
Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 Recovery or Post-Vaccination

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Subjects
2.2. Quantitative Determination of IgG Antibodies against SARS-CoV-2
2.3. Cellular Response Analysis
Cell Stimulation
2.4. Interferon-Gamma ELISA
2.5. Statistical Analysis
3. Results
3.1. Characteristic of Study Group
3.2. Comparisons of an Antibody Level between Subgroups
3.3. Correlation of the Antibody Titer with Age and Sex
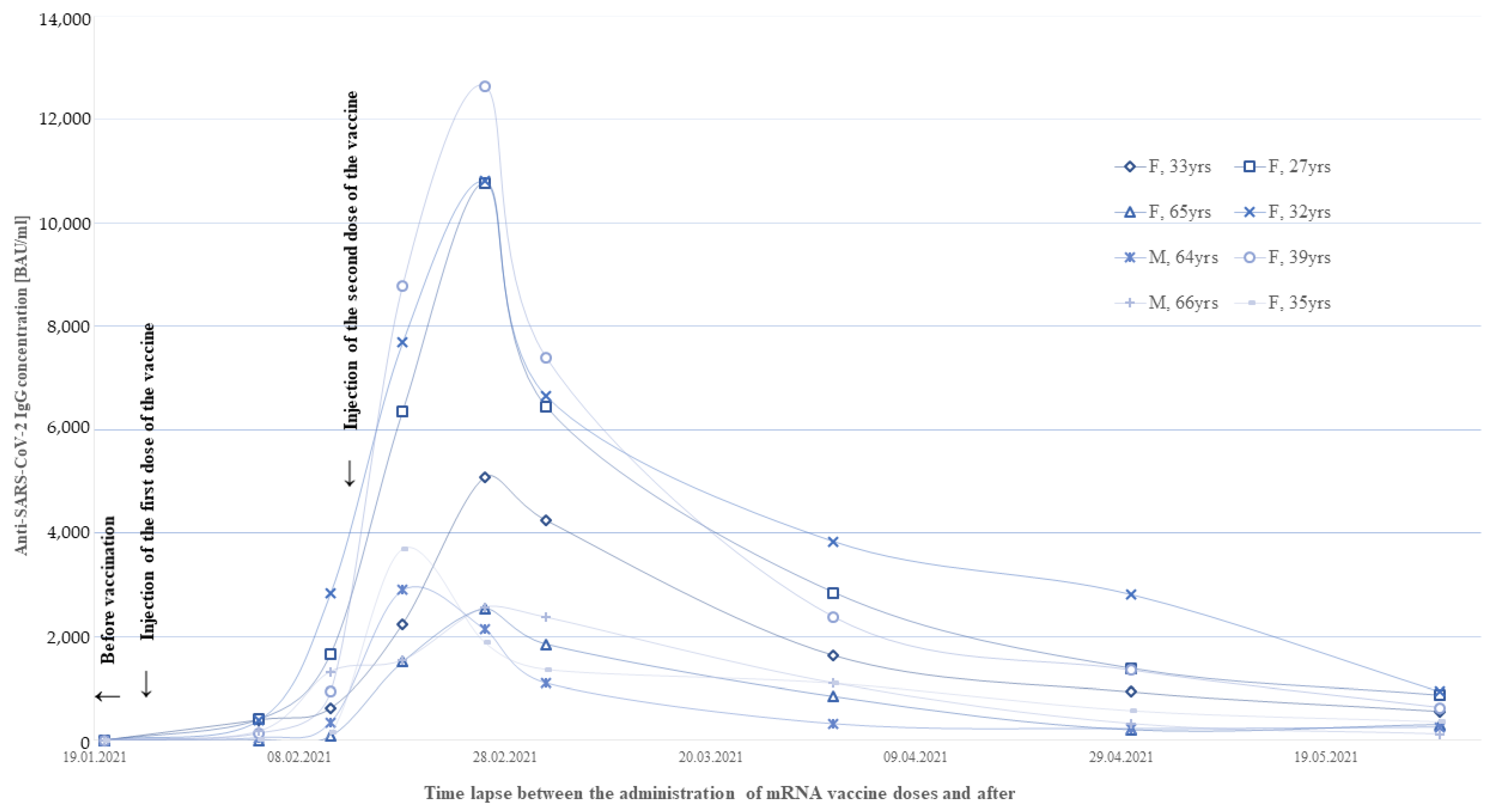
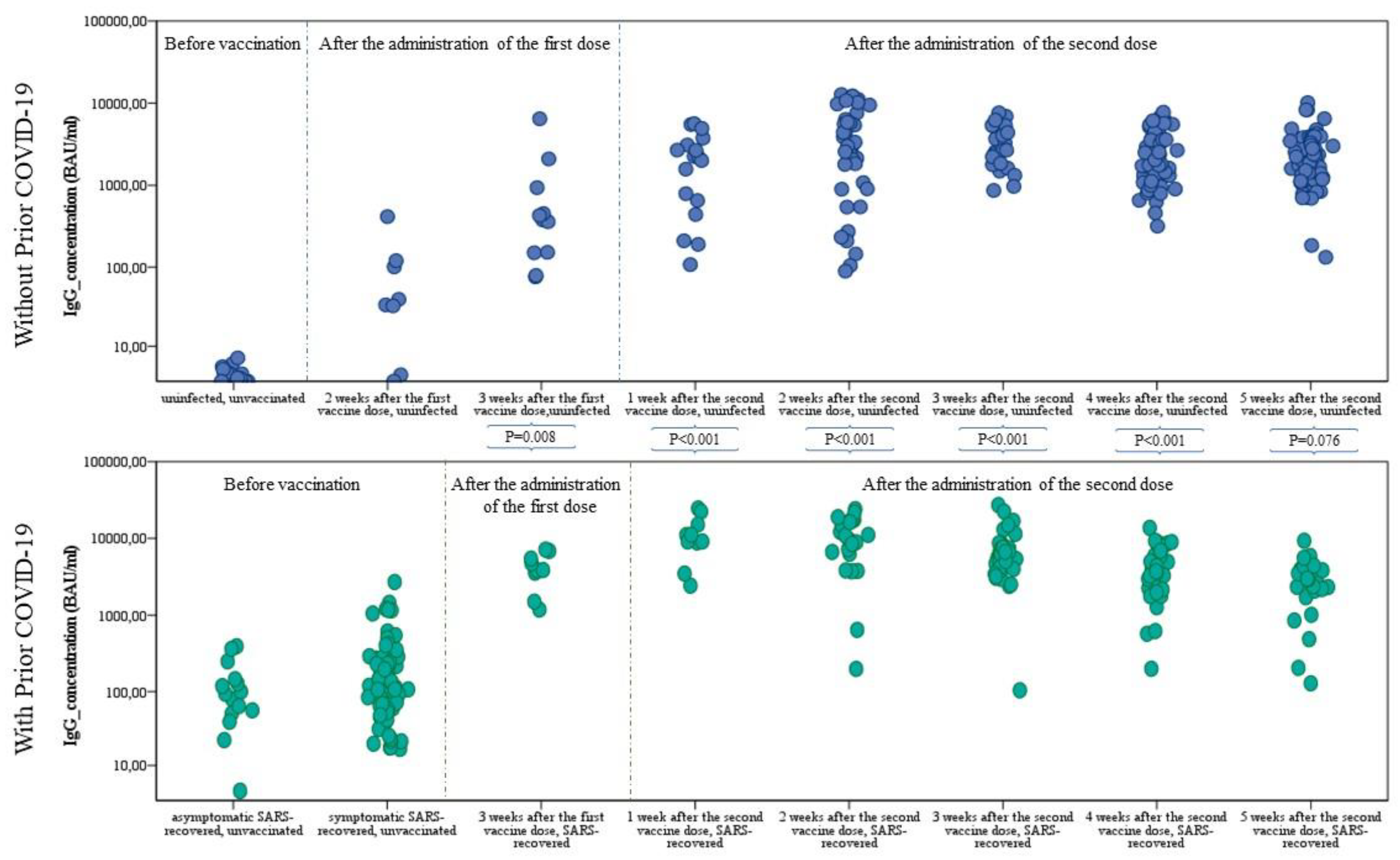
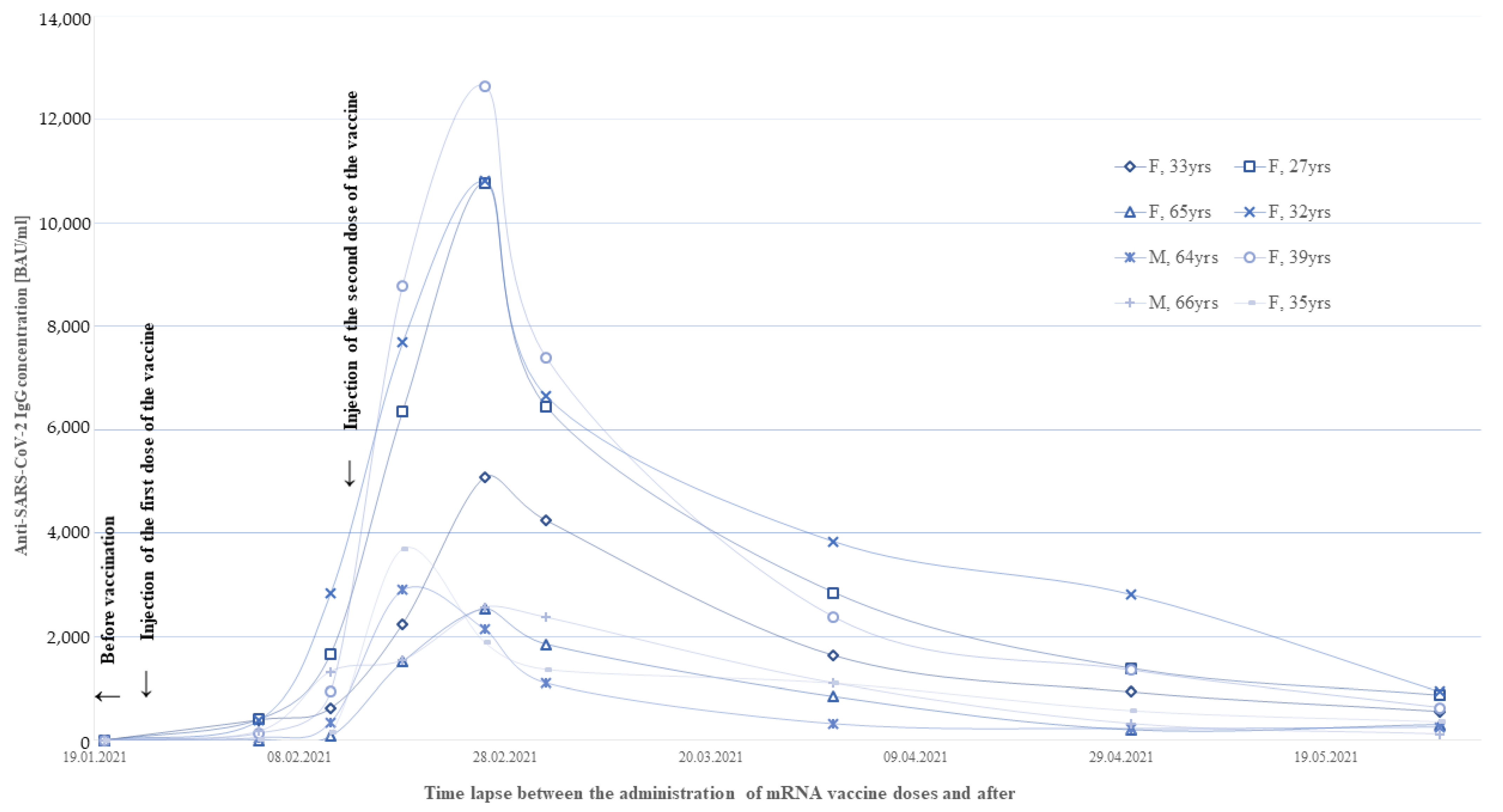
3.4. Monitoring of the Humoral Response in the First Weeks after Vaccination
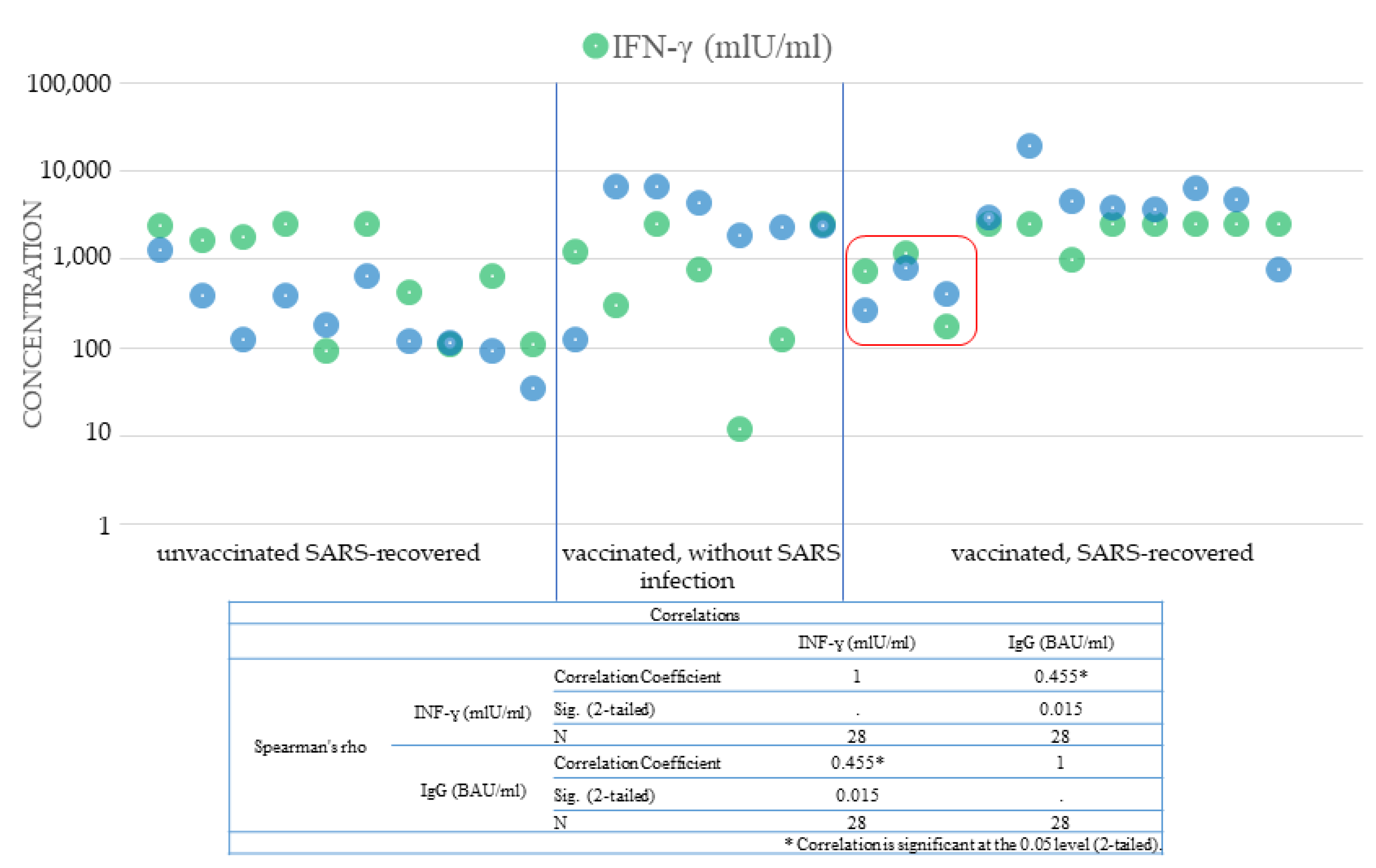
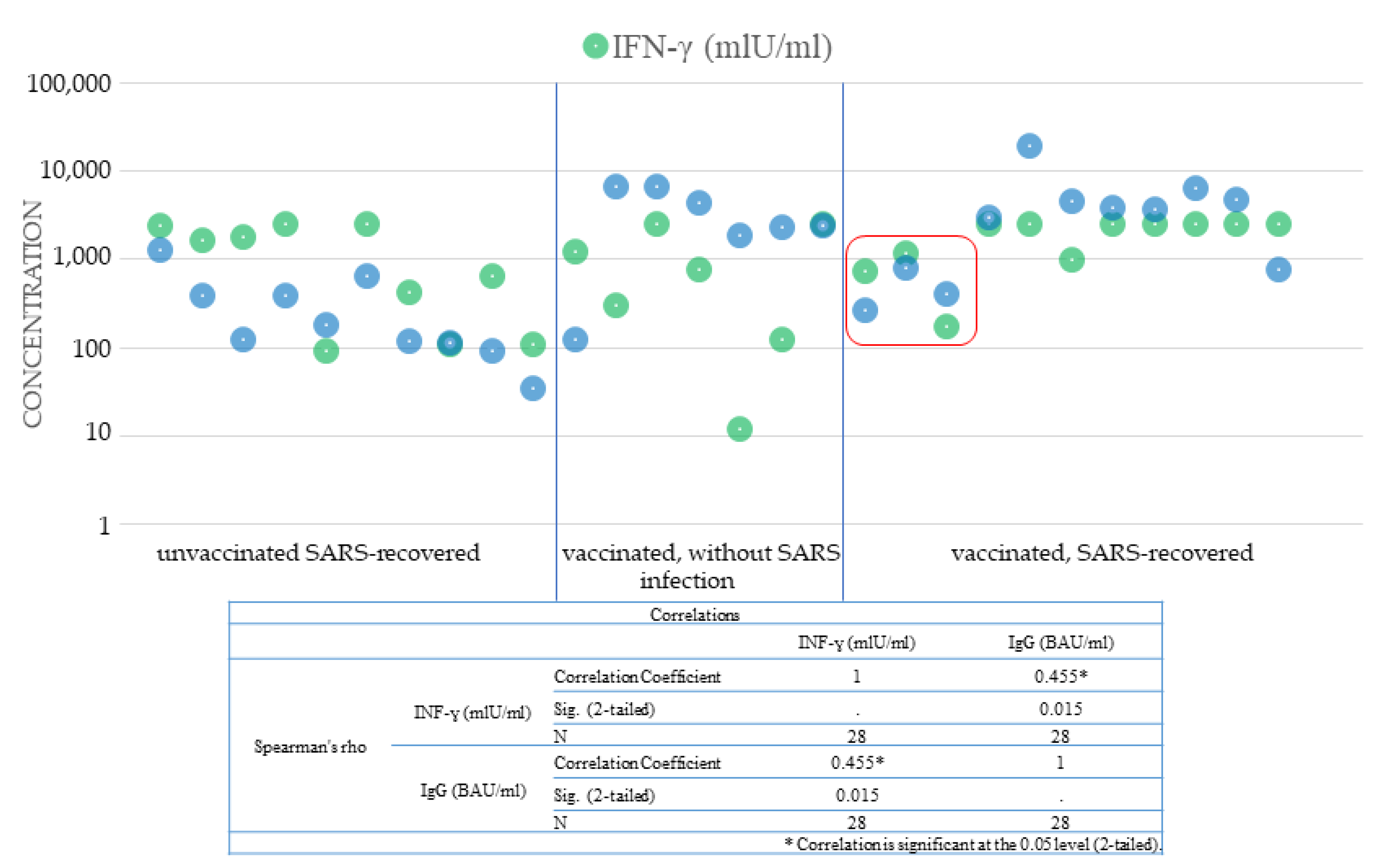
3.5. Humoral Immunity and Cellular Immunity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Statement
References
- Li, D.D.; Li, Q.H. SARS-CoV-2: Vaccines in the pandemic era. Mil. Med. Res. 2021, 8, 1. [Google Scholar] [CrossRef]
- WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 28 May 2021).
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501.e1415. [Google Scholar] [CrossRef]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Bonifacius, A.; Tischer-Zimmermann, S.; Dragon, A.C.; Gussarow, D.; Vogel, A.; Krettek, U.; Godecke, N.; Yilmaz, M.; Kraft, A.R.M.; Hoeper, M.M.; et al. COVID-19 immune signatures reveal stable antiviral T cell function despite declining humoral responses. Immunity 2021, 54, 340–354.e346. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological Memory to SARS-CoV-2 Assessed for up to 8 Months after Infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Post, N.; Eddy, D.; Huntley, C.; van Schalkwyk, M.C.I.; Shrotri, M.; Leeman, D.; Rigby, S.; Williams, S.V.; Bermingham, W.H.; Kellam, P.; et al. Antibody response to SARS-CoV-2 infection in humans: A systematic review. PLoS ONE 2020, 15, e0244126. [Google Scholar] [CrossRef]
- Krammer, F.; Simon, V. Serology assays to manage COVID-19. Science 2020, 368, 1060–1061. [Google Scholar] [CrossRef]
- Ashour, H.M.; Elkhatib, W.F.; Rahman, M.M.; Elshabrawy, H.A. Insights into the Recent 2019 Novel Coronavirus (SARS-CoV-2) in Light of Past Human Coronavirus Outbreaks. Pathogens 2020, 9, 186. [Google Scholar] [CrossRef] [Green Version]
- Pfizer. Pfizer and BioNTech Announce Vaccine Candidate against COVID-19 Achieved Success in First Interim Analysis from Phase 3 Study; Pfizer: New York, NY, USA, 2020. [Google Scholar]
- Summary of Product Characteristics. Comirnaty Concentrate for Dispersion for Injection. COVID-19 mRNA Vaccine. Available online: https://www.ema.europa.eu/en/documents/product-information/comirnaty-epar-product-information_en.pdf (accessed on 13 March 2021).
- Information for Healthcare Professionals on Pfizer/BioNTech COVID-19 Vaccine. Updated 31 March 2021. Available online: https://www.gov.uk/government/publications/regulatory-approval-of-pfizer-biontech-vaccine-for-covid-19/information-for-healthcare-professionals-on-pfizerbiontech-covid-19-vaccine (accessed on 12 April 2021).
- Wang, J.; Peng, Y.; Xu, H.; Cui, Z.; Williams, R.O., 3rd. The COVID-19 Vaccine Race: Challenges and Opportunities in Vaccine Formulation. AAPS PharmSciTech 2020, 21, 225. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodes-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Hassan, A.O.; Case, J.B.; Winkler, E.S.; Thackray, L.B.; Kafai, N.M.; Bailey, A.L.; McCune, B.T.; Fox, J.M.; Chen, R.E.; Alsoussi, W.B.; et al. A SARS-CoV-2 Infection Model in Mice Demonstrates Protection by Neutralizing Antibodies. Cell 2020, 182, 744–753.e744. [Google Scholar] [CrossRef]
- Hansen, J.; Baum, A.; Pascal, K.E.; Russo, V.; Giordano, S.; Wloga, E.; Fulton, B.O.; Yan, Y.; Koon, K.; Patel, K.; et al. Studies in humanized mice and convalescent humans yield a SARS-CoV-2 antibody cocktail. Science 2020, 369, 1010–1014. [Google Scholar] [CrossRef]
- Rydyznski Moderbacher, C.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-Specific Adaptive Immunity to SARS-CoV-2 in Acute COVID-19 and Associations with Age and Disease Severity. Cell 2020, 183, 996–1012.e1019. [Google Scholar] [CrossRef] [PubMed]
- Poon, M.M.L.; Farber, D.L. Lasting memories of SARS-CoV-2 infection. J. Exp. Med. 2021, 218, e20210210. [Google Scholar] [CrossRef]
- Petrone, L.; Petruccioli, E.; Vanini, V.; Cuzzi, G.; Najafi Fard, S.; Alonzi, T.; Castilletti, C.; Palmieri, F.; Gualano, G.; Vittozzi, P.; et al. A whole blood test to measure SARS-CoV-2-specific response in COVID-19 patients. Clin. Microbiol. Infect. 2021, 27, 286.e7. [Google Scholar] [CrossRef]
- Public Health England. Report to JCVI on Estimated Efficacy of a Single Dose of Pfizer BioNTech (BNT162b2 mRNA) Vaccine and of a Single Dose of ChAdOx1 Vaccine (AZD1222); Public Health England: London, UK, 2020. [Google Scholar]
- Angyal, A.; Longet, S.; Moore, S.; Payne, R.P.; Harding, A.; Tipton, T.; Rongkard, P.; Ali, M.; Hering, L.M.; Meardon, N.; et al. T-Cell and Antibody Responses to First BNT162b2 Vaccine Dose in Previously SARS-CoV-2-Infected and Infection-Naive UK Healthcare Workers: A Multicentre, Prospective, Observational Cohort Study. 2021. Available online: https://ssrn.com/abstract=3812375 (accessed on 12 April 2021). [CrossRef]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermudez-Gonzalez, M.C.; Bielak, D.A.; Carreno, J.M.; Chernet, R.L.; et al. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef]
- Saadat, S.; Tehrani, Z.R.; Logue, J.; Newman, M.; Frieman, M.B.; Harris, A.D.; Sajadi, M.M. Binding and Neutralization Antibody Titers after a Single Vaccine Dose in Health Care Workers Previously Infected with SARS-CoV-2. JAMA 2021, 325, 1467–1469. [Google Scholar] [CrossRef]
- Ebinger, J.E.; Fert-Bober, J.; Printsev, I.; Wu, M.; Sun, N.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; van Eyk, J.E.; Braun, J.G.; et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat. Med. 2021, 27, 981–984. [Google Scholar] [CrossRef]
- Mazzoni, A.; di Lauria, N.; Maggi, L.; Salvati, L.; Vanni, A.; Capone, M.; Lamacchia, G.; Mantengoli, E.; Spinicci, M.; Zammarchi, L.; et al. First-dose mRNA vaccination is sufficient to reactivate immunological memory to SARS-CoV-2 in recovered COVID-19 subjects. J. Clin. Investig. 2021, 131, e149150. [Google Scholar] [CrossRef]
- Gobbi, F.; Buonfrate, D.; Moro, L.; Rodari, P.; Piubelli, C.; Caldrer, S.; Riccetti, S.; Sinigaglia, A.; Barzon, L. Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses 2021, 13, 422. [Google Scholar] [CrossRef]
- FDA. FDA Statement on Following the Authorized Dosing Schedules for COVID-19 Vaccines; FDA: Silver Spring, MD, USA, 2021. [Google Scholar]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Risk of SARS-CoV-2 Transmission from Newly-Infected Individuals with Documented Previous Infection or Vaccination; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Chia, W.N.; Zhu, F.; Ong, S.W.X.; Young, B.E.; Fong, S.W.; le Bert, N.; Tan, C.W.; Tiu, C.; Zhang, J.; Tan, S.Y.; et al. Dynamics of SARS-CoV-2 neutralising antibody responses and duration of immunity: A longitudinal study. Lancet Microbe 2021, 2, e240–e249. [Google Scholar] [CrossRef]
- Skelly, D.T.; Harding, A.C.; Gilbert-Jaramillo, J.; Knight, M.L.; Longet, S.; Brown, A.; Adele, S.; Adland, E.; Brown, H.; Team, M.L.; et al. Two doses of SARS-CoV-2 vaccination induce more robust immune responses to emerging SARS-CoV-2 variants of concern than does natural infection. Res. Sq. 2021. preprint. [Google Scholar] [CrossRef]
- Reynolds, C.J.; Pade, C.; Gibbons, J.M.; Butler, D.K.; Otter, A.D.; Menacho, K.; Fontana, M.; Smit, A.; Sackville-West, J.E.; Cutino-Moguel, T.; et al. Prior SARS-CoV-2 infection rescues B and T cell responses to variants after first vaccine dose. Science 2021, 372, 1418–1423. [Google Scholar] [CrossRef]
- Blain, H.; Tuaillon, E.; Gamon, L.; Pisoni, A.; Miot, S.; Picot, M.C.; Bousquet, J. Spike Antibody Levels of Nursing Home Residents With or Without Prior COVID-19 3 Weeks After a Single BNT162b2 Vaccine Dose. JAMA 2021, 325, 1898–1899. [Google Scholar] [CrossRef]
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; del Molino del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Coyle, P.; Malek, J.A.; Ahmed, A.A.; Mohamoud, Y.A.; Younuskunju, S.; Ayoub, H.H.; Al Kanaani, Z.; Al Kuwari, E.; et al. SARS-CoV-2 reinfection in a cohort of 43,000 antibody-positive individuals followed for up to 35 weeks. medRxiv 2021. preprint. [Google Scholar] [CrossRef]
- Perez, G.; Banon, T.; Gazit, S.; Moshe, S.B.; Wortsman, J.; Grupel, D.; Peretz, A.; Tov, A.B.; Chodick, G.; Mizrahi-Reuveni, M.; et al. A 1 to 1000 SARS-CoV-2 reinfection proportion in members of a large healthcare provider in Israel: A preliminary report. medRxiv 2021. preprint. [Google Scholar] [CrossRef]
- Keehner, J.; Horton, L.E.; Pfeffer, M.A.; Longhurst, C.A.; Schooley, R.T.; Currier, J.S.; Abeles, S.R.; Torriani, F.J. SARS-CoV-2 Infection after Vaccination in Health Care Workers in California. N. Engl. J. Med. 2021, 384, 1774–1775. [Google Scholar] [CrossRef]
- White, E.M.; Yang, X.; Blackman, C.; Feifer, R.A.; Gravenstein, S.; Mor, V. Incident SARS-CoV-2 Infection among mRNA-Vaccinated and Unvaccinated Nursing Home Residents. N. Engl. J. Med. 2021, 385, 474–476. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (Years) | |||||||||||
| SARS-CoV-2 and Vaccination Status | N | ≤35 | 36–45 | 46–55 | 56–65 | 65+ | ≤35 | 36–45 | 46–55 | 56–65 | 65+ |
| Unvaccinated | |||||||||||
| Without prior SARS-CoV-2 infection | 24 | 4 | 2 | 3 | 5 | 0 | 2 | 4 | 2 | 1 | 1 |
| Convalescents | 97 | 13 | 14 | 14 | 16 | 7 | 4 | 7 | 8 | 7 | 7 |
| Vaccinated with the first dose (2–3 weeks after vaccination) | |||||||||||
| Without prior SARS-CoV-2 infection | 19 | 6 | 2 | 1 | 2 | 2 | 0 | 2 | 0 | 2 | 2 |
| Convalescents | 9 | 1 | 1 | 3 | 3 | 0 | 0 | 0 | 0 | 0 | 1 |
| Vaccinated with the second dose (1–5 weeks after vaccination) | |||||||||||
| Without prior SARS-CoV-2 infection | 203 | 32 | 38 | 40 | 36 | 13 | 5 | 12 | 9 | 11 | 7 |
| Convalescents | 125 | 14 | 35 | 23 | 24 | 8 | 6 | 4 | 3 | 3 | 5 |
| Total | 477 | 70 | 92 | 84 | 86 | 30 | 17 | 29 | 22 | 24 | 23 |
| COVID-19 and/or Vaccination Status | IgG_concentration (BAU/mL) | ||||
| Mean | Median | Minimum | Maximum |  | |
| uninfected, unvaccinated | 3.57 | 3.20 | 3.20 | 8.56 | |
| asymptomatic SARS-recovered. unvaccinated | 112.59 | 94.95 | 3.20 | 296.40 | |
| symptomatic SARS-recovered. unvaccinated | 236.52 | 124.33 | 13.63 | 1,920.00 | |
| 2 weeks after the first vaccine dose. uninfected | 91.36 | 46.99 | 3.55 | 404.45 | |
| 3 weeks after the first vaccine dose.uninfected | 1,209.40 | 384.00 | 67.62 | 7,680.00 | |
| 3 weeks after the first vaccine dose. SARS-recovered | 4,397.00 | 3,989.00 | 1,666.00 | 10,068.00 | |
| 1 week after the second vaccine dose. uninfected | 2,228.53 | 1,747.20 | 106.02 | 7,045.00 | |
| 1 week after the second vaccine dose. SARS-recovered | 11,940.33 | 11,973.25 | 2,280.30 | 19,200.00 | |
| 2 weeks after the second vaccine dose. uninfected | 4,261.08 | 2,563.20 | 78.00 | 12,650.50 | |
| 2 weeks after the second vaccine dose. SARS-recovered | 10,241.42 | 10,375.75 | 198.70 | 19,638.00 | |
| 3 weeks after the second vaccine dose. uninfected | 3,327.63 | 3,039.60 | 880.00 | 8,677.00 | |
| 3 weeks after the second vaccine dose. SARS-recovered | 7,442.47 | 5,516.00 | 168.50 | 19,865.00 | |
| 4 weeks after the second vaccine dose. uninfected | 2,658.50 | 2,379.50 | 235.50 | 7,805.00 | |
| 4 weeks after the second vaccine dose. SARS-recovered | 4,490.81 | 4,196.50 | 210.50 | 10,391.50 | |
| 5 weeks after the second vaccine dose. uninfected | 2,474.46 | 2,294.50 | 166.00 | 9,836.50 | |
| 5 weeks after the second vaccine dose. SARS-recovered | 3,190.51 | 3,096.25 | 160.00 | 10,135.50 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tretyn, A.; Szczepanek, J.; Skorupa, M.; Jarkiewicz-Tretyn, J.; Sandomierz, D.; Dejewska, J.; Ciechanowska, K.; Jarkiewicz-Tretyn, A.; Koper, W.; Pałgan, K. Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 Recovery or Post-Vaccination. Cells 2021, 10, 1952. https://doi.org/10.3390/cells10081952
Tretyn A, Szczepanek J, Skorupa M, Jarkiewicz-Tretyn J, Sandomierz D, Dejewska J, Ciechanowska K, Jarkiewicz-Tretyn A, Koper W, Pałgan K. Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 Recovery or Post-Vaccination. Cells. 2021; 10(8):1952. https://doi.org/10.3390/cells10081952
Chicago/Turabian StyleTretyn, Andrzej, Joanna Szczepanek, Monika Skorupa, Joanna Jarkiewicz-Tretyn, Dorota Sandomierz, Joanna Dejewska, Karolina Ciechanowska, Aleksander Jarkiewicz-Tretyn, Wojciech Koper, and Krzysztof Pałgan. 2021. "Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 Recovery or Post-Vaccination" Cells 10, no. 8: 1952. https://doi.org/10.3390/cells10081952