The Neutrophil-to-Lymphocyte Ratio is Related to Disease Activity in Relapsing Remitting Multiple Sclerosis

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
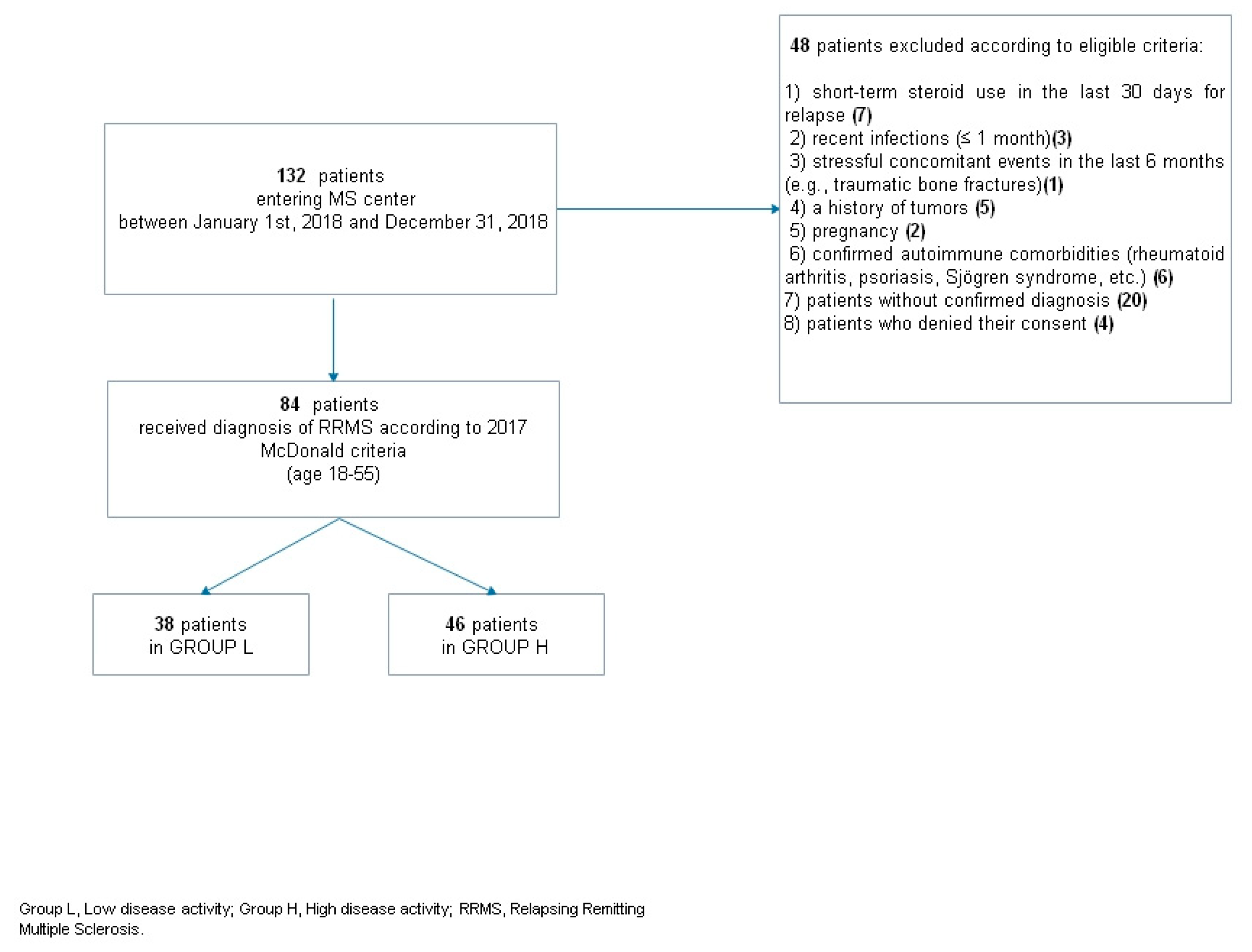
2.1. Clinical Data
2.2. Blood Tests
2.3. Outcomes
2.4. Ethical Standards
2.5. Statistical Analysis
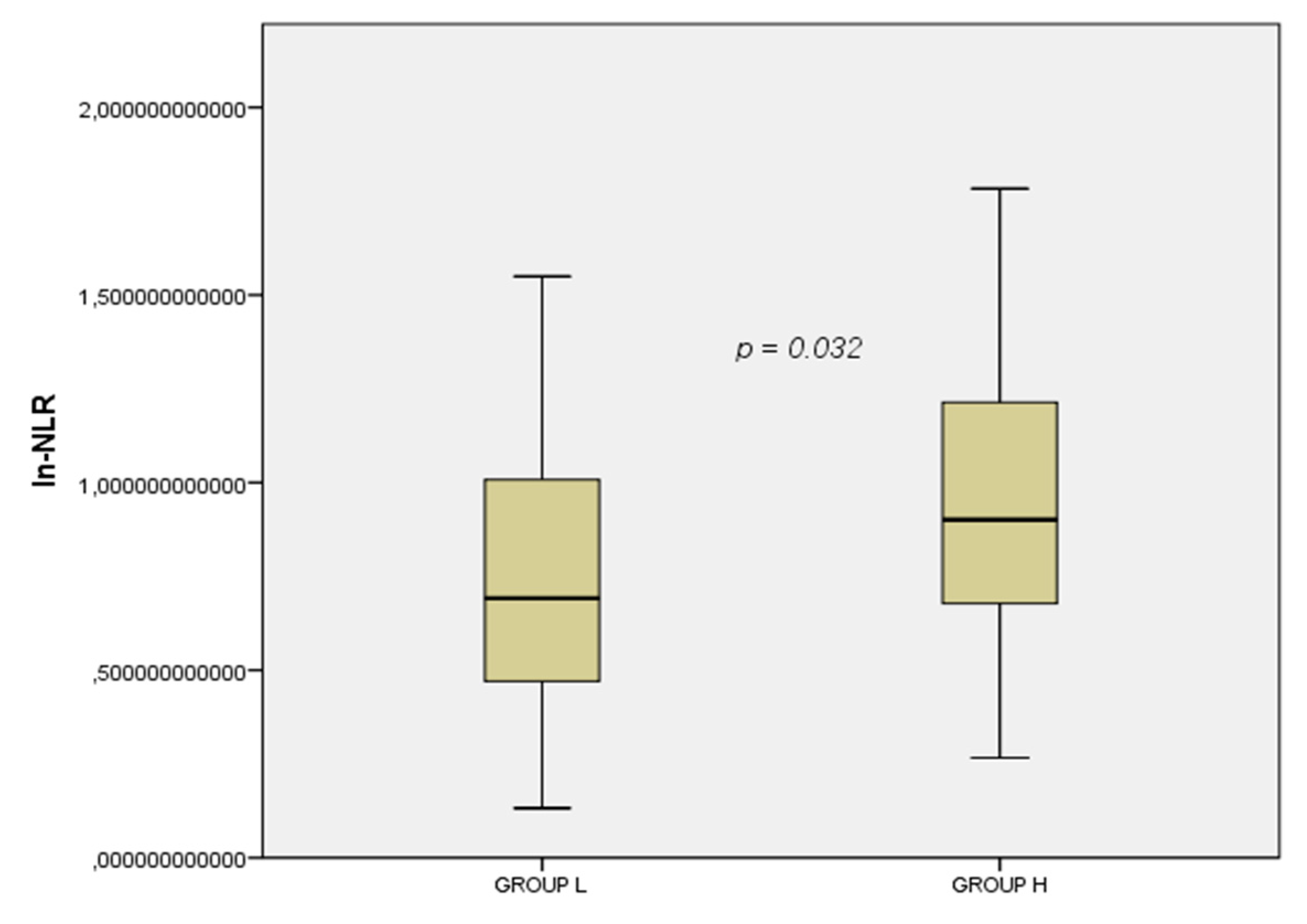
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple Sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.; Zanghì, A.; Gastaldi, M.; Patti, F.; Zappia, M.; Franciotta, D. Placing CD20-targeted B cell depletion in multiple sclerosis therapeutic scenario: Present and future perspectives. Autoimmun. Rev. 2019, 18, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Woodberry, T.; Bouffler, S.E.; Wilson, A.S.; Buckland, R.L.; Brustle, A. The Emerging Role of Neutrophil Granulocytes in Multiple Sclerosis. J. Clin. Med. 2018, 7, 511. [Google Scholar] [CrossRef] [PubMed]
- Naegele, M.; Tillack, K.; Reinhardt, S.; Schippling, S.; Martin, R.; Sospedra, M. Neutrophils in multiple sclerosis are characterized by a primed phenotype. J. Neuroimmunol. 2012, 242, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Qiu, L.; Li, Z.; Wang, X.Y.; Yi, H. Understanding the Multifaceted Role of Neutrophils in Cancer and Autoimmune Diseases. Front. Immunol. 2018, 9, 2456. [Google Scholar] [CrossRef] [PubMed]
- Casserly, C.S.; Nantes, J.C.; Hawkins, R.F.W.; Vallieres, L. Neutrophil perversion in demyelinating autoimmune diseases: Mechanisms to medicine. Autoimmun. Rev. 2017, 16, 294–307. [Google Scholar] [CrossRef] [PubMed]
- Demirci, S.; Demirci, S.; Kutluhan, S.; Koyuncuoglu, H.R.; Yurekli, V.A. The clinical significance of the neutrophil-to-lymphocyte ratio in multiple sclerosis. Int. J. Neurosci. 2016, 126, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Guzel, I.; Mungan, S.; Oztekin, Z.N.; Ak, F. Is there an association between the Expanded Disability Status Scale and inflammatory markers in multiple sclerosis? J. Chin. Med. Assoc. JCMA 2016, 79, 54–57. [Google Scholar] [CrossRef]
- Hasselbalch, I.C.; Sondergaard, H.B.; Koch-Henriksen, N.; Olsson, A.; Ullum, H.; Sellebjerg, F.; Otural, A.B. The neutrophil-to-lymphocyte ratio is associated with multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2018, 4. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Derfuss, T.; Bergvall, N.K.; Sfikas, N.; Tomic, D.L. Efficacy of fingolimod in patients with highly active relapsing–remitting multiple sclerosis. Curr. Med. Res. Opin. 2015, 31, 1687–1691. [Google Scholar] [CrossRef] [PubMed]
- Fernández, Ó. Is there a change of paradigm towards more effective treatment early in the course of apparent high-risk MS? Mult. Scler. Relat. Disord. 2017, 17, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, M.; Kappos, L.; Calabresi, P.A.; Confavreux, C.; Giovannoni, G.; Galetta, S.L.; Havrdova, E.; Lublin, F.D.; Miller, D.H.; O’Connor, P.W.; et al. The efficacy of natalizumab in patients with relapsing multiple sclerosis: Subgroup analyses of AFFIRM and SENTINEL. J. Neurol. 2009, 256, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Krieger, S.; Singer, B.; Freedman, M.; Lycke, J.; Berkovich, R.; Margolin, D.; Thangavelu, K.; Havrdova, E. Treatment-Naive Patients with Highly Active RRMS Demonstrated Durable Efficacy with Alemtuzumab over 5 Years (S51.003). Neurology 2016, 86, S51.003. [Google Scholar]
- Zeng, Z.; Wang, C.; Wang, B.; Wang, N.; Yang, Y.; Guo, S.; Du, Y. Prediction of neutrophil-to-lymphocyte ratio in the diagnosis and progression of autoimmune encephalitis. Neurosci. Lett. 2019, 694, 129–135. [Google Scholar] [CrossRef]
- Erre, G.L.; Paliogiannis, P.; Castagna, F.; Mangoni, A.A.; Carru, C.; Passiu, G.; Zinellu, A. Meta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur. J. Clin. Investig. 2019, 49, e13037. [Google Scholar] [CrossRef]
- Bisgaard, A.K.; Pihl-Jensen, G.; Frederiksen, J.L. The neutrophil-to-lymphocyte ratio as disease actvity marker in multiple sclerosis and optic neuritis. Mult. Scler. Relat. Disord. 2017, 18, 213–217. [Google Scholar] [CrossRef]
- Al-Hussain, F.; Alfallaj, M.M.; Alahmari, A.N.; Almazyad, A.N.; Alsaeed, T.K.; Abdurrahman, A.A.; Murtaza, G.; Bashir, S. Relationship between Neutrophil-to-Lymphocyte Ratio and Stress in Multiple Sclerosis Patients. J. Clin. Diagn. Res. JCDR 2017, 11, CC01–CC044. [Google Scholar]
- Hemond, C.C.; Glanz, B.I.; Bakshi, R.; Chitnis, T.; Healy, B.C. The neutrophil-to-lymphocyte and monocyte-to-lymphocyte ratios are independently associated with neurological disability and brain atrophy in multiple sclerosis. BMC Neurol. 2019, 19, 23. [Google Scholar] [CrossRef]
- Giovannoni, G.; Miller, D.H.; Losseff, N.A.; Sailer, M.; Lewellyn-Smith, N.; Thompson, A.J.; Thompson, E.J. Serum inflammatory markers and clinical/MRI markers of disease progression in multiple sclerosis. J. Neurol. 2001, 248, 487–495. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Group L (n = 38) | Group H (n = 46) | P-Value | |
|---|---|---|---|
| Men | 19 (50%) | 19 (41.3%) | 0.42 |
| Women | 19 (50%) | 27 (58.7%) | |
| AGE | 43 ± 13.4 | 36.9 ± 12.5 | 0.23 |
| L% | 29 ± 8.5 | 27.8 ± 6.6 | 0.95 |
| N% | 62.3 ± 7.7 | 63.3 ± 7.7 | 0.57 |
| lnNLR | 0.7 ± 0.4 | 1 ± 0.4 | 0.032 |
| EDSS value | 1.5 (1.0–3.0) | 2.5 (1.0–5.0) | 0.020 |
| Patient Characteristics vs. ln-NLR | V-Cramer Index | P-Value |
|---|---|---|
| Gender | 0.016 | 0.289 |
| Age | 0.052 | 0.637 |
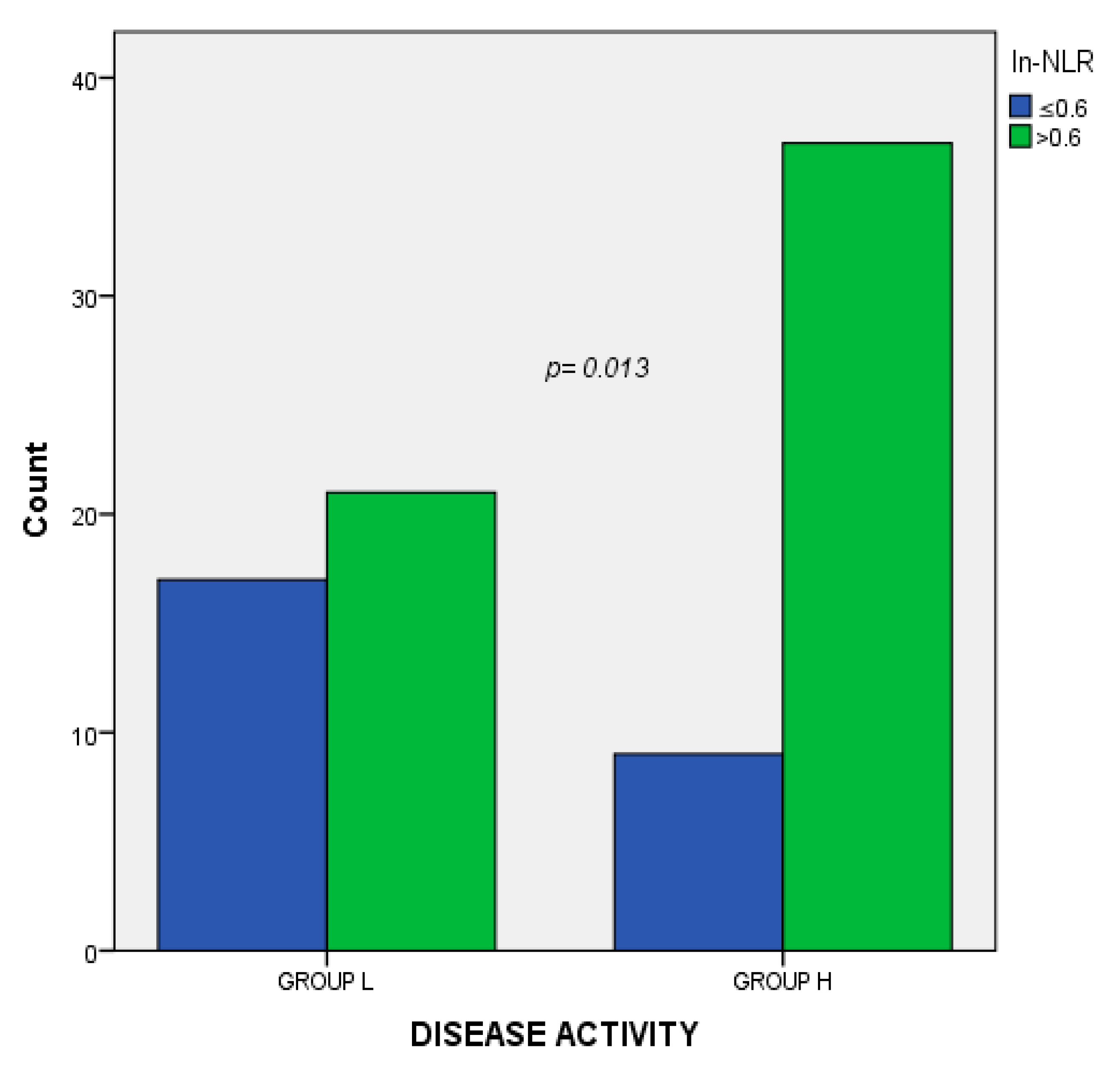
| Disease activity | 0.271 | 0.013 |
| EDSS value at onset | 0.062 | 0.567 |
| Exp B | P-Value | Confidence | Interval (95%) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Gender | 0.887 | 0.778 | 0.352 | 2.18 |
| Age | 1.00 | 0.555 | 1.00 | 1.00 |
| ln-NLR | 3.5 | 0.03 | 1.08 | 11.4 |
| EDSS value at onset | 1.00 | 0.926 | 1.00 | 1.00 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Amico, E.; Zanghì, A.; Romano, A.; Sciandra, M.; Palumbo, G.A.M.; Patti, F. The Neutrophil-to-Lymphocyte Ratio is Related to Disease Activity in Relapsing Remitting Multiple Sclerosis. Cells 2019, 8, 1114. https://doi.org/10.3390/cells8101114
D’Amico E, Zanghì A, Romano A, Sciandra M, Palumbo GAM, Patti F. The Neutrophil-to-Lymphocyte Ratio is Related to Disease Activity in Relapsing Remitting Multiple Sclerosis. Cells. 2019; 8(10):1114. https://doi.org/10.3390/cells8101114
Chicago/Turabian StyleD’Amico, Emanuele, Aurora Zanghì, Alessandra Romano, Mariangela Sciandra, Giuseppe Alberto Maria Palumbo, and Francesco Patti. 2019. "The Neutrophil-to-Lymphocyte Ratio is Related to Disease Activity in Relapsing Remitting Multiple Sclerosis" Cells 8, no. 10: 1114. https://doi.org/10.3390/cells8101114
APA StyleD’Amico, E., Zanghì, A., Romano, A., Sciandra, M., Palumbo, G. A. M., & Patti, F. (2019). The Neutrophil-to-Lymphocyte Ratio is Related to Disease Activity in Relapsing Remitting Multiple Sclerosis. Cells, 8(10), 1114. https://doi.org/10.3390/cells8101114