A Review of Biomarkers and Their Clinical Impact in Resected Early-Stage Non-Small-Cell Lung Cancer
by
 ,
,
Weibo Cao
1,2,† ,
,
Quanying Tang
1,2,†,
Jingtong Zeng
1,2,
Xin Jin
1,2,
Lingling Zu
1,2 and
Song Xu
1,2,* 1
Department of Lung Cancer Surgery, Tianjin Medical University General Hospital, Tianjin 300052, China
2
Tianjin Key Laboratory of Lung Cancer Metastasis and Tumor Microenvironment, Lung Cancer Institute, Tianjin Medical University General Hospital, Tianjin 300052, China
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Cancers 2023, 15(18), 4561; https://doi.org/10.3390/cancers15184561
Submission received: 23 July 2023
/
Revised: 28 August 2023
/
Accepted: 8 September 2023
/
Published: 14 September 2023
(This article belongs to the Special Issue Advances in Precision Medicine: Targeting Known and Emerging Oncogenic Targets in Lung Cancer)
Abstract
:Simple Summary
Non-small-cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancers, and the postoperative survival of early-stage NSCLC patients remains unsatisfactory. Over the last several decades, mutant genes, immunological checkpoints, and blood-based biomarkers have been developed and tested to have diverse effects on the survival of early-stage NSCLC. Herein, we reviewed the pertinent literature to determine the prognostic effect of related indicators on early-stage NSCLC, and we will accurately predict patient outcomes and guide patient treatment in the future.
Abstract
The postoperative survival of early-stage non-small-cell lung cancer (NSCLC) patients remains unsatisfactory. In this review, we examined the relevant literature to ascertain the prognostic effect of related indicators on early-stage NSCLC. The prognostic effects of the epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK), mesenchymal–epithelial transition (MET), C-ros oncogene 1 (ROS1), or tumour protein p53 (TP53) alterations in resected NSCLC remains debatable. Kirsten rat sarcoma viral oncogene homologue (KRAS) alterations indicate unfavourable outcomes in early-stage NSCLC. Meanwhile, adjuvant or neoadjuvant EGFR-targeted agents can substantially improve prognosis in early-stage NSCLC with EGFR alterations. Based on the summary of current studies, resected NSCLC patients with overexpression of programmed death-ligand 1 (PD-L1) had worsening survival. Conversely, PD-L1 or PD-1 inhibitors can substantially improve patient survival. Considering blood biomarkers, perioperative peripheral venous circulating tumour cells (CTCs) and pulmonary venous CTCs predicted unfavourable prognoses and led to distant metastases. Similarly, patients with detectable perioperative circulating tumour DNA (ctDNA) also had reduced survival. Moreover, patients with perioperatively elevated carcinoembryonic antigen (CEA) in the circulation predicted significantly worse survival outcomes. In the future, we will incorporate mutated genes, immune checkpoints, and blood-based biomarkers by applying artificial intelligence (AI) to construct prognostic models that predict patient survival accurately and guide individualised treatment.
1. Introduction
Lung cancer mortality is predominant among cancer patients worldwide [1], and approximately 85% of lung cancers are non-small-cell lung cancer (NSCLC) [2]. The comprehensive treatment paradigm for early-stage NSCLC has changed rapidly over the past 20 years, and radical resection of cancerous lesions remains the preferred treatment option for early-stage NSCLC [3].
Nevertheless, postoperative survival of patients remains unsatisfactory, with five-year survival rates for stage I to III lung cancer ranging from 90% to 12% [4]. With the improvement in molecular testing, more mutant genes have been detected in NSCLC, such as the epidermal growth factor receptor (EGFR) and Kirsten rat sarcoma viral oncogene homologue (KRAS) genes [5,6]. Immune checkpoint inhibitors (ICIs) target multiple immune checkpoints, including the programmed death ligand 1 (PD-L1) and the programmed cell death protein-1 (PD-1) [7,8]. Patients with lung cancer recurrences often indicate tumour micro-metastases indexes in the blood circulation, which can often reflect the molecular characteristics of micro-metastases.
In this review, we included relevant literature to discuss further the prognostic value and clinical significance of related biomarkers in early-stage NSCLC patients.
2. Methods
The literature from PubMed and published in English was reviewed. We conducted the literature search using a combination of the following keywords: “Carcinoma, Non-Small-Cell Lung” OR “Adenocarcinoma of Lung” OR “Squamous cell lung cancer” AND “Surgical Procedures, Operative” AND “Mutation” OR “Programmed cell death-1” OR “Programmed cell death-ligand 1” OR “Tumor mutational burden” OR “Neoplastic Cells, Circulating” OR “Biomarkers”. Detailed retrieval strategies are listed in Supplementary Text S1. The deadline for the literature search was 1 February 2023. The included literature was selected from studies related to the theme of the review.
3. Results
3.1. Genetic Alterations
With an improvement in molecular detection techniques, increasing genetic alterations have been detected in NSCLC. Therefore, we summarised the effects of genetic modifications on the prognoses of resectable early-stage NSCLC (Table 1).
3.1.1. EGFR Alterations
The EGFR belongs to the tyrosine kinase receptors (TKRs) superfamily, which also includes ErbB2/human epidermal growth factor receptor 2 (HER2), ErbB3/HER3, and ErbB4/HER4 [52]. EGFR binds to its ligand and activates downstream signalling pathways involved in cell proliferation, migration, and survival. It has been shown that EGFR is critical for the biology of epithelial-derived malignancies, and therefore, potential novel inhibitors targeting EGFR deserve extensive exploration [53,54].
EGFR genetic alteration rates are standard in all pathological types of NSCLC, particularly in LUAD [55,56]. Meanwhile, many EGFR alteration subtypes and molecular changes have been found in early-stage NSCLC. Regarding stage II–III nonsquamous NSCLC patients receiving surgery and platinum-based adjuvant chemotherapy, it was found that EGFR alteration was an independent predictor for shorter relapse-free survival (RFS) and tumour recurrence [9]. For stage I–III resected LUAD, the risk of brain and bone metastases was higher in patients with EGFR alterations. However, in all patients included, the RFS of patients with EGFR alterations was not different from those with wild-type EGFR. Alterations in EGFR only had a statistically shorter RFS than the wild-type group in patients with solid nodules, stage II–III, or acinar/papillary/invasive mucinous predominantly LUAD [10]. Even in patients with pN0-1M0 LUAD, favourable EGFR alterations were indicated as risk factors for postoperative recurrence. The recurrence risk stratification was dependent upon the pathological stage and degree of histological malignancy [11]. When assessing the molecular changes in EGFR, its amplification was associated with poorer RFS in early-stage EGFR-mutant LUAD [12], and a higher level of EGFR amplification correlated with poorer survival in surgically treated NSCLC patients [13].
However, Isaka et al. found that EGFR alterations were significantly associated with favourable RFS in patients with recurrent LUAD after surgical resection, and a longer median RFS was observed in patients with EGFR alterations (20.2 months) compared to wild-type patients (13.3 months) [14]. It has been confirmed that patients with mutant EGFRs had a greater chance of survival than those with wild-type EGFRs for resectable NSCLC [15,16]. Additionally, the prognostic effect of alterations in EGFR for early-stage NSCLC differed even for the pathological stage. EGFR alterations did not impact the survival of stage IA NSCLC but were favourable prognostic factors for better disease-specific survival (DSS) and OS in patients with stage IB NSCLC [17]. Based on the original studies above, EGFR alterations’ prognosis in early-stage resected NSCLC remains controversial.
When alterations in the EGFR subtypes were studied, it was found that EGFR alterations in exons 18–19 (five-year survival: 100%) represented better survival outcomes in resected NSCLC than those without such alterations (five-year survival: 47%) [18]. The prognostic effect of exon 21 L858R alterations and EGFR exon 19 deletions on resected NSCLC patients differed by stage. Exons 19 and 21 did not significantly differ in median OS for location I patients. However, exon 19 deletions had an exceptionally favourable OS compared to exon 21 L858R alterations in stage II and III patients [19]. Furthermore, for pN1-N2 LUAD, patients with exon 19 deletions had longer disease-free survival (DFS) and OS than those with exon 21 L858R alterations [20]. However, a study of resectable LUAD showed that exon 19 deletions were more likely to have an extrathoracic recurrence and significantly shortened RFS when compared to exon 21 L858R alterations, suggesting that exon 19 deletions were poor prognostic factors [21]. EGFR T790 alterations tended to be independent of shorter RFS and OS in resected NSCLC [22]. Phosphorylated EGFR (pEGFR) could independently predict shorter survival in stage I NSCLC patients undergoing surgery [23].
Since EGFR alterations are common in NSCLC patients, targeted agents for EGFR alterations have also been extensively studied. The ADAURA trial found that patients with stage IB–IIIA, EGFR-mutated NSCLC (n = 682) who received postoperative adjuvant osimertinib had better DFS compared to placebo (four-year DFS: osimertinib 73% vs. placebo 38%) [57]. The updated data from the ADAURA trial revealed that patients in the osimertinib group had more prolonged OS than the placebo group (five-year OS: osimertinib 88% vs. placebo 78%) [58]. Hence, adjuvant osimertinib provided a survival benefit for IB–IIIA NSCLC with EGFR alterations. Another clinical trial (ADJUVANT) reported that for NSCLC with stage II–IIIA EGFR alterations, adjuvant gefitinib (28.7 months) resulted in significantly longer median DFS than vinorelbine plus cisplatin (18 months) [59]. In the study (Emerging-CTONG 1103) involving IIIA (N2) resectable NSCLC patients with EGFR alterations, investigators examined the efficacy of neoadjuvant/adjuvant erlotinib and gemcitabine plus cisplatin (GC chemotherapy). Although neoadjuvant erlotinib (54.1%) had a higher objective response rate (ORR) than GC chemotherapy (54.1%), the difference was not statistically significant (p = 0.092). The median progression-free survival (PFS) with erlotinib (21.5 months) was substantially longer than that with GC chemotherapy (11.4 months) [60]. Therefore, in early-stage NSCLC patients with EGFR alterations, adjuvant or neoadjuvant EGFR-TKIs can significantly prolong patient survival compared to placebo or platinum-based chemotherapy.
3.1.2. KRAS Alterations
KRAS, belonging to the RAS gene family, is activated by binding to GTP and triggers many cellular activation processes, including transcription, translation, cell survival, and apoptosis [61].
KRAS G12C (KRASG12C) was significantly associated with a worsening DFS in stage I–III resectable LUAD. However, patients with the KRAS-mutant (KRASMUT) and the wild-type KRAS (KRASWT) did not differ in DFS [24]. Another study also confirmed that NSCLC patients (Stage I–III) with KRASMUT had similar OS to those with KRASWT [25]. KRASMUT, as an independent prognostic factor, was correlated with inferior DFS and OS compared to KRASWT in stage I LUAD [26]. Meanwhile, KRAS alterations were associated with worsening DFS, OS, and a higher recurrence risk in early-stage LUAD, especially in tumours with predominantly solid components [27,28]. Regarding early-stage resected NSCLC, KRAS alterations were prognostic determinants for worsening survival [16]. Conversely, Ayyoub et al. showed that KRAS alterations were associated with superior DSS in resected NSCLC [29].
Subgroup analyses of a meta-analysis involving NSCLC patients (n = 6939) revealed that KRAS alterations predicted an unfavourable OS for stage I–IIIA NSCLC [62]. In general, KRAS genetic alterations predicted adverse outcomes in resected NSCLC.
3.1.3. ALK Alterations
Anaplastic lymphoma kinase (ALK), a transmembrane receptor tyrosine kinase (RTK), has a highly homologous sequence to insulin receptor kinases. Oligomerase is the primary driver of ALK’s downstream signalling, and fusion proteins such as echinoderm microtubule-associated protein-like 4 (EML4)-ALK and nucleophosmin (NPM)-ALK are critical components of the downstream signalling pathway’s activation [63,64].
For patients with stage I LUAD undergoing surgery, ALK rearrangement exhibited a significantly worsening RFS but did not affect OS [30]. Furthermore, patients with ALK alterations experienced worse RFS than those with EGFR alterations in early-stage resected NSCLC [31]. However, a study published by Matsuura et al. confirmed that ALK rearrangement was a more favourable biomarker for cancer-specific survival (CSS) and OS than non-ALK rearrangement in resected NSCLC [32]. This may be attributed to the effect of ALK-targeted inhibitors. A different study demonstrated that EML4-ALK mutant 3 had a substantially shorter DFS in patients with resected NSCLC [33]. However, several studies concluded that ALK rearrangement had no predictive value in surgically resected NSCLC [34,35]. In summary, there were no conclusive conclusions about the prognostic effect of ALK rearrangement on early-stage NSCLC.
3.1.4. MET Alterations
The mesenchymal–epithelial transition (MET) gene is an oncogene that encodes RTK, which binds to the hepatocyte growth factor (HGF) and promotes the aggressive nature of the tumours by inducing angiogenesis [65]. C-MET had diverse prognostic outcomes on resectable LUAD (Stage IB–IIIA) depending on EGFR alteration status. C-MET significantly correlated with reduced RFS and OS in EGFR-negative groups but not EGFR-positive groups [36]. Resectable NSCLC patients with MET-increased gene copy number had a higher risk of death and shorter survival [37]. MET amplification and overexpression have been found in NSCLC, but they did not affect survival in stage I–III NSCLC [38]. For patients with resected stage I–IIIA LUAD, there was no difference in survival between MET exon 14 (METex14) skipping and the other significant genetic alterations [39].
3.1.5. ROS1 Alterations
The C-ros oncogene 1 (ROS1) encodes RTK, but its corresponding ligand is unrecognised, and therefore, our understanding of the function of ROS1 is limited [66]. Kim et al. indicated that the ROS1 fusion gene was an independent biomarker for disease recurrence in resectable stage I–II LUAD [40]. However, Chen et al. indicated no difference in survival (p = 0.555) between the ROS1 fusion-positivity and fusion-negativity groups in early-stage LUAD, but this might be attributed to the limited number of ROS1 fusion individuals [41].
3.1.6. TP53 Alterations
Tumour protein p53 (TP53) is a tumour antioncogene, which encodes the p53 tumour suppressor protein and functions to protect cellular DNA, as well as affecting cell metabolism, differentiation, and apoptosis [67]. The TP53 alteration was an independent predictor for poor RFS in resected EGFR-mutant LUAD [12]. Compared with a single EGFR alteration, a single TP53 alteration as a negative biomarker had a shorter RFS in stage I–II LUAD [40]. Jao et al. concluded that TP53 also leads to worse DFS and OS in resectable NSCLC [42]. A different study confirmed that TP53 did not correlate with DFS in stage I LUAD and LUSC but only conferred reduced OS in stage I LUAD, not in LUSC [43].
The study by Zhou et al. further demonstrated that p53 pathway alterations correlated with poor DFS in surgically treated LUAD [44]. Regarding stage I–III NSCLC patients, p53 alterations (Exons 5-8) had an adverse prognostic effect on survival [45,46]. Hence, the prognosis of TP53 alterations in resected NSCLC remains debatable.
3.1.7. Other Genetic Alterations
Rearranged during transfection (RET) as an oncogene expresses cellular surface receptors, and its ligand is a neurotrophic factor derived from glial cell lines. The RET gene is involved in kidney and nervous system development and even the formation of tumours [68]. RET fusion genes, as prognostic biomarkers, were correlated with tumour recurrence in early-stage resected LUAD [40]. The V-RAF murine sarcoma viral oncogene homolog B1 (BRAF) gene encodes the BRAF protein. It is involved in the mitogen-activated protein kinase (MAPK) pathway, which regulates cell proliferation, differentiation, and apoptosis [69]. BRAF alterations were independent biomarkers for improved DFS and OS in resectable LUAD [28].
For patients with resected LUSC, a significant association was found between PIK3CA alterations and longer OS and a longer time to recurrence (TTR) [47]. However, Song et al. concluded that PIK3CA alterations were correlated with worsening OS in stage I–IIIA resected LUAD [48]. Another study also demonstrated that PIK3CA correlated with poor survival in stage I NSCLC [49]. Furthermore, thyroid transcription factor-1 (TTF-1) gene amplification was a prognostic predictor for worsening DFS and OS in resected LUAD [50]. When considering resected EGFR-mutant LUAD, patients with protein kinase D (PKD)/TP53 co-alterations had shorter DFS than those without co-alterations [51].
3.2. Immune-Related Indicators
Tumour-induced immunosuppression encourages tumours to escape immune surveillance, and immunotherapy can activate the immune system and induce a sustained anti-tumour immune response. Several essential immune checkpoints, including PD-L1, PD-1, programmed death-ligand 2 (PD-L2), and T-cell immunoglobulin and mucin-domain-containing-3 (TIM-3), were found to be targets of ICIs. Herein, we included immune-related indicators to explore their prognostic relevance in resected NSCLC (Table 2).
3.2.1. PD-L1
Patients with PD-L1 overexpression had significantly inferior survival in stage I–III resectable LUAD, especially in acinar/papillary-dominant LUAD [70,71,72]. Takada et al. indicated that the 1% cut-off level of PD-L1 was more sensitive in predicting postoperative prognosis than the 5% level. Early-stage LUAD patients with positive PD-L1 were correlated with poor DFS and OS at the 1% cut-off level [73]. For patients with stage I–III LUSC (n = 205), PD-L1 was also an effective marker for worsening OS at the 1% cut-off level [74]. A study by Azuma et al. examined the relationship between PD-L1 and EGFR alterations in stage I–IIIB NSCLC. The high expression level of PD-L1 correlated with EGFR alterations caused by EGFR signalling. Furthermore, high PD-L1 expression was a harmful indicator for OS (Median OS: high 55.9 months vs. low 72.6 months) [75]. Similarly, PD-L1 ≥ 1% was correlated with worsening DFS and OS in stage I–IIIA EGFR-mutated NSCLC [76]. Regarding the prognostic effects of CD8 (cut-off values: 543 per mm2) and PD-L1 (cut-off values: 1%) in resected NSCLC, CD8 positivity/PD-L1 negativity was favourable for RFS and OS [77]. Handa et al. also verified that NSCLC patients (Stage I) with high levels of PD-L1 (>5%) had a worse prognosis than patients with low levels of PD-L1 (five-year RFS: high 63.4% vs. low 81%, p = 0.061). When considering surrounding immune cells, the intratumoural CD8 level influenced the predictive value of PD-L1. It concluded that PD-L1 had no predictive effect on survival in high-level cohorts of intratumoural CD8, but overexpression of PD-L1 predicted significantly poor RFS in cohorts with low-level CD8 (five-year RFS: PD-L1 (>5%) 63.4% vs. PD-L1 (≤5%) 81%, p = 0.034) [78].
Stage I LUAD patients with high PD-L1 expression (≥5%) had a favourable prognosis for RFS but not OS [79]. Regarding stage IIB–IIIB LUAD, Gross et al. concluded that patients with high PD-L1 expression (≥1%) on tumour cells and tumour-associated macrophages (TAMs) received survival benefits from adjuvant chemotherapy [89]. Similarly, PD-L1 was correlated with a longer OS in early-stage NSCLC [80]. Teramoto et al. indicated that the prognostic effect of PD-L1 differed by the pathological stage. Postoperative RFS in location I NSCLC with high PD-L1 expression was significantly prolonged over those with low PD-L1 expression (five-year RFS: high 94.1% vs. low 75.1%, p = 0.031). Conversely, for patients with stage II–IIIA NSCLC, high PD-L1 expression was prone to postoperative recurrence [81]. However, Song et al. validated that PD-L1 was not correlated with DFS and OS in resected LUAD [82].
A meta-analysis involving 15 studies predicted that PD-L1 as an independent prognostic indicator was related to unfavourable DFS and OS [83]. In conclusion, high levels of PD-L1 indicated poor survival in resected NSCLC compared to low levels.
3.2.2. Other Immune-Related Markers
For early-stage LUAD patients, overexpression of PD-L2 (>1%) significantly predicted worsening DFS and OS [72]. TIM-3 positivity on tumour cells (≥24%) and tumour-infiltrating lymphocytes (TILs, ≥11%) was predictive of poor RFS and OS in early-stage LUAD. Subgroup analyses were conducted to investigate TIM-3/PD-1/CD8 expression levels for the prognosis of LUAD. The TIM-3 positivity/PD-1 positivity/CD8 negativity subgroup had the worst prognosis, whereas the TIM-3 negativity/PD-1 negativity/CD8 positivity subgroup had the best forecast [84]. Regarding early-stage nonsmoking patients, tumour mutation burden (TMB) was a poor prognostic indicator for OS [85]. Conversely, another study demonstrated that TMB had no prognostic value on stage I–II resected LUAD [86]. High OX40 (CD134) expression on TILs tended to unfavourable RFS and OS in location I NSCLC [87]. However, OX40, expressed on the surface of tumour-immune infiltrated cell membranes, correlated with favourable OS in stage I–III NSCLC [88].
We have summarised the prognostic significance of immune checkpoints for NSCLC patients. Meanwhile, we included relevant clinical trials to investigate the effect of ICIs on the prognosis of early-stage NSCLC. An RCT (IMpover010) enrolled 1280 NSCLC patients undergoing radical resection (IB–IIIA). After receiving four cycles of platinum-based chemotherapy, patients were randomised (1:1) to receive either 16 processes of adjuvant atezolizumab (PD-L1 inhibitor) or optimal supportive care. Finally, atezolizumab significantly prolonged DFS in stage II–IIIA patients with PD-L1 on tumours ≥ 1% (HR: 0.66; 95% CI: 0.50–0.88; p = 0.0039) and in all patients with stage II–IIIA (HR: 0.79; 95% CI: 0.64–0.96; p = 0.020) compared to optimal supportive treatment [90]. Another RCT (Checkmate 816) included resectable stage IB–IIIA NSCLC patients who underwent neoadjuvant nivolumab (PD-1 inhibitor) plus platinum-based chemotherapy (n = 179) or platinum-based chemotherapy alone (n = 179). The median event-free survival (EFS) was considerably longer in the neoadjuvant nivolumab plus chemotherapy group (31.6 months) than in the neoadjuvant chemotherapy group (20.8 months). The pathological complete response (pCR) rates were 24% and 2.2% in both groups, respectively [91]. A single-arm trial included 30 resectable NSCLC patients (Stage IB–IIIA) receiving neoadjuvant atezolizumab, carboplatin, and paclitaxel. A high proportion of patients (17/30, 57%) had a primary pathologic response (MPR) [92]. Although PD-L is a poor prognostic factor, adjuvant PD-L1 inhibitors can prolong survival in early-stage NSCLC. Additionally, the prophetic role of PD-1 is currently unknown, but neoadjuvant inhibitors of PD-1 can extend patient EFS.
3.3. Blood-Based Biomarkers
Although radical resection remains the preferred treatment option for early-stage NSCLC, the recurrence rates for lung cancer are still very high, indicating that micro-metastases still exist in the perioperative period. Therefore, we included studies on blood biomarkers, such as circulating tumour cells (CTCs), routine blood examinations, circulating nucleic acids, and tumour markers, to explore their prognostic value on early-stage NSCLC (Table 3).
3.3.1. CTCs
CTCs shed from the primary cancerous lesion and circulating in the bloodstream can result in tumour recurrence or distant metastases [162]. Several prospective studies have shown that preoperative peripheral venous CTCs were associated with unfavourable DFS and OS in resectable NSCLC [93,94]. Concerning peripheral folate receptor-positive CTCs (FR+ CTCs) in resected NSCLC, their high preoperative levels correlated with poor RFS and OS [95]. Meanwhile, in a study including patients with stage I–IIIA NSCLC (n = 30), a value of ≥3 for PD-L1+/EMT+ CTCs in preoperative peripheral blood predicted poor RFS and OS, but RFS failed to reach statistical differences, most likely attributed to the small sample size [96]. Miguel-Pérez et al. compared the prognostic effect of peripheral CTCs in LUAD and LUSC and concluded that postoperative CTCs were only associated with poor RFS and OS in LUAD [97]. Additionally, postoperative peripheral thyroid transcription factor-1 CTCs (TTF-1+ CTCs) predicted a worse PFS on early-stage NSCLC [98]. Li et al. revealed that preoperative and postoperative LUNX+ CTCS in peripheral blood were independent predictors of unfavourable DFS and OS in resected NSCLC [99]. Moreover, Crosbie et al. collected blood samples (10 mL) from the tumour-draining pulmonary veins of stage I–IIIA NSCLC patients (n = 30) and indicated that CTCs in pulmonary veins predicted worsening survival [100]. Similarly, CTCs with pulmonary vein dissemination before tumour resection in NSCLC were associated with lung-cancer-specific recurrence and poor DFS [101]—An RCT compared vein-first ligation versus artery-first ligation on CTCs and survival outcomes in resected NSCLC patients. The ligation of pulmonary veins first prevented CTCs from entering the circulation, and patients in the vein-first ligation had significantly better DFS, OS, and lung-cancer-specific survival (LCSS) [163]. In conclusion, a meta-analysis by Wankhede et al. revealed that baseline and postoperative CTCs correlated with worsening DFS and OS in early-stage NSCLC [102]. Therefore, CTCs in preoperative and postoperative peripheral blood and pulmonary veins may result in tumour recurrence and metastasis, ultimately leading to a poor prognosis.
3.3.2. Routine Examinations in Blood
Routine blood examinations have been performed on cancer patients during hospitalisation, and the results may reveal prognostic information about the patients.
Hemoglobin (Hb)
Regarding stage IB–II NSCLC patients, worsening OS was seen when baseline Hb was <120 g/L. By contrast, it had a tendency for favourable RFS in patients receiving adjuvant chemotherapy (ACT) with a nadir during-treatment Hb (<100 g/L) and favourable RFS and OS in patients with a maximum during-treatment decrease in Hb (>30%) [103].
Platelet (PLT)
Elevated PLT (>253 × 109/L) and lymphocytes (>1.8 × 109/L) in preoperative peripheral blood were independent prognostic factors for postoperative recurrence in pT1 NSCLC [104]. Hou et al. also revealed that high preoperative PLT (>215 × 109/L) correlated with unfavourable PFS in early-stage NSCLC [105].
White Blood Cells
Several studies have examined the role of circulatory inflammatory markers in the prognosis of NSCLC patients. Elevated white blood cells above the median (8.6 × 109 cells/L) were correlated with worsening RFS and OS in resected NSCLC (Stage I–IIIA) [106]. Kobayashi et al. confirmed that preoperative lymphocytes (cut-off values: 1900 mm−3) were independent favourable predictors for OS in resected NSCLC, but neutrophils (cut-off values: 4500 mm−3) were not [107]. A study involving 142 NSCLC patients (Stage IB–IIIA) concluded that preoperative lymphocytes (cut-off values: 1800 mm−3) were associated with a better DFS but not with OS, and neutrophils did not affect prognosis [108]. Conversely, Mitchell et al. concluded that preoperative elevated circulating neutrophils (>103 cells/µL) correlated with poor OS, but preoperative lymphocytes were not [109]. Another study examined the effect of giant peripheral tumour-macrophage fusion cells (TMFs) on the survival of stage I–IIIA NSCLC. More than one TMF and gigantic TMF sizes higher than or equal to 50 um were associated with worsening DFS and OS [110].
The circulating preoperative neutrophil–lymphocyte ratio (NLR) as a significant prognostic indicator was associated with reduced survival in early-stage NSCLC [111,112]. Another study confirmed that preoperative NLR (cut-off value: 3.3) was a marker for poor DFS and OS, whereas the platelet–lymphocyte ratio (PLR, cut-off values: 171) did not correlate with prognosis. Therefore, NLR was superior to PLR in terms of prognosis for pN0 NSCLC [113]. Seitlinger et al. focused on the preoperative and postoperative NLR in the prognosis of resected NSCLC. Both high NLR levels (>4.07) were associated with reduced OS and TTR [114]. A meta-analysis including 21 studies on the survival of early-stage NSCLC indicated that pretreatment-raised NLR (≥2.5) and PLR (≥150) were correlated with inferior DFS and OS [115]. Regarding the prognostic implications of the lymphocyte–monocyte ratio (LMR), a high baseline LMR (>3.68) may predict favourable DFS and OS in early-stage NSCLC [116]. The preoperative circulating uric acid-to-lymphocyte ratio (ULR, cut-off values: 3.83) was an independent predictor correlated with shortened DFS and OS in NSCLC patients (Stage I–II) [117]. Yan et al. combined neutrophil × platelet/lymphocyte to redefine the systemic immune-inflammation index (SII). High levels of preoperative SII (≥402.37) in resected NSCLC were indicative of worse DFS and OS [118].
3.3.3. Circulating Nucleic Acids
Circulating nucleic acids, including several DNA or RNA molecules, originate from cell apoptosis and necrosis in the circulation [164]. Several studies confirmed that circulating DNA and RNA were prognostic predictors in resected NSCLC.
Circulating Tumour DNA (ctDNA)
CtDNA is cell-derived free DNA from tumour cells in the blood. Regarding the prognostic significance of perioperative ctDNA in early-stage NSCLC, the study (DYNAMIC) revealed that detectable ctDNA at three days and one month after surgery predicted worsening RFS and OS when compared to undetectable ctDNA [119]. Similarly, postoperatively detectable plasma ctDNA was a worse predictor for PFS and OS [120]. Wang et al. also demonstrated that detectable ctDNA was positively correlated with an increasing possibility of tumour recurrence or metastasis in 82 patients with stage I LUAD [121]. Another study by Qiu et al. classified stage II–III NSCLC patients by considering whether they received adjuvant chemotherapy (ACT) or had postoperative detectable ctDNA, and patients with high levels of ctDNA had significantly reduced RFS when compared to patients with low levels of ctDNA, whether they received ACT or not [122]. LUNGCA-1 confirmed that high levels of ctDNA preoperatively predicted poor RFS. The authors performed postoperative ctDNA-based molecular residual disease (MRD) detection and concluded that MRD indicated tumour recurrence [123]. Furthermore, several studies revealed that stage I–III NSCLC patients with both presurgical and postsurgical positive ctDNA had poorer survival than patients with negative ctDNA [124,125]. Therefore, perioperatively detectable ctDNA can predict reduced survival in patients with early-stage NSCLC.
MicroRNAs (MiRNAs)
Circulating miRNAs as noninvasive indicators still have prognostic value in early-stage NSCLC. Hu et al. developed four serum miRNAs (miR-486, miR-30d, miR-1, and miR-499) as a microRNA signature, revealing that high levels of miR-486 and miR-30d and low levels of miR-1 and miR-499 significantly correlated with poor OS in stage I–IIIA NSCLC [126]. Heegaard et al. studied the prognosis of paired plasma and serum miRNAs in stage I–II NSCLC. It concluded that only high plasma expression of miR-let-7b was associated with increased CSS, and all serum miRNAs did not correlate with patient prognosis [127]. Another study demonstrated that NSCLC patients (Stage I–III) with higher exosome miR-451a in plasma had reduced DFS and OS compared to patients with lower exosome miR-451a [128]. Han et al. isolated several miRNAs in extracellular vesicles (EV) from pulmonary tumour drainage veins (TDVs) and identified miR-203a-3p as a recurrence marker in the 18-patient screening cohort. They further verified that miR-203a-3p was a prognostic indicator for unfavourable TTR in the 70-patient validation cohort [129].
3.3.4. Tumour Markers
The prognostic effect of tumour markers in early-stage NSCLC has been intensely reported.
Carcinoembryonic Antigen (CEA)
Sawabata et al. reported that pathological I–II NSCLC patients with high preoperative serum CEA (>7.0 ng/mL) exhibited significantly reduced five-year survival rates when compared to patients with normal CEA (five-year survival: high 49% vs. average 72%). Furthermore, patients with persistently high CEA after surgery had worse survival than those who returned to normal levels (five-year survival: high 18% vs. average 68%) [130]. Several studies also concluded that preoperative serum CEA significantly correlated with poor survival in resected NSCLC [131,132,133,134,135,136,137]. Hashinokuchi et al. even studied the combination of preoperative maximum standardised uptake value (SUVmax, cut-off values: 2.96) and CEA (cut-off values: 5.3 ng/mL) on the prognosis of stage IA LUAD. The survival time of patients with higher SC (SUVmax and CEA) levels was significantly reduced compared to patients with lower levels [138]. Regarding the predictive effects of postoperative CEA, serum elevated CEA was the significant determinant for worsening prognosis in stage I NSCLC [139,140,141,142]. In summary, high perioperative levels of CEA act as a predictor for poor survival in NSCLC patients.
CYFRA 21-1
Several studies have concluded that preoperative serum CYFRA21-1 was an independent predictor for unfavourable survival in early-stage NSCLC [135,143,144]. However, Kozu et al. revealed that preoperative CYFRA21-1 (cut-off values: 3.5 ng/mL) did not predict recurrence or survival in stage I NSCLC [136]. Mizuguchi et al. concluded that preoperative circulating CYFRA21-1 (cut-off values: 3.2 ng/mL) and Sialyl Lewisx (SLX, cut-off values: 36 U/mL) were independent predictors for poor survival in stage I NSCLC. Moreover, patients with the combination of CYFRA21-1 and SLX positivity had a significantly worse prognosis than those with negativity (five-year survival: positivity 13% vs. negativity 80%) [145]. The study by Muley et al. combined preoperative CYFRA21-1 (cut-off values: 3.3 ng/mL) and CEA (cut-off values: 9.8 ng/mL) to form a new parameter named tumour marker index (TMI) and demonstrated that elevated TMI (>0.54) negatively affected OS in stage I–II NSCLC patients [146].
Other Tumour Markers
Preoperative serum neuron-specific enolase (NSE), squamous cell carcinoma antigen (SCC-Ag), CA125, and CA199 had no significant effect on stage I NSCLC patients’ prognoses [147]. Reinmuth et al. also confirmed that NSE and SCC-Ag did not affect the survival of early-stage NSCLC (Stage I–IIIA) [143]. In contrast, a retrospective study demonstrated that preoperatively elevated NSE (>12.5 ng/mL) and CA125 (>35 U/mL) significantly correlated with poor DFS and OS in resected NSCLC patients. Furthermore, SCC-Ag (cut-off values: 1.5 ng/mL) did not affect all patients’ survival. However, SCC-Ag was only associated with reduced DFS and OS in LUSC patients [148]. Another retrospective study revealed that preoperative increased CA125 (>3.2 ng/mL) or CA199 (>3.2 ng/mL) correlated with poor RFS in resected LUAD patients (Stage IA-IIIA) [149]. Therefore, the prognostic value of circulating NSE, SCC-Ag, CA125, and CA199 in early-stage NSCLC remains debatable.
3.3.5. Other Blood Biomarkers
C-Reactive Protein (CRP)
CRP is a marker for the circulating inflammatory response, and stage I–III patients with elevated preoperative CRP (>10 mg/L) had shorter CSS compared to patients with normal CRP (median survival: elevated 26.2 months vs. normal 75.9 months) [150]. Similarly, the preoperative levels of CRP ≥20 mg/L also correlated with worsening OS in stage I–II NSCLC, which was also confirmed in the validation group [151].
Fibrinogen and D-Dimer
Preoperative increased serum fibrinogen (≥4 g/L) was an effective predictor for worsening PFS and OS in resected NSCLC [152]. D-dimers are predictors of circulating fibrinolytic system activation. Assessing 232 patients with stage I–IIIA NSCLC, it was found that preoperative plasma D-dimer (cut-off values: 0.3 ug/mL) in plasma was an independent marker for reduced OS (one-year OS: high 76.5% vs. average 93.9%) [153]. Jiang et al. confirmed that preoperative and postoperative plasma high levels of fibrinogen (≥4 g/L) and D-dimer (≥0.55 mg/L) correlated with reduced DFS and OS in early-stage NSCLC [154]. However, Hou et al. confirmed that preoperative fibrinogen and D-dimer did not correlate with patient survival. This may be attributed to the short follow-up of 13.2 months [105].
Albumin
Kawai et al. revealed that preoperative (>23 mg/dL) and postoperative (>15 mg/dL) elevated albumin was an independent determinant for unfavourable DFS in resected NSCLC (Stage IA-IIIB) [155]. Preoperative circulating albumin and lymphocytes were combined as the prognostic nutritional index (PNI), and resected NSCLC patients with higher levels of PNI (≥48) had a greater prolonged RFS and OS than patients with lower levels [156]. Yamauchi et al. calculated the CRP–albumin ratio (CAR) to elucidate its prognostic effect in IIIA LUAD patients (n = 156), concluding that CAR (cut-off values: 0.6) was an unfavourable biomarker for RFS [157]. The study by Li et al. also confirmed that resected NSCLC patients with a preoperative albumin–globulin score (AGS) of 2 had significantly reduced DFS and OS than patients with an AGS of 0 or 1 [158]. For early-stage NSCLC patients receiving lobectomy, the preoperative albumin–globulin ratio (AGR, cut-off values: 1.76) independently predicted favourable survival [159].
Osteopontin (OPN)
Several investigators have examined the predictive effects of OPN in NSCLC patients receiving radical surgery. Patients with high preoperative serum levels of OPN (>81.3 ng/mL) had a poorer prognosis than patients with low levels (five-year survival: high 63.7% vs. low 82.0%) [160]. However, another study indicated that serum OPN did not affect the prognosis of resected NSCLC patients [161].
4. Conclusions
Treatment modalities for early-stage NSCLC have changed dramatically over the last decades, yet the postoperative survival of these patients remains unsatisfactory. Hence, we included mutant genes, immune-related indicators from resected tumours, and blood biomarkers to explore their prognostic effect on NSCLC. The prognostic impact of alterations on the EGFR, ALK, MET, ROS1, or TP53 in resected NSCLC remains debatable for mutant genes. KRAS alterations indicate unfavourable outcomes in early-stage NSCLC. Regarding early-stage NSCLC with EGFR alterations, adjuvant or neoadjuvant EGFR-TKIs can significantly improve patient prognosis. Due to limited data on other driver genes with low alteration frequencies, the forecast can only be assessed with further studies. Based on current studies, resected NSCLC patients with high levels of PD-L1 exhibited lower survival than those with low levels. Conversely, PD-L1 or PD-1 inhibitors can substantially increase patient survival. Other immune checkpoints (PD-1, PD-L2, and TIM-3) also lacked prognostic value owing to the limited number of studies. For circulating indicators, preoperative and postoperative peripheral venous CTCs and pulmonary venous CTCs predicted unfavourable prognoses, leading to distant metastases in NSCLC. Similarly, patients with detectable perioperative ctDNA also had inferior survival. CEA, as a circulating tumour marker, has been studied extensively. Patients with preoperatively and postoperatively elevated CEA in the circulation predicted significantly reduced survival outcomes.
Several genetic alterations and immune and circulatory indicators show superior predictions for the prognoses and treatment responses of early-stage NSCLC. Autonomous artificial intelligence (AI) systems combined with CT images can provide noninvasive whole-lung analyses to forecast the projections of lung cancer patients receiving EGFR-TKI therapy [165]. Additionally, the AI algorithms identified 32 preoperative markers in the blood, including CA125, CA199, and CRP, to predict the outcomes of epithelial ovarian cancer [166]. In the future, we will incorporate mutated genes, immune checkpoints, and blood-based biomarkers by applying AI to construct new prognostic models that predict patient outcomes accurately and guide individualised treatment (Figure 1). Furthermore, combined models as biological factors should be incorporated into the tumour–node-metastasis (TNM) staging system.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers15184561/s1, Text S1: Detailed retrieval strategies in PubMed.
Author Contributions
Conceptualization, Q.T.; methodology, X.J.; validation, W.C., Q.T. and J.Z.; writing—original draft preparation, W.C.; writing—review and editing, S.X. and L.Z.; supervision, S.X. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the National Natural Science Foundation of China (82172776), Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-061B and TJWJ2022XK005), and Diversified Input Project of Tianjin National Natural Science Foundation (21JCYBJC01770).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef] [PubMed]
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143 (Suppl. S5), e278S–e313S. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Asamura, H.; Bankier, A.A.; Beasley, M.B.; Detterbeck, F.; Flieder, D.B.; Goo, J.M.; MacMahon, H.; Naidich, D.; Nicholson, A.G.; et al. The IASLC Lung Cancer Staging Project: Proposals for Coding T Categories for Subsolid Nodules and Assessment of Tumor Size in Part-Solid Tumors in the Forthcoming Eighth Edition of the TNM Classification of Lung Cancer. J. Thorac. Oncol. 2016, 11, 1204–1223. [Google Scholar] [CrossRef] [PubMed]
- da Cunha Santos, G.; Shepherd, F.A.; Tsao, M.S. EGFR mutations and lung cancer. Annu. Rev. Pathol. 2011, 6, 49–69. [Google Scholar] [CrossRef]
- Reck, M.; Carbone, D.P.; Garassino, M.; Barlesi, F. Targeting KRAS in non-small-cell lung cancer: Recent progress and new approaches. Ann. Oncol. 2021, 32, 1101–1110. [Google Scholar] [CrossRef]
- Yu, H.; Boyle, T.A.; Zhou, C.; Rimm, D.L.; Hirsch, F.R. PD-L1 Expression in Lung Cancer. J. Thorac. Oncol. 2016, 11, 964–975. [Google Scholar] [CrossRef]
- Dyck, L.; Mills, K.H.G. Immune checkpoints and their inhibition in cancer and infectious diseases. Eur. J. Immunol. 2017, 47, 765–779. [Google Scholar] [CrossRef]
- Takahashi, T.; Sakai, K.; Kenmotsu, H.; Yoh, K.; Daga, H.; Ohira, T.; Ueno, T.; Aoki, T.; Hayashi, H.; Yamazaki, K.; et al. Predictive value of EGFR mutation in non-small-cell lung cancer patients treated with platinum doublet postoperative chemotherapy. Cancer Sci. 2022, 113, 287–296. [Google Scholar] [CrossRef]
- Deng, C.; Zhang, Y.; Ma, Z.; Fu, F.; Deng, L.; Li, Y.; Chen, H. Prognostic value of epidermal growth factor receptor gene mutation in resected lung adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2021, 162, 664–674.e7. [Google Scholar] [CrossRef]
- Ito, M.; Miyata, Y.; Tsutani, Y.; Ito, H.; Nakayama, H.; Imai, K.; Ikeda, N.; Okada, M. Positive EGFR mutation status is a risk of recurrence in pN0-1 lung adenocarcinoma when combined with pathological stage and histological subtype: A retrospective multi-center analysis. Lung Cancer 2020, 141, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Liu, Z.; Wang, Y.; Zhang, Y.; Qian, F.; Lu, J.; Wang, H.; Gu, P.; Hu, M.; Chen, Y.; et al. The clinicopathological and molecular characteristics of resected EGFR-mutant lung adenocarcinoma. Cancer Med. 2022, 11, 1299–1309. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Shimizu, S.; Okuda, K.; Kawano, O.; Yukiue, H.; Yano, M.; Fujii, Y. Epidermal growth factor receptor gene amplification in surgical resected Japanese lung cancer. Lung Cancer 2009, 64, 295–300. [Google Scholar] [CrossRef]
- Isaka, T.; Nakayama, H.; Ito, H.; Yokose, T.; Yamada, K.; Masuda, M. Impact of the epidermal growth factor receptor mutation status on the prognosis of recurrent adenocarcinoma of the lung after curative surgery. BMC Cancer 2018, 18, 959. [Google Scholar] [CrossRef] [PubMed]
- Izar, B.; Sequist, L.; Lee, M.; Muzikansky, A.; Heist, R.; Iafrate, J.; Dias-Santagata, D.; Mathisen, D.; Lanuti, M. The impact of EGFR mutation status on outcomes in patients with resected stage I non-small cell lung cancers. Ann. Thorac. Surg. 2013, 96, 962–968. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-P.; Wu, H.-D.I.; Chang, J.W.-C.; Wu, Y.-C.; Yang, H.-Y.; Chen, Y.-T.; Hsieh, W.-Y.; Chen, Y.-T.; Chen, Y.-R.; Huang, S.-F. Prognostic implications of epidermal growth factor receptor and KRAS gene mutations and epidermal growth factor receptor gene copy numbers in patients with surgically resectable non-small cell lung cancer in Taiwan. J. Thorac. Oncol. 2010, 5, 1175–1184. [Google Scholar] [CrossRef]
- Isaka, T.; Ito, H.; Nakayama, H.; Yokose, T.; Yamada, K.; Masuda, M. Effect of epidermal growth factor receptor mutation on early-stage non-small cell lung cancer according to the 8th TNM classification. Lung Cancer 2020, 145, 111–118. [Google Scholar] [CrossRef]
- Na, I.I.; Rho, J.K.; Choi, Y.J.; Kim, C.H.; Koh, J.S.; Ryoo, B.-Y.; Yang, S.H.; Lee, J.C. Clinical features reflect exon sites of EGFR mutations in patients with resected non-small-cell lung cancer. J. Korean Med. Sci. 2007, 22, 393–399. [Google Scholar] [CrossRef]
- Renaud, S.; Seitlinger, J.; Guerrera, F.; Reeb, J.; Beau-Faller, M.; Voegeli, A.-C.; Siat, J.; Clément-Duchêne, C.; Tiotiu, A.; Santelmo, N.; et al. Prognostic Value of Exon 19 Versus 21 EGFR Mutations Varies According to Disease Stage in Surgically Resected Non-small Cell Lung Cancer Adenocarcinoma. Ann. Surg. Oncol. 2018, 25, 1069–1078. [Google Scholar] [CrossRef]
- Isaka, T.; Nakayama, H.; Yokose, T.; Ito, H.; Miyagi, Y.; Matsuzaki, T.; Nagata, M.; Furumoto, H.; Nishii, T.; Katayama, K.; et al. Epidermal Growth Factor Receptor Mutations and Prognosis in Pathologic N1-N2 Pulmonary Adenocarcinoma. Ann. Thorac. Surg. 2016, 102, 1821–1828. [Google Scholar] [CrossRef]
- Hayasaka, K.; Shiono, S.; Matsumura, Y.; Yanagawa, N.; Suzuki, H.; Abe, J.; Sagawa, M.; Sakurada, A.; Katahira, M.; Takahashi, S.; et al. Epidermal Growth Factor Receptor Mutation as a Risk Factor for Recurrence in Lung Adenocarcinoma. Ann. Thorac. Surg. 2018, 105, 1648–1654. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Kawaguchi, T.; Watanabe, M.; Isa, S.-I.; Ando, M.; Tamiya, A.; Kubo, A.; Kitagawa, C.; Yoshimoto, N.; Koh, Y. Prognostic impact of pretreatment T790M mutation on outcomes for patients with resected, EGFR-mutated, non-small cell lung cancer. BMC Cancer 2022, 22, 775. [Google Scholar] [CrossRef] [PubMed]
- Sonnweber, B.; Dlaska, M.; Skvortsov, S.; Dirnhofer, S.; Schmid, T.; Hilbe, W. High predictive value of epidermal growth factor receptor phosphorylation but not of EGFRvIII mutation in resected stage I non-small cell lung cancer (NSCLC). J. Clin. Pathol. 2006, 59, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.D.; Caso, R.; Tan, K.S.; Mastrogiacomo, B.; Sanchez-Vega, F.; Liu, Y.; Connolly, J.G.; Murciano-Goroff, Y.R.; Bott, M.J.; Adusumilli, P.S.; et al. Mutation is Associated with Increased Risk of Recurrence in Surgically Resected Lung Adenocarcinoma. Clin. Cancer Res. 2021, 27, 2604–2612. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.P.; Janjigian, Y.Y.; Ahye, N.; Riely, G.J.; Chaft, J.E.; Sima, C.S.; Shen, R.; Zheng, J.; Dycoco, J.; Kris, M.G.; et al. Distinct clinical course of EGFR-mutant resected lung cancers: Results of testing of 1118 surgical specimens and effects of adjuvant gefitinib and erlotinib. J. Thorac. Oncol. 2012, 7, 1815–1822. [Google Scholar] [CrossRef]
- Izar, B.; Zhou, H.; Heist, R.S.; Azzoli, C.G.; Muzikansky, A.; Scribner, E.E.F.; Bernardo, L.A.; Dias-Santagata, D.; Iafrate, A.J.; Lanuti, M. The prognostic impact of KRAS, its codon and amino acid specific mutations, on survival in resected stage I lung adenocarcinoma. J. Thorac. Oncol. 2014, 9, 1363–1369. [Google Scholar] [CrossRef]
- Kadota, K.; Sima, C.S.; Arcila, M.E.; Hedvat, C.; Kris, M.G.; Jones, D.R.; Adusumilli, P.S.; Travis, W.D. KRAS Mutation Is a Significant Prognostic Factor in Early-stage Lung Adenocarcinoma. Am. J. Surg. Pathol. 2016, 40, 1579–1590. [Google Scholar] [CrossRef]
- Kneuertz, P.J.; Carbone, D.P.; D’Souza, D.M.; Shilo, K.; Abdel-Rasoul, M.; Zhao, W.; Williams, T.M.; Jones, D.; Merritt, R.E. Prognostic value and therapeutic implications of expanded molecular testing for resected early stage lung adenocarcinoma. Lung Cancer 2020, 143, 60–66. [Google Scholar] [CrossRef]
- Ayyoub, M.; Memeo, L.; Alvarez-Fernández, E.; Colarossi, C.; Costanzo, R.; Aiello, E.; Martinetti, D.; Valmori, D. Assessment of MAGE-A expression in resected non-small cell lung cancer in relation to clinicopathologic features and mutational status of EGFR and KRAS. Cancer Immunol. Res. 2014, 2, 943–948. [Google Scholar] [CrossRef]
- Fujibayashi, Y.; Tane, S.; Kitazume, M.; Kuroda, S.; Kimura, K.; Kitamura, Y.; Nishio, W. Resected stage I anaplastic lymphoma kinase-positive lung adenocarcinoma has a negative impact on recurrence-free survival. Thorac. Cancer 2022, 13, 1109–1116. [Google Scholar] [CrossRef]
- Chaft, J.E.; Dagogo-Jack, I.; Santini, F.C.; Eng, J.; Yeap, B.Y.; Izar, B.; Chin, E.; Jones, D.R.; Kris, M.G.; Shaw, A.T.; et al. Clinical outcomes of patients with resected, early-stage ALK-positive lung cancer. Lung Cancer 2018, 122, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, Y.; Ninomiya, H.; Ichinose, J.; Nakao, M.; Okumura, S.; Nishio, M.; Mun, M. Prognostic impact and distinctive characteristics of surgically resected anaplastic lymphoma kinase-rearranged lung adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2022, 163, 441–451.e1. [Google Scholar] [CrossRef] [PubMed]
- Tao, H.; Shi, L.; Zhou, A.; Li, H.; Gai, F.; Huang, Z.; Che, N.; Liu, Z. Distribution of EML4-ALK fusion variants and clinical outcomes in patients with resected non-small cell lung cancer. Lung Cancer 2020, 149, 154–161. [Google Scholar] [CrossRef]
- Sun, J.-M.; Lira, M.; Pandya, K.; Choi, Y.-L.; Ahn, J.S.; Mao, M.; Han, J.; Park, K.; Ahn, M.-J.; Kim, J. Clinical characteristics associated with ALK rearrangements in never-smokers with pulmonary adenocarcinoma. Lung Cancer 2014, 83, 259–264. [Google Scholar] [CrossRef]
- Paik, J.H.; Choi, C.-M.; Kim, H.; Jang, S.J.; Choe, G.; Kim, D.K.; Kim, H.J.; Yoon, H.; Lee, C.-T.; Jheon, S.; et al. Clinicopathologic implication of ALK rearrangement in surgically resected lung cancer: A proposal of diagnostic algorithm for ALK-rearranged adenocarcinoma. Lung Cancer 2012, 76, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.-H.; Lee, I.H.; Lee, J.E.; Hong, S.H.; Kim, T.-J.; Lee, K.-Y.; Kim, Y.K.; Kim, S.J.; Sung, S.W.; Park, J.K.; et al. Clinical Significance of C-MET Overexpression and Epidermal Growth Factor Receptor Mutation in Platinum-Based Adjuvant Chemotherapy Outcome in Surgically Resected Lung Adenocarcinoma. Ann. Surg. Oncol. 2017, 24, 770–777. [Google Scholar] [CrossRef]
- Cappuzzo, F.; Marchetti, A.; Skokan, M.; Rossi, E.; Gajapathy, S.; Felicioni, L.; Del Grammastro, M.; Sciarrotta, M.G.; Buttitta, F.; Incarbone, M.; et al. Increased MET gene copy number negatively affects survival of surgically resected non-small-cell lung cancer patients. J. Clin. Oncol. 2009, 27, 1667–1674. [Google Scholar] [CrossRef]
- Bubendorf, L.; Dafni, U.; Schöbel, M.; Finn, S.P.; Tischler, V.; Sejda, A.; Marchetti, A.; Thunnissen, E.; Verbeken, E.K.; Warth, A.; et al. Prevalence and clinical association of MET gene overexpression and amplification in patients with NSCLC: Results from the European Thoracic Oncology Platform (ETOP) Lungscape project. Lung Cancer 2017, 111, 143–149. [Google Scholar] [CrossRef]
- Lee, G.D.; Lee, S.E.; Oh, D.-Y.; Yu, D.-B.; Jeong, H.M.; Kim, J.; Hong, S.; Jung, H.S.; Oh, E.; Song, J.-Y.; et al. MET Exon 14 Skipping Mutations in Lung Adenocarcinoma: Clinicopathologic Implications and Prognostic Values. J. Thorac. Oncol. 2017, 12, 1233–1246. [Google Scholar] [CrossRef]
- Kim, I.A.; Hur, J.Y.; Kim, H.J.; Park, J.H.; Hwang, J.J.; Lee, S.A.; Lee, S.E.; Kim, W.S.; Lee, K.Y. Targeted Next-Generation Sequencing Analysis for Recurrence in Early-Stage Lung Adenocarcinoma. Ann. Surg. Oncol. 2021, 28, 3983–3993. [Google Scholar] [CrossRef]
- Chen, Y.-F.; Hsieh, M.-S.; Wu, S.-G.; Chang, Y.-L.; Shih, J.-Y.; Liu, Y.-N.; Tsai, M.-F.; Tsai, T.-H.; Yu, C.-J.; Yang, J.C.-H.; et al. Clinical and the prognostic characteristics of lung adenocarcinoma patients with ROS1 fusion in comparison with other driver mutations in East Asian populations. J. Thorac. Oncol. 2014, 9, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Jao, K.; Tomasini, P.; Kamel-Reid, S.; Korpanty, G.J.; Mascaux, C.; Sakashita, S.; Labbé, C.; Leighl, N.B.; Liu, G.; Feld, R.; et al. The prognostic effect of single and multiple cancer-related somatic mutations in resected non-small-cell lung cancer. Lung Cancer 2018, 123, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Wang, Y.; Ren, F.; Li, X.; Ren, D.; Dong, M.; Chen, G.; Song, Z.; Chen, J. Impact of genetic alterations on outcomes of patients with stage I nonsmall cell lung cancer: An analysis of the cancer genome atlas data. Cancer Med. 2020, 9, 7686–7694. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Sanchez-Vega, F.; Caso, R.; Tan, K.S.; Brandt, W.S.; Jones, G.D.; Yan, S.; Adusumilli, P.S.; Bott, M.; Huang, J.; et al. Analysis of Tumor Genomic Pathway Alterations Using Broad-Panel Next-Generation Sequencing in Surgically Resected Lung Adenocarcinoma. Clin. Cancer Res. 2019, 25, 7475–7484. [Google Scholar] [CrossRef] [PubMed]
- Ludovini, V.; Pistola, L.; Gregorc, V.; Floriani, I.; Rulli, E.; Piattoni, S.; Di Carlo, L.; Semeraro, A.; Darwish, S.; Tofanetti, F.R.; et al. Plasma DNA, microsatellite alterations, and p53 tumor mutations are associated with disease-free survival in radically resected non-small cell lung cancer patients: A study of the perugia multidisciplinary team for thoracic oncology. J. Thorac. Oncol. 2008, 3, 365–373. [Google Scholar] [CrossRef]
- Laudanski, J.; Niklinska, W.; Burzykowski, T.; Chyczewski, L.; Niklinski, J. Prognostic significance of p53 and bcl-2 abnormalities in operable nonsmall cell lung cancer. Eur. Respir. J. 2001, 17, 660–666. [Google Scholar] [CrossRef]
- McGowan, M.; Hoven, A.S.; Lund-Iversen, M.; Solberg, S.; Helland, Å.; Hirsch, F.R.; Brustugun, O.T. PIK3CA mutations as prognostic factor in squamous cell lung carcinoma. Lung Cancer 2017, 103, 52–57. [Google Scholar] [CrossRef]
- Song, Z.; Yu, X.; Zhang, Y. Mutation and prognostic analyses of PIK3CA in patients with completely resected lung adenocarcinoma. Cancer Med. 2016, 5, 2694–2700. [Google Scholar] [CrossRef]
- Imperatori, A.; Sahnane, N.; Rotolo, N.; Franzi, F.; Nardecchia, E.; Libera, L.; Romualdi, C.; Cattoni, M.; Sessa, F.; Dominioni, L.; et al. LINE-1 hypomethylation is associated to specific clinico-pathological features in Stage I non-small cell lung cancer. Lung Cancer 2017, 108, 83–89. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, H.R.; Lee, C.Y.; Shin, M.; Shim, H.S. EGFR and TTF-1 gene amplification in surgically resected lung adenocarcinomas: Clinicopathologic significance and effect on response to EGFR-tyrosine kinase inhibitors in recurred cases. Ann. Surg. Oncol. 2013, 20, 3015–3022. [Google Scholar] [CrossRef]
- Liu, D.-H.; Zhao, Z.-R.; Lin, Y.-B.; Zhou, W.-J.; Hou, J.-Y.; Ye, Z.-H.; Long, H. Prognostic Effect of TP53 and PKD Co-Mutations in Patients with Resected Epidermal Growth Factor Receptor-Mutated Lung Adenocarcinoma. Ann. Surg. Oncol. 2019, 26, 1934–1941. [Google Scholar] [CrossRef] [PubMed]
- Lemmon, M.A.; Schlessinger, J.; Ferguson, K.M. The EGFR family: Not so prototypical receptor tyrosine kinases. Cold Spring Harb. Perspect. Biol. 2014, 6, a020768. [Google Scholar] [CrossRef] [PubMed]
- London, M.; Gallo, E. Epidermal growth factor receptor (EGFR) involvement in epithelial-derived cancers and its current antibody-based immunotherapies. Cell Biol. Int. 2020, 44, 1267–1282. [Google Scholar] [CrossRef]
- Wheeler, D.L.; Dunn, E.F.; Harari, P.M. Understanding resistance to EGFR inhibitors-impact on future treatment strategies, nature reviews. Clin. Oncol. 2010, 7, 493–507. [Google Scholar]
- Lai, Y.; Zhang, Z.; Li, J.; Sun, D.; Zhou, Y.A.; Jiang, T.; Han, Y.; Huang, L.; Zhu, Y.; Li, X.; et al. EGFR mutations in surgically resected fresh specimens from 697 consecutive Chinese patients with non-small cell lung cancer and their relationships with clinical features. Int. J. Mol. Sci. 2013, 14, 24549–24559. [Google Scholar] [CrossRef] [PubMed]
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar]
- Herbst, R.S.; Wu, Y.-L.; John, T.; Grohe, C.; Majem, M.; Wang, J.; Kato, T.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; et al. Adjuvant Osimertinib for Resected EGFR-Mutated Stage IB–IIIA Non-Small-Cell Lung Cancer: Updated Results From the Phase III Randomized ADAURA Trial. J. Clin. Oncol. 2023, 41, 1830–1840. [Google Scholar] [CrossRef]
- Tsuboi, M.; Herbst, R.S.; John, T.; Kato, T.; Majem, M.; Grohé, C.; Wang, J.; Goldman, J.W.; Lu, S.; Su, W.-C.; et al. Overall Survival with Osimertinib in Resected EGFR-Mutated NSCLC. N. Engl. J. Med. 2023, 389, 137–147. [Google Scholar] [CrossRef]
- Zhong, W.-Z.; Wang, Q.; Mao, W.-M.; Xu, S.-T.; Wu, L.; Shen, Y.; Liu, Y.-Y.; Chen, C.; Cheng, Y.; Xu, L.; et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II–IIIA (N1-N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): A randomised, open-label, phase 3 study. Lancet Oncol. 2018, 19, 139–148. [Google Scholar] [CrossRef]
- Zhong, W.-Z.; Chen, K.-N.; Chen, C.; Gu, C.-D.; Wang, J.; Yang, X.-N.; Mao, W.-M.; Wang, Q.; Qiao, G.-B.; Cheng, Y.; et al. Erlotinib Versus Gemcitabine Plus Cisplatin as Neoadjuvant Treatment of Stage IIIA-N2 EGFR-Mutant Non-Small-Cell Lung Cancer (EMERGING-CTONG 1103): A Randomized Phase II Study. J. Clin. Oncol. 2019, 37, 2235–2245. [Google Scholar] [CrossRef]
- Malumbres, M.; Barbacid, M. RAS oncogenes: The first 30 years. Nat. Rev. Cancer 2003, 3, 459–465. [Google Scholar] [CrossRef]
- Meng, D.; Yuan, M.; Li, X.; Chen, L.; Yang, J.; Zhao, X.; Ma, W.; Xin, J. Prognostic value of K-RAS mutations in patients with non-small cell lung cancer: A systematic review with meta-analysis. Lung Cancer 2013, 81, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.W.; Kirstein, M.N.; Valentine, M.B.; Dittmer, K.G.; Shapiro, D.N.; Saltman, D.L.; Look, A.T. Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin’s lymphoma. Science 1994, 263, 1281–1284. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, B.; Palmer, R.H. The role of the ALK receptor in cancer biology. Ann. Oncol. 2016, 27 (Suppl. S3), iii4–iii15. [Google Scholar] [CrossRef]
- Koch, J.P.; Aebersold, D.M.; Zimmer, Y.; Medová, M. MET targeting: Time for a rematch. Oncogene 2020, 39, 2845–2862. [Google Scholar] [CrossRef] [PubMed]
- Drilon, A.; Jenkins, C.; Iyer, S.; Schoenfeld, A.; Keddy, C.; Davare, M.A. ROS1-dependent cancers—Biology, diagnostics and therapeutics. Nature reviews. Clin. Oncol. 2021, 18, 35–55. [Google Scholar]
- Borrero, L.J.H.; El-Deiry, W.S. Tumor suppressor p53: Biology, signaling pathways, and therapeutic targeting. Biochim. Biophys. Acta Rev. Cancer 2021, 1876, 188556. [Google Scholar] [CrossRef]
- Ibáñez, C.F. Structure and physiology of the RET receptor tyrosine kinase. Cold Spring Harb. Perspect. Biol. 2013, 5, a009134. [Google Scholar] [CrossRef] [PubMed]
- Zaman, A.; Wu, W.; Bivona, T.G. Targeting Oncogenic BRAF: Past, Present, and Future. Cancers 2019, 11, 1197. [Google Scholar] [CrossRef]
- Cha, Y.J.; Kim, H.R.; Lee, C.Y.; Cho, B.C.; Shim, H.S. Clinicopathological and prognostic significance of programmed cell death ligand-1 expression in lung adenocarcinoma and its relationship with p53 status. Lung Cancer 2016, 97, 73–80. [Google Scholar] [CrossRef]
- Kim, M.; Chung, Y.S.; Kim, K.A.; Shim, H.S. Prognostic factors of acinar- or papillary-predominant adenocarcinoma of the lung. Lung Cancer 2019, 137, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Takamori, S.; Takada, K.; Azuma, K.; Jogo, T.; Shimokawa, M.; Toyokawa, G.; Hirai, F.; Tagawa, T.; Kawahara, A.; Akiba, J.; et al. Prognostic Impact of Programmed Death-Ligand 2 Expression in Primary Lung Adenocarcinoma Patients. Ann. Surg. Oncol. 2019, 26, 1916–1924. [Google Scholar] [CrossRef] [PubMed]
- Takada, K.; Okamoto, T.; Shoji, F.; Shimokawa, M.; Akamine, T.; Takamori, S.; Katsura, M.; Suzuki, Y.; Fujishita, T.; Toyokawa, G.; et al. Clinical Significance of PD-L1 Protein Expression in Surgically Resected Primary Lung Adenocarcinoma. J. Thorac. Oncol. 2016, 11, 1879–1890. [Google Scholar] [CrossRef] [PubMed]
- Takada, K.; Okamoto, T.; Toyokawa, G.; Kozuma, Y.; Matsubara, T.; Haratake, N.; Akamine, T.; Takamori, S.; Katsura, M.; Shoji, F.; et al. The expression of PD-L1 protein as a prognostic factor in lung squamous cell carcinoma. Lung Cancer 2017, 104, 7–15. [Google Scholar] [CrossRef]
- Azuma, K.; Ota, K.; Kawahara, A.; Hattori, S.; Iwama, E.; Harada, T.; Matsumoto, K.; Takayama, K.; Takamori, S.; Kage, M.; et al. Association of PD-L1 overexpression with activating EGFR mutations in surgically resected nonsmall-cell lung cancer. Ann. Oncol. 2014, 25, 1935–1940. [Google Scholar] [CrossRef]
- Saw, S.P.L.; Ng, W.P.; Zhou, S.; Lai, G.G.Y.; Tan, A.C.; Ang, M.-K.; Lim, W.-T.; Kanesvaran, R.; Ng, Q.S.; Jain, A.; et al. PD-L1 score as a prognostic biomarker in asian early-stage epidermal growth factor receptor-mutated lung cancer. Eur. J. Cancer 2023, 178, 139–149. [Google Scholar] [CrossRef]
- Kim, S.-H.; Go, S.-I.; Song, D.H.; Park, S.W.; Kim, H.R.; Jang, I.; Kim, J.D.; Lee, J.S.; Lee, G.-W. Prognostic impact of CD8 and programmed death-ligand 1 expression in patients with resectable non-small cell lung cancer. Br. J. Cancer 2019, 120, 547–554. [Google Scholar] [CrossRef]
- Handa, Y.; Tsutani, Y.; Shiroma, N.; Kai, Y.; Mimae, T.; Miyata, Y.; Takeshima, Y.; Arihiro, K.; Okada, M. Prognostic Impact of Programmed Death-ligand 1 and Surrounding Immune Status on Stage I Lung Cancer. Clin. Lung Cancer 2020, 21, e302–e314. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Lin, M.-W.; Chang, Y.-L.; Wu, C.-T.; Yang, P.-C. Programmed cell death-ligand 1 expression in surgically resected stage I pulmonary adenocarcinoma and its correlation with driver mutations and clinical outcomes. Eur. J. Cancer 2014, 50, 1361–1369. [Google Scholar] [CrossRef]
- Cooper, W.A.; Tran, T.; Vilain, R.E.; Madore, J.; Selinger, C.I.; Kohonen-Corish, M.; Yip, P.; Yu, B.; O’Toole, S.A.; McCaughan, B.C.; et al. PD-L1 expression is a favorable prognostic factor in early stage non-small cell carcinoma. Lung Cancer 2015, 89, 181–188. [Google Scholar] [CrossRef]
- Teramoto, K.; Igarashi, T.; Kataoka, Y.; Ishida, M.; Hanaoka, J.; Sumimoto, H.; Daigo, Y. Biphasic prognostic significance of PD-L1 expression status in patients with early- and locally advanced-stage non-small cell lung cancer. Cancer Immunol. Immunother. 2021, 70, 1063–1074. [Google Scholar] [CrossRef]
- Song, Z.; Yu, X.; Cheng, G.; Zhang, Y. Programmed death-ligand 1 expression associated with molecular characteristics in surgically resected lung adenocarcinoma. J. Transl. Med. 2016, 14, 188. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Zhu, S.; Guo, H.; Li, X.; Zhao, S.; Wang, Y.; Lei, X.; Huang, D.; Peng, L.; Li, Z.; et al. The Impact of Programmed Death-Ligand 1 Expression on the Prognosis of Early Stage Resected Non-Small Cell Lung Cancer: A Meta-Analysis of Literatures. Front. Oncol. 2021, 11, 567978. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Xie, H.; Dai, C.; Ren, Y.; She, Y.; Xu, L.; Chen, D.; Xie, D.; Zhang, L.; Jiang, G.; et al. Characterization of TIM-3 expression and its prognostic value in patients with surgically resected lung adenocarcinoma. Lung Cancer 2018, 121, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Ruel, L.-J.; Li, Z.; Gaudreault, N.; Henry, C.; Armero, V.S.; Boudreau, D.K.; Zhang, T.; Landi, M.T.; Labbé, C.; Couture, C.; et al. Tumor Mutational Burden by Whole-Genome Sequencing in Resected NSCLC of Never Smokers. Cancer Epidemiol. Biomarkers Prev. 2022, 31, 2219–2227. [Google Scholar] [CrossRef] [PubMed]
- Bubendorf, L.; Zoche, M.; Dafni, U.; Rüschoff, J.H.; Prince, S.S.; Marti, N.; Stavrou, A.; Kammler, R.; Finn, S.P.; Moch, H.; et al. Prognostic impact of tumour mutational burden in resected stage I and II lung adenocarcinomas from a European Thoracic Oncology Platform Lungscape cohort. Lung Cancer 2022, 174, 27–35. [Google Scholar] [CrossRef]
- He, Y.; Zhang, X.; Jia, K.; Dziadziuszko, R.; Zhao, S.; Deng, J.; Wang, H.; Hirsch, F.R.; Zhou, C. OX40 and OX40L protein expression of tumor infiltrating lymphocytes in non-small cell lung cancer and its role in clinical outcome and relationships with other immune biomarkers. Transl. Lung Cancer Res. 2019, 8, 352–366. [Google Scholar] [CrossRef]
- Massarelli, E.; Lam, V.K.; Parra, E.R.; Rodriguez-Canales, J.; Behrens, C.; Diao, L.; Wang, J.; Blando, J.; Byers, L.A.; Yanamandra, N.; et al. High OX-40 expression in the tumor immune infiltrate is a favorable prognostic factor of overall survival in non-small cell lung cancer. J. Immunother. Cancer 2019, 7, 351. [Google Scholar] [CrossRef]
- Gross, D.J.; Chintala, N.K.; Vaghjiani, R.G.; Grosser, R.; Tan, K.S.; Li, X.; Choe, J.; Li, Y.; Aly, R.G.; Emoto, K.; et al. Tumor and Tumor-Associated Macrophage Programmed Death-Ligand 1 Expression Is Associated with Adjuvant Chemotherapy Benefit in Lung Adenocarcinoma. J. Thorac. Oncol. 2022, 17, 89–102. [Google Scholar] [CrossRef]
- Felip, E.; Altorki, N.; Zhou, C.; Csőszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H.; et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB–IIIA non-small-cell lung cancer (IMpower010): A randomised, multicentre, open-label, phase 3 trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.R.; Brahmer, J.R.; Swanson, S.J.; et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef] [PubMed]
- Shu, C.A.; Gainor, J.F.; Awad, M.M.; Chiuzan, C.; Grigg, C.M.; Pabani, A.; Garofano, R.F.; Stoopler, M.B.; Cheng, S.K.; White, A.; et al. Neoadjuvant atezolizumab and chemotherapy in patients with resectable non-small-cell lung cancer: An open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Dandachi, N.; Tiran, V.; Lindenmann, J.; Brcic, L.; Fink-Neuboeck, N.; Kashofer, K.; Absenger, G.; Bezan, A.; Cote, R.J.; Datar, R.; et al. Frequency and clinical impact of preoperative circulating tumor cells in resectable non-metastatic lung adenocarcinomas. Lung Cancer 2017, 113, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Hofman, V.; Bonnetaud, C.; Ilie, M.I.; Vielh, P.; Vignaud, J.M.; Fléjou, J.F.; Lantuejoul, S.; Piaton, E.; Mourad, N.; Butori, C.; et al. Preoperative circulating tumor cell detection using the isolation by size of epithelial tumor cell method for patients with lung cancer is a new prognostic biomarker. Clin. Cancer Res. 2011, 17, 827–835. [Google Scholar] [CrossRef]
- Li, H.; Li, B.; Pan, Y.; Zhang, Y.; Xiang, J.; Zhang, Y.; Sun, Y.; Yu, X.; He, W.; Hu, H. Preoperative Folate Receptor-Positive Circulating Tumor Cell Level Is a Prognostic Factor of Long Term Outcome in Non-Small Cell Lung Cancer Patients. Front. Oncol. 2020, 10, 621435. [Google Scholar] [CrossRef]
- Manjunath, Y.; Upparahalli, S.V.; Avella, D.M.; Deroche, C.B.; Kimchi, E.T.; Staveley-O’Carroll, K.F.; Smith, C.J.; Li, G.; Kaifi, J.T. PD-L1 Expression with Epithelial Mesenchymal Transition of Circulating Tumor Cells Is Associated with Poor Survival in Curatively Resected Non-Small Cell Lung Cancer. Cancers 2019, 11, 806. [Google Scholar] [CrossRef]
- de Miguel-Pérez, D.; Bayarri-Lara, C.I.; Ortega, F.G.; Russo, A.; Rodriguez, M.J.M.; Alvarez-Cubero, M.J.; Serrano, E.M.; Lorente, J.A.; Rolfo, C.; Serrano, M.J. Post-Surgery Circulating Tumor Cells and AXL Overexpression as New Poor Prognostic Biomarkers in Resected Lung Adenocarcinoma. Cancers 2019, 11, 1750. [Google Scholar] [CrossRef]
- Yoon, S.O.; Kim, Y.T.; Jung, K.C.; Jeon, Y.K.; Kim, B.-H.; Kim, C.-W. TTF-1 mRNA-positive circulating tumor cells in the peripheral blood predict poor prognosis in surgically resected non-small cell lung cancer patients. Lung Cancer 2011, 71, 209–216. [Google Scholar] [CrossRef]
- Li, J.; Shi, S.-B.; Shi, W.-L.; Wang, Y.; Yu, L.-C.; Zhu, L.-R.; Ge, L.-P. LUNX mRNA-positive cells at different time points predict prognosis in patients with surgically resected nonsmall cell lung cancer. Transl. Res. J. Lab. Clin. Med. 2014, 163, 27–35. [Google Scholar] [CrossRef]
- Crosbie, P.A.J.; Shah, R.; Krysiak, P.; Zhou, C.; Morris, K.; Tugwood, J.; Booton, R.; Blackhall, F.; Dive, C. Circulating Tumor Cells Detected in the Tumor-Draining Pulmonary Vein Are Associated with Disease Recurrence after Surgical Resection of NSCLC. J. Thorac. Oncol. 2016, 11, 1793–1797. [Google Scholar] [CrossRef]
- Chemi, F.; Rothwell, D.G.; McGranahan, N.; Gulati, S.; Abbosh, C.; Pearce, S.P.; Zhou, C.; Wilson, G.A.; Jamal-Hanjani, M.; Birkbak, N.; et al. Pulmonary venous circulating tumor cell dissemination before tumor resection and disease relapse. Nat. Med. 2019, 25, 1534–1539. [Google Scholar] [CrossRef]
- Wankhede, D.; Grover, S.; Hofman, P. Circulating Tumor Cells as a Predictive Biomarker in Resectable Lung Cancer: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 6112. [Google Scholar] [CrossRef]
- Gauthier, I.; Ding, K.; Winton, T.; Shepherd, F.A.; Livingston, R.; Johnson, D.H.; Rigas, J.R.; Whitehead, M.; Graham, B.; Seymour, L. Impact of hemoglobin levels on outcomes of adjuvant chemotherapy in resected non-small cell lung cancer: The JBR.10 trial experience. Lung Cancer 2007, 55, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Sulibhavi, A.; Asokan, S.; Miller, M.I.; Moreira, P.; Daly, B.D.; Fernando, H.C.; Litle, V.R.; Suzuki, K. Peripheral Blood Lymphocytes and Platelets Are Prognostic in Surgical pT1 Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2020, 109, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Hou, C.; Jiang, F.; Ma, H.; Zhu, Q.; Wang, Z.; Zhao, B.; Xue, T.; Tan, S.; Yang, R.; Qian, Y.; et al. Prognostic role of preoperative platelet, fibrinogen, and D-dimer levels in patients with non-small cell lung cancer: A multicenter prospective study. Thorac. Cancer 2019, 10, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Carus, A.; Ladekarl, M.; Hager, H.; Pilegaard, H.; Nielsen, P.S.; Donskov, F. Tumor-associated neutrophils and macrophages in non-small cell lung cancer: No immediate impact on patient outcome. Lung Cancer 2013, 81, 130–137. [Google Scholar] [CrossRef]
- Kobayashi, N.; Usui, S.; Kikuchi, S.; Goto, Y.; Sakai, M.; Onizuka, M.; Sato, Y. Preoperative lymphocyte count is an independent prognostic factor in node-negative non-small cell lung cancer. Lung Cancer 2012, 75, 223–227. [Google Scholar] [CrossRef]
- Zhang, J.; Huang, S.-H.; Li, H.; Li, Y.; Chen, X.-L.; Zhang, W.-Q.; Chen, H.-G.; Gu, L.-J. Preoperative lymphocyte count is a favorable prognostic factor of disease-free survival in non-small-cell lung cancer. Med. Oncol. 2013, 30, 352. [Google Scholar] [CrossRef]
- Mitchell, K.G.; Diao, L.; Karpinets, T.; Negrao, M.V.; Tran, H.T.; Parra, E.R.; Corsini, E.M.; Reuben, A.; Federico, L.; Bernatchez, C.; et al. Neutrophil expansion defines an immunoinhibitory peripheral and intratumoral inflammatory milieu in resected non-small cell lung cancer: A descriptive analysis of a prospectively immunoprofiled cohort. J. Immunother. Cancer 2020, 8, e000405. [Google Scholar] [CrossRef]
- Manjunath, Y.; Mitchem, J.B.; Suvilesh, K.N.; Avella, D.M.; Kimchi, E.T.; Staveley-O’Carroll, K.F.; Deroche, C.B.; Pantel, K.; Li, G.; Kaifi, J.T. Circulating Giant Tumor-Macrophage Fusion Cells Are Independent Prognosticators in Patients With NSCLC. J. Thorac. Oncol. 2020, 15, 1460–1471. [Google Scholar] [CrossRef]
- Takahashi, Y.; Horio, H.; Hato, T.; Harada, M.; Matsutani, N.; Morita, S.; Kawamura, M. Prognostic Significance of Preoperative Neutrophil-Lymphocyte Ratios in Patients with Stage I Non-small Cell Lung Cancer After Complete Resection. Ann. Surg. Oncol. 2015, 22 (Suppl. S3), S1324–S1331. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qu, X.; Kam, N.-W.; Wang, K.; Shen, H.; Liu, Q.; Du, J. An inflammation-related nomogram for predicting the survival of patients with non-small cell lung cancer after pulmonary lobectomy. BMC Cancer 2018, 18, 692. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Jiang, Y.; Qu, X.; Shen, H.; Liu, Q.; Du, J. Evaluation of preoperative hematologic markers as prognostic factors and establishment of novel risk stratification in resected pN0 non-small-cell lung cancer. PLoS ONE 2014, 9, e111494. [Google Scholar] [CrossRef] [PubMed]
- Seitlinger, J.; Prieto, M.; Guerrera, F.; Streit, A.; Gauchotte, G.; Siat, J.; Falcoz, P.-E.; Massard, G.; Ferri, L.; Spicer, J.; et al. Neutrophil-to-lymphocyte ratio is correlated to driver gene mutations in surgically-resected non-small cell lung cancer and its post-operative evolution impacts outcomes. Clin. Lung Cancer 2022, 23, e29–e42. [Google Scholar] [CrossRef]
- Cao, W.; Yu, H.; Zhu, S.; Lei, X.; Li, T.; Ren, F.; Zhou, N.; Tang, Q.; Zu, L.; Xu, S. Clinical significance of preoperative neutrophil-lymphocyte ratio and platelet-lymphocyte ratio in the prognosis of resected early-stage patients with non-small cell lung cancer: A meta-analysis. Cancer Med. 2022, 12, 7065–7076. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Shen, H.; Wang, G.; Zhang, P.; Liu, Q.; Du, J. Prognostic significance of systemic inflammation-based lymphocyte- monocyte ratio in patients with lung cancer: Based on a large cohort study. PLoS ONE 2014, 9, e108062. [Google Scholar] [CrossRef]
- Yang, Z.; Li, S.; Zhao, L.; Lv, W.; Ju, J.; Zhang, W.; Li, J.; Che, G. Serum uric acid to lymphocyte ratio: A novel prognostic biomarker for surgically resected early-stage lung cancer. A propensity score matching analysis. Clin. Chim. Acta 2020, 503, 35–44. [Google Scholar] [CrossRef]
- Yan, X.; Li, G. Preoperative systemic immune-inflammation index predicts prognosis and guides clinical treatment in patients with non-small cell lung cancer. Biosci. Rep. 2020, 40, BSR20200352. [Google Scholar] [CrossRef]
- Chen, K.; Zhao, H.; Shi, Y.; Yang, F.; Wang, L.T.; Kang, G.; Nie, Y.; Wang, J. Perioperative Dynamic Changes in Circulating Tumor DNA in Patients with Lung Cancer (DYNAMIC). Clin. Cancer Res. 2019, 25, 7058–7067. [Google Scholar] [CrossRef]
- Waldeck, S.; Mitschke, J.; Wiesemann, S.; Rassner, M.; Andrieux, G.; Deuter, M.; Mutter, J.; Lüchtenborg, A.-M.; Kottmann, D.; Titze, L.; et al. Early assessment of circulating tumor DNA after curative-intent resection predicts tumor recurrence in early-stage and locally advanced non-small-cell lung cancer. Mol. Oncol. 2022, 16, 527–537. [Google Scholar] [CrossRef]
- Yang, W.; You, N.; Jia, M.; Yeung, S.-C.J.; Ou, W.; Yu, M.; Wang, Y.; Fu, X.; Zhang, Z.; Yang, J.; et al. Undetectable circulating tumor DNA levels correlate with low risk of recurrence/metastasis in postoperative pathologic stage I lung adenocarcinoma patients. Lung Cancer 2020, 146, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Qiu, B.; Guo, W.; Zhang, F.; Lv, F.; Ji, Y.; Peng, Y.; Chen, X.; Bao, H.; Xu, Y.; Shao, Y.; et al. Dynamic recurrence risk and adjuvant chemotherapy benefit prediction by ctDNA in resected NSCLC. Nat. Commun. 2021, 12, 6770. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Mei, J.; Kang, R.; Deng, S.; Chen, Y.; Yang, Y.; Feng, G.; Deng, Y.; Gan, F.; Lin, Y.; et al. Perioperative ctDNA-Based Molecular Residual Disease Detection for Non-Small Cell Lung Cancer: A Prospective Multicenter Cohort Study (LUNGCA-1). Clin. Cancer Res. 2022, 28, 3308–3317. [Google Scholar] [CrossRef]
- Li, N.; Wang, B.-X.; Li, J.; Shao, Y.; Li, M.-T.; Li, J.-J.; Kuang, P.-P.; Liu, Z.; Sun, T.-Y.; Wu, H.-Q.; et al. Perioperative circulating tumor DNA as a potential prognostic marker for operable stage I to IIIA non-small cell lung cancer. Cancer 2022, 128, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Gale, D.; Heider, K.; Ruiz-Valdepenas, A.; Hackinger, S.; Perry, M.; Marsico, G.; Rundell, V.; Wulff, J.; Sharma, G.; Knock, H.; et al. Residual ctDNA after treatment predicts early relapse in patients with early-stage non-small cell lung cancer. Ann. Oncol. 2022, 33, 500–510. [Google Scholar] [CrossRef]
- Hu, Z.; Chen, X.; Zhao, Y.; Tian, T.; Jin, G.; Shu, Y.; Chen, Y.; Xu, L.; Zen, K.; Zhang, C.; et al. Serum microRNA signatures identified in a genome-wide serum microRNA expression profiling predict survival of non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 1721–1726. [Google Scholar] [CrossRef]
- Heegaard, N.H.H.; Schetter, A.J.; Welsh, J.A.; Yoneda, M.; Bowman, E.D.; Harris, C.C. Circulating micro-RNA expression profiles in early stage nonsmall cell lung cancer. Int. J. Cancer 2012, 130, 1378–1386. [Google Scholar] [CrossRef]
- Kanaoka, R.; Iinuma, H.; Dejima, H.; Sakai, T.; Uehara, H.; Matsutani, N.; Kawamura, M. Usefulness of Plasma Exosomal MicroRNA-451a as a Noninvasive Biomarker for Early Prediction of Recurrence and Prognosis of Non-Small Cell Lung Cancer. Oncology 2018, 94, 311–323. [Google Scholar] [CrossRef]
- Han, B.; Molins, L.; He, Y.; Viñolas, N.; Sánchez-Lorente, D.; Boada, M.; Guirao, A.; Díaz, T.; Martinez, D.; Ramirez, J.; et al. Characterization of the MicroRNA Cargo of Extracellular Vesicles Isolated from a Pulmonary Tumor-Draining Vein Identifies miR-203a-3p as a Relapse Biomarker for Resected Non-Small Cell Lung Cancer. Int. J. Mol. Sci. 2022, 23, 7138. [Google Scholar] [CrossRef]
- Sawabata, N.; Ohta, M.; Takeda, S.-I.; Hirano, H.; Okumura, Y.; Asada, H.; Maeda, H. Serum carcinoembryonic antigen level in surgically resected clinical stage I patients with non-small cell lung cancer. Ann. Thorac. Surg. 2002, 74, 174–179. [Google Scholar] [CrossRef]
- Okada, M.; Sakamoto, T.; Nishio, W.; Uchino, K.; Tsubota, N. Characteristics and prognosis of patients after resection of nonsmall cell lung carcinoma measuring 2 cm or less in greatest dimension. Cancer 2003, 98, 535–541. [Google Scholar] [CrossRef]
- Sakao, Y.; Nakazono, T.; Sakuragi, T.; Natsuaki, M.; Itoh, T. Predictive factors for survival in surgically resected clinical IA peripheral adenocarcinoma of the lung. Ann. Thorac. Surg. 2004, 77, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Fukai, R.; Sakao, Y.; Sakuraba, M.; Oh, S.; Shiomi, K.; Sonobe, S.; Saitoh, Y.; Miyamoto, H. The prognostic value of carcinoembryonic antigen in T1N1M0 and T2N1M0 non-small cell carcinoma of the lung. Eur. J. Cardio-Thorac. Surg. 2007, 32, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Higashi, K.; Sakuma, T.; Ito, K.; Niho, S.; Ueda, Y.; Kobayashi, T.; Sekiguchi, R.; Takahashi, T.; Kato, T.; Tonami, H. Combined evaluation of preoperative FDG uptake on PET, ground-glass opacity area on CT, and serum CEA level: Identification of both low and high risk of recurrence in patients with resected T1 lung adenocarcinoma. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Hanagiri, T.; Sugaya, M.; Takenaka, M.; Oka, S.; Baba, T.; Shigematsu, Y.; Nagata, Y.; Shimokawa, H.; Uramoto, H.; Takenoyama, M.; et al. Preoperative CYFRA 21-1 and CEA as prognostic factors in patients with stage I non-small cell lung cancer. Lung Cancer 2011, 74, 112–117. [Google Scholar] [CrossRef]
- Kozu, Y.; Maniwa, T.; Takahashi, S.; Isaka, M.; Ohde, Y.; Nakajima, T. Risk factors for both recurrence and survival in patients with pathological stage I non-small-cell lung cancer. Eur. J. Cardio-Thorac. Surg. 2013, 44, e53–e58. [Google Scholar] [CrossRef]
- Kuo, S.-W.; Chen, J.-S.; Huang, P.-M.; Hsu, H.-H.; Lai, H.-S.; Lee, J.-M. Prognostic significance of histologic differentiation, carcinoembryonic antigen value, and lymphovascular invasion in stage I non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2014, 148, 1200–1207.e3. [Google Scholar] [CrossRef]
- Hashinokuchi, A.; Haratake, N.; Takenaka, T.; Matsudo, K.; Nagano, T.; Watanabe, K.; Kosai, K.; Oku, Y.; Ono, Y.; Takamori, S.; et al. Clinical significance of the combination of preoperative SUVmax and CEA in patients with clinical stage IA lung adenocarcinoma. Thorac. Cancer 2022, 13, 2624–2632. [Google Scholar] [CrossRef]
- Sawabata, N.; Maeda, H.; Yokota, S.; Takeda, S.-I.; Koma, M.; Tokunaga, T.; Ito, M. Postoperative serum carcinoembryonic antigen levels in patients with pathologic stage IA nonsmall cell lung carcinoma: Subnormal levels as an indicator of favorable prognosis. Cancer 2004, 101, 803–809. [Google Scholar] [CrossRef]
- Yamazaki, M.; Ishikawa, H.; Kunii, R.; Tasaki, A.; Sato, S.; Ikeda, Y.; Yoshimura, N.; Hashimoto, T.; Tsuchida, M.; Aoyama, H. A combination of preoperative CT findings and postoperative serum CEA levels improves recurrence prediction for stage I lung adenocarcinoma. Eur. J. Radiol. 2015, 84, 178–184. [Google Scholar] [CrossRef]
- Wang, Y.; Zheng, D.; Chen, T.; Zhang, J.; Yao, F.; Chen, H. Survival Prediction and Adjuvant Chemotherapy Based on Tumor Marker for Stage IB Lung Adenocarcinoma. Ann. Thorac. Surg. 2020, 109, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Kashiwabara, K.; Saeki, S.; Sasaki, J.-I.; Nomura, M.; Kohrogi, H. Combined evaluation of postoperative serum levels of carcinoembryonic antigen less than or equal to 2.5 ng/mL and absence of vascular invasion may predict no recurrence of stage I adenocarcinoma lung cancer. J. Thorac. Oncol. 2008, 3, 1416–1420. [Google Scholar] [CrossRef] [PubMed]
- Reinmuth, N.; Brandt, B.; Semik, M.; Kunze, W.-P.; Achatzy, R.; Scheld, H.H.; Broermann, P.; Berdel, W.E.; Macha, H.N.; Thomas, M. Prognostic impact of Cyfra21-1 and other serum markers in completely resected non-small cell lung cancer. Lung Cancer 2002, 36, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Lee, J.G.; Kim, J.; Park, Y.; Lee, S.K.; Bae, M.K.; Lee, C.Y.; Kim, D.J.; Chung, K.Y. Preoperative serum CYFRA 21-1 level as a prognostic factor in surgically treated adenocarcinoma of lung. Lung Cancer 2013, 79, 156–160. [Google Scholar] [CrossRef]
- Mizuguchi, S.; Nishiyama, N.; Iwata, T.; Nishida, T.; Izumi, N.; Tsukioka, T.; Inoue, K.; Uenishi, T.; Wakasa, K.; Suehiro, S. Serum Sialyl Lewis x and cytokeratin 19 fragment as predictive factors for recurrence in patients with stage I non-small cell lung cancer. Lung Cancer 2007, 58, 369–375. [Google Scholar] [CrossRef]
- Muley, T.; Fetz, T.-H.; Dienemann, H.; Hoffmann, H.; Herth, F.J.F.; Meister, M.; Ebert, W. Tumor volume and tumor marker index based on CYFRA 21-1 and CEA are strong prognostic factors in operated early stage NSCLC. Lung Cancer 2008, 60, 408–415. [Google Scholar] [CrossRef]
- Ma, S.; Shen, L.; Qian, N.; Chen, K. The prognostic values of CA125, CA19.9, NSE, AND SCC for stage I NSCLC are limited. Cancer Biomark. 2011, 10, 155–162. [Google Scholar] [CrossRef]
- Yu, D.; Du, K.; Liu, T.; Chen, G. Prognostic value of tumor markers, NSE, CA125 and SCC, in operable NSCLC Patients. Int. J. Mol. Sci. 2013, 14, 11145–11156. [Google Scholar] [CrossRef]
- Isaksson, S.; George, A.M.; Jönsson, M.; Cirenajwis, H.; Jönsson, P.; Bendahl, P.-O.; Brunnström, H.; Staaf, J.; Saal, L.H.; Planck, M. Pre-operative plasma cell-free circulating tumor DNA and serum protein tumor markers as predictors of lung adenocarcinoma recurrence. Acta Oncol. 2019, 58, 1079–1086. [Google Scholar] [CrossRef]
- O’Dowd, C.; McRae, L.A.; McMillan, D.C.; Kirk, A.; Milroy, R. Elevated preoperative C-reactive protein predicts poor cancer specific survival in patients undergoing resection for non-small cell lung cancer. J. Thorac. Oncol. 2010, 5, 988–992. [Google Scholar] [CrossRef]
- Alifano, M.; Falcoz, P.E.; Seegers, V.; Roche, N.; Schussler, O.; Younes, M.; Antonacci, F.; Forgez, P.; Dechartres, A.; Massard, G.; et al. Preresection serum C-reactive protein measurement and survival among patients with resectable non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2011, 142, 1161–1167. [Google Scholar] [CrossRef]
- Sheng, L.; Luo, M.; Sun, X.; Lin, N.; Mao, W.; Su, D. Serum fibrinogen is an independent prognostic factor in operable nonsmall cell lung cancer. Int. J. Cancer 2013, 133, 2720–2725. [Google Scholar] [CrossRef]
- Zhang, P.P.; Sun, J.W.; Wang, X.Y.; Liu, X.M.; Li, K. Preoperative plasma D-dimer levels predict survival in patients with operable non-small cell lung cancer independently of venous thromboembolism. Eur. J. Surg. Oncol. 2013, 39, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.-G.; Li, J.; Shi, S.-B.; Chen, P.; Ge, L.-P.; Jiang, Q.; Tang, X.-P. Value of fibrinogen and D-dimer in predicting recurrence and metastasis after radical surgery for non-small cell lung cancer. Med. Oncol. 2014, 31, 22. [Google Scholar] [CrossRef] [PubMed]
- Kawai, H.; Ota, H. Low perioperative serum prealbumin predicts early recurrence after curative pulmonary resection for non-small-cell lung cancer. World J. Surg. 2012, 36, 2853–2857. [Google Scholar] [CrossRef]
- Okada, S.; Shimada, J.; Kato, D.; Tsunezuka, H.; Teramukai, S.; Inoue, M. Clinical Significance of Prognostic Nutritional Index After Surgical Treatment in Lung Cancer. Ann. Thorac. Surg. 2017, 104, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, Y.; Safi, S.; Muley, T.; Warth, A.; Herth, F.J.F.; Dienemann, H.; Hoffmann, H.; Eichhorn, M.E. C-reactive protein-albumin ratio is an independent prognostic predictor of tumor recurrence in stage IIIA-N2 lung adenocarcinoma patients. Lung Cancer 2017, 114, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Qin, S.; Sun, X.; Liu, D.; Zhang, B.; Xiao, G.; Ren, H. Prognostic Significance of Albumin-Globulin Score in Patients with Operable Non-Small-Cell Lung Cancer. Ann. Surg. Oncol. 2018, 25, 3647–3659. [Google Scholar] [CrossRef]
- Guo, X.; Shao, J.; Zhai, B.; Zou, Q.; Yan, J.; Gu, H.; Wang, G. Relationship and prognostic significance between preoperative serum albumin to globulin ratio and CT features of non-small cell lung cancer. Eur. J. Radiol. 2020, 128, 109039. [Google Scholar] [CrossRef]
- Takenaka, M.; Hanagiri, T.; Shinohara, S.; Yasuda, M.; Chikaishi, Y.; Oka, S.; Shimokawa, H.; Nagata, Y.; Nakagawa, M.; Uramoto, H.; et al. Serum level of osteopontin as a prognostic factor in patients who underwent surgical resection for non-small-cell lung cancer. Clin. Lung Cancer 2013, 14, 288–294. [Google Scholar] [CrossRef]
- Rud, A.K.; Boye, K.; Oijordsbakken, M.; Lund-Iversen, M.; Halvorsen, A.R.; Solberg, S.K.; Berge, G.; Helland, A.; Brustugun, O.T.; Mælandsmo, G.M. Osteopontin is a prognostic biomarker in non-small cell lung cancer. BMC Cancer 2013, 13, 540. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating tumor cells: Biology and clinical significance. Signal Transduct. Target Ther. 2021, 6, 404. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Guo, C.; He, J.; Tan, Q.; Mei, J.; Yang, Z.; Liu, C.; Pu, Q.; Ma, L.; Yuan, Y.; et al. Effect of Vein-First vs Artery-First Surgical Technique on Circulating Tumor Cells and Survival in Patients with Non-Small Cell Lung Cancer: A Randomized Clinical Trial and Registry-Based Propensity Score Matching Analysis. JAMA Surg. 2019, 154, e190972. [Google Scholar] [CrossRef] [PubMed]
- Szilágyi, M.; Pös, O.; Márton, É.; Buglyó, G.; Soltész, B.; Keserű, J.; Penyige, A.; Szemes, T.; Nagy, B. Circulating Cell-Free Nucleic Acids: Main Characteristics and Clinical Application. Int. J. Mol. Sci. 2020, 21, 6827. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yu, H.; Gan, Y.; Wu, Z.; Li, E.; Li, X.; Cao, J.; Zhu, Y.; Wang, L.; Deng, H.; et al. Mining whole-lung information by artificial intelligence for predicting EGFR genotype and targeted therapy response in lung cancer: A multicohort study. Lancet Digit. Health 2022, 4, e309–e319. [Google Scholar] [CrossRef]
- Kawakami, E.; Tabata, J.; Yanaihara, N.; Ishikawa, T.; Koseki, K.; Iida, Y.; Saito, M.; Komazaki, H.; Shapiro, J.S.; Goto, C.; et al. Application of Artificial Intelligence for Preoperative Diagnostic and Prognostic Prediction in Epithelial Ovarian Cancer Based on Blood Biomarkers. Clin. Cancer Res. 2019, 25, 3006–3015. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of constructing prognostic models by applying AI. AI, artificial intelligence.
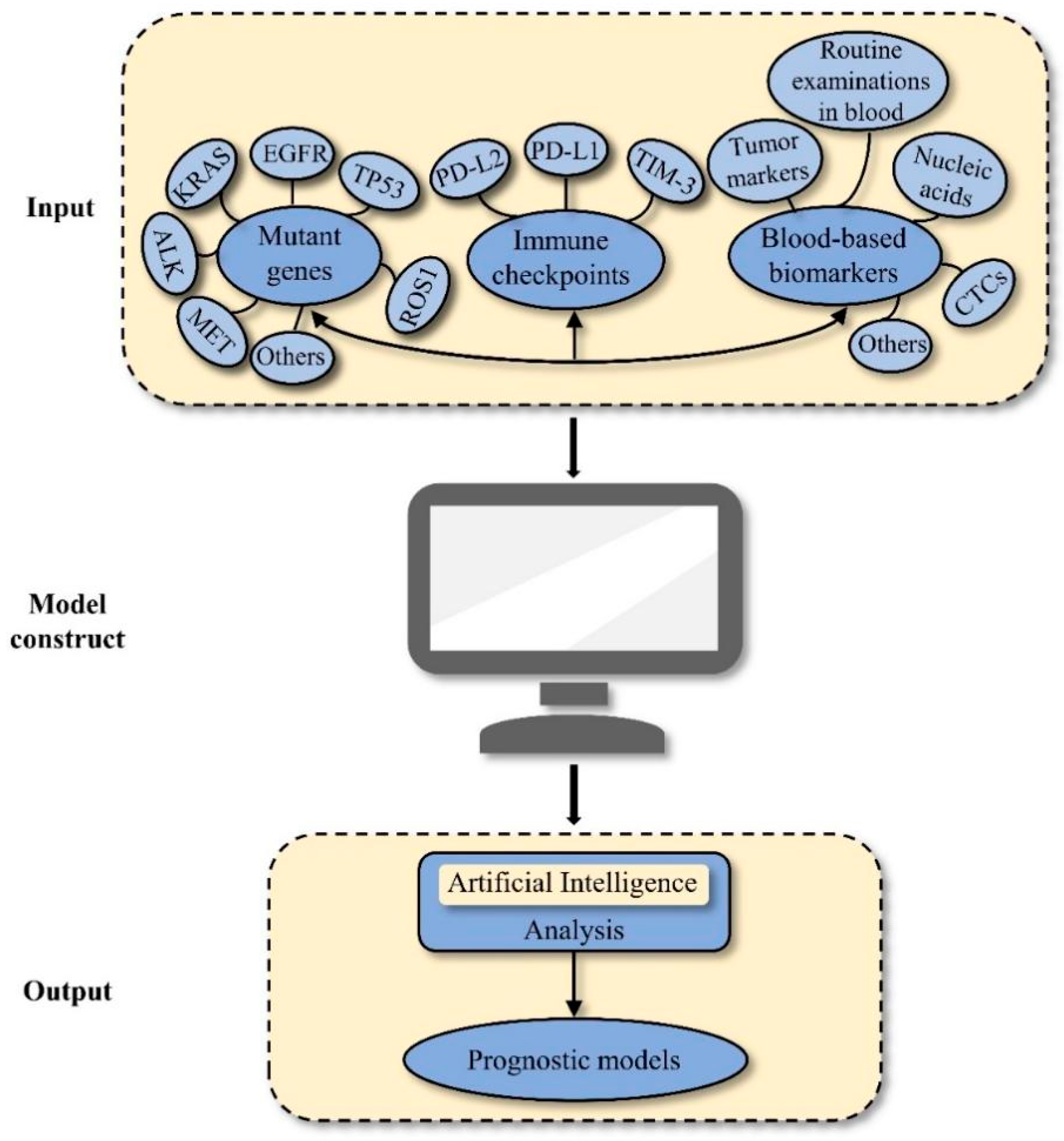

{kind=link}
Table 1.
Summary of studies relating to genetic alterations in resected early-stage NSCLC.
| Mutant Genes | Ref. (NOP) | Study Design | Histology | Phase | Ethnicity | Median Follow-Up (Months) | Percentage of Genetic Alterations | Prognostic Implication |
|---|---|---|---|---|---|---|---|---|
| EGFR | ||||||||
| EGFR alterations | [9] (374) | RCT | Ns-NSCLC | II–IIIA | Japanese | NA | 37.2% | Worse RFS |
| EGFR alterations | [10] (1512) | R | LUAD | I–III | Chinese | 53.2 | 61.8% | Worse RFS |
| EGFR alterations | [11] (1155) | R | LUAD | I–IIIA (N0-1) | Japanese | 36 | 50.6% | Worse RFS |
| EGFR amplification | [12] (637) | P | LUAD | I–IIIA (≤3 cm) | Chinese | 30.57 | 5.8% | Worse RFS |
| EGFR amplification | [13] (109) | R | NSCLC | I–III | Japanese | NA | 5.5% | Worse OS |
| EGFR alterations | [14] (237) | P | LUAD | I–III | Japanese | NA | 45.5% | Improved RFS |
| EGFR alterations | [15] (307) | R | NSCLC | I | American | 30 | 20.2% | Improved DFS and OS |
| EGFR alterations | [16] (164) | R | NSCLC | I–IIIA | Chinese | NA | 31.7% | Improved OS |
| EGFR alterations | [17] (1231) | R | NSCLC | I | Japanese | 36 | 44.3% | IA: No impact on survival; IB: Improved DSS and OS |
| EGFR exons 18-19 | [18] (133) | P | NSCLC | I–III | Korean | 29 | 7.5% | Improved OS |
| EGFR exon 19 | [19] (276) | R | LUAD | I–III | French/Italian | 46 | 55.1% | Stage I: No impact on OS; Stage II/III: Improved OS |
| EGFR exon 19 | [20] (202) | R | LUAD | II–IIIA (N1-2) | Japanese | NA | 27.2% | Improved DFS and OS |
| EGFR exon 19 | [21] (835) | R | LUAD | I–III | Japanese | 47 | 21% | Worse RFS |
| EGFR T790M | [22] (373) | P | NSCLC | I–IIIB | Japanese | 48.6 | 79.9% | Worse RFS and OS |
| Phosphorylated EGFR | [23] (49) | P | NSCLC | I | Austrian | 29.3 | NA | Worse survival |
| KRAS | ||||||||
| KRAS G12C | [24] (604) | P | LUAD | I–III | American | 30.1 | 16% | Worse DFS |
| KRAS alterations | [25] (1118) | R | LUAD | I–III | American | 27 | 25% | No impact on OS |
| KRAS alterations | [26] (312) | R | LUAD | I | American | 36 | 41% | Worse DFS and OS |
| KRAS alterations | [27] (482) | R | LUAD | I–II | American | 56.8 | 27% | Worse OS |
| KRAS alterations | [28] (324) | R | LUAD | I–III | American | 33.67 | 38.1% | Worse DFS and OS |
| KRAS alterations | [16] (164) | R | NSCLC | I–IIIA | Chinese | NA | 4.3% | Worse OS |
| KRAS alterations | [29] (216) | R | NSCLC | I–IIIA | Spanish | 14.25 | 13.4% | Improved DSS |
| ALK | ||||||||
| ALK rearrangement | [30] (124) | R | LUAD | I | Japanese | NA | 19.4% | Worse RFS; No impact on OS |
| ALK rearrangement | [31] (764) | R | NSCLC | I–III | American | 60.5 | 4% | Worse RFS; No impact on OS |
| ALK rearrangement | [32] (1925) | R | LUAD | I–IIIB | Japanese | 72 | 3.9% | Improved CSS and OS |
| EML4-ALK fusion variant 3 | [33] (55) | R | NSCLC | I–III | Chinese | 34.8 | 34.6% | Worse DFS |
| ALK rearrangement | [34] (231) | R | LUAD | I–IIIB | Korean | 26 | 9% | No impact on DFS and OS |
| ALK rearrangement | [35] (735) | R | NSCLC | I–III | Korean | 45 | 3.8% | No impact on DFS and OS |
| MET | ||||||||
| MET alterations | [36] (311) | R | LUAD | IB–IIIA | Korean | 22.8 | 45.3% | Worse RFS and OS in EGFRmut (-) group |
| MET alterations | [37] (265) | R | NSCLC | I–II | Italian | 40 | NA | Worse OS |
| MET amplification | [38] (1540) | R | NSCLC | I–III | International | 57.3 | 22.8% | No impact on OS |
| METex14 skipping | [39] (795) | R | LUAD | I–III | Korean | NA | 2.1% | No impact on OS |
| ROS1 | ||||||||
| ROS1 fusion | [40] (230) | R | LUAD | I–II | Korean | 49 | NA | Worse RFS |
| ROS1 fusion | [41] (160) | P | LUAD | I–IIIA | Chinese | 50.1 | 3.1% | No impact on OS |
| TP53 | ||||||||
| TP53 alterations | [12] (637) | P | LUAD | I–IIIA (≤3 cm) | Chinese | 30.57 | 28.1% | Worse RFS |
| TP53 alterations | [40] (230) | R | LUAD | I–II | Korean | 49 | 18.3% | Worse RFS |
| TP53 alterations | [42] (214) | R | NSCLC | I–III | Canadian | 54 | 50% | Worse DFS and OS |
| TP53 alterations | [43] (50) | R | NSCLC | IA | American | NA | NA | LUAD: Worse OS; No impact on DFS; LUSC: No effect on DFS and OS |
| p53 pathway alterations | [44] (492) | P | LUAD | I–III | American | 19 | NA | Worse DFS |
| p53 alterations | [45] (76) | P | NSCLC | I–IIIB | Italian | 23 | 54% | Worse DFS |
| p53 alterations | [46] (102) | P | NSCLC | I–IIIA | Polish | 28 | NA | Worse OS |
| Others | ||||||||
| RET fusion | [40] (230) | R | LUAD | I–II | Korean | 49 | NA | Worse RFS |
| BRAF alterations | [28] (324) | R | LUAD | I–III | American | 33.67 | 5.9% | Worse DFS and OS |
| PIK3CA alterations | [47] (308) | P | LUSC | I–III | Norwegian | 67.6 | 11.4% | Improved OS and TTR |
| PIK3CA alterations | [48] (810) | R | LUAD | I–IIIA | Chinese | NA | 2.8% | Worse OS |
| PIK3CA alterations | [49] (167) | R | NSCLC | I | Italian | 120 | 3.6% | Worse survival |
| TTF-1 amplification | [50] (118) | R | LUAD | I–III | Korean | NA | 12.7% | Worse DFS and OS |
| PKD and TP53 co-alterations | [51] (147) | P | LUAD | I–III | Chinese | 31.3 | 7% | Worse DFS; No impact on OS |
Abbreviations: EGFR, epidermal growth factor receptor; KRAS, Kirsten rat sarcoma viral oncogene homologue; ALK, anaplastic lymphoma kinase; MET, mesenchymal-epithelial transition; METex14, MET exon 14; ROS1, C-ros oncogene 1; TP53, tumour protein p53; RET, rearranged during transfection; BRAF, V-RAF murine sarcoma viral oncogene homolog B1; TTF-1, thyroid transcription factor-1; PKD, protein kinase D; Ref, reference; NOP, number of the population; RCT, randomised controlled trial; R, retrospective study; P, prospective study; NSCLC, non-small-cell lung cancer; Ns-NSCLC, nonsquamous non-small-cell lung cancer; LUAD, lung adenocarcinoma; LUSC, lung squamous cell carcinoma; NA, not available; DFS, disease-free survival; RFS, relapse-free survival; OS, overall survival; DSS, disease-specific survival; R, retrospective study; P, prospective study; Meta, meta-analysis; TTR, time to recurrence.
Table 2.
Summary of studies relating to immune-related indicators in resected early-stage NSCLC.
| Immune-Related Indicators | Ref. (NOP) | Study Design | Histology | Phase | Ethnicity | Median Follow-Up (Months) | Percentage of Indicators Overexpression | Prognostic Implication |
|---|---|---|---|---|---|---|---|---|
| PD-L1 | [70] (316) | R | LUAD | I–III | Korean | NA | 18.6% | Worse RFS and OS |
| PD-L1 | [71] (193) | R | LUAD | I–III | Korean | NA | 21.2% | Worse RFS and OS |
| PD-L1; PD-L2 | [72] (433) | R | LUAD | I–III | Japanese | NA | NA | Worse DFS and OS |
| PD-L1 | [73] (417) | R | LUAD | I–III | Japanese | NA | 34.5% | Worse DFS and OS |
| PD-L1 | [74] (205) | R | LUSC | I–III | Japanese | NA | 51.7% | Worse OS |
| PD-L1 | [75] (164) | R | NSCLC | I–IIIB | Japanese | 55.6 | 50% | Worse OS |
| PD-L1 | [76] (455) | R | NSCLC | I–IIIA | Asian | 47 | NA | Worse DFS and OS |
| PD-L1 | [77] (136) | R | NSCLC | I–III | Korean | 84 | 25.7% | Worse RFS and OS |
| PD-L1 | [78] (126) | R | NSCLC | I | Japanese | 47.5 | 18.3% | CD8-high cohort: No impact on RFS; CD8-low cohort: Worse RFS |
| PD-L1 | [79] (163) | R | LUAD | I | Chinese | 71 | 39.9% | Improved RFS; No impact on OS |
| PD-L1 | [80] (678) | R | NSCLC | I–III | Australian | NA | 7.4% | Improved OS |
| PD-L1 | [81] (228) | R | NSCLC | I–IIIA | Japanese | NA | 24.1% | Stage I: Improved RFS; Stage II–IIIA: Worse RFS |
| PD-L1 | [82] (386) | R | LUAD | I–III | Chinese | 54 | 48.3% | No impact on DFS and OS |
| PD-L1 | [83] (3790) | Meta | NSCLC | I–III | International | NA | NA | Worse DFS and OS |
| TIM-3 | [84] (223) | R | LUAD | I–III | Chinese | NA | 48% | Worse RFS and OS |
| TMB | [85] (92) | R | NSCLC | I–III | Canadian | NA | NA | Worse OS |
| TMB | [86] (78) | R | LUAD | I–II | Caucasian | 56.1 | NA | No impact on RFS and OS |
| OX40 | [87] (139) | R | NSCLC | I | Polish | NA | NA | Worse RFS and OS |
| OX40 | [88] (100) | R | NSCLC | I–III | American | NA | NA | Improved OS |
Abbreviations: PD-L1, programmed death-ligand 1; PD-L2, programmed death-ligand 2; TIM-3, T-cell immunoglobulin and mucin-domain-containing-3; TMB, tumour mutation burden; Ref, reference; NOP, number of the population; R, retrospective study; P, prospective study; Meta, meta-analysis; NSCLC, non-small-cell lung cancer; LUAD, lung adenocarcinoma; LUSC, lung squamous cell carcinoma; NA, not available; DFS, disease-free survival; RFS, relapse-free survival; OS, overall survival.
Table 3.
Summary of studies relating to blood-based biomarkers in resected early-stage NSCLC.
| Blood-Based Biomarkers | Ref. (NOP) | Study Design | Histology | Phase | Ethnicity | Median Follow-Up (Months) | Prognostic Implications |
|---|---|---|---|---|---|---|---|
| CTCs | |||||||
| CTCs | [93] (40) | P | LUAD | I–IIIA | Austrian | 16 | Worse DFS |
| CTCs | [94] (137) | P | NSCLC | I–II | French | NA | Worse DFS and OS |
| FR+ CTCs | [95] (52) | P | NSCLC | I–III | Chinese | NA | Worse RFS and OS |
| PD-L1+/EMT+ CTCs | [96] (30) | P | NSCLC | I–IIIA | American | 14.3 | Worse RFS and OS |
| CTCs | [97] (97) | P | NSCLC | I–III | Spanish | LAUD: 30.5; LUSC: 32 | LUAD: Worse RFS and OS; LUSC: No impact on survival |
| TTF-1+ CTCs | [98] (79) | P | NSCLC | I–III | Korean | NA | Worse PFS |
| LUNX+ CTCS | [99] (68) | P | NSCLC | I–IIIA | Chinese | 39.5 | Worse DFS and OS |
| CTCs | [100] (30) | P | NSCLC | I–III | British | 22 | Worse DFS and OS |
| CTCs | [101] (100) | P | NSCLC | I–III | British | 33.1 | Worse DFS |
| CTCs | [102] (1321) | Meta | NSCLC | I–IIIA | International | Range: 13–84 | Worse DFS and OS |
| Routine examinations of blood | |||||||
| Hb | [103] (482) | R | NSCLC | IB–II | Canadian | NA | Baseline Hb: Worse OS; During-treatment Hb: Improved RFS and OS |
| PLT; Lymphocyte | [104] (103) | R | NSCLC | I | American | 42 | Worse RFS |
| PLT | [105] (395) | P | NSCLC | I–III | Chinese | 13.2 | Worse PFS |
| White blood cells | [106] (335) | P | NSCLC | I–IIIA | Danish | NA | Worse RFS and OS |
| Lymphocyte; Neutrophil | [107] (237) | R | NSCLC | I–III | Japanese | NA | Lymphocyte: Improved OS; Neutrophil: No impact on OS |
| Lymphocyte; Neutrophil | [108] (142) | R | NSCLC | IB–IIIA | Chinese | NA | Lymphocyte: Improved DFS/No impact on OS; Neutrophil: No impact on survival |
| Neutrophil; Lymphocyte | [109] (1524) | P | NSCLC | I–IIIA | American | 60.7 | Neutrophil: Worse OS; Lymphocyte: No impact on OS |
| TMFs | [110] (115) | P | NSCLC | I–IIIA | Colombian | 26.6 | Worse DFS and OS |
| NLR | [111] (343) | R | NSCLC | I | Japanese | 73.5 | Worse RFS and OS |
| NLR | [112] (952) | R | NSCLC | I–III | Chinese | 40 | Worse OS |
| NLR; PLR | [113] (400) | R | NSCLC | I–II (N0) | Chinese | 46 | NLR: Worse DFS and OS; PLR: No impact on survival |
| NLR | [114] (2027) | R | NSCLC | I–III | French | 69 | Worse OS and TTR |
| NLR; PLR | [115] (14,242) | Meta | NSCLC | I–III | International | NA | Worse DFS and OS |
| LMR | [116] (1453) | R | NSCLC | I–III | Chinese | NA | Improved DFS and OS |
| ULR | [117] (335) | P | NSCLC | I–II | Chinese | 51 | Worse DFS and OS |
| SII | [118] (538) | R | NSCLC | I–IIIA | Chinese | 54 | Worse DFS and OS |
| Circulating nucleic acids | |||||||
| ctDNA | [119] (205) | P | NSCLC | I–IIIA | Chinese | 17.6 | Worse RFS and OS |
| ctDNA | [120] (33) | P | NSCLC | I–IIIB | German | 26.2 | Worse PFS and OS |
| ctDNA | [121] (82) | P | LUAD | I | Chinese | 22.83 | Worse DFS |
| ctDNA | [122] (89) | P | LUAD | IIB–IIIA | Chinese | NA | Worse RFS |
| ctDNA | [123] (330) | P | NSCLC | I–III | Chinese | 35.6 | Worse RFS |
| ctDNA | [124] (119) | P | NSCLC | I–IIIA | Chinese | 30.7 | Worse RFS and OS |
| ctDNA | [125] (88) | P | NSCLC | I–III | British | 36 | Worse RFS and OS |
| Four-miRNA signature (miR-486 and miR-30d, miR-1, miR-499) | [126] (303) | R | NSCLC | I–IIIA | Chinese | NA | High miR-486 and miR-30d; Low miR-1 and miR-499: Worse OS |
| MiR-let-7b | [127] (220) | R | NSCLC | I–II | American | NA | Improved CSS |
| MiR-451a | [128] (285) | R | NSCLC | I–III | Japanese | 24 | Worse DFS and OS |
| MiR-203a-3p | [129] (88) | R | NSCLC | I–III | Spanish | Screening/Validation cohort: 66.07/54.23 | Worse TTR |
| Tumour markers | |||||||
| CEA | [130] (253) | R | NSCLC | I–II | Japanese | NA | Worse OS |
| CEA | [131] (265) | R | NSCLC | I–IIIB | Japanese | 43 | Worse DSS and OS |
| CEA | [132] (65) | R | LUAD | IA | Japanese | NA | Worse DFS and OS |
| CEA | [133] (45) | R | NSCLC | T1-2N1M0 | Japanese | 39.8 | Worse OS |
| CEA | [134] (87) | R | LUAD | I–IIIB (≤3 cm) | Japanese | NA | Worse DFS |
| CEA; CYFRA 21-1 | [135] (341) | R | NSCLC | I | Japanese | NA | Worse OS |
| CEA; CYFRA 21-1 | [136] (467) | R | NSCLC | I | Japanese | 54 | CEA: Worse DFS and OS; CYFRA 21-1: No impact on survival |
| CEA | [137] (758) | R | NSCLC | I | Chinese | NA | Worse PFS |
| Combination of SUVmax and CEA | [138] (410) | R | LUAD | IA | Japanese | NA | Worse RFS and OS |
| CEA | [139] (242) | R | NSCLC | IA | Japanese | 64 | Worse survival |
| CEA | [140] (250) | R | LUAD | I | Japanese | 73.2 | Worse DFS |
| CEA | [141] (600) | R | LUAD | IB | Chinese | 46.7 | Worse RFS and OS |
| CEA | [142] (136) | R | LUAD | I | Japanese | 28.3 | Worse RFS |
| CYFRA 21-1; NSE; SCC-Ag | [143] (67) | P | NSCLC | I–IIIA | German | 86 | CYFRA 21-1: Worse DFS and OS; NSE; SCC-Ag: No impact on survival |
| CYFRA 21-1 | [144] (298) | R | LUAD | I–III | Korean | 43.3 | Worse DFS and OS |
| Combination of CYFRA 21-1 and SLX | [145] (137) | R | NSCLC | I | Japanese | NA | Worse survival |
| TMI | [146] (261) | R | NSCLC | I–II | German | 59.8 | Worse OS |
| NSE; SCC-Ag; CA125; CA199 | [147] (164) | R | NSCLC | I | Chinese | 26 | No impact on survival |
| NSE; CA125; SCC-Ag | [148] (481) | R | NSCLC | I–IIIB | Chinese | NA | NSE; CA125: Worse DFS and OS; SCC-Ag: No impact on survival |
| CA125; CA199 | [149] (58) | R | LUAD | I–IIIA | Swedish | 39.6 | Worse RFS |
| Other blood biomarkers | |||||||
| CRP | [150] (96) | R | NSCLC | I–III | British | 75 | Worse CSS |
| CRP | [151] (229) | R | NSCLC | I–II | French | 89.2 | Worse OS |
| Fibrinogen | [152] (567) | R | NSCLC | I–IIIB | Chinese | NA | Worse PFS and OS |
| D-dimer | [153] (232) | R | NSCLC | I–IIIA | Chinese | 47 | Worse OS |
| Fibrinogen; D-dimer | [154] (184) | R | NSCLC | I–IIIA | Chinese | 18.5 | Worse DFS and OS |
| Fibrinogen; D-dimer | [105] (395) | P | NSCLC | I–III | Chinese | 13.2 | Worse PFS |
| Prealbumin | [155] (44) | P | NSCLC | I–III | Japanese | NA | Improved DFS |
| PNI | [156] (248) | R | NSCLC | I–III | Japanese | 51 | Improved RFS and OS |
| CAR | [157] (156) | R | NSCLC | IIIA (N2) | German | NA | Worse RFS |
| AGS | [158] (312) | R | NSCLC | I–III | Chinese | 41 | Worse DFS and OS |
| AGR | [159] (180) | R | NSCLC | I–III | Chinese | NA | Improved OS |
| OPN | [160] (244) | R | NSCLC | I–III | Japanese | NA | Worse survival |
| OPN | [161] (201) | R | NSCLC | I–III | Norwegian | 34 | No impact on survival |
Abbreviations: CTCs, circulating tumour cells; Hb, hemoglobin; PLT, platelet; TMFs, tumour-macrophage fusion cells; NLR, neutrophil–lymphocyte ratio; PLR, platelet–lymphocyte ratio; LMR, lymphocyte–monocyte ratio; ULR, uric acid-to-lymphocyte ratio; SII, systemic immune-inflammation index (SII); ctDNA, circulating tumour DNA; CEA, carcinoembryonic antigen; SLX, Sialyl Lewisx; TMI, tumour marker index; NSE, neuron-specific enolase; SCC-Ag, squamous cell carcinoma antigen; CRP, C-reactive protein; PNI, prognostic nutritional index; CAR, CRP–albumin ratio; AGS, albumin–globulin score; AGR, albumin–globulin ratio; OPN, osteopontin; Ref, reference; NOP, number of the population; R, retrospective study; P, prospective study; Meta, meta-analysis; NSCLC, non-small-cell lung cancer; LUAD, lung adenocarcinoma; LUSC, lung squamous cell carcinoma; NA, not available; DFS, disease-free survival; RFS, relapse-free survival; PFS, progression-free survival; OS, overall survival; TTR, time to recurrence; DSS, disease-specific survival; CSS, cancer-specific survival.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cao, W.; Tang, Q.; Zeng, J.; Jin, X.; Zu, L.; Xu, S. A Review of Biomarkers and Their Clinical Impact in Resected Early-Stage Non-Small-Cell Lung Cancer. Cancers 2023, 15, 4561. https://doi.org/10.3390/cancers15184561
AMA Style
Cao W, Tang Q, Zeng J, Jin X, Zu L, Xu S. A Review of Biomarkers and Their Clinical Impact in Resected Early-Stage Non-Small-Cell Lung Cancer. Cancers. 2023; 15(18):4561. https://doi.org/10.3390/cancers15184561
Chicago/Turabian StyleCao, Weibo, Quanying Tang, Jingtong Zeng, Xin Jin, Lingling Zu, and Song Xu. 2023. "A Review of Biomarkers and Their Clinical Impact in Resected Early-Stage Non-Small-Cell Lung Cancer" Cancers 15, no. 18: 4561. https://doi.org/10.3390/cancers15184561
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.