
Strategy for Pediatric Patients with Relapsed or Refractory Anaplastic Lymphoma Kinase-Positive Anaplastic Large Cell Lymphoma: A Review

Department of Pediatrics, School of Medicine, Institute of Medical, Pharmaceutical and Health Sciences, Kanazawa University, 13-1 Takara-machi, Kanazawa 920-8641, Ishikawa, Japan
*
Author to whom correspondence should be addressed.
Cancers 2023, 15(24), 5733; https://doi.org/10.3390/cancers15245733
Submission received: 8 October 2023
/
Revised: 10 November 2023
/
Accepted: 28 November 2023
/
Published: 7 December 2023
(This article belongs to the Special Issue Pediatric Cancer: From Molecular Targets to Effective Therapies)
Abstract
:Simple Summary
Anaplastic lymphoma kinase (ALK)-positive anaplastic large cell lymphoma (ALCL) is an aggressive T-cell lymphoma characterized by large T-cells with strong CD30 and ALK expression. Approximately 30% of patients treated with conventional chemotherapy experience a relapse or refractory disease and have a poor prognosis. Several risk factors associated with poor prognosis have been identified in pediatric ALK-positive ALCL, such as the morphological pattern of the small cell variant or lymphohistiocytic variant, leukemic presentation, the presence of minimal disseminated disease, or involvement of the central nervous system. Relapsed or refractory ALK-positive ALCL requires salvage therapy. Recently, targeted therapies such as ALK inhibitors and brentuximab vedotin have demonstrated dramatic responses in chemoresistant ALK-positive ALCL. Hematopoietic stem cell transplantation has also been reported to be an effective therapy. This article reviews pediatric ALK-positive ALCL, focusing on the risk factors associated with poor prognosis and treatment strategies for relapsed or refractory disease.
Abstract
Anaplastic lymphoma kinase (ALK)-positive anaplastic large cell lymphoma (ALCL) is an aggressive T-cell lymphoma characterized by large T-cells with strong CD30 and ALK expression. Although conventional chemotherapy is effective in most patients, approximately 30% experience a relapse or refractory disease and have a poor prognosis. Several risk factors associated with poor prognosis have been identified in pediatric ALK-positive ALCL. These include morphological patterns with the small cell variant or lymphohistiocytic variant, leukemic presentation, the presence of minimal disseminated disease, or involvement of the central nervous system. Relapsed or refractory ALK-positive ALCL is often resistant to conventional chemotherapy; therefore, salvage therapy is required. In recent years, targeted therapies such as ALK inhibitors and brentuximab vedotin (BV) have been developed. ALK inhibitors block the continuous activation of ALK kinase, a driver mutation that leads to cell proliferation in ALK-positive ALCL. Additionally, BV is an antibody–drug conjugate that targets CD30-positive cells. Both ALK inhibitors and BV have displayed dramatic effects in chemoresistant ALK-positive ALCL. Weekly vinblastine treatment and hematopoietic stem cell transplantation have also been reported to be effective therapies. This article reviews pediatric ALK-positive ALCL, focusing on risk factors and treatment strategies for pediatric patients with relapsed or refractory ALK-positive ALCL.
1. Introduction
Anaplastic large cell lymphoma (ALCL) is an aggressive T-cell lymphoma characterized by large T-cells with strong CD30 expression [1]. Moreover, ALCL accounts for 10–15% of pediatric non-Hodgkin’s lymphoma cases and was first described in 1985 by Stein et al. [2]. ALCL is classified into two subtypes based on anaplastic lymphoma kinase (ALK) expression: ALK-positive ALCL and ALK-negative ALCL [3]. In pediatric patients, ALK-positive ALCL accounts for 80–100% of the cases, with a male predominance, whereas ALK-negative ALCL is more common in adults [1,2,4]. Although ALK-negative ALCL generally has a worse prognosis than ALK-positive ALCL in adults, pediatric patients with ALK-positive and ALK-negative ALCL have similar prognoses [4,5]. In more than 90% of patients with ALK-positive ALCL, a rearrangement of the ALK gene was detected. Specifically, nucleophosmin (NPM)-ALK was present in 80% of the cases, whereas tropomyosin 3 (TPM3)-ALK was present in 15% [6,7]. The NPM-ALK fusion gene results from a chromosomal translocation, t(2;5)(p23;q35), which brings together the ALK gene at 2p23 and the NPM gene at 5q35 [8]. Conventional chemotherapy is effective in treating ALK-positive ALCL and is associated with a favorable prognosis, with 5-year event-free survival rates (EFSs) ranging from 65 to 75% [9]. However, about 25–35% of ALK-positive ALCL patients experience relapsed or refractory disease. In addition, certain subtypes, such as “small cell variant” and “lymphohistiocytic variant,” have chemoresistant characteristics and poor prognosis, with a 5-year EFS of approximately 50% [10]. Relapsed or refractory ALK-positive ALCL is often resistant to conventional chemotherapy. Therefore, salvage therapy is required. In recent years, targeted therapies, such as ALK inhibitors and brentuximab vedotin (BV) have been developed, and they have demonstrated dramatic responses in chemoresistant ALK-positive ALCL [11,12,13]. Additionally, hematopoietic stem cell transplantation (HSCT) has been reported as an effective therapy for relapsed or refractory ALK-positive ALCL [14,15,16]. In this article, we review pediatric ALK-positive ALCL cases and discuss strategies for the treatment of pediatric patients with relapsed or refractory ALK-positive ALCL.
2. Clinical Features
ALK-positive ALCL typically manifests as a highly aggressive stage III to IV disease with systemic symptoms, especially high fever [1]. Extranodal lesions are frequently observed in ALK-positive ALCL (60%), such as those affecting the skin (19–21%), bone (17–19%), soft tissues (16–17%), bone marrow (11–12%), lungs (11–21%), and liver (8–14%) [4]. However, the involvement of the gut and central nervous system (CNS) is uncommon [4]. Bone marrow involvement is defined as the existence of ALCL cells in bone marrow determined through the analysis of the bone marrow smears.
3. Oncogenic Mechanism
Rearrangements of the ALK gene have been detected in more than 90% of patients with ALK-positive ALCL. The expression of the wild-type ALK protein is strictly restricted to a few scattered cells in the CNS from birth [8]. Upon ligand binding, the wild-type ALK protein undergoes homodimerization, which activates tyrosine kinases in the intracellular tail of the ALK molecule. The NPM-ALK fusion protein consists of an NPM oligomerization domain and an intracytoplasmic ALK region, including the tyrosine kinase domain. The expression of the NPM-ALK fusion gene is controlled by the NPM promoter, resulting in the continuous production of the NPM-ALK protein [17]. Homodimerization of the NPM-ALK protein by the NPM oligomerization domain activates ALK tyrosine kinase, leading to cell proliferation [1]. Even in TPM3 or tropomyosin-receptor kinase fused (TFG) genes, which are other partner genes of the ALK gene and include a dimerization domain, homodimerization of each fusion protein by dimerization domains contributes to the activation of ALK tyrosine kinase and oncogenic activity [1].
4. Risk Factors with Poor Prognosis
Several risk factors associated with poor prognosis have been identified in pediatric ALK-positive ALCL. These include morphological patterns with the small cell variant or lymphohistiocytic variant, leukemic presentation, MDD, and CNS involvement [18,19].
4.1. Morphological Pattern
The common type of ALK-positive ALCL is characterized by large tumor cells with horseshoe-shaped nuclei, abundant cytoplasm containing numerous vacuoles, and strong positive staining for ALK and CD30 [1]. The small cell variant is a subtype of ALK-positive ALCL characterized by the coexistence of mainly small tumor cells that stain negative or weakly positive for ALK and CD30, along with a minor population of large tumor cells that stain strongly positive for ALK and CD30 [1]. Additionally, the small cell variant accounts for 6% of all ALK-positive ALCL cases [20]. The small cell variant has been identified as a risk factor for relapsed or refractory diseases [18]. Small tumor cells in the small cell variant have been reported to be more resistant to chemotherapy than large tumor cells [21].
The lymphohistiocytic variant is characterized by numerous histiocytes surrounding CD30-positive large tumor cells [1]. Immunohistochemistry revealed that the histiocytes were negative for the nuclear proliferation marker Ki-67, indicating that they had assembled reactively rather than were undergoing neoplastic proliferation [1]. The lymphohistiocytic variant has been reported to be a risk factor for relapsed or refractory disease [18].
4.2. Leukemic Presentation
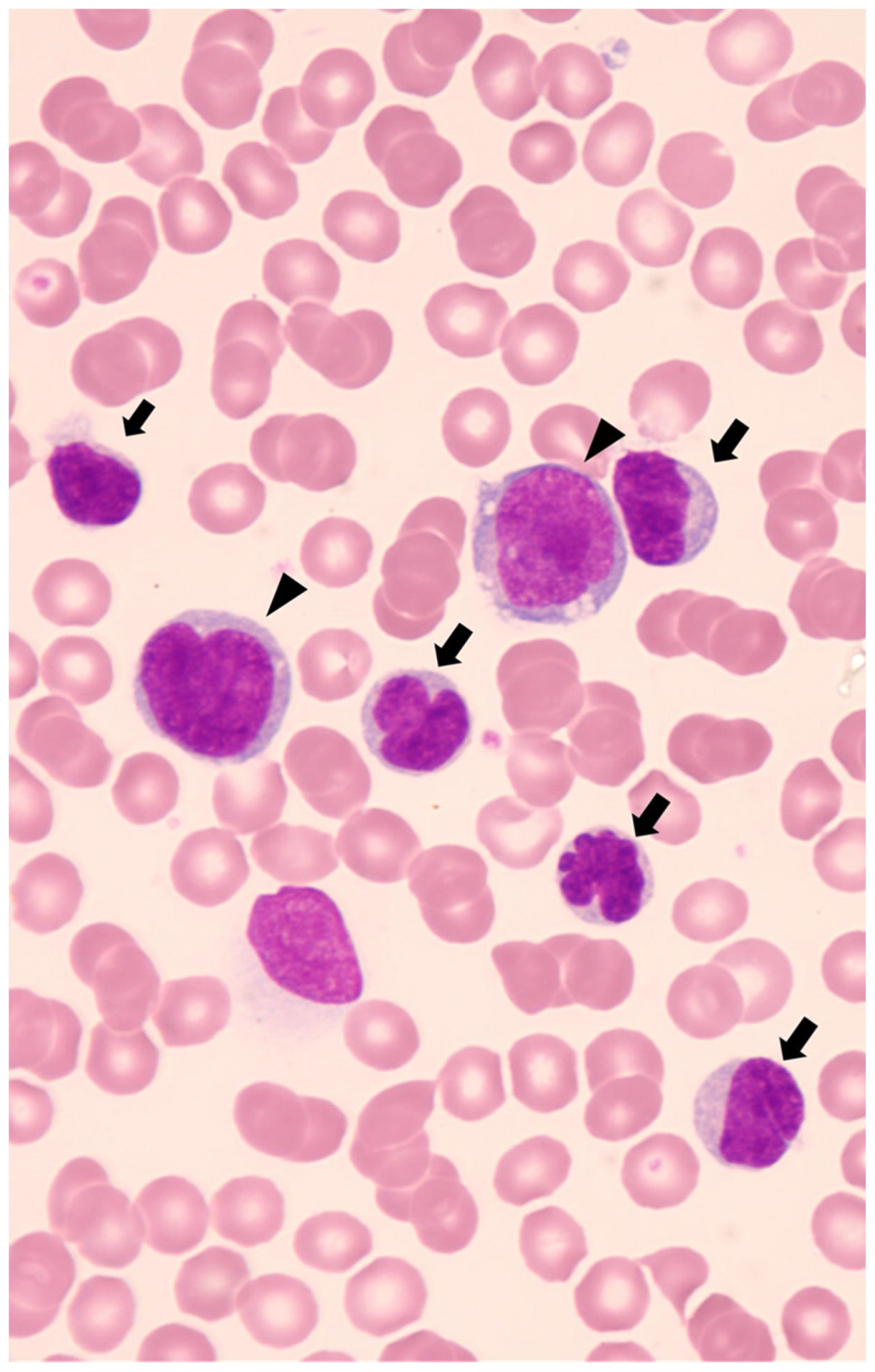
Leukemic presentation is defined as the presence of circulating ALCL cells in peripheral blood and is associated with an extremely poor prognosis. Leukemic presentation is extremely rare, accounting for less than 5% of all ALCL cases, and 75% of patients with leukemic presentation have a small cell variant histology [22]. Furthermore, most pediatric patients with leukemic presentation are associated with the NPM-ALK fusion gene. Diffuse lung infiltrates, respiratory distress, and pleural effusion are characteristic clinical features of leukemic presentation and have been reported in 50% of patients [22]. The diagnosis of ALK-positive ALCL with a leukemic presentation can be challenging because the condition mimics T-cell leukemia [22]. Identification of lymphoma cells with characteristic karyomorphism, such as “flower-cell” or “cerebriform cell,” will contribute to the diagnosis of leukemic presentation. (Figure 1) Moreover, when these characteristic cells present immunophenotypic findings as CD30- and ALK-positive, they can assist in the diagnosis of ALK-positive ALCL with a leukemic presentation [22]. Notably, lymphoma cells in peripheral blood often express myeloid-associated antigens, including CD13, CD11b, and lysozyme [22]. Whereas we encountered a patient with a leukemic presentation of a small cell variant whose circulating small tumor cells exhibited low expression of CD30 and ALK on immunohistochemistry and flow cytometry, with only one-tenth of NPM-ALK mRNA expression compared to large tumor cells [21]. This case highlights the importance of careful examination of cell morphology, even if CD30 and ALK expression in circulating tumor cells is low. Additionally, the lower percentage of tumor cells in the bone marrow than in the peripheral blood may contribute to the diagnosis of leukemic presentation [23]. As leukemic presentation has a very poor prognosis, an accurate diagnosis is crucial for selecting effective salvage therapies.
4.3. Minimal Disseminated Disease
Minimal disseminated disease (MDD) is defined as a minimal lesion detected in the peripheral blood and/or bone marrow using PCR to target the ALK-associated fusion gene. The NPM-ALK fusion gene is commonly targeted in many reports [18].
With regard to the PCR methods used to detect MDD, qualitative PCR (RT-PCR), RQ-PCR, and digital PCR (dPCR) have been reported. Damm-Welk et al. described that the sensitivity of RT-PCR was 10−5 NPM-ALK-positive cells per control cells [24]. In total, 48–61% of patients have a positive RT-PCR result in bone marrow, which indicates a poorer prognosis compared to those with a negative RT-PCR result [23,24,25]. They reported that, in positive and negative RT-PCR, the cumulative incidence of relapse was 50% and 15%, 5-year EFS was 38% and 82%, and 5-year OS was 60% and 86%, respectively [24]. The RQ-PCR method for NPM-ALK detects each copy number of NPM-ALK and internal control genes such as ABL. Then, NPM-ALK copy numbers are normalized using the copy numbers of internal control gene. The normalized copy numbers (NCNs) have been defined as NPM-ALK copy numbers per 104 copies of ABL in several reports [24,26]. More than 10 NCNs are related to poor prognosis [24,26]. Damm-Welk et al. reported that in more than 10 NCNs and 10 or fewer NCNs in bone marrow, the cumulative incidence of relapse was 71% and 18%, 5-year EFS was 23% and 78%, and 5-year OS was 46% and 85%, respectively [24].In recent years, MDD detection using dPCR has been reported [27]. More than 30 NCNs have been linked poor prognosis [27,28]. A study by Damm-Welk et al. revealed that the 5-year progression-free survival (PFS) was 35%, 69%, and 74% for patients with more than 30 NCNs, 30 or fewer NCNs, and negative in bone marrow, respectively [27]. Although MDD quantification using the RQ-PCR method cannot be compared across different laboratories and international settings, the dPCR method demonstrates high inter-laboratory reproducibility [27].
4.4. CNS Involvement
In pediatric patients with ALCL, CNS involvement is rare, occurring in only 2.6% of cases [19]. Solitary ALCL localized in the CNS has been reported in only three cases [19]. Recently, CNS involvement was identified as a poor prognostic factor. Patients with CNS involvement have a worse prognosis than those with common ALK-positive ALCL, with a 5-year overall survival (OS) of 74% and 5-year EFS of 50% [19]. The lymphohistiocytic variant morphology and leukemic presentation have been reported as risk factors for CNS involvement. In particular, 36% of the patients with lymphohistiocytic variants developed CNS involvement [23].
5. Treatment
5.1. Treatment for Newly Diagnosed ALK-Positive ALCL
Anthracycline-based combination chemotherapy is the standard treatment for pediatric patients with newly diagnosed ALK-positive ALCL. Various national groups have reported the outcomes of treatment for patients with newly diagnosed ALCL (Table 1) [18,29,30,31,32,33,34,35]. The largest trial was the ALCL99 trial (NCT00006455), which included 420 pediatric and young adult patients with ALCL. Of these, 404 were ALK-positive and 16 were ALK-negative. The 5-year OS rate was 91% and the 5-year PFS was 72% [18]. Patients with the morphological pattern of the small cell variant or lymphohistiocytic variant had a poor prognosis, with a 10-year PFS of 50% compared to 79% for other morphologies (p < 0.0001) [18]. Patients with the small cell variant or lymphohistiocytic variant often exhibit a refractory course and require salvage therapies.
The Children’s Oncology Group (COG) has recently released the interim results of the ANHL12P1 trial, which examined the ALCL99 regimen with BV (arm BV) or crizotinib (arm crizotinib) for pediatric patients with newly diagnosed ALK-positive ALCL (NCT01979536). The arm BV included 68 patients with ALK-positive ALCL, with a 2-year OS of 97% and a 2-year EFS of 79% [36]. The addition of BV did not increase toxicity [25]. The crizotinib arm included 66 patients, with a 2-year OS of 95% and a 2-year EFS of 77% [37]. The addition of crizotinib increased thromboembolic events, which 13 out of 66 patients experienced [37]. In this study, the morphological subtypes were not analyzed.
The CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) regimen is recommended in adult patients with newly diagnosed ALCL. For adult patients with limited stages, involved site radiation therapy is also generally recommended. A recent study by Horwitz et al. reported the results of the ECHELON-2 phase 3 trial of the A+CHP regimen, which is a BV with combination chemotherapy consisting of cyclophosphamide, doxorubicin, and prednisone (CHP) for adult patients with newly diagnosed CD30-positive peripheral T-cell lymphoma, including ALCL (NCT01777152) [38]. The study reported that the A+CHP regimen had a better median PFS compared to the CHOP regimen (48.2 months vs. 20.8 months, p = 0.011), while the risk of adverse events was equivalent in both regimens. Consequently, the A+CHP regimen is considered a more effective treatment option for adult patients, positioning the modality as the standard next-generation treatment [38].
5.2. Treatment for Relapsed or Refractory ALK-Positive ALCL
No established standard treatment is available for relapsed or refractory ALK-positive ALCL. However, several treatments have been reported to be effective, including weekly vinblastine, BV, and ALK inhibitors. In addition, nivolumab has also been reported as a potential new treatment option. After complete remission, HSCT has also been reported as a curative treatment for relapsed or refractory ALK-positive ALCL (Table 2).
5.2.1. Weekly Vinblastine
A report by the French Society for Pediatric Oncology (SFOP) highlighted the effectiveness of weekly vinblastine treatment (6 mg/m2/week) in pediatric patients with relapsed or refractory ALK-positive ALCL. Of the 30 evaluable patients, 25 (83%) patients achieved a complete response (CR) after weekly vinblastine treatment [9]. Notably, seven patients remained in CR for more than 2 years after the end of vinblastine treatment without HSCT. This indicated that vinblastine treatment has the potential to be curative. Vinblastine re-administration was also effective in patients with relapse who terminated the vinblastine salvage therapy. Six of the seven patients with relapse achieved CR with vinblastine treatment [9]. The 5-year OS was 65% and the 5-year EFS was 30% [9]. However, the optimal duration of treatment remains unclear. Notably, as vinblastine has a low penetrance into the CNS, relapse in the CNS requires caution during vinblastine treatment [46]. The most common adverse event with weekly vinblastine administration was mild leukopenia (34%) [9,39]. The incidence of extrahematological toxicity was low.
5.2.2. Brentuximab Vedotin
Brentuximab vedotin (BV) is an antibody–drug conjugate that targets CD30-positive cells. The CD30-antibody is linked to the microtubule-disrupting agent monomethyl auristatin E (MMAE) [11]. Locatelli et al. reported the results of a phase 1/2 study on BV in pediatric patients with relapsed or refractory ALCL (NCT01492088). The study included 17 pediatric patients with ALCL, of whom 12 were ALK-positive and 5 were ALK-negative. The overall response rate was 53%, with a CR rate of 41% (7 of the 17 patients). Notably, 9 of the 17 patients had undergone HSCT [11]. In adult patients with ALCL, Pro et al. reported the results of a phase 2 study of BV with relapsed or refractory ALCL (NCT00866047). The study included 57 adult patients, 16 of whom were ALK-positive, and 42 were ALK-negative. The overall response rate was 86%, with a CR rate of 57% (33 of the 58 patients) [12]. The 5-year OS rate of all patients treated with BV was 60%. This study also revealed that the 5-year PFS rates in patients with or without consolidative HSCT after BV treatment were 69% and 48%, respectively [13]. The 5-year OS rates were 75% and 81%, respectively [13]. Thus, consolidative HSCT improved the PFS in patients with CR who responded to BV treatment. Intriguingly, 8 of the 58 patients (14%) remained in sustained CR for more than 5 years without HSCT or other treatments. This result suggests that BV has the potential to cure relapsed or refractory ALCL [13]. Notably, as BV has low penetrance into the CNS, relapse in the CNS requires caution during BV treatment [46].
The most common adverse events in the 36 pediatric patients treated with BV were fever (44%), nausea (36%), and peripheral neuropathy (33%) [11]. Peripheral neuropathy with BV is caused by tubulin inhibition by MMAE and is dose-limiting and cumulative [47]. However, the aforementioned effects are typically transient and reversible. According to a report by Locatelli et al., 11 of 12 patients who developed peripheral neuropathy with BV recovered without sequela [11]. The most common grade 3 and higher adverse events were a decrease in neutrophil count (11%), increased gamma-glutamyl transpeptidase (6%), and fever (6%) [11]. Similar adverse events have been observed in adult and pediatric patients treated with BV. Among the 58 adult patients treated with BV, the most common adverse events were peripheral neuropathy (41%), nausea (40%), and fever (34%). The most common grade 3 and higher adverse events were decreased neutrophil count (21%), thrombocytopenia (14%), and peripheral neuropathy (12%) [12]. In adult patients, peripheral neuropathy is also the most transient and reversible, as 30 of 33 patients with BV-related peripheral neuropathy recovered [13]. Pancreatitis and progressive polyfocal leukoencephalopathy are rare, severe adverse events [48,49].
Repeated BV administration may lead to acquired drug resistance. Some studies have suggested that drug resistance is caused by resistance to MMAE, multidrug resistance protein 1 upregulation, and CD30 downregulation [50,51]. While some reports indicated that CD30 expression does not affect the efficacy of BV [47,52]. The contribution of CD30 downregulation in BV drug resistance remains controversial.
5.2.3. ALK Inhibitors
Continuous activation of ALK kinase caused by the ALK fusion protein is a driver mutation in ALK-positive ALCL, leading to the continuous growth of cancer cells. Therefore, ALK inhibitors have been developed to prevent the proliferation of cancer cells. Moreover, ALK inhibitors have displayed a high overall response rate in relapsed and refractory ALK-positive ALCL. These inhibitors were initially developed for ALK-rearrangement non-small cell lung cancer (NSCLC) [53]. Currently, five ALK inhibitors have been developed: crizotinib, alectinib, ceritinib, brigatinib, and lorlatinib. They are classified into first to third generations, and only the first-generation ALK inhibitor crizotinib and second-generation ALK inhibitor alectinib have been approved for ALK-positive ALCL. Crizotinib was approved by the United States Food and Drug Administration (FDA) in 2021, and alectinib was approved by the Ministry of Health, Labour and Welfare of Japan in 2020. Although the second-generation ALK inhibitor ceritinib has not been approved for ALK-positive ALCL, several studies have indicated that ceritinib is effective for relapsed or refractory ALK-positive ALCL [42,54].
Crizotinib
Crizotinib is a first-generation ALK inhibitor approved for patients with relapsed or refractory ALK-positive ALCL in the United States of America in 2021. The COG reported the results of a clinical trial of crizotinib in pediatric patients with relapsed or refractory ALK-positive ALCL (NCT00939770). This study included 26 patients with ALK-positive ALCL. The overall response rate was 88%, with a CR rate of 81% (21 of the 26 patients) [43]. Eventually, 12 of 26 patients underwent HSCT. Currently, whether crizotinib has the potential to treat relapsed or refractory ALCL is unknown. Therefore, after achieving CR with crizotinib treatment, patients may undergo HSCT or continue receiving crizotinib as maintenance therapy. The most common grade 3 and higher adverse event was a decrease in the neutrophil count, which was reported in 33% of patients treated with crizotinib at a 165 mg/m2/dose and 70% of patients treated with a 280 mg/m2/dose [43]. Visual disturbances such as photopsia, blurred vision, and vitreous floaters are also common adverse events reported in adult patients, with an incidence rate of 40–60% [40,55]. These visual disturbances were mostly transient and occurred within the first week of initiating crizotinib treatment [55]. Adverse gastrointestinal events, including nausea (54%), diarrhea (42%), vomiting (41%), and constipation (29%) were also commonly reported in adult patients who received crizotinib [40].
When crizotinib is used as maintenance therapy, the optimal timing of crizotinib discontinuation remains unclear. Even if patients achieve and maintain CR for several years with crizotinib maintenance therapy, immediate relapse caused by crizotinib discontinuation has been reported in both pediatric and adult patients [56]. In this study, two patients who had been in CR for 45 and 27 months relapsed within 20 days after discontinuing crizotinib [56]. Notably, since crizotinib has low CNS penetrance, CNS relapse requires caution during crizotinib treatment [46,57]. Repeated crizotinib administration may lead to acquired drug resistance. Some studies on both ALK-positive ALCL and ALK-positive NSCLC have suggested that acquired resistance to crizotinib is linked to various mutations in ALK, including the L1196M ALK mutation, known as the gatekeeper mutation in the ALK kinase domain [58,59].
Alectinib
Alectinib is a second-generation ALK inhibitor that overcomes various crizotinib-resistant ALK mutations, including the L1196M gatekeeper mutation [60]. Fukano et al. reported the results of a phase 2 trial of alectinib in pediatric patients with relapsed or refractory ALK-positive ALCL (UMIN000016991). In this study, patients received oral doses of alectinib 300 mg twice daily, except for those weighing less than 35 kg, who received 150 mg twice daily. This study included 10 patients with ALK-positive ALCL. The overall response rate was 80%, with a CR rate of 60% (6 of the 10 patients) [61]. Eventually, 2 of the 10 patients underwent allogeneic HSCT in CR following alectinib treatment.
Alectinib is associated with a low incidence of adverse gastrointestinal events. Furthermore, gastrointestinal adverse events such as nausea, vomiting, and diarrhea have been reported in less than 15% of adult patients with NSCLC who received alectinib. The frequency of gastrointestinal adverse events of alectinib was lower than that of other ALK inhibitors [40]. The most common grade 3 or higher adverse event was a decrease in neutrophil count (20%) [61]. Currently, whether alectinib has the potential to treat relapsed or refractory ALCL is unknown. Therefore, after achieving CR with alectinib treatment, patients may undergo HSCT or continue to receive alectinib as maintenance therapy. Several patients have been reported to survive for over a year with continuous alectinib administration as well-tolerated maintenance therapy [41,61].
Although alectinib overcomes various crizotinib-resistant ALK mutations, continuous administration of alectinib induces acquired drug resistance caused by ALK mutation in patients with NSCLC and ALK-positive ALCL [62,63]. Additionally, the gatekeeper L1196M ALK mutation, which is usually overcome by alectinib, can also lead to alectinib resistance. An in vitro study demonstrated that echinoderm microtubule-associated protein-like 4 (EML4)-ALK-expressing cells that acquired L1196M ALK mutations were more susceptible to alectinib than crizotinib but less susceptible to alectinib than cells with wild-type ALK [62]. We have reported a pediatric patient with relapsed ALK-positive ALCL caused by an acquired L1196M ALK mutation during alectinib administration [63]. The most notable characteristic of alectinib is the high penetrance of the drug in the CNS, in contrast to crizotinib, vinblastine, and BV. A linear relationship exists between the concentration of alectinib in the cerebrospinal fluid and the unbound systemic concentration [40]. Alectinib has been reported to be effective in treating patients with relapsed or refractory CNS lesions caused by ALK-positive ALCL [21,64].
Ceritinib
Ceritinib is a second-generation ALK inhibitor. Although the drug has not yet been approved for ALK-positive ALCL, one study reported that three patients with relapsed or refractory ALK-positive ALCL were treated with ceritinib, of which two patients achieved CR and one patient achieved partial response [54]. Additionally, an independent report indicated that ceritinib treatment led to CR in a patient with relapsed and refractory ALK-positive ALCL [42]. In a previous study investigating the susceptibility of EML4-ALK expressing cells with various ALK mutations to ALK inhibitors, ceritinib proved effective against crizotinib- and alectinib-resistant ALK mutations such as I1171N and I1171S [62]. Currently, whether ceritinib has the potential to cure relapsed or refractory ALCL is unknown. Adverse gastrointestinal events, including nausea (82%), diarrhea (75%), vomiting (65%), and constipation (32%), are commonly reported in adult patients with NSCLC who receive ceritinib [65]. The most common grade 3 or higher adverse events reported were an increase in the levels of alanine aminotransferase (21%), aspartate aminotransferase (11%), and lipase (7%), along with an increase in diarrhea (7%) [65].
5.2.4. Nivolumab
Nivolumab is an antibody that blocks the ligand activation of the programmed death-1 cell receptor (PD-1). The programmed death ligand 1(PD-L1), which is activated by the NPM-ALK fusion protein, leads to PD1 activation, resulting in immune system suppression and allowing the tumor to evade immune control. Several patients with relapsed or refractory ALK-positive ALCL have been reported to respond to nivolumab and achieve CR [44,45]. The NIVO-ALCL trial (NCT 03703050) is based on these findings and is ongoing to test nivolumab monotherapy as a consolidative immunotherapy or in case of progression after target therapies in patients with relapsed or refractory ALCL.
5.2.5. Hematopoietic Stem Cell Transplantation
Hematopoietic stem cell transplantation (HSCT) can be a curative treatment if used in consolidation for relapsed or refractory ALK-positive ALCL. Autologous and allogeneic HSCT have also been previously reported.
Autologous HSCT
At first, the SFOP reported the effectiveness of HSCT in 15 pediatric patients with relapsed ALCL, including 14 autologous and 1 allogeneic HSCT [66]. The result demonstrated a 3-year DFS of 45%. Woessmann et al. analyzed 37 pediatric patients with relapsed ALCL who underwent reinduction chemotherapy followed by autologous HSCT. The results demonstrated a 5-year EFS of 59 ± 8% and a 5-year OS of 77 ± 7% after the first relapse [14]. This study also revealed that the timing of first relapse and CD3 expression in lymphoma cells significantly affected the outcomes of autologous HSCT. Patients who underwent autologous HSCT for relapse during the frontline therapy had a very poor prognosis, with an EFS of 0%. Furthermore, patients with CD3-positive ALCL who underwent autologous HSCT had a worse prognosis than those with CD3-negative ALCL (EFS:18% vs. 72%). Therefore, allogeneic HSCT is recommended for patients with relapse during the frontline therapy and CD3-positive ALCL [14]. Several studies have compared the effectiveness of autologous and allogeneic HSCT and found that allogeneic HSCT leads to better EFS rates than autologous HSCT [67]. Gross et al. reported a higher 5-year EFS for allogeneic HSCT (46%) compared to autologous HSCT (35%) [68]. Similarly, Fukano et al. reported that allogeneic HSCT showed better EFS than autologous HSCT: 5-year EFS 50% vs. 38% [40].
Moreover, Knorr et al. have recently reported the results of the ALCL-Relapse trial (NCT00317408): autologous HSCT was less effective for pediatric patients who experienced early relapse within one year after initial diagnosis [69]. In their study, autologous HSCT was less effective than allogeneic HSCT in patients with early relapse, regardless of CD3 positivity. The 5-year EFS for CD3-positive ALCL patients was 25% with autologous HSCT, compared to 65% with allogeneic HSCT. Similarly, the 5-year EFS for CD3-negative ALCL patients was 30% with autologous HSCT, compared to 78% with allogeneic HSCT. Given this, the authors concluded that autologous HSCT should not be undertaken as consolidation therapy for pediatric patients with relapsed or refractory ALCL [69].
Allogeneic HSCT
Strullu et al. reported the effectiveness of allogeneic HSCT in 34 pediatric patients with relapsed or refractory ALK-positive ALCL. The 5-year OS was 70% and the 5-year EFS was 58% [15]. In another study, the Berlin-Frankfurt-Munster group (BFM) reported the efficacy of allogeneic HSCT in 20 pediatric patients with relapsed or refractory ALK-positive ALCL. The 3-year EFS was 75% [16]. Allogeneic HSCT is also effective in patients with chemotherapy-resistant diseases, suggesting a graft-versus-ALCL effect [16]. As mentioned above, several studies comparing the effects of autologous and allogeneic HSCT discovered that allogeneic HSCT resulted in better EFS rates compared to autologous HSCT [67]. However, up-front allogeneic HSCT is not recommended for ALK-positive ALCL patients who achieve a partial or complete response following induction therapy [70]. The efficacy of up-front allogeneic HSCT has not been reported, even in patients with risk factors for poor prognosis, such as morphological patterns with small cell variant or lymphohistiocytic variant, leukemic presentation, MDD, and CNS involvement.
In conditioning regimens followed by allogeneic HSCT, the reduced-intensity conditioning (RIC) regimen resulted in better outcomes than the myeloablative conditioning (MAC) regimen [71]. Fukano et al. reported that the RIC regimen leads to better OS and EFS as compared to the MAC regimen: 5-year OS 100% vs. 48.5% and 5-year EFS 87.5% vs. 42.8% [71]. By reducing treatment-related mortality, the RIC regimen may improve allogeneic HSCT outcomes compared to the MAC regimen. The JPLSG-ALCL-RIC18 trial is ongoing in Japan to test the efficacy of the RIC regimen followed by allogeneic HSCT.
Patients with a leukemic presentation of refractory ALK-positive ALCL may require allogeneic HSCT. As ALK-positive ALCL with leukemic presentation is extremely rare, no consensus on the standard treatment is present [23]. Out of the 24 patients previously reported in the literature with leukemic presentation, including the information on their survival status, only 8 patients (33%) were alive [20,21,22,23,72,73,74,75,76,77,78,79]. The eight patients with leukemic presentation are summarized in Table 3 [20,21,22,23,72,74]. Of the eight patients, only two achieved a CR after frontline chemotherapy (cases 1 and 2). The patients survived without additional treatment, including HSCT. In contrast, the remaining six patients who did not achieve CR with frontline chemotherapy received salvage chemotherapy. Four out of six patients who achieved CR underwent HSCT as consolidation therapy, while the remaining two patients who achieved non-CR after salvage chemotherapy underwent HSCT as salvage therapy. All three patients who provided information about their conditioning regimen received total-body irradiation (TBI) as part of their treatment. Furthermore, all four patients reported that their donor source was allogeneic HSCT. Therefore, allogeneic HSCT with a TBI conditioning regimen may be necessary for patients with chemoresistant ALK-positive ALCL with a leukemic presentation.
An important point to note is that the high incidence of CNS relapse implies that CNS-directed therapy should not be omitted in patients with a leukemic presentation [23].
The optimal timing for discontinuing ALK inhibitors remains unclear when they are used as a bridging therapy for HSCT. In some reports, ALK inhibitors were terminated a day before conditioning therapy for HSCT [57,80]. However, a pediatric patient who terminated treatment with an ALK inhibitor a day before conditioning therapy relapsed 40 days after HSCT [63]. Similar to other treatment strategies, re-administration of ALK inhibitors as maintenance therapy following HSCT has been reported [57]. Establishing the optimal timing for discontinuation of ALK inhibitors before HSCT and determining the appropriate maintenance therapy after HSCT is warranted. In addition, involved site radiation therapy may be considered in refractory patients with focal disease [81].
5.2.6. Treatment Strategy for Pediatric Patients with Relapsed or Refractory ALK-Positive ALCL
The standard therapy for pediatric patients with relapsed or refractory ALCL has not yet been firmly established. However, recent studies have shed light on the recommended treatment options. The result of the ALCL-Relapse trial (NCT00317408), the first prospective trial on pediatric patients with relapsed ALCL, can help to determine the best course of treatment. In the ALCL-Relapse trial, patients were classified into four risk groups based on the time of relapse and CD3 expression, and reinduction approaches were selected according to these four risk groups [69]. Patients with progression during frontline therapy were classified as very high risk. Patients with a CD3-positive relapse were classified as high risk. Patients with a CD3-negative relapse within one year after initial diagnosis were classified as intermediate risk. Patients with a CD3-negative relapse later than one year after initial diagnosis were classified as low risk. Patients with very high risk and high risk treated with allogeneic HSCT after reinduction chemotherapy showed good outcomes, with 5-year EFS of 41% and 62%, and 5-year OS of 59% and 73%, respectively, while patients with intermediate risk treated with autologous HSCT after carmustine-etoposide-cytarabine-melphalan showed poor outcome, with 5-year EFS of 30% and 5-year OS of 78%. This result indicates that autologous HSCT is not recommended for patients with early relapse within one year after initial diagnosis. Patients with low risk treated with weekly vinblastine for 24 months showed good prognosis, with 5-year EFS of 81% and 5-year OS of 90% [69]. Ultimately, allogeneic HSCT is recommended as standard consolidation therapy for pediatric patients with progression during frontline therapy or relapse of a CD3-positive ALCL. Furthermore, weekly vinblastine monotherapy for 24 months is recommended for pediatric patients with late relapse, later than 12 months after initial diagnosis, of a CD3-negative ALCL. Although there is no consensus of treatment for pediatric patients with early relapse of CD3-negative ALCL, within 12 months after initial diagnosis, allogeneic HSCT may be suitable for them and should be considered for future testing.
In conditioning regimens followed by allogeneic HSCT, a retrospective study revealed that the RIC regimen resulted in better outcomes than the MAC regime [71]. The JPLSG-ALCL-RIC18 trial is currently ongoing in Japan to evaluate the efficacy of the RIC regimen followed by allogeneic HSCT prospectively.
Although both ALK inhibitors and BV can induce CR in 40–80% of pediatric patients with relapsed or refractory ALCL, it remains unclear whether these drugs can offer cure without additional therapy [11,43,61]. Therefore, ALK inhibitors and BV should be administered as reinduction therapy before consolidation using allogeneic HSCT in all but patients with late relapse of a CD3-negative ALCL [69]. It should be noted that some of these therapies may be off-label for pediatric patients in certain countries.
As a strategy for patients with characteristic risk factors, we suggest treatment in patients with leukemic presentation and CNS involvement.
For patients with leukemic presentation showing chemoresistance, we suggest undergoing allogeneic HSCT with a TBI conditioning regimen, which has been reported to rescue patients [20,21,22].
For patients with CNS involvement, it is recommended to use treatment regimens including HD-MTX and/or HD-AraC as CNS-penetrating chemotherapy [19]. Additionally, cranial radiotherapy (18–24 Gy) has also been reported to be effective for ALCL patients with CNS involvement, especially those with intracerebral mass [19]. Recent studies have shown that alectinib, an ALK inhibitor that penetrates the CNS, is also effective in treating CNS involvement and may even replace cranial radiotherapy [21,82]. The necessity of cranial radiotherapy for ALCL patients with CNS involvement will require further investigation due to neurological sequelae.
6. Conclusions
ALK-positive ALCL typically responds well to conventional chemotherapy, as demonstrated in the ALCL99 trial. However, patients with risk factors, such as the small cell variant or lymphohistiocytic variant, leukemic presentation, MDD-positive status, or CNS involvement, may experience a refractory course, requiring salvage therapies, including weekly vinblastine, BV, ALK inhibitors, and HSCT. Especially for patients with CNS involvement, a CNS-penetrating drug such as alectinib, HD-MTX, or HD-AraC should be considered. In the future, we need a solution for acquired drug resistance in salvage therapies, including BV and ALK inhibitors, and the development of novel treatments for relapsed or refractory ALK-positive ALCL.
Author Contributions
K.N. and Y.I. wrote and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are available in this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Stein, H.; Foss, H.-D. CD30+ Anaplastic Large Cell Lymphoma: A Review of Its Histopathologic, Genetic, and Clinical Features. Blood 2000, 96, 3681–3695. [Google Scholar] [CrossRef] [PubMed]
- Perkins, S.L.; Pickering, D.; Lowe, E.J.; Zwick, D.; Abromowitch, M.; Davenport, G.; Cairo, M.S.; Sanger, W.G. Childhood Anaplastic Large Cell Lymphoma Has a High Incidence of ALK Gene Rearrangement as Determined by Immunohistochemical Staining and Fluorescent in Situ Hybridisation: A Genetic and Pathological Correlation. Br. J. Haematol. 2005, 131, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. (Eds.) WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; IARC: Lyon, France, 2017; ISBN 978-92-832-4494-3. [Google Scholar]
- Falini, B.; Pileri, S.; Zinzani, P.L.; Carbone, A.; Zagonel, V.; Wolf-Peeters, C.; Verhoef, G.; Menestrina, F.; Todeschini, G.; Paulli, M.; et al. ALK+ Lymphoma: Clinico-Pathological Findings and Outcome. Blood 1999, 93, 2697–2706. [Google Scholar] [PubMed]
- Shiota, M.; Nakamura, S.; Ichinohasama, R.; Abe, M.; Akagi, T.; Takeshita, M.; Mori, N.; Fujimoto, J.; Miyauchi, J.; Mikata, A.; et al. Anaplastic Large Cell Lymphomas Expressing the Novel Chimeric Protein P80NPM/ALK. A Distinct Clinicopathologic Entity. Blood 1995, 86, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Tsuyama, N.; Sakamoto, K.; Sakata, S.; Dobashi, A.; Takeuchi, K. Anaplastic Large Cell Lymphoma: Pathology, Genetics, and Clinical Aspects. J. Clin. Exp. Hematop. 2017, 57, 120–142. [Google Scholar] [CrossRef] [PubMed]
- Bohling, S.D.; Jenson, S.D.; Crockett, D.K.; Schumacher, J.A.; Elenitoba-Johnson, K.S.J.; Lim, M.S. Analysis of Gene Expression Profile of TPM3-ALK Positive Anaplastic Large Cell Lymphoma Reveals Overlapping and Unique Patterns with That of NPM-ALK Positive Anaplastic Large Cell Lymphoma. Leuk. Res. 2008, 32, 383–393. [Google Scholar] [CrossRef]
- Mathew, P.; Sanger, W.G.; Weisenburger, D.D.; Valentine, M.; Valentine, V.; Pickering, D.; Higgins, C.; Hess, M.; Cui, X.; Srivastava, D.K.; et al. Detection of the t(2;5)(p23;q35) and NPM-ALK Fusion in Non-Hodgkin’s Lymphoma by Two-Color Fluorescence In Situ Hybridization. Blood 1997, 89, 1678–1685. [Google Scholar] [CrossRef] [PubMed]
- Brugières, L.; Pacquement, H.; Le Deley, M.-C.; Leverger, G.; Lutz, P.; Paillard, C.; Baruchel, A.; Frappaz, D.; Nelken, B.; Lamant, L.; et al. Single-Drug Vinblastine As Salvage Treatment for Refractory or Relapsed Anaplastic Large-Cell Lymphoma: A Report From the French Society of Pediatric Oncology. J. Clin. Oncol. 2009, 27, 5056–5061. [Google Scholar] [CrossRef]
- Lamant, L.; McCarthy, K.; d’Amore, E.; Klapper, W.; Nakagawa, A.; Fraga, M.; Maldyk, J.; Simonitsch-Klupp, I.; Oschlies, I.; Delsol, G.; et al. Prognostic Impact of Morphologic and Phenotypic Features of Childhood ALK-Positive Anaplastic Large-Cell Lymphoma: Results of the ALCL99 Study. J. Clin. Oncol. 2011, 29, 4669–4676. [Google Scholar] [CrossRef]
- Locatelli, F.; Mauz-Koerholz, C.; Neville, K.; Llort, A.; Beishuizen, A.; Daw, S.; Pillon, M.; Aladjidi, N.; Klingebiel, T.; Landman-Parker, J.; et al. Brentuximab Vedotin for Paediatric Relapsed or Refractory Hodgkin’s Lymphoma and Anaplastic Large-Cell Lymphoma: A Multicentre, Open-Label, Phase 1/2 Study. Lancet Haematol. 2018, 5, e450–e461. [Google Scholar] [CrossRef]
- Pro, B.; Advani, R.; Brice, P.; Bartlett, N.L.; Rosenblatt, J.D.; Illidge, T.; Matous, J.; Ramchandren, R.; Fanale, M.; Connors, J.M.; et al. Brentuximab Vedotin (SGN-35) in Patients With Relapsed or Refractory Systemic Anaplastic Large-Cell Lymphoma: Results of a Phase II Study. J. Clin. Oncol. 2012, 30, 2190–2196. [Google Scholar] [CrossRef] [PubMed]
- Pro, B.; Advani, R.; Brice, P.; Bartlett, N.L.; Rosenblatt, J.D.; Illidge, T.; Matous, J.; Ramchandren, R.; Fanale, M.; Connors, J.M.; et al. Five-Year Results of Brentuximab Vedotin in Patients with Relapsed or Refractory Systemic Anaplastic Large Cell Lymphoma. Blood 2017, 130, 2709–2717. [Google Scholar] [CrossRef] [PubMed]
- Woessmann, W.; Zimmermann, M.; Lenhard, M.; Burkhardt, B.; Rossig, C.; Kremens, B.; Lang, P.; Attarbaschi, A.; Mann, G.; Oschlies, I.; et al. Relapsed or Refractory Anaplastic Large-Cell Lymphoma in Children and Adolescents After Berlin-Frankfurt-Muenster (BFM)–Type First-Line Therapy: A BFM-Group Study. J. Clin. Oncol. 2011, 29, 3065–3071. [Google Scholar] [CrossRef] [PubMed]
- Strullu, M.; Thomas, C.; Le Deley, M.-C.; Chevance, A.; Kanold, J.; Bertrand, Y.; Jubert, C.; Dalle, J.-H.; Paillard, C.; Baruchel, A.; et al. Hematopoietic Stem Cell Transplantation in Relapsed ALK+ Anaplastic Large Cell Lymphoma in Children and Adolescents: A Study on Behalf of the SFCE and SFGM-TC. Bone Marrow Transplant. 2015, 50, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Woessmann, W.; Peters, C.; Lenhard, M.; Burkhardt, B.; Sykora, K.-W.; Dilloo, D.; Kremens, B.; Lang, P.; Fuhrer, M.; Kuhne, T.; et al. Allogeneic Haematopoietic Stem Cell Transplantation in Relapsed or Refractory Anaplastic Large Cell Lymphoma of Children and Adolescents—A Berlin-Frankfurt-Munster Group Report. Br. J. Haematol. 2006, 133, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Bischof, D.; Pulford, K.; Mason, D.Y.; Morris, S.W. Role of the Nucleophosmin (NPM) Portion of the Non-Hodgkin’s Lymphoma-Associated NPM-Anaplastic Lymphoma Kinase Fusion Protein in Oncogenesis. Mol. Cell. Biol. 1997, 17, 2312–2325. [Google Scholar] [CrossRef] [PubMed]
- Mussolin, L.; Le Deley, M.-C.; Carraro, E.; Damm-Welk, C.; Attarbaschi, A.; Williams, D.; Burke, A.; Horibe, K.; Nakazawa, A.; Wrobel, G.; et al. Prognostic Factors in Childhood Anaplastic Large Cell Lymphoma: Long Term Results of the International ALCL99 Trial. Cancers 2020, 12, 2747. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.; Mori, T.; Reiter, A.; Woessman, W.; Rosolen, A.; Wrobel, G.; Zsiros, J.; Uyttebroeck, A.; Marky, I.; Le Deley, M.-C.; et al. Central Nervous System Involvement in Anaplastic Large Cell Lymphoma in Childhood: Results from a Multicentre European and Japanese Study: CNS Involvement in Anaplastic Large Cell Lymphoma. Pediatr. Blood Cancer 2013, 60, E118–E121. [Google Scholar] [CrossRef]
- Imamura, R.; Mouri, F.; Nomura, K.; Nakamura, T.; Oku, E.; Morishige, S.; Takata, Y.; Seki, R.; Osaki, K.; Hashiguchi, M.; et al. Successful Treatment of Small Cell Variant Anaplastic Large Cell Lymphoma with Allogeneic Peripheral Blood Stem Cell Transplantation, and Review of the Literature. Int. J. Hematol. 2013, 97, 139–143. [Google Scholar] [CrossRef]
- Noguchi, K.; Ikawa, Y.; Takenaka, M.; Sakai, Y.; Fujiki, T.; Kuroda, R.; Wada, T. Characterisation of Two Tumour Cell Populations in the Small Cell Variant of Anaplastic Lymphoma Kinase-positive Anaplastic Large Cell Lymphoma. Br. J. Haematol. 2022, 196, 241–243. [Google Scholar] [CrossRef]
- Onciu, M.; Behm, F.G.; Raimondi, S.C.; Moore, S.; Harwood, E.L.; Pui, C.-H.; Sandlund, J.T. ALK-Positive Anaplastic Large Cell Lymphoma With Leukemic Peripheral Blood Involvement Is a Clinicopathologic Entity With an Unfavorable Prognosis: Report of Three Cases and Review of the Literature. Am. J. Clin. Pathol. 2003, 120, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, A.; Paillard, C.; Ducassou, S.; Perel, Y.; Plantaz, D.; Strullu, M.; Eischen, A.; Lutz, P.; Lamant, L.; Le Deley, M.-C.; et al. Paediatric Anaplastic Large Cell Lymphoma with Leukaemic Presentation in Children: A Report of Nine French Cases. Br. J. Haematol. 2014, 165, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Damm-Welk, C.; Busch, K.; Burkhardt, B.; Schieferstein, J.; Viehmann, S.; Oschlies, I.; Klapper, W.; Zimmermann, M.; Harbott, J.; Reiter, A.; et al. Prognostic Significance of Circulating Tumor Cells in Bone Marrow or Peripheral Blood as Detected by Qualitative and Quantitative PCR in Pediatric NPM-ALK–Positive Anaplastic Large-Cell Lymphoma. Blood 2007, 110, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Mussolin, L.; Pillon, M.; d’Amore, E.S.; Santoro, N.; Lombardi, A.; Fagioli, F.; Zanesco, L.; Rosolen, A. Prevalence and Clinical Implications of Bone Marrow Involvement in Pediatric Anaplastic Large Cell Lymphoma. Leukemia 2005, 19, 1643–1647. [Google Scholar] [CrossRef] [PubMed]
- Iijima-Yamashita, Y.; Mori, T.; Nakazawa, A.; Fukano, R.; Takimoto, T.; Tsurusawa, M.; Kobayashi, R.; Horibe, K. Prognostic Impact of Minimal Disseminated Disease and Immune Response to NPM-ALK in Japanese Children with ALK-Positive Anaplastic Large Cell Lymphoma. Int. J. Hematol. 2018, 107, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Damm-Welk, C.; Lovisa, F.; Contarini, G.; Lüdersen, J.; Carraro, E.; Knörr, F.; Förster, J.; Zimmermann, M.; Sala, A.; Vinti, L.; et al. Quantification of Minimal Disease by Digital PCR in ALK-Positive Anaplastic Large Cell Lymphoma: A Step towards Risk Stratification in International Trials? Cancers 2022, 14, 1703. [Google Scholar] [CrossRef] [PubMed]
- Damm-Welk, C.; Kutscher, N.; Zimmermann, M.; Attarbaschi, A.; Schieferstein, J.; Knörr, F.; Oschlies, I.; Klapper, W.; Woessmann, W. Quantification of Minimal Disseminated Disease by Quantitative Polymerase Chain Reaction and Digital Polymerase Chain Reaction for NPM-ALK as a Prognostic Factor in Children with Anaplastic Large Cell Lymphoma. Haematologica 2020, 105, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Brugières, L.; Deley, M.C.L.; Pacquement, H.; Meguerian-Bedoyan, Z.; Terrier-Lacombe, M.J.; Robert, A.; Pondarré, C.; Leverger, G.; Devalck, C.; Rodary, C.; et al. CD30+ Anaplastic Large-Cell Lymphoma in Children: Analysis of 82 Patients Enrolled in Two Consecutive Studies of the French Society of Pediatric Oncology. Blood 1998, 92, 3591–3598. [Google Scholar]
- Seidemann, K. Short-Pulse B-Non-Hodgkin Lymphoma-Type Chemotherapy Is Efficacious Treatment for Pediatric Anaplastic Large Cell Lymphoma: A Report of the Berlin-Frankfurt-Munster Group Trial NHL-BFM 90. Blood 2001, 97, 3699–3706. [Google Scholar] [CrossRef]
- Williams, D.M.; Hobson, R.; Imeson, J.; Gerrard, M.; McCarthy, K.; Pinkerton, C.R.; The United Kingdom Children’s Cancer Study Group. Anaplastic Large Cell Lymphoma in Childhood: Analysis of 72 Patients Treated on The United Kingdom Children’s Cancer Study Group Chemotherapy Regimens. Br. J. Haematol. 2002, 117, 812–820. [Google Scholar] [CrossRef]
- Rosolen, A.; Pillon, M.; Garaventa, A.; Burnelli, R.; d’Amore, E.S.; Giuliano, M.; Comis, M.; Cesaro, S.; Tettoni, K.; Luisa Moleti, M.; et al. Anaplastic Large Cell Lymphoma Treated with a Leukemia-like Therapy: Report of the Italian Association of Pediatric Hematology and Oncology (AIEOP) LNH-92 Protocol. Cancer 2005, 104, 2133–2140. [Google Scholar] [CrossRef] [PubMed]
- Laver, J.H.; Kraveka, J.M.; Hutchison, R.E.; Chang, M.; Kepner, J.; Schwenn, M.; Tarbell, N.; Desai, S.; Weitzman, S.; Weinstein, H.J.; et al. Advanced-Stage Large-Cell Lymphoma in Children and Adolescents: Results of a Randomized Trial Incorporating Intermediate-Dose Methotrexate and High-Dose Cytarabine in the Maintenance Phase of the APO Regimen: A Pediatric Oncology Group Phase III Trial. J. Clin. Oncol. 2005, 23, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Lowe, E.J.; Sposto, R.; Perkins, S.L.; Gross, T.G.; Finlay, J.; Zwick, D.; Abromowitch, M. Intensive Chemotherapy for Systemic Anaplastic Large Cell Lymphoma in Children and Adolescents: Final Results of Children’s Cancer Group Study 5941. Pediatr. Blood Cancer 2009, 52, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.; Kraveka, J.M.; Weitzman, S.; Lowe, E.; Smith, L.; Lynch, J.C.; Chang, M.; Kinney, M.C.; Perkins, S.L.; Laver, J.; et al. Advanced Stage Anaplastic Large Cell Lymphoma in Children and Adolescents: Results of ANHL0131, a Randomized Phase III Trial of APO versus a Modified Regimen with Vinblastine: A Report from the Children’s Oncology Group. Pediatr. Blood Cancer 2014, 61, 2236–2242. [Google Scholar] [CrossRef] [PubMed]
- Lowe, E.J.; Reilly, A.F.; Lim, M.S.; Gross, T.G.; Saguilig, L.; Barkauskas, D.A.; Wu, R.; Alexander, S.; Bollard, C.M. Brentuximab Vedotin in Combination with Chemotherapy for Pediatric Patients with ALK+ ALCL: Results of COG Trial ANHL12P1. Blood 2021, 137, 3595–3603. [Google Scholar] [CrossRef] [PubMed]
- Lowe, E.J.; Reilly, A.F.; Lim, M.S.; Gross, T.G.; Saguilig, L.; Barkauskas, D.A.; Wu, R.; Alexander, S.; Bollard, C.M. Crizotinib in Combination With Chemotherapy for Pediatric Patients With ALK+ Anaplastic Large-Cell Lymphoma: The Results of Children’s Oncology Group Trial ANHL12P1. J. Clin. Oncol. 2023, 41, 2043–2053. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, S.; O’Connor, O.A.; Pro, B.; Illidge, T.; Fanale, M.; Advani, R.; Bartlett, N.L.; Christensen, J.H.; Morschhauser, F.; Domingo-Domenech, E.; et al. Brentuximab Vedotin with Chemotherapy for CD30-Positive Peripheral T-Cell Lymphoma (ECHELON-2): A Global, Double-Blind, Randomised, Phase 3 Trial. Lancet 2019, 393, 229–240. [Google Scholar] [CrossRef]
- Gadner, H.; Grois, N.; Arico, M.; Broadbent, V.; Ceci, A.; Jakobson, A.; Komp, D.; Michaelis, J.; Nicholson, S.; Pötschger, U.; et al. A Randomized Trial of Treatment for Multisystem Langerhans’ Cell Histiocytosis. J. Pediatr. 2001, 138, 728–734. [Google Scholar] [CrossRef]
- Gadgeel, S.M.; Gandhi, L.; Riely, G.J.; Chiappori, A.A.; West, H.L.; Azada, M.C.; Morcos, P.N.; Lee, R.-M.; Garcia, L.; Yu, L.; et al. Safety and Activity of Alectinib against Systemic Disease and Brain Metastases in Patients with Crizotinib-Resistant ALK-Rearranged Non-Small-Cell Lung Cancer (AF-002JG): Results from the Dose-Finding Portion of a Phase 1/2 Study. Lancet Oncol. 2014, 15, 1119–1128. [Google Scholar] [CrossRef]
- Saito, S.; Tashiro, H.; Sumiyoshi, R.; Matsuo, T.; Yamamoto, T.; Matsumoto, K.; Ooi, J.; Shirafuji, N. Second Allogeneic Transplantation Using Umbilical Cord Blood for a Patient with Relapsed ALK+ Anaplastic Large Cell Lymphoma after Allogeneic Bone Marrow Transplantation in the Era of ALK Inhibitors: A Case Report. Medicine 2021, 100, e25576. [Google Scholar] [CrossRef]
- Subbiah, V.; Kuravi, S.; Ganguly, S.; Welch, D.R.; Vivian, C.J.; Mushtaq, M.U.; Hegde, A.; Iyer, S.; Behrang, A.; Ali, S.M.; et al. Precision Therapy with Anaplastic Lymphoma Kinase Inhibitor Ceritinib in ALK-Rearranged Anaplastic Large Cell Lymphoma. ESMO Open 2021, 6, 100172. [Google Scholar] [CrossRef] [PubMed]
- Mossé, Y.P.; Voss, S.D.; Lim, M.S.; Rolland, D.; Minard, C.G.; Fox, E.; Adamson, P.; Wilner, K.; Blaney, S.M.; Weigel, B.J. Targeting ALK With Crizotinib in Pediatric Anaplastic Large Cell Lymphoma and Inflammatory Myofibroblastic Tumor: A Children’s Oncology Group Study. J. Clin. Oncol. 2017, 35, 3215–3221. [Google Scholar] [CrossRef] [PubMed]
- Hebart, H.; Lang, P.; Woessmann, W. Nivolumab for Refractory Anaplastic Large Cell Lymphoma: A Case Report. Ann. Intern. Med. 2016, 165, 607–608. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, C.; Abbou, S.; Minard-Colin, V.; Geoerger, B.; Scoazec, J.Y.; Vassal, G.; Jaff, N.; Heuberger, L.; Valteau-Couanet, D.; Brugieres, L. Efficacy of Nivolumab in a Patient with Systemic Refractory ALK+ Anaplastic Large Cell Lymphoma. Pediatr. Blood Cancer 2018, 65, e26902. [Google Scholar] [CrossRef] [PubMed]
- Ruf, S.; Hebart, H.; Hjalgrim, L.L.; Kabickova, E.; Lang, P.; Steinbach, D.; Schwabe, G.C.; Woessmann, W. CNS Progression during Vinblastine or Targeted Therapies for High-risk Relapsed ALK-positive Anaplastic Large Cell Lymphoma: A Case Series. Pediatr. Blood Cancer 2018, 65, e27003. [Google Scholar] [CrossRef] [PubMed]
- Van Der Weyden, C.A.; Pileri, S.A.; Feldman, A.L.; Whisstock, J.; Prince, H.M. Understanding CD30 Biology and Therapeutic Targeting: A Historical Perspective Providing Insight into Future Directions. Blood Cancer J. 2017, 7, e603. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.D.; Evens, A.M.; Fenske, T.S.; Hamlin, P.; Coiffier, B.; Engert, A.; Moskowitz, A.J.; Ghosh, N.; Petrich, A.M.; Lomasney, J.; et al. Pancreatitis in Patients Treated with Brentuximab Vedotin: A Previously Unrecognized Serious Adverse Event. Blood 2014, 123, 2895–2897. [Google Scholar] [CrossRef] [PubMed]
- Carson, K.R.; Newsome, S.D.; Kim, E.J.; Wagner-Johnston, N.D.; Von Geldern, G.; Moskowitz, C.H.; Moskowitz, A.J.; Rook, A.H.; Jalan, P.; Loren, A.W.; et al. Progressive Multifocal Leukoencephalopathy Associated with Brentuximab Vedotin Therapy: A Report of 5 Cases from the Southern Network on Adverse Reactions (SONAR) Project: Brentuximab-Associated PML. Cancer 2014, 120, 2464–2471. [Google Scholar] [CrossRef]
- Chen, R.; Hou, J.; Newman, E.; Kim, Y.; Donohue, C.; Liu, X.; Thomas, S.H.; Forman, S.J.; Kane, S.E. CD30 Downregulation, MMAE Resistance, and MDR1 Upregulation Are All Associated with Resistance to Brentuximab Vedotin. Mol. Cancer Ther. 2015, 14, 1376–1384. [Google Scholar] [CrossRef]
- Al-Rohil, R.N.; Torres-Cabala, C.A.; Patel, A.; Tetzlaff, M.T.; Ivan, D.; Nagarajan, P.; Curry, J.L.; Miranda, R.N.; Duvic, M.; Prieto, V.G.; et al. Loss of CD30 Expression after Treatment with Brentuximab Vedotin in a Patient with Anaplastic Large Cell Lymphoma: A Novel Finding. J. Cutan. Pathol. 2016, 43, 1161–1166. [Google Scholar] [CrossRef]
- Jagadeesh, D.; Horwitz, S.; Bartlett, N.L.; Kim, Y.; Jacobsen, E.; Duvic, M.; Little, M.; Trepicchio, W.; Fenton, K.; Onsum, M.; et al. Response to Brentuximab Vedotin by CD30 Expression in Non-Hodgkin Lymphoma. Oncology 2022, 27, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Kwak, E.L.; Shaw, A.T.; Ou, S.-H.I.; Varella-Garcia, M.; Stubbs, H.; Gandhi, L.; Ratain, M.J.; Wilner, K.; Iafrate, A.J. Anaplastic Lymphoma Kinase Inhibition in Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2010, 363, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Richly, H.; Kim, T.M.; Schuler, M.; Kim, D.-W.; Harrison, S.J.; Shaw, A.T.; Boral, A.L.; Yovine, A.; Solomon, B. Ceritinib in Patients with Advanced Anaplastic Lymphoma Kinase–Rearranged Anaplastic Large-Cell Lymphoma. Blood 2015, 126, 1257–1258. [Google Scholar] [CrossRef]
- Iseki, M.; Kaburaki, T.; Aihara, M.; Sawamura, H. Late-Onset Ocular Toxicity Presenting as Uveitis Caused by Crizotinib. Neuro-Ophthalmol. 2022, 46, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Gambacorti-Passerini, C.; Mussolin, L.; Brugieres, L. Abrupt Relapse of ALK-Positive Lymphoma after Discontinuation of Crizotinib. N. Engl. J. Med. 2016, 374, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Cleary, J.M.; Rodig, S.; Barr, P.M.; Shinagare, A.B.; Clark, J.W.; Shapiro, G.I.; Armand, P. Crizotinib as Salvage and Maintenance With Allogeneic Stem Cell Transplantation for Refractory Anaplastic Large Cell Lymphoma. J. Natl. Compr. Cancer Netw. 2014, 12, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Gambacorti Passerini, C.; Farina, F.; Stasia, A.; Redaelli, S.; Ceccon, M.; Mologni, L.; Messa, C.; Guerra, L.; Giudici, G.; Sala, E.; et al. Crizotinib in Advanced, Chemoresistant Anaplastic Lymphoma Kinase–Positive Lymphoma Patients. JNCI J. Natl. Cancer Inst. 2014, 106, djt378. [Google Scholar] [CrossRef]
- Kay, M.; Dehghanian, F. Exploring the Crizotinib Resistance Mechanism of NSCLC with the L1196M Mutation Using Molecular Dynamics Simulation. J. Mol. Model. 2017, 23, 323. [Google Scholar] [CrossRef]
- Sakamoto, H.; Tsukaguchi, T.; Hiroshima, S.; Kodama, T.; Kobayashi, T.; Fukami, T.A.; Oikawa, N.; Tsukuda, T.; Ishii, N.; Aoki, Y. CH5424802, a Selective ALK Inhibitor Capable of Blocking the Resistant Gatekeeper Mutant. Cancer Cell 2011, 19, 679–690. [Google Scholar] [CrossRef]
- Fukano, R.; Mori, T.; Sekimizu, M.; Choi, I.; Kada, A.; Saito, A.M.; Asada, R.; Takeuchi, K.; Terauchi, T.; Tateishi, U.; et al. Alectinib for Relapsed or Refractory Anaplastic Lymphoma Kinase-positive Anaplastic Large Cell Lymphoma: An Open-label Phase II Trial. Cancer Sci. 2020, 111, 4540–4547. [Google Scholar] [CrossRef]
- Gainor, J.F.; Dardaei, L.; Yoda, S.; Friboulet, L.; Leshchiner, I.; Katayama, R.; Dagogo-Jack, I.; Gadgeel, S.; Schultz, K.; Singh, M.; et al. Molecular Mechanisms of Resistance to First- and Second-Generation ALK Inhibitors in ALK-Rearranged Lung Cancer. Cancer Discov. 2016, 6, 1118–1133. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, K.; Ikawa, Y.; Takenaka, M.; Sakai, Y.; Fujiki, T.; Kuroda, R.; Ikeda, H.; Abe, T.; Sakai, S.; Wada, T. Acquired L1196M ALK Mutation in Anaplastic Lymphoma Kinase-positive Anaplastic Large Cell Lymphoma during Alectinib Administration. eJHaem 2023, 4, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Li, J.; Gu, W.-Y.; Jin, L.; Duan, Y.-L.; Huang, S.; Zhang, M.; Wang, X.-S.; Liu, Y.; Zhou, C.-J.; et al. Central Nervous System Relapse in a Pediatric Anaplastic Large Cell Lymphoma Patient with CLTC/ALK Translocation Treated with Alectinib: A Case Report. World J. Clin. Cases 2020, 8, 1685–1692. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Kim, D.-W.; Mehra, R.; Tan, D.S.W.; Felip, E.; Chow, L.Q.M.; Camidge, D.R.; Vansteenkiste, J.; Sharma, S.; De Pas, T.; et al. Ceritinib in ALK -Rearranged Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 370, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Brugières, L.; Quartier, P.; Le Deley, M.C.; Pacquement, H.; Perel, Y.; Bergeron, C.; Schmitt, C.; Landmann, J.; Patte, C.; Terrier-Lacombe, M.J.; et al. Relapses of Childhood Anaplastic Large-Cell Lymphoma: Treatment Results in a Series of 41 Children—A Report from the French Society of Pediatric Oncology. Ann. Oncol. 2000, 11, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Fukano, R.; Mori, T.; Kobayashi, R.; Mitsui, T.; Fujita, N.; Iwasaki, F.; Suzumiya, J.; Chin, M.; Goto, H.; Takahashi, Y.; et al. Haematopoietic Stem Cell Transplantation for Relapsed or Refractory Anaplastic Large Cell Lymphoma: A Study of Children and Adolescents in Japan. Br. J. Haematol. 2015, 168, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Gross, T.G.; Hale, G.A.; He, W.; Camitta, B.M.; Sanders, J.E.; Cairo, M.S.; Hayashi, R.J.; Termuhlen, A.M.; Zhang, M.-J.; Davies, S.M.; et al. Hematopoietic Stem Cell Transplantation for Refractory or Recurrent Non-Hodgkin Lymphoma in Children and Adolescents. Biol. Blood Marrow Transplant. 2010, 16, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Knörr, F.; Brugières, L.; Pillon, M.; Zimmermann, M.; Ruf, S.; Attarbaschi, A.; Mellgren, K.; Burke, G.A.A.; Uyttebroeck, A.; Wróbel, G.; et al. Stem Cell Transplantation and Vinblastine Monotherapy for Relapsed Pediatric Anaplastic Large Cell Lymphoma: Results of the International, Prospective ALCL-Relapse Trial. J. Clin. Oncol. 2020, 38, 3999–4009. [Google Scholar] [CrossRef]
- Fossard, G.; Broussais, F.; Coelho, I.; Bailly, S.; Nicolas-Virelizier, E.; Toussaint, E.; Lancesseur, C.; Le Bras, F.; Willems, E.; Tchernonog, E.; et al. Role of Up-Front Autologous Stem-Cell Transplantation in Peripheral T-Cell Lymphoma for Patients in Response after Induction: An Analysis of Patients from LYSA Centers. Ann. Oncol. 2018, 29, 715–723. [Google Scholar] [CrossRef]
- Fukano, R.; Mori, T.; Fujita, N.; Kobayashi, R.; Mitsui, T.; Kato, K.; Suzuki, R.; Suzumiya, J.; Fukuda, T.; Shindo, M.; et al. Successful Outcome with Reduced-Intensity Condition Regimen Followed by Allogeneic Hematopoietic Stem Cell Transplantation for Relapsed or Refractory Anaplastic Large-Cell Lymphoma. Int. J. Hematol. 2019, 110, 723–728. [Google Scholar] [CrossRef]
- Bayle, C.; Charpentier, A.; Duchayne, E.; Manel, A.-M.; Pages, M.-P.; Robert, A.; Lamant, L.; Dastugue, N.; Bertrand, Y.; Dijoud, F.; et al. Leukaemic Presentation of Small Cell Variant Anaplastic Large Cell Lymphoma: Report of Four Cases: Leukaemic Form of Anaplastic Large Cell Lymphoma. Br. J. Haematol. 1999, 104, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Villamor, N.; Rozman, M.; Esteve, J.; Aymerich, M.; Colomer, D.; Aguilar, J.L.; Campo, E.; Montserrat, E. Anaplastic Large-Cell Lymphoma with Rapid Evolution to Leukemic Phase. Ann. Hematol. 1999, 78, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Meech, S.J.; McGavran, L.; Odom, L.F.; Liang, X.; Meltesen, L.; Gump, J.; Wei, Q.; Carlsen, S.; Hunger, S.P. Unusual Childhood Extramedullary Hematologic Malignancy with Natural Killer Cell Properties That Contains Tropomyosin 4–Anaplastic Lymphoma Kinase Gene Fusion. Blood 2001, 98, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Awaya, N.; Mori, S.; Takeuchi, H.; Mori, S.; Sugano, Y.; Kamata, T.; Takeuchi, T.; Abe, T. CD30 and the NPM-ALK Fusion Protein (P80) Are Differentially Expressed between Peripheral Blood and Bone Marrow in Primary Small Cell Variant of Anaplastic Large Cell Lymphoma. Am. J. Hematol. 2002, 69, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.-Y.; Cho, H.-J.; Suk, J.-H.; Tak, E.-Y.; Ko, Y.H.; Kim, K.; Kim, S.-H. A Novel Complex t(2;5;13)(P23;Q35;Q14) in Small Cell Variant Type Anaplastic Large Cell Lymphoma with Peripheral Involvement. Cancer Genet. Cytogenet. 2004, 154, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Grewal, J.S.; Smith, L.B.; Winegarden, J.D.; Krauss, J.C.; Tworek, J.A.; Schnitzer, B. Highly Aggressive ALK-Positive Anaplastic Large Cell Lymphoma with a Leukemic Phase and Multi-Organ Involvement: A Report of Three Cases and a Review of the Literature. Ann. Hematol. 2007, 86, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, D.; Nagatoshi, Y.; Nagayama, J.; Inagaki, J.; Itonoaga, N.; Takeshita, M.; Okamura, J. Anaplastic Large Cell Lymphoma in Leukemic Presentation: A Case Report and a Review of the Literature. J. Pediatr. Hematol./Oncol. 2008, 30, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.T.; Condron, M.R.; Nguyen, N.D.; De, J.; Medeiros, L.J.; Padula, A. Anaplastic Large Cell Lymphoma in Leukemic Phase: Extraordinarily High White Blood Cell Count. Pathol. Int. 2009, 59, 345–353. [Google Scholar] [CrossRef]
- Nakai, R.; Fukuhara, S.; Maeshima, A.M.; Kim, S.; Ito, Y.; Hatta, S.; Suzuki, T.; Yuda, S.; Makita, S.; Munakata, W.; et al. Alectinib, an Anaplastic Lymphoma Kinase (ALK) Inhibitor, as a Bridge to Allogeneic Stem Cell Transplantation in a Patient with ALK-positive Anaplastic Large-cell Lymphoma Refractory to Chemotherapy and Brentuximab Vedotin. Clin. Case Rep. 2019, 7, 2500–2504. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). In Non-Hodgkin’s Lymphomas; NCCN: Plymouth Meeting, PA, USA, 2015.
- Tanaka, M.; Miura, H.; Ishimaru, S.; Furukawa, G.; Kawamura, Y.; Kozawa, K.; Yamada, S.; Ito, F.; Kudo, K.; Yoshikawa, T. Future Perspective for ALK-Positive Anaplastic Large Cell Lymphoma with Initial Central Nervous System (CNS) Involvement: Could Next-Generation ALK Inhibitors Replace Brain Radiotherapy for the Prevention of Further CNS Relapse? Pediatr. Rep. 2023, 15, 333–340. [Google Scholar] [CrossRef]
Figure 1.
May-Giemsa-stained blood smears at the onset. Numerous small-sized lymphocytes with lobulated nuclei called “flower-cell” or “cerebriform cell” (arrow), and a few large-sized lymphocytes with basophilic and vacuolated cytoplasm (arrowhead) are displayed.
Figure 1.
May-Giemsa-stained blood smears at the onset. Numerous small-sized lymphocytes with lobulated nuclei called “flower-cell” or “cerebriform cell” (arrow), and a few large-sized lymphocytes with basophilic and vacuolated cytoplasm (arrowhead) are displayed.

{kind=link}
Table 1.
Clinical trials for pediatric patients with ALK-positive ALCL.
| Protocol | Study Group | Study Period | Treatment Strategy | Number of Patients | EFS (Year) | OS (Year) | Reference |
|---|---|---|---|---|---|---|---|
| HM89/91 | SFOP | 1988–1997 | COPADM (CY, DXR, PSL, MTX, VCR) × 2 with maintenance treatment | 82 | 66% (3) | 83% (3) | Blood. 1998 [29] |
| NHL-BFM90 | BFM | 1990–1995 | K1/2 arm: 3/6 courses (MTX, DEX, oxazaphorins, ETP, AraC, DXR, IT) K3 arm: 6 intensified courses including HD-MTX/HD-AraC/HD-ETP | 89 | 76% (5) | ND | Blood. 2001 [30] |
| NHL 9000/9602 | UKCCSG | 1990–1998 | NHL 9000 including VCR, DXR, PSL, MTX, AraC, 6-TG NHL 9602 including COPADM × 3 with CYM (CY, MTX) × 2 intensified courses including HD-MTX/HD-AraC for CNS-positive disease | 72 | 59% (5) | 65% (5) | Br. J. Haematol. 2002 [31] |
| LNH92 | AIEOP | 1993–1997 | Induction therapy (CY, VCR, DEX, DNR, IT), consolidation therapy (6-TG, AraC, ASP, HD-MTX, IT) with maintenance treatment | 34 | 65% (5) | 85% (5) | Cancer. 2005 [32] |
| POG9315 | POG | 1994–2000 | APO (DXR, VCR, PSL, 6MP, MTX) with randomization of ID-MTX and HD-AraC | 86 | 72% (4) | 88% (4) | J. Clin. Oncol. 2005 [33] |
| CCG5941 | CCG | 1996–2001 | Induction therapy (VCR, PSL, CY, DNR, ASP, IT, G-CSF), consolidation therapy (VCR, PSL, ETP, 6-TG, AraC, ASP, MTX, IT, G-CSF) with maintenance treatment | 86 | 68% (5) | 80% (5) | Pediatr. Blood Cancer. 2009 [34] |
| ALCL99 | EICNHL | 1999–2006 | DEX, CY, IT, IFO, AraC, ETP with randomization of VBL | 352 | 72% (10) | 92% (10) | Cancers (Basel). 2020 [18] |
| ANHL0131 | COG | 2004–2008 | APO (DXR, VCR, PSL, 6MP, MTX) with randomization of VBL | 125 | Non-VBL arm: 74% (3) VBL arm: 79% (3) | Non-VBL arm: 84% (3) VBL arm: 86% (3) | Pediatr. Blood Cancer. 2014 [35] |
ALK, anaplastic lymphoma kinase; ALCL, anaplastic large cell lymphoma; EFS, event-free survival rates; OS, overall survival; SFOP, French Society of Pediatric Oncology; BFM, Berlin-Frankfurt-Munster; UKCCSG, United Kingdom Children’s Cancer Study Group; AIEOP, Italian Association of Pediatric Hematology and Oncology; POG, Pediatric Oncology Group; CCG, Children’s Cancer Study Group; CY, cyclophosphamide; DXR, doxorubicin; PSL, prednisolone; MTX, methotrexate; VCR, vincristine; DEX, dexamethasone; ETP, etoposide; AraC, cytarabine; IT, intrathecal therapy; HD, high-dose; 6-TG, 6-thioguanine; DNR, daunorubicin; ASP, asparaginase; 6-MP, 6-mercaptopurine; ID, intermediate-dose; IFO, ifosphamide; VBL, vinblastine; ND, no data; CNS, central nervous system.
Table 2.
Characteristics of salvage therapies for ALK-positive ALCL.
| Number of Patients | CR Rate | EFS (Year) | OS (Year) | CNS Penetrability | Adverse Effect | Reference | ||
|---|---|---|---|---|---|---|---|---|
| Weekly vinblastine | 31 | 83% | 65% (5) | 30% (5) | Low | Mild leukopenia (34%) | J. Pediatr. 2001 [39], J. Clin. Oncol. 2009 [9] | |
| Brentuximab vedotin | 17 | 41% (ORR: 53%) | ND | ND | Low | Fever (44%), nausea (36%), peripheral neuropathy (33%) | Lancet Haematol. 2018 [11] | |
| ALK inhibitor | Crizotinib | 26 | 81% (ORR: 88%) | ND | ND | Low | Visual disturbance (40–60%), gastrointestinal symptoms (29–54%) | J. Clin. Oncol. 2017 [40] |
| Alectinib | 10 | 60% (ORR: 80%) | 70% (1) | 70% (1) | High | Gastrointestinal symptoms (<15%) | Cancer Sci. 2020 [41] | |
| Ceritinib | 3 | 2 out of 3 cases: CR 1 out of 3 cases: PR | ND | ND | ND | Gastrointestinal symptoms (32–82%) | Blood. 2015 [42], ESMO Open. 2021 [43] | |
| Nivolumab | 2 case reports | 2 out of 2 cases: CR | ND | ND | ND | ND | Ann. Intern. Med. 2016 [44], Pediatr. Blood Cancer. 2018 [45] | |
ALK, anaplastic lymphoma kinase; ALCL, anaplastic large cell lymphoma; CR, complete response; EFS, event-free survival rates; OS, overall survival; ORR, overall response ratio; PR, partial response; HSCT, hematopoietic stem cell transplantation; ND, no data; CNS, central nervous system.
Table 3.
Survival cases with ALK-positive ALCL with leukemic presentation.
| Case | Age (Year)/Sex | CNS Lesion | Extranodal Lesion | 1st Line | 2nd Line | 3rd Line | HSCT | Status at HSCT | Conditioning Regimen | Donor Source | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1/M | ND | Li, Sp, PE | CsA, mPSL, CY, AraC, DXR, VP, MTX → CR | - | - | Blood. 2001 [74] | ||||
| 2 | 12/F | - | Li, Sp | ALCL99+VBL → CR | - | - | Br. J. Haematol. 2014 [23] | ||||
| 3 | 10/F | - | Li, Sp, Sk, Lu | ALCL99 → PR | DEX, VDS, AraC, VP → CR | + | 1st CR | ND | ND | Br. J. Haematol. 2014 [23] | |
| 4 | 11/M | - | Li, Sp, Sk, Lu, A | ALCL99 → CR → relapse | VBL+glucocorticoid → 2nd CR | + | 2nd CR | ND | ND | Br. J. Haematol. 2014 [23] | |
| 5 | 18/F | - | Li, Sp, Sk, Lu | CHOP → relapse | chemotherapy | + | 2nd CR | ND | Allo | Br. J. Haematol. 1999 [72] | |
| 6 | 6/F | - | K, Lu | DXR, PSL, VCR → PR | MTX, IFO, VP, DEX → PR | AraC, CCNU, VBL, BLM → PR | + | PR | TBI/TEPA/VP/CY/alemtuzumab | Allo | Am. J. Clin. Pathol. 2003 [22] |
| 7 | 40/M | + | Li, Sp | chemotherapy for ALL → PR, CNS+ | IT, MTX, AraC → CNS- | + | PR | TBI/VP/CY | Allo | Int. Hematol. 2013 [20] | |
| 8 | 10/M | - | Li, Sp, Lu, Sk, PE | ALCL99 → PR, CNS+ | alectinib → CR | + | 1st CR | TBI/VP/CY | Allo | Br. J. Haematol. 2022 [21] |
ALK, anaplastic lymphoma kinase; ALCL, anaplastic large cell lymphoma; CNS, central nervous system; HSCT, hematopoietic stem cell transplantation; ND, no data; Li, liver; Sp, spleen; Lu, lung; Sk, skin; K, kidney; PE, pleural effusion; A, ascites; CsA, cyclosporin A; mPSL, methylprednisolone; CY, cyclophosphamide; AraC, cytarabine; DXR, doxorubicin; VP, etoposide; MTX, methotrexate; ALCL99, ALCL99 protocol regimen; VBL, vinblastine; CHOP, CHOP regimen; VCR, vincristine; ALL, acute lymphoblastic leukemia; CR, complete response; PR, partial response; CNS+, CNS lesion-positive; CNS-, CNS lesion-negative; DEX, dexamethasone; VDS, vindesine; IFO, ifosphamide; IT, intrathecal injection; CCNU, lomustine; BLM, bleomycin; TBI, total-body irradiation; TEPA, thiotepa; allo, allogeneic.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Noguchi, K.; Ikawa, Y. Strategy for Pediatric Patients with Relapsed or Refractory Anaplastic Lymphoma Kinase-Positive Anaplastic Large Cell Lymphoma: A Review. Cancers 2023, 15, 5733. https://doi.org/10.3390/cancers15245733
AMA Style
Noguchi K, Ikawa Y. Strategy for Pediatric Patients with Relapsed or Refractory Anaplastic Lymphoma Kinase-Positive Anaplastic Large Cell Lymphoma: A Review. Cancers. 2023; 15(24):5733. https://doi.org/10.3390/cancers15245733
Chicago/Turabian StyleNoguchi, Kazuhiro, and Yasuhiro Ikawa. 2023. "Strategy for Pediatric Patients with Relapsed or Refractory Anaplastic Lymphoma Kinase-Positive Anaplastic Large Cell Lymphoma: A Review" Cancers 15, no. 24: 5733. https://doi.org/10.3390/cancers15245733
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.