
Safety and Efficacy of Single-Fraction Carbon-Ion Radiotherapy for Early-Stage Lung Cancer with Interstitial Pneumonia
 ,
,  , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Carbon-Ion Radiotherapy Procedure
2.3. Follow-Up
2.4. Chart Review
2.5. Patient Characteristics
3. Results
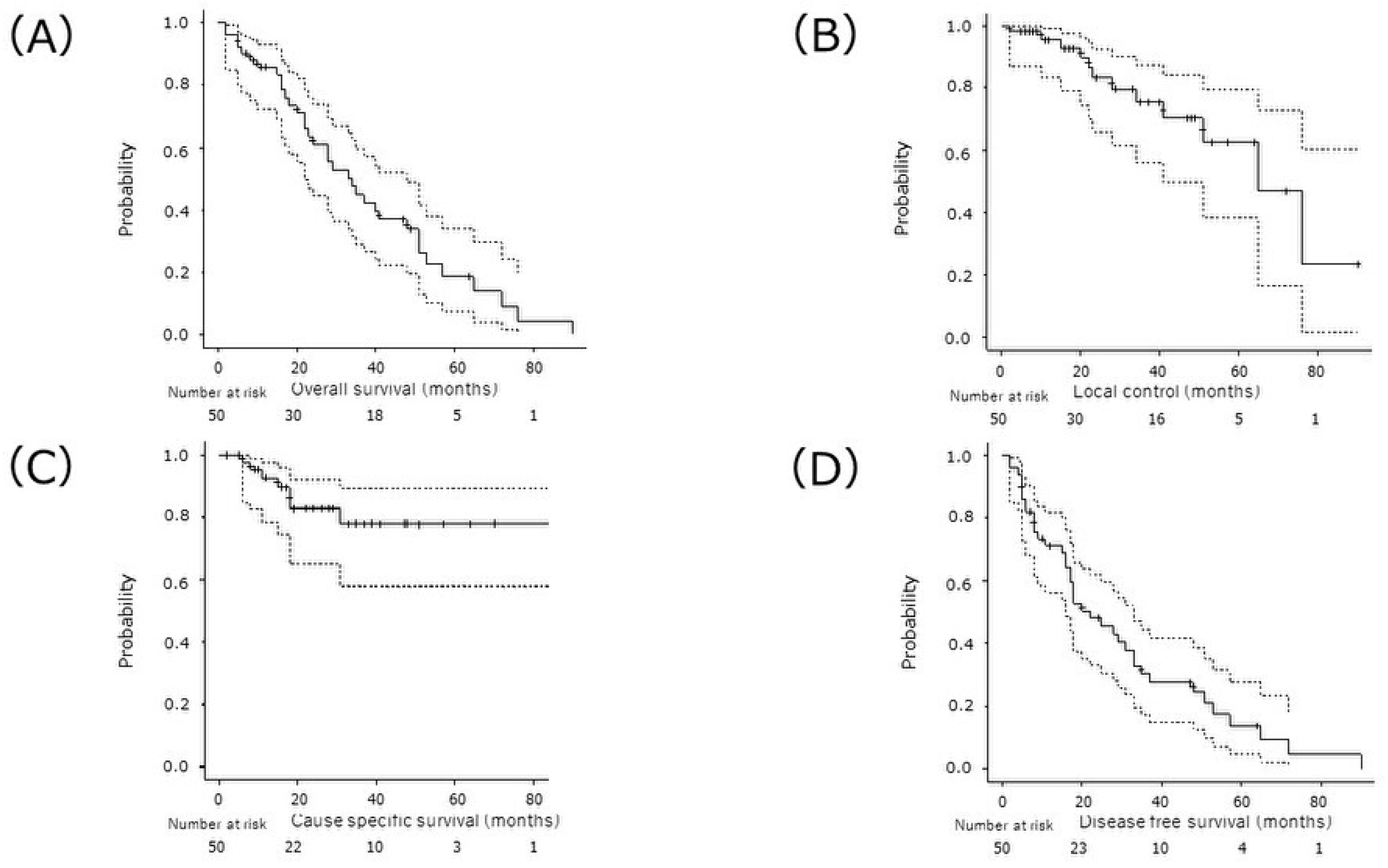
3.1. Treatment Outcomes
3.2. Prognostic Factors for OS
3.3. Adverse Events
4. Discussion
4.1. Radiation Therapy for IP-Complicated LC
4.2. Patient Background Related to Severe RP
4.3. Importance of Lung Doses
4.4. Treatment Effect
4.5. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oldham, J.M.; Collard, H.R. Comorbid Conditions in Idiopathic Pulmonary Fibrosis: Recognition and Management. Front. Med. 2017, 4, 123. [Google Scholar] [CrossRef]
- Ozawa, Y.; Suda, T.; Naito, T.; Enomoto, N.; Hashimoto, D.; Fujisawa, T.; Nakamura, Y.; Inui, N.; Nakamura, H.; Chida, K. Cumulative incidence of and predictive factors for lung cancer in IPF. Respirology 2009, 14, 723–728. [Google Scholar] [CrossRef]
- Ogura, T.; Takigawa, N.; Tomii, K.; Kishi, K.; Inoue, Y.; Ichihara, E.; Homma, S.; Takahashi, K.; Akamatsu, H.; Ikeda, S.; et al. Summary of the Japanese Respiratory Society statement for the treatment of lung cancer with comorbid interstitial pneumonia. Respir. Investig. 2019, 57, 512–533. [Google Scholar] [CrossRef]
- Ichihara, E.; Miyahara, N.; Maeda, Y.; Kiura, K. Managing Lung Cancer with Comorbid Interstitial Pneumonia. Intern. Med. 2020, 59, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Kondo, H.; Watanabe, A.; Nakajima, J.; Niwa, H.; Horio, H.; Okami, J.; Okumura, N.; Sugio, K.; Teramukai, S.; et al. A simple risk scoring system for predicting acute exacerbation of interstitial pneumonia after pulmonary resection in lung cancer patients. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Otsubo, K.; Kishimoto, J.; Ando, M.; Kenmotsu, H.; Minegishi, Y.; Horinouchi, H.; Kato, T.; Ichihara, E.; Kondo, M.; Atagi, S.; et al. Nintedanib plus chemotherapy for nonsmall cell lung cancer with idiopathic pulmonary fibrosis: A randomised phase 3 trial. Eur. Respir. J. 2022, 60, 2200380. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, S.; Kato, T.; Kenmotsu, H.; Ogura, T.; Sato, Y.; Hino, A.; Harada, T.; Kubota, K.; Tokito, T.; Okamoto, I.; et al. Atezolizumab for Pretreated Non-Small Cell Lung Cancer with Idiopathic Interstitial Pneumonia: Final Analysis of Phase II AMBITIOUS Study. Oncologist 2022, 27, 720-e702. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Azuma, K.; Sasada, T.; Okamoto, M.; Hattori, S.; Imamura, Y.; Yamada, K.; Tajiri, M.; Yoshida, T.; Zaizen, Y.; et al. Chemotherapy for non-small cell lung cancer complicated by idiopathic interstitial pneumonia. Oncol. Lett. 2012, 4, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Ichimura, T.; Hinata, M.; Ichikura, D.; Suzuki, S. Safety of immune checkpoint inhibitors in non-small-cell lung cancer patients with idiopathic interstitial pneumonia: A matched case–control study. Cancer Chemother. Pharmacol. 2022, 89, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, H.; Kobayashi-Shibata, S.; Terahara, A.; Okuma, K.; Haga, A.; Wakui, R.; Ohtomo, K.; Nakagawa, K. Prescreening based on the presence of CT-scan abnormalities and biomarkers (KL-6 and SP-D) may reduce severe radiation pneumonitis after stereotactic radiotherapy. Radiat. Oncol. 2010, 5, 32. [Google Scholar] [CrossRef]
- Glick, D.; Lyen, S.; Kandel, S.; Shapera, S.; Le, L.W.; Lindsay, P.; Wong, O.; Bezjak, A.; Brade, A.; Cho, B.J.; et al. Impact of Pretreatment Interstitial Lung Disease on Radiation Pneumonitis and Survival in Patients Treated with Lung Stereotactic Body Radiation Therapy (SBRT). Clin. Lung Cancer 2018, 19, e219–e226. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Nakayama, Y.; Kudo, S.; Hayakawa, T.; Nakamura, N.; Kitamoto, Y.; Takahashi, S.; Tsujino, K.; Kubo, N.; Tamaki, Y.; et al. Nationwide survey of radiation therapy in Japan for lung cancer complicated with interstitial lung disease. J. Radiat. Res. 2020, 61, 563–574. [Google Scholar] [CrossRef]
- Kanai, T.; Furusawa, Y.; Fukutsu, K.; Itsukaichi, H.; Eguchi-Kasai, K.; Ohara, H. Irradiation of mixed beam and design of spread-out bragg peak for heavy-ion radiotherapy. Radiat. Res. 1997, 147, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, D.; Kusunoki, T.; Takayama, Y.; Kusano, Y.; Minohara, S.; Kano, K.; Anno, W.; Tsuchida, K.; Takakusagi, Y.; Mizoguchi, N.; et al. Comparison of Dose Distribution between VMAT-SBRT and Scanning Carbon-ion Radiotherapy for Early-stage NSCLC. Anticancer. Res. 2021, 41, 4571–4575. [Google Scholar] [CrossRef] [PubMed]
- Wink, K.C.; Roelofs, E.; Simone, C.B.; Dechambre, D.; Santiago, A.; van der Stoep, J.; Dries, W.; Smits, J.; Avery, S.; Ammazzalorso, F.; et al. Photons, protons or carbon ions for stage I non-small cell lung cancer—Results of the multicentric ROCOCO in silico study. Radiother. Oncol. 2018, 128, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Demizu, Y.; Fujii, O.; Iwata, H.; Fuwa, N. Carbon ion therapy for early-stage non-small-cell lung cancer. BioMed Res. Int. 2014, 2014, 727962. [Google Scholar] [CrossRef] [PubMed]
- Hamada, N.; Imaoka, T.; Masunaga, S.-I.; Ogata, T.; Okayasu, R.; Takahashi, A.; Kato, T.A.; Kobayashi, Y.; Ohnishi, T.; Ono, K.; et al. Recent advances in the biology of heavy-ion cancer therapy. J. Radiat. Res. 2010, 51, 365–383. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Miyamoto, T.; Nakajima, M.; Karube, M.; Hayashi, K.; Tsuji, H.; Tsujii, H.; Kamada, T.; Fujisawa, T. A Dose Escalation Clinical Trial of Single-Fraction Carbon Ion Radiotherapy for Peripheral Stage I Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 673–680. [Google Scholar] [CrossRef]
- Ono, T.; Yamamoto, N.; Nomoto, A.; Nakajima, M.; Isozaki, Y.; Kasuya, G.; Ishikawa, H.; Nemoto, K.; Tsuji, H. Long Term Results of Single-Fraction Carbon-Ion Radiotherapy for Non-small Cell Lung Cancer. Cancers 2020, 13, 112. [Google Scholar] [CrossRef]
- Karube, M.; Yamamoto, N.; Nakajima, M.; Yamashita, H.; Nakagawa, K.; Miyamoto, T.; Tsuji, H.; Fujisawa, T.; Kamada, T. Single-Fraction Carbon-Ion Radiation Therapy for Patients 80 Years of Age and Older with Stage I Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 542–548. [Google Scholar] [CrossRef]
- Ono, T.; Yamamoto, N.; Nomoto, A.; Nakajima, M.; Iwai, Y.; Isozaki, Y.; Kasuya, G.; Ishikawa, H.; Nemoto, K.; Tsuji, H. The Risk Factors for Radiation Pneumonitis after Single-Fraction Carbon-Ion Radiotherapy for Lung Cancer or Metastasis. Cancers 2021, 13, 3229. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Ryerson, C.J.; Vittinghoff, E.; Ley, B.; Lee, J.S.; Mooney, J.J.; Jones, K.D.; Elicker, B.M.; Wolters, P.J.; Koth, L.L.; King, T.E.; et al. Predicting survival across chronic interstitial lung disease: The ILD-GAP model. Chest 2014, 145, 723–728. [Google Scholar] [CrossRef]
- Kondoh, S.; Chiba, H.; Nishikiori, H.; Umeda, Y.; Kuronuma, K.; Otsuka, M.; Yamada, G.; Ohnishi, H.; Mori, M.; Kondoh, Y.; et al. Validation of the Japanese disease severity classification and the GAP model in Japanese patients with idiopathic pulmonary fibrosis. Respir. Investig. 2016, 54, 327–333. [Google Scholar] [CrossRef]
- Miyamoto, T.; Baba, M.; Yamamoto, N.; Koto, M.; Sugawara, T.; Yashiro, T.; Kadono, K.; Ezawa, H.; Tsujii, H.; Mizoe, J.-E.; et al. Curative treatment of Stage I non–small-cell lung cancer with carbon ion beams using a hypofractionated regimen. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 750–758. [Google Scholar] [CrossRef]
- Nakajima, M.; Yamamoto, N.; Hayashi, K.; Karube, M.; Ebner, D.K.; Takahashi, W.; Anzai, M.; Tsushima, K.; Tada, Y.; Tatsumi, K.; et al. Carbon-ion radiotherapy for non-small cell lung cancer with interstitial lung disease: A retrospective analysis. Radiat. Oncol. 2017, 12, 144. [Google Scholar] [CrossRef]
- Mori, S.; Inaniwa, T.; Furukawa, T.; Zenklusen, S.; Shirai, T.; Noda, K. Effects of a difference in respiratory cycle between treatment planning and irradiation for phase-controlled rescanning and carbon pencil beam scanning. Br. J. Radiol. 2013, 86, 20130163. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, W.; Mori, S.; Nakajima, M.; Yamamoto, N.; Inaniwa, T.; Furukawa, T.; Shirai, T.; Noda, K.; Nakagawa, K.; Kamada, T. Carbon-ion scanning lung treatment planning with respiratory-gated phase-controlled rescanning: Simulation study using 4-dimensional CT data. Radiat. Oncol. 2014, 9, 238. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. Published 27 November 2017, Revised Version 4.0* 14 June 2010. Available online: http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf (accessed on 1 December 2023).
- Yamaguchi, S.; Ohguri, T.; Ide, S.; Aoki, T.; Imada, H.; Yahara, K.; Narisada, H.; Korogi, Y. Stereotactic body radiotherapy for lung tumors in patients with subclinical interstitial lung disease: The potential risk of extensive radiation pneumonitis. Lung Cancer 2013, 82, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Yoshitake, T.; Shioyama, Y.; Asai, K.; Nakamura, K.; Sasaki, T.; Ohga, S.; Kamitani, T.; Yamaguchi, T.; Ohshima, K.; Matsumoto, K.; et al. Impact of Interstitial Changes on Radiation Pneumonitis after Stereotactic Body Radiation Therapy for Lung Cancer. Anticancer. Res. 2015, 35, 4909–4913. [Google Scholar] [PubMed]
- Ueki, N.; Matsuo, Y.; Togashi, Y.; Kubo, T.; Shibuya, K.; Iizuka, Y.; Mizowaki, T.; Togashi, K.; Mishima, M.; Hiraoka, M. Impact of pretreatment interstitial lung disease on radiation pneumonitis and survival after stereotactic body radiation therapy for lung cancer. J. Thorac. Oncol. 2015, 10, 116–125. [Google Scholar] [CrossRef]
- Onishi, H.; Yamashita, H.; Shioyama, Y.; Matsumoto, Y.; Takayama, K.; Matsuo, Y.; Miyakawa, A.; Matsushita, H.; Aoki, M.; Nihei, K.; et al. Stereotactic Body Radiation Therapy for Patients with Pulmonary Interstitial Change: High Incidence of Fatal Radiation Pneumonitis in a Retrospective Multi-Institutional Study. Cancers 2018, 10, 257. [Google Scholar] [CrossRef]
- Liu, Y.; Zhu, Y.; Wu, R.; Hu, M.; Zhang, L.; Lin, Q.; Weng, D.; Sun, X.; Liu, Y.; Xu, Y. Stereotactic body radiotherapy for early stage non-small cell lung cancer in patients with subclinical interstitial lung disease. Transl. Lung Cancer Res. 2020, 9, 2328–2336. [Google Scholar] [CrossRef]
- Finazzi, T.; Ronden-Kianoush, M.I.; Spoelstra, F.O.B.; Nossent, E.J.; Nijman, S.F.M.; Bahce, I.; Dickhoff, C.; Senan, S. Stereotactic ablative radiotherapy in patients with early-stage non-small cell lung cancer and co-existing interstitial lung disease. Acta Oncol. 2020, 59, 569–573. [Google Scholar] [CrossRef]
- Tsurugai, Y.; Takeda, A.; Sanuki, N.; Enomoto, T.; Kaneko, T.; Hara, Y.; Mizuno, T.; Saeki, N.; Aoki, Y.; Oku, Y.; et al. Stereotactic body radiotherapy for lung cancer patients with idiopathic interstitial pneumonias. Radiother. Oncol. 2017, 125, 310–316. [Google Scholar] [CrossRef]
- Onishi, H.; Marino, K.; Yamashita, H.; Terahara, A.; Onimaru, R.; Kokubo, M.; Shioyama, Y.; Kozuka, T.; Matsuo, Y.; Aruga, T.; et al. Case Series of 23 Patients Who Developed Fatal Radiation Pneumonitis After Stereotactic Body Radiotherapy for Lung Cancer. Technol. Cancer Res. Treat. 2018, 17, 1533033818801323. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yoo, H.; Pyo, H.; Ahn, Y.C.; Noh, J.M.; Ju, S.G.; Lee, W.; Park, B.; Kim, J.M.; Kang, N.; et al. Impact of Underlying Pulmonary Diseases on Treatment Outcomes in Early-Stage Non-Small Cell Lung Cancer Treated with Definitive Radiotherapy. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 2273–2281. [Google Scholar] [CrossRef]
- Okano, N.; Suefuji, H.; Nakajima, M.; Tokumaru, S.; Kubo, N.; Yoshida, D.; Suzuki, O.; Ishikawa, H.; Satouchi, M.; Nakayama, H.; et al. Clinical results of carbon-ion radiotherapy for stage I non-small cell lung cancer with concomitant interstitial lung disease: A Japanese national registry study (J-CROS-LUNG). J. Radiat. Res. 2023, 64, i2–i7. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Iwata, H.; Hattori, Y.; Nakajima, K.; Nomura, K.; Hayashi, K.; Toshito, T.; Yamamori, E.; Akita, K.; Mizoe, J.-E.; et al. Outcomes of proton therapy for non-small cell lung cancer in patients with interstitial pneumonia. Radiat. Oncol. 2022, 17, 56. [Google Scholar] [CrossRef] [PubMed]
- Noh, J.M.; Yoo, H.; Lee, W.; Park, H.Y.; Shin, S.H.; Pyo, H. Prospective Study of Proton Therapy for Lung Cancer Patients with Poor Lung Function or Pulmonary Fibrosis. Cancers 2022, 14, 1445. [Google Scholar] [CrossRef]
- Saito, T.; Ohnishi, K.; Ishikawa, H.; Nakamura, M.; Hoshiai, S.; Numajiri, H.; Murofushi, K.N.; Mizumoto, M.; Okumura, T.; Sakurai, H. Hypofractionated Proton Beam Therapy for cT1-2N0M0 Non-small Cell Lung Cancer Patients With Interstitial Lung Disease. Anticancer. Res. 2021, 41, 5635–5642. [Google Scholar] [CrossRef] [PubMed]
- Okano, N.; Kubo, N.; Yamaguchi, K.; Kouno, S.; Miyasaka, Y.; Mizukami, T.; Shirai, K.; Saitoh, J.-I.; Ebara, T.; Kawamura, H.; et al. Efficacy and Safety of Carbon-Ion Radiotherapy for Stage I Non-Small Cell Lung Cancer with Coexisting Interstitial Lung Disease. Cancers 2021, 13, 4204. [Google Scholar] [CrossRef] [PubMed]
- Matson, S.M.; Baqir, M.; Moua, T.; Marll, M.; Kent, J.; Iannazzo, N.S.; Boente, R.D.; Donatelli, J.M.; Dai, J.; Diaz, F.J.; et al. Treatment Outcomes for Rheumatoid Arthritis-Associated Interstitial Lung Disease: A Real-World, Multisite Study of the Impact of Immunosuppression on Pulmonary Function Trajectory. Chest 2023, 163, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Diridollou, T.; Sohier, L.; Rousseau, C.; Angibaud, A.; Chauvin, P.; Gaignon, T.; Tas, M.; Lemerre, J.; Kerjouan, M.; Salé, A.; et al. Idiopathic pulmonary fibrosis: Significance of the usual interstitial pneumonia (UIP) CT-scan patterns defined in new international guidelines. Respir. Med. Res. 2020, 77, 72–78. [Google Scholar] [CrossRef]
- Takahara, Y.; Tanaka, T.; Ishige, Y.; Shionoya, I.; Yamamura, K.; Sakuma, T.; Nishiki, K.; Nakase, K.; Nojiri, M.; Kato, R.; et al. Risk factors for acute exacerbation in lung cancer complicated by interstitial lung disease with slight reticular shadows. Thorac. Cancer 2021, 12, 2758–2766. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Dickinson, P.; Shrimali, R.; Salem, A.; Agarwal, S. Is Thoracic Radiotherapy an Absolute Contraindication for Treatment of Lung Cancer Patients with Interstitial Lung Disease? A Systematic Review. Clin. Oncol. 2022, 34, e493–e504. [Google Scholar] [CrossRef] [PubMed]
- Kondoh, Y.; Taniguchi, H.; Kataoka, K.; Furukawa, T.; Ando, M.; Murotani, K.; Mishima, M.; Inoue, Y.; Ogura, T.; Bando, M.; et al. Disease severity staging system for idiopathic pulmonary fibrosis in Japan. Respirology 2017, 22, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Yan, T.; Zhou, X.; Cao, P.; Luo, C.; Zhou, L.; Xu, Y.; Liu, Y.; Xue, J.; Wang, J.; et al. Acute severe radiation pneumonitis among non-small cell lung cancer (NSCLC) patients with moderate pulmonary dysfunction receiving definitive concurrent chemoradiotherapy: Impact of pre-treatment pulmonary function parameters. Strahlenther. Onkol. 2020, 196, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Semrau, S.; Klautke, G.; Fietkau, R. Baseline cardiopulmonary function as an independent prognostic factor for survival of inoperable non–small-cell lung cancer after concurrent chemoradiotherapy: A single-center analysis of 161 cases. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Guerra, J.L.L.; Gomez, D.R.; Zhuang, Y.; Levy, L.B.; Eapen, G.; Liu, H.; Mohan, R.; Komaki, R.; Cox, J.D.; Liao, Z. Changes in pulmonary function after three-dimensional conformal radiotherapy, intensity-modulated radiotherapy, or proton beam therapy for non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e537–e543. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, S.; Zheng, S.; Lin, J.; Hu, S.; Zhuang, J.; Lin, Q.; Xie, X.; Zheng, K.; Zhang, W.; et al. The role of lung ultrasound B-lines and serum KL-6 in the screening and follow-up of rheumatoid arthritis patients for an identification of interstitial lung disease: Review of the literature, proposal for a preliminary algorithm, and clinical application to cases. Arthritis Res. Ther. 2021, 23, 212. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Rabaneda, E.F.; Atienza-Mateo, B.; Blanco, R.; Cavagna, L.; Ancochea, J.; Castañeda, S.; González-Gay, M. Efficacy and safety of abatacept in interstitial lung disease of rheumatoid arthritis: A systematic literature review. Autoimmun. Rev. 2021, 20, 102830. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, Y.; Nagata, Y.; Wakabayashi, M.; Ishikura, S.; Onishi, H.; Kokubo, M.; Karasawa, K.; Shioyama, Y.; Onimaru, R.; Hiraoka, M. Impact of pre-treatment C-reactive protein level and skeletal muscle mass on outcomes after stereotactic body radiotherapy for T1N0M0 non-small cell lung cancer: A supplementary analysis of the Japan Clinical Oncology Group study JCOG0403. J. Radiat. Res. 2021, 62, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Qiu, T.; Patel, N.; Zhou, S.; Xue, T.; Zhang, H. Clinical Management of Risk of Radiation Pneumonia with Serum Markers During the Radiotherapy for Patients with Thoracic Malignant Tumors. Cancer Manag. Res. 2019, 11, 10249–10256. [Google Scholar] [CrossRef]
- Lee, Y.H.; Kim, Y.S.; Lee, S.N.; Lee, H.C.; Oh, S.J.; Kim, S.J.; Kim, Y.K.; Han, D.H.; Yoo, I.R.; Kang, J.H.; et al. Interstitial Lung Change in Pre-radiation Therapy Computed Tomography Is a Risk Factor for Severe Radiation Pneumonitis. Cancer Res. Treat. 2015, 47, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Liu, H.; Wu, H.; Liang, S.; Xu, Y. Risk factors for radiation pneumonitis in lung cancer patients with subclinical interstitial lung disease after thoracic radiation therapy. Radiat. Oncol. 2021, 16, 70. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Nyberg, F.; Morgan, G. The epidemiology of interstitial lung disease and its association with lung cancer. Br. J. Cancer 2004, 91 (Suppl. S2), S3–S10. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.Y.; Kano, M.R. Stromal barriers to nanomedicine penetration in the pancreatic tumor microenvironment. Cancer Sci. 2018, 109, 2085–2092. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Factors | Median (IQR) |
|---|---|
| Follow-up period (months) | 23.5 (10–47.5) |
| Age (years) | 76 (71–81) |
| Gender (female: male) | 45:5 |
| ECOG-PS (0:1:2-) | 36:14:0 |
| Brinkman index | 900 (552–1245) |
| Pre-RT Laboratory Data | |
| serum KL-6 (U/L) | 753 (524–858) |
| serum SP-D (ng/L) | 109 (77–179.5) |
| serum CRP (mg/L) | 0.20 (0.1–0.64) |
| Pre-RT Respiratory function | |
| %VC (%) | 87.9 (71.1–100.2) |
| %FVC (%) | 78.6 (64.5–90.2) |
| %DLco (%) | 58.1 (46.1–74.5) |
| Operable (Yes:No) | 8:42 |
| SBRT feasibility (Yes:No) | 0:50 |
| UIP pattern (Yes No) | 32:18 |
| Autoimmune disease (Yes:No) | 9:41 |
| History of AEs (Yes:No) | 7:43 |
| Use of HOT (Yes:No) | 5:45 |
| Oral corticosteroid therapy (Yes:No) | 11:39 |
| Clinical stage (UICC7th) | |
| 1A | 32 |
| 1B | 13 |
| 2A | 4 |
| 2B | 1 |
| Tumor location | |
| Upper/Middle lobe | 22 |
| Lower lobe | 28 |
| Histology | |
| Adenocarcinoma | 7 |
| Squamous cell carcinoma | 10 |
| Clinically diagnosed | 33 |
| Characteristics | Median | IQR |
|---|---|---|
| GTV | ||
| Volume (mL) | 7.15 | (3.80–15.08) |
| Max dose | 50.63 | (50.43–51.18) |
| Min dose | 49.03 | (48.85–49.34) |
| Lung-GTV | ||
| MLD (Gy) | 2.63 | (1.87–3.18) |
| V5Gy (%) | 10.00 | (6.49–12.12) |
| V10Gy (%) | 7.59 | (5.23–10.23) |
| V20Gy (%) | 5.18 | (3.72–6.92) |
| Univariate | Multivariate | ||
|---|---|---|---|
| Variable | p-Value | p-Value | |
| Age | >75 vs. ≤75 | 0.32 | |
| Gender | male vs. female | 0.92 | |
| T stage (UICC8th) | 1 vs. 2 | 0.43 | |
| SpO2 | <90 vs. ≥90 | 0.60 | |
| History of AEs | Yes vs. No | 0.92 | |
| PSL | Yes vs. No | 0.75 | |
| Autoimmune disease | Yes vs. No | 0.44 | |
| UIP | Yes vs. No | 0.91 | |
| Respiratory function | |||
| %VC | <80 vs. ≥80 | 0.70 | |
| %DLco | <65 vs. ≥65 | 0.92 | |
| %FEV1 | <70 vs. ≥70 | 0.84 | |
| pre-CIRT serum markers | |||
| KL-6 | >500 vs. ≤500 | 0.22 | |
| SP-D | >110 vs. ≤110 | 0.53 | |
| CRP | >0.3 vs. ≤0.3 | 0.39 | |
| DVH parameter | |||
| lungV5 (%) | >10 vs. ≤10 | 0.030 * | |
| lungV20 (%) | >5 vs. ≤5 | 0.00050 * | 0.0012 * |
| mean lung dose (Gy) | >3 vs. ≤3 | 0.027 * |
| Case No. | RP Grade | Onset Time | c-Stage | Location | BI | rGAP Stage | Treatment | KL-6 | SP-D | CRP | UIP Pattern | V5 (%) | V20 (%) | MLD (Gy) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 1.5M | 1A2 | Rt-U | 1260 | 2 | 638 | 200 | 1.02 | + | 6.46 | 3.88 | 2.04 | |
| 2 | 2 | 4M | 1A3 | Rt-L | 900 | 3 | HOT, PSL | 805 | 65.6 | 0.12 | + | 12.87 | 7.21 | 3.27 |
| 3 | 3 | 6M | 1A3 | Lt-U | 900 | 2 | 1695 | 150 | 0.82 | + | 11.55 | 7.33 | 3.37 | |
| 4 | 3 | 3M | 1A2 | Lt-L | 800 | 2 | 388 | 52.9 | 0.07 | - | 6.68 | 3.88 | 1.9 | |
| 5 | 5 | 1M | 1B | Rt-L | 900 | 1 | 544 | 105 | 0.75 | + | 19.18 | 8.07 | 4.22 | |
| 6 | 5 | 1M | 1B | Lt-U | 680 | 3 | HOT, PSL | 824 | 106 | 0.59 | + | 8.64 | 5.48 | 2.75 |
| Pre-SBRT Factors | G2-5 RP | G0-1 RP | Total | p Value * | |
|---|---|---|---|---|---|
| Age | ≥75 | 4 | 25 | 29 | 1 |
| <75 | 2 | 18 | 20 | ||
| Gender | Male | 5 | 39 | 44 | 0.50 |
| Female | 1 | 4 | 5 | ||
| Smoking history | BI ≥ 1000 | 1 | 20 | 21 | 0.22 |
| BI < 1000 | 5 | 23 | 28 | ||
| UIP pattern in CT | (+) | 5 | 26 | 31 | 0.39 |
| (−) | (−) | 1 | 17 | 18 | |
| History of AEs | (+) | 1 | 6 | 7 | 1.00 |
| (−) | 5 | 37 | 42 | ||
| Severity of IP | SpO2 < 95% | 4 | 10 | 13 | 0.048 * |
| SpO2 ≥ 95% | 2 | 33 | 36 | ||
| Respiratory function | |||||
| %VC | <80% | 2 | 17 | 19 | 1.00 |
| ≥80% | 4 | 26 | 30 | ||
| %DLco | <65% | 5 | 25 | 30 | 0.38 |
| ≥65% | 1 | 18 | 19 | ||
| %FEV1 | <70% | 5 | 25 | 30 | 0.38 |
| ≥70% | 1 | 18 | 19 | ||
| Serum markers | |||||
| Serum KL-6 | ≥500 U/mL | 5 | 36 | 41 | 1.00 |
| <500 U/mL | 1 | 7 | 8 | ||
| Serum SP-D | ≥110 ng/mL | 2 | 20 | 22 | 0.67 |
| <110 ng/mL | 4 | 23 | 27 | ||
| Serum CRP | ≥0.3 mg/dL | 4 | 18 | 22 | 0.39 |
| <0.3 mg/dL | 2 | 25 | 27 | ||
| DVH parameters | |||||
| lung V5 | >10% | 3 | 22 | 25 | 1.00 |
| ≤10% | 3 | 21 | 24 | ||
| lung V20 | >5% | 4 | 22 | 26 | 0.67 |
| ≤5% | 2 | 21 | 23 | ||
| MLD | >3Gy | 3 | 15 | 18 | 0.66 |
| ≤3Gy | 3 | 28 | 31 | ||
| rGAP model | Stage 1 | 1 | 20 | 21 | |
| Stage 2 | 3 | 19 | 22 | ||
| Stage 3 | 2 | 4 | 6 |
| Auther | Year | Patients | Diagnosis | Modality | Total Dose | Fraction | Follow | OS2y | RP Grade (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n) | (Gy) | (M) | (%) | Grade2 | Grade3 | Grade4–5 | |||||
| Yamashita | 2010 | 13 | IP | SBRT | 48 | 4 | 14.7 | N/A | N/A | N/A | 54 |
| Tsurugai | 2017 | 42 | IIPs | SBRT | 40–60 | 8–22 | 32.4 | 42.2 | N/A | 12 | 0 |
| Hashimoto | 2019 | 29 | IP | Proton | 66–74 | 10–37 | 21.1 | 45 | 6.9 | 6.9 | 0 |
| Noh | 2020 | 15 | IPF | Proton | 60–69 | 4–30 | 19.8 | 43.9 | 20 | 20 | 13.3 |
| Present study | 49 | IP | Carbon | 50 | 1 | 23.5 | 60.8 | 4.1 | 4.1 | 4.1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aoki, S.; Ishikawa, H.; Nakajima, M.; Yamamoto, N.; Mori, S.; Omatsu, T.; Tada, Y.; Mizobuchi, T.; Ikeda, S.; Yoshino, I.; et al. Safety and Efficacy of Single-Fraction Carbon-Ion Radiotherapy for Early-Stage Lung Cancer with Interstitial Pneumonia. Cancers 2024, 16, 562. https://doi.org/10.3390/cancers16030562
Aoki S, Ishikawa H, Nakajima M, Yamamoto N, Mori S, Omatsu T, Tada Y, Mizobuchi T, Ikeda S, Yoshino I, et al. Safety and Efficacy of Single-Fraction Carbon-Ion Radiotherapy for Early-Stage Lung Cancer with Interstitial Pneumonia. Cancers. 2024; 16(3):562. https://doi.org/10.3390/cancers16030562
Chicago/Turabian StyleAoki, Shuri, Hitoshi Ishikawa, Mio Nakajima, Naoyoshi Yamamoto, Shinichiro Mori, Tokuhiko Omatsu, Yuji Tada, Teruaki Mizobuchi, Satoshi Ikeda, Ichiro Yoshino, and et al. 2024. "Safety and Efficacy of Single-Fraction Carbon-Ion Radiotherapy for Early-Stage Lung Cancer with Interstitial Pneumonia" Cancers 16, no. 3: 562. https://doi.org/10.3390/cancers16030562