, Domestic and Institutional Areas. Test Method and Requirements without Mechanical Action; British Standards Institute: London, UK, 2001; Available online: https://www.ivami.com/en/biocidal-activities-and-toxicology-with-disinfectants-25-accredited-tests/3321-en-13697-bactericidal-and-or-fungicidal-activity-on-non-porous-surfaces-une-en-13697-2015-b-quantitative-test-for-evaluation-of-bactericidal-fungicidal-activity-in-food-industrial-domestic-and-institutional-areas-b-accredited-by-enac-b (accessed on 12 December 2018).
- Fraise, A.P.; Lambert, P.A.; Masillard, J.-Y.; Russell, H.A.S. (Eds.) Principles and Practice of Disinfection, Preservation & Sterilization, 6th ed.; Blackwell: Oxford, UK, 2004. [Google Scholar]
- Vella, D.; Zoppis, I.; Mauri, G.; Mauri, P.; Di Silvestre, D. From protein-protein interactions to protein co-expression networks: a new perspective to evaluate large-scale proteomic data. EURASIP J. Bioinform. Syst. Boil. 2017, 6. [Google Scholar] [CrossRef]
- Rossi, S.; Marciello, M.; Sandri, G.; Ferrari, F.; Bonferoni, M.C.; Papetti, A.; Caramella, C.; Dacarro, C.; Grisoli, P. Wound Dressings Based on Chitosans and Hyaluronic Acid for the Release of Chlorhexidine Diacetate in Skin Ulcer Therapy. Pharm. Dev. Technol. 2007, 12, 415–422. [Google Scholar] [CrossRef]
- Amato, E.; Diaz-Fernandez, Y.A.; Taglietti, A.; Pallavicini, P.; Pasotti, L.; Cucca, L.; Milanese, C.; Grisoli, P.; Dacarro, C.; Fernandez-Hechavarria, J.M.; et al. Synthesis, Characterization and Antibacterial Activity against Gram Positive and Gram Negative Bacteria of Biomimetically Coated Silver Nanoparticles. Langmuir 2011, 27, 9165–9173. [Google Scholar] [CrossRef]
- Baligar, P.; Kochat, V.; Arindkar, S.K.; Equbal, Z.; Mukherjee, S.; Patel, S.; Nagarajan, P.; Mohanty, S.; Teckman, J.H.; Mukhopadhyay, A. Bone Marrow Stem Cell Therapy Partially Ameliorates Pathological Consequences in Livers of Mice Expressing Mutant Human a1-Antitrypsin. Hepatology 2017, 65, 1319–1335. [Google Scholar] [CrossRef]
- Vader, P.; Mol, E.A.; Pasterkamp, G.; Schiffelers, R.M. Extracellular vesicles for drug delivery. Adv. Drug Deliv. Rev. 2016, 106, 148–156. [Google Scholar] [CrossRef]
- Tsui, N.B.Y.; O Ng, E.K.; Lo, Y.M.D. Stability of endogenous and added RNA in blood specimens, serum, and plasma. Clin. Chem. 2002, 48, 1647–1653. [Google Scholar]
- Alvarez-Erviti, L.; Seow, Y.; Yin, H.; Betts, C.; Lakhal, S.; A Wood, M.J. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nat. Biotechnol. 2011, 29, 341–345. [Google Scholar] [CrossRef]
- Zhuang, X.; Zhang, H.-G. Abstract 4831: Treatment of brain inflammatory diseases by delivering exosome encapsulated anti-inflammatory drugs from the nasal region to the brain. Exp. Mol. Ther. 2012, 72, 4831. [Google Scholar]
- Kusuma, G.D.; Carthew, J.; Lim, R.; Frith, J.E.; Kusuma, D.G.D.; Carthew, D.J.; Frith, D.J.E. Effect of the Microenvironment on Mesenchymal Stem Cell Paracrine Signaling: Opportunities to Engineer the Therapeutic Effect. Stem Cells Dev. 2017, 26, 617–631. [Google Scholar] [CrossRef]
- Saparov, A.; Ogay, V.; Nurgozhin, T.; Jumabay, M.; Chen, W.C.W. Preconditioning of Human Mesenchymal Stem Cells to Enhance Their Regulation of the Immune Response. Stem Cells Int. 2016, 2016, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Noone, C.; Kihm, A.; English, K.; O’Dea, S.; Mahon, B.P. IFN-γ Stimulated Human Umbilical-Tissue-Derived Cells Potently Suppress NK Activation and Resist NK-Mediated Cytotoxicity In Vitro. Stem Cells Dev. 2013, 22, 3003–3014. [Google Scholar] [CrossRef]
- Crisostomo, P.R.; Wang, Y.; Markel, T.A.; Wang, M.; Lahm, T.; Meldrum, D.R. Human mesenchymal stem cells stimulated by TNF-, LPS, or hypoxia produce growth factors by an NF B- but not JNK-dependent mechanism. Am. J. Physiol. Cell Physiol. 2008, 294, 675–682. [Google Scholar] [CrossRef]
- Stoller, J.K.; Aboussouan, L.S. A Review of alpha(1)-Antitrypsin Deficiency. Am. J. Respir. Crit. Care Med. 2012, 185, 246–259. [Google Scholar] [CrossRef]
- Nelson, D.L.; Cox, M.M. Lehninger Principles of Biochemistry; Springer: Berlin, Germany, 2017. [Google Scholar]
- Alcayaga-Miranda, F.; Cuenca, J.; Khoury, M. Antimicrobial Activity of Mesenchymal Stem Cells: Current Status and New Perspectives of Antimicrobial Peptide-Based Therapies. Front. Immunol. 2017, 8, 1109. [Google Scholar] [CrossRef]
- Lin, L.; Du, L. The role of secreted factors in stem cells-mediated immune regulation. Cell. Immunol. 2018, 326, 24–32. [Google Scholar] [CrossRef]
- Porzionato, A.; Zaramella, P.; Dedja, A.; Guidolin, D.; Van Wemmel, K.; Macchi, V.; Jurga, M.; Perilongo, G.; De Caro, R.; Baraldi, E.; et al. Intratracheal administration of clinical-grade mesenchymal stem cell-derived extracellular vesicles reduces lung injury in a rat model of bronchopulmonary dysplasia. Am. J. Physiol. Cell. Mol. Physiol. 2019, 316, L6–L19. [Google Scholar] [CrossRef]
- Cosenza, S.; Toupet, K.; Maumus, M.; Luz-Crawford, P.; Blanc-Brude, O.; Jorgensen, C.; Noël, D. Mesenchymal stem cells-derived exosomes are more immunosuppressive than microparticles in inflammatory arthritis. Theranostics 2018, 8, 1399–1410. [Google Scholar] [CrossRef]
- Di Trapani, M.; Bassi, G.; Midolo, M.; Gatti, A.; Takam, P.; Cassaro, A.; Carusone, R.; Adamo, A.; Krampera, M. Differential and transferable modulatory effects of mesenchymal stromal cell-derived extracellular vesicles on t, b and nk cell functions. Haematologica 2016, 101. [Google Scholar] [CrossRef]
- Sicco, C.L.; Reverberi, D.; Balbi, C.; Ulivi, V.; Principi, E.; Pascucci, L.; Becherini, P.; Bosco, M.C.; Varesio, L.; Franzin, C.; et al. Mesenchymal Stem Cell-Derived Extracellular Vesicles as Mediators of Anti-Inflammatory Effects: Endorsement of Macrophage Polarization. Stem Cells Transl. Med. 2017, 6, 1018–1028. [Google Scholar] [CrossRef]
- Taggart, C.; Mall, M.A.; Lalmanach, G.; Cataldo, D.; Ludwig, A.; Janciauskiene, S.; Heath, N.; Meiners, S.; Overall, C.M.; Schultz, C.; et al. Protean proteases: at the cutting edge of lung diseases. Eur. Respir. J. 2017, 49, 1501200. [Google Scholar] [CrossRef] [Green Version]
- Théry C, A.S.; Raposo, G.; Clayton, A. Isolation and Characterization of Exosomes from Cell Culture Supernatants and Biological Fluids. Curr. Protoc. Cell Biol. 2006. [Google Scholar]
- Daviskas, E.; Anderson, S.D.; Young, I.H. Effect of mannitol and repetitive coughing on the sputum properties in bronchiectasis. Respir. Med. 2010, 104, 371–377. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lyo-Secretome Batch | AAT (µg/mg) | AAT (nM) |
|---|---|---|
| 1 | 0.78 ± 0.06 | 15.0 ± 1.1 |
| 2 | 0.83 ± 0.08 | 16.0 ± 1.5 |
| 3 | 1.24 ± 0.09 | 23.8 ± 1.7 |
| MSC-Secretome Fraction | AAT (µg/mg) | AAT (nM) |
|---|---|---|
| EV | 1.37 ± 0.25 | 26.3 ± 4.8 |
| HMW | 0.16 ± 0.05 | 3.1 ± 0.9 |
| LMW | 1.38 ± 0.64 | 26.5± 12 |
| Sample | Km | Vmax | ||
|---|---|---|---|---|
| Mean | St. err. | Mean | St. err. | |
| EV | 20.2a | 2.534 | 0.878a | 0.03708 |
| LMW | 10.2b | 2.534 | 0.827a | 0.03708 |
| HMW | 9.85b | 2.534 | 0.818a | 0.03708 |
| ST | 20.6a | 2.534 | 0.894a | 0.03708 |
| DEX | 15.6b | 2.534 | 0.861a | 0.03708 |
| IL-1β | 15.6b | 2.534 | 0.860a | 0.03708 |
| IL-1β + DEX | 11.7b | 2.534 | 0.876a | 0.03708 |
| AAT | 11.2b | 2.196 | 0.569b | 0.03214 |
| CTR + | 20.5a | 2.158 | 0.0484c | 0.03158 |
| CTR - | 9.96b | 2.158 | 0.856a | 0.03158 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bari, E.; Ferrarotti, I.; Di Silvestre, D.; Grisoli, P.; Barzon, V.; Balderacchi, A.; Torre, M.L.; Rossi, R.; Mauri, P.; Corsico, A.G.; et al. Adipose Mesenchymal Extracellular Vesicles as Alpha-1-Antitrypsin Physiological Delivery Systems for Lung Regeneration. Cells 2019, 8, 965. https://doi.org/10.3390/cells8090965
Bari E, Ferrarotti I, Di Silvestre D, Grisoli P, Barzon V, Balderacchi A, Torre ML, Rossi R, Mauri P, Corsico AG, et al. Adipose Mesenchymal Extracellular Vesicles as Alpha-1-Antitrypsin Physiological Delivery Systems for Lung Regeneration. Cells. 2019; 8(9):965. https://doi.org/10.3390/cells8090965
Chicago/Turabian StyleBari, Elia, Ilaria Ferrarotti, Dario Di Silvestre, Pietro Grisoli, Valentina Barzon, Alice Balderacchi, Maria Luisa Torre, Rossana Rossi, Pierluigi Mauri, Angelo Guido Corsico, and et al. 2019. "Adipose Mesenchymal Extracellular Vesicles as Alpha-1-Antitrypsin Physiological Delivery Systems for Lung Regeneration" Cells 8, no. 9: 965. https://doi.org/10.3390/cells8090965