

Optimization of Indocyanine Green for Intraoperative Fluorescent Image-Guided Localization of Lung Cancer; Analysis Based on Solid Component of Lung Nodule
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animal Experiment
2.2. Footpad Tumor Detection by Intravenous Injection of Indocyanine Green in Mouse Model
2.3. Lung Cancer Detection by Intravenous Injection of Indocyanine Green in Rabbit Lung Cancer Model
2.4. Human Lung Cancer Study Design
2.5. Surgical Procedures of Patient with Lung Cancer
2.6. Statistical Analyses
3. Results
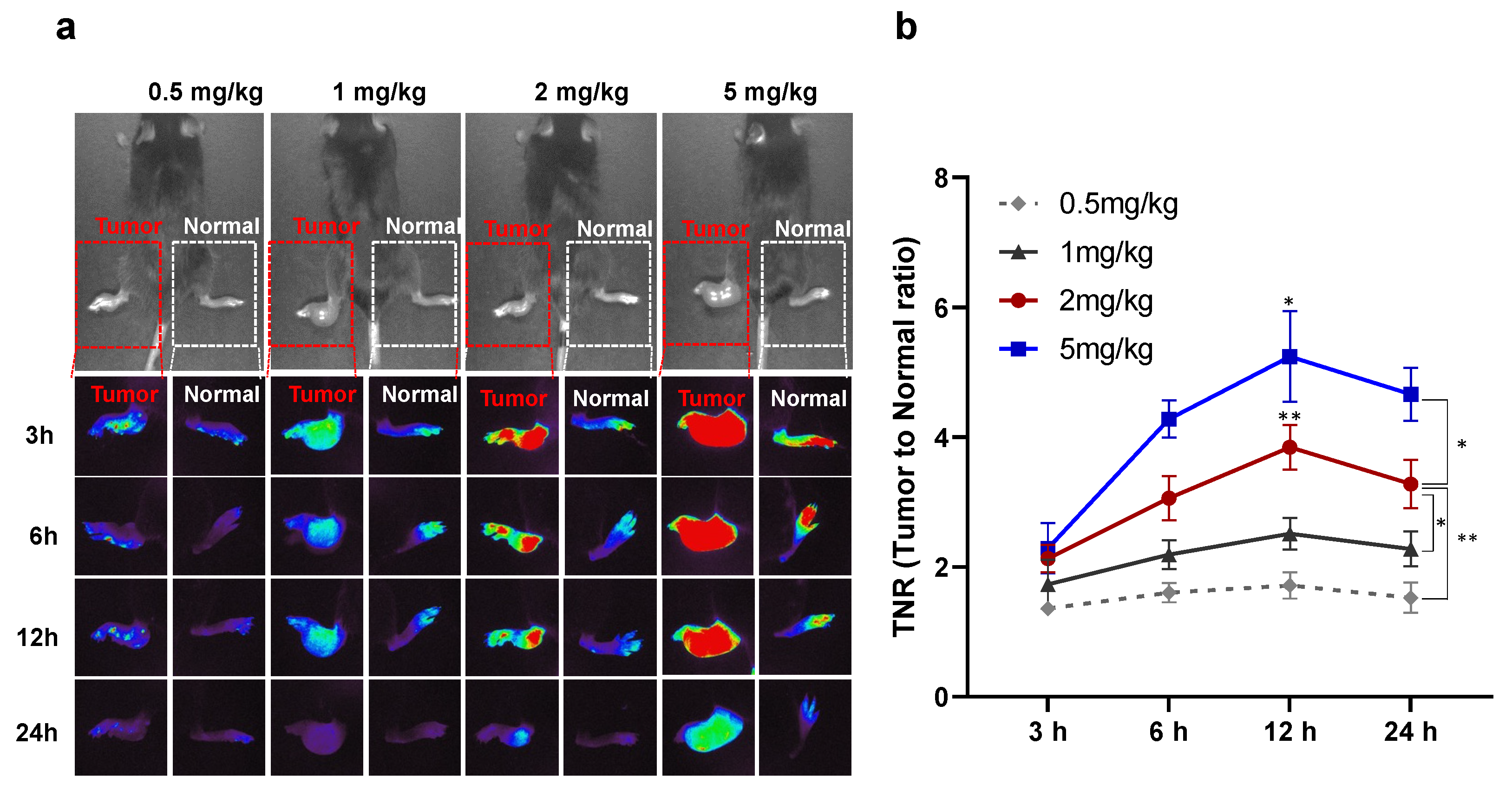
3.1. Optimization of Injection Time and Dose of Indocyanine Green for Lung Cancer Detection in a Preclinical Study
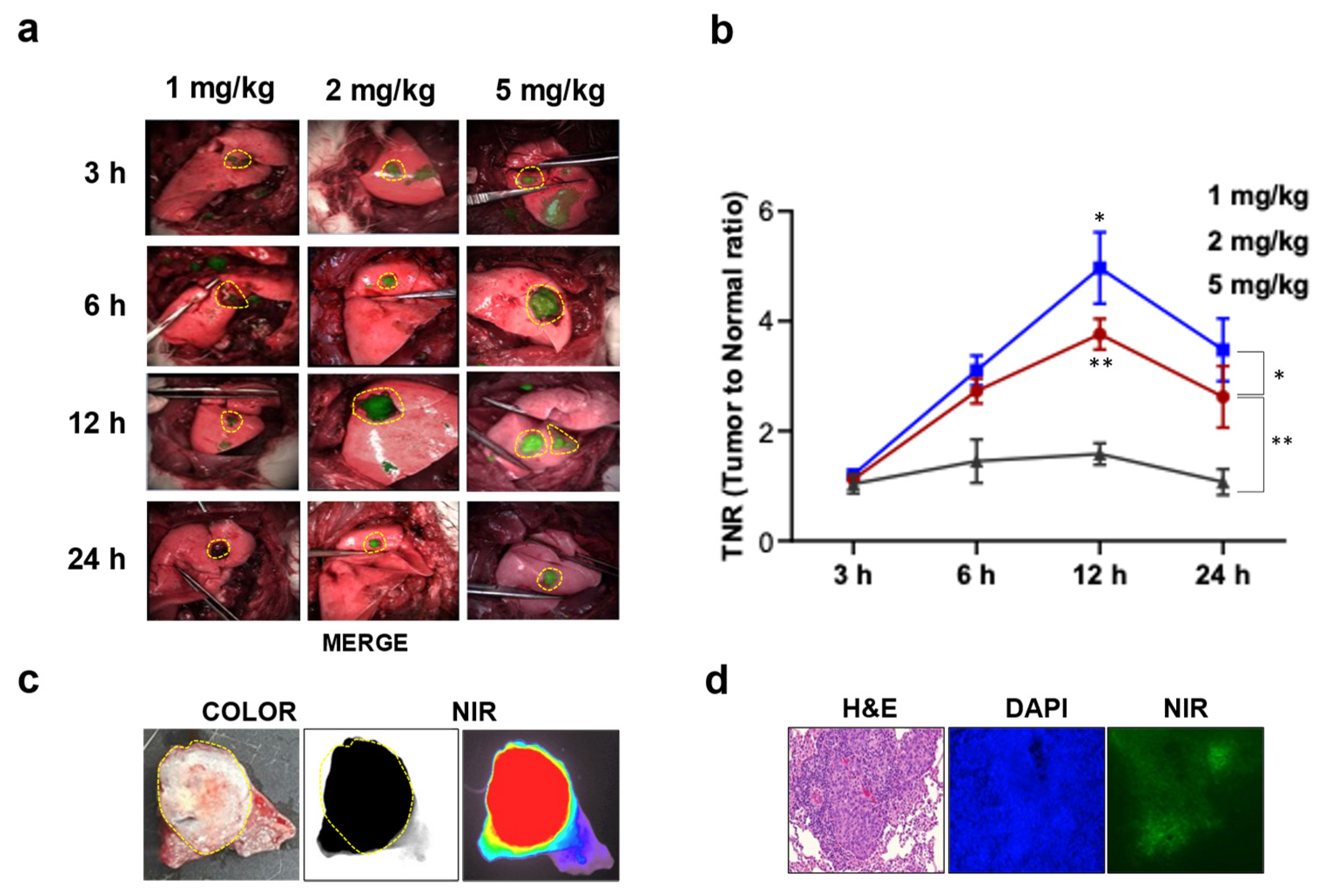
3.2. Intraoperative Fluorescence Image-Guided Thoracoscopic Resection of Lung Cancer in a Rabbit Model
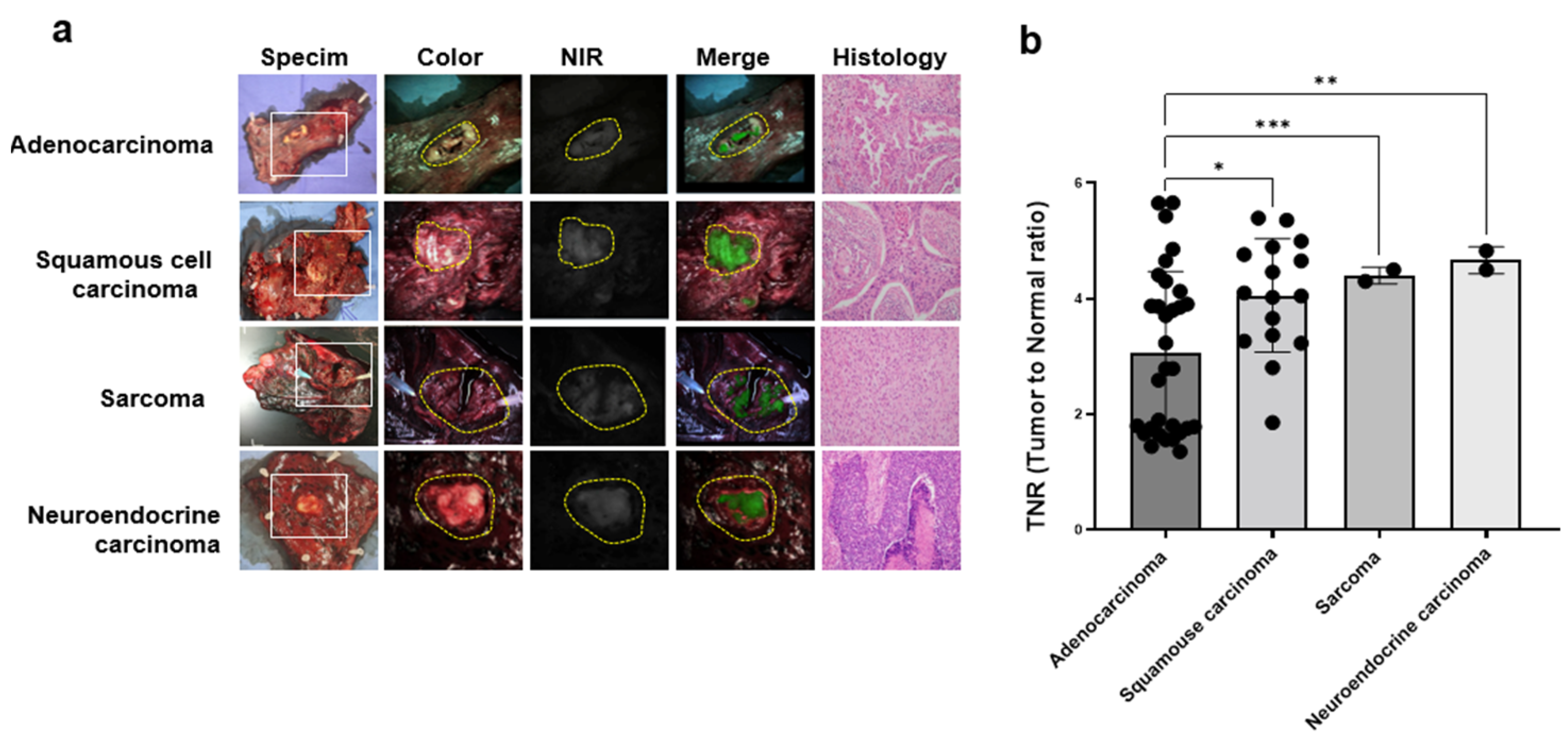
3.3. Identification of Lung Cancer Using Indocyanine Green Fluorescent Imaging in Patients with Lung Cancer
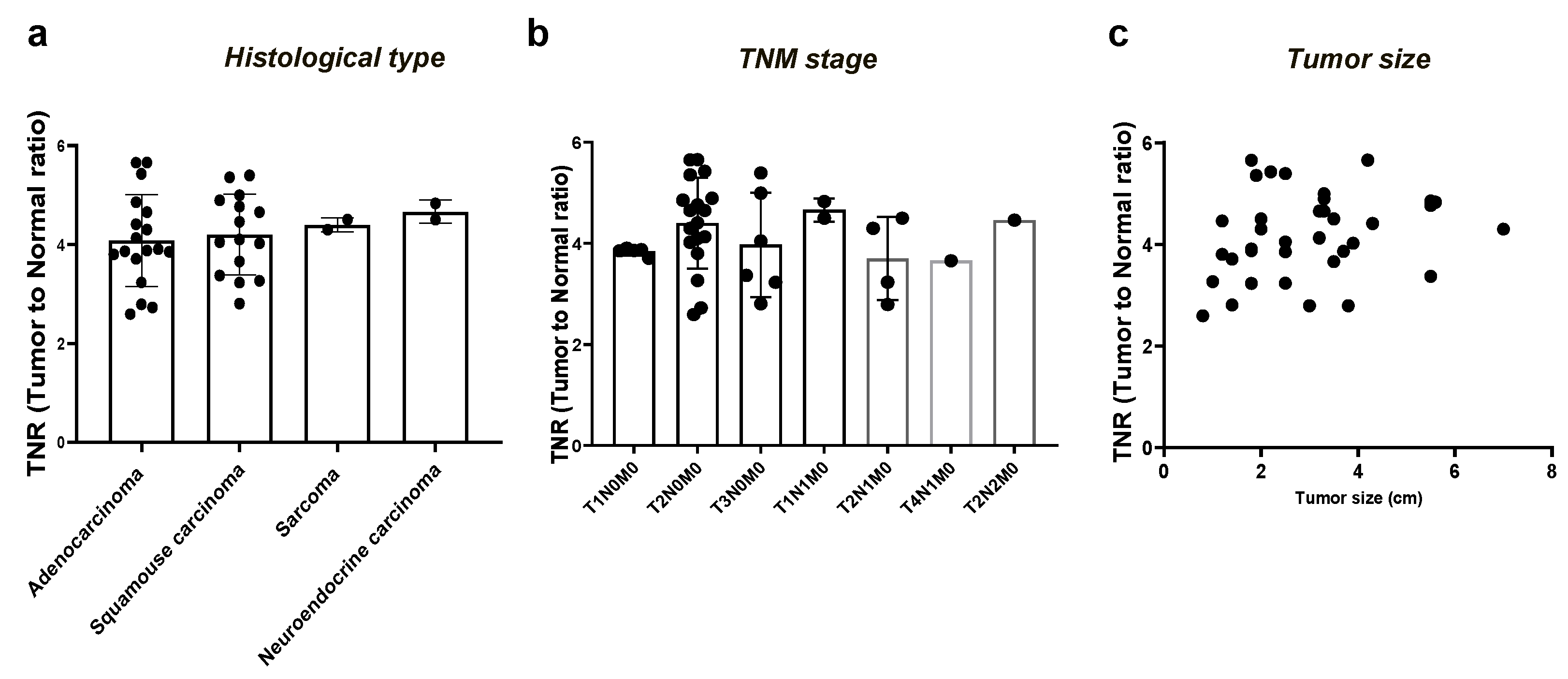
3.4. Comparison of the Tumor-to-Normal Ratio in Lung Cancer Based on the Consolidation-to-Tumor Ratio
3.5. Evaluation of the Feasibility of ICG-Based Lung Cancer Detection in Clinical Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Church, T.R.; Black, W.C.; Aberle, D.R.; Berg, C.D.; Clingan, K.L.; Duan, F.; Fagerstrom, R.M.; Gareen, I.F.; Gierada, D.S.; Jones, G.C.; et al. Results of initial low-dose computed tomographic screening for lung cancer. N. Engl. J. Med. 2013, 368, 1980–1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naruke, T.; Goya, T.; Tsuchiya, R.; Suemasu, K. Prognosis and survival in resected lung carcinoma based on the new international staging system. J. Thorac. Cardiovasc. Surg. 1988, 96, 440–447. [Google Scholar] [CrossRef]
- Low, M.; Ben-Or, S. Thoracic Surgery in Early-Stage Small Cell Lung Cancer. Thorac. Surg. Clin. 2018, 28, 9–14. [Google Scholar] [CrossRef]
- Wolf, A.S.; Richards, W.G.; Jaklitsch, M.T.; Gill, R.; Chirieac, L.R.; Colson, Y.L.; Mohiuddin, K.; Mentzer, S.J.; Bueno, R.; Sugarbaker, D.J.; et al. Lobectomy versus sublobar resection for small (2 cm or less) non-small cell lung cancers. Ann. Thorac. Surg. 2011, 92, 1819–1823; discussion 1824–1815. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Saji, H.; Aokage, K.; Watanabe, S.I.; Okada, M.; Mizusawa, J.; Nakajima, R.; Tsuboi, M.; Nakamura, S.; Nakamura, K.; et al. Comparison of pulmonary segmentectomy and lobectomy: Safety results of a randomized trial. J. Thorac. Cardiovasc. Surg. 2019, 158, 895–907. [Google Scholar] [CrossRef]
- Russell, P.A.; Wainer, Z.; Wright, G.M.; Daniels, M.; Conron, M.; Williams, R.A. Does lung adenocarcinoma subtype predict patient survival?: A clinicopathologic study based on the new International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary lung adenocarcinoma classification. J. Thorac. Oncol. 2011, 6, 1496–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA A Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [Green Version]
- Hou, B.; Deng, X.F.; Zhou, D.; Liu, Q.X.; Dai, J.G. Segmentectomy versus wedge resection for the treatment of high-risk operable patients with stage I non-small cell lung cancer: A meta-analysis. Ther. Adv. Respir. Dis. 2016, 10, 435–443. [Google Scholar] [CrossRef] [Green Version]
- Narsule, C.K.; Ebright, M.I.; Fernando, H.C. Sublobar versus lobar resection: Current status. Cancer J. 2011, 17, 23–27. [Google Scholar] [CrossRef]
- Chao, Y.K.; Wen, C.T.; Fang, H.Y.; Hsieh, M.J. A single-center experience of 100 image-guided video-assisted thoracoscopic surgery procedures. J. Thorac. Dis. 2018, 10, S1624–S1630. [Google Scholar] [CrossRef] [PubMed]
- Gill, R.R.; Zheng, Y.; Barlow, J.S.; Jayender, J.; Girard, E.E.; Hartigan, P.M.; Chirieac, L.R.; Belle-King, C.J.; Murray, K.; Sears, C.; et al. Image-guided video assisted thoracoscopic surgery (iVATS)—Phase I-II clinical trial. J. Surg. Oncol. 2015, 112, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Tarumi, S.; Misaki, N.; Kasai, Y.; Chang, S.S.; Go, T.; Yokomise, H. Clinical trial of video-assisted thoracoscopic segmentectomy using infrared thoracoscopy with indocyanine green. Eur. J. Cardio-Thorac. Surg. 2014, 46, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.; Tokuishi, K.; Anami, K.; Miyawaki, M.; Moroga, T.; Kamei, M.; Suehiro, S.; Ono, K.; Takeno, S.; Chujo, M.; et al. Video-assisted thoracoscopic indocyanine green fluorescence imaging system shows sentinel lymph nodes in non-small-cell lung cancer. J. Thorac. Cardiovasc. Surg. 2011, 141, 141–144. [Google Scholar] [CrossRef] [Green Version]
- Whitson, B.A.; Groth, S.S.; Duval, S.J.; Swanson, S.J.; Maddaus, M.A. Surgery for early-stage non-small cell lung cancer: A systematic review of the video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann. Thorac. Surg. 2008, 86, 2008–2016; discussion 2016–2008. [Google Scholar] [CrossRef] [PubMed]
- Han, K.N.; Kim, H.K. Imaging techniques for minimally invasive thoracic surgery-Korea University Guro Hospital experiences. J. Thorac. Dis. 2018, 10, S731–S738. [Google Scholar] [CrossRef]
- Kidane, B.; Yasufuku, K. Advances in Image-Guided Thoracic Surgery. Thorac. Surg. Clin. 2016, 26, 129–138. [Google Scholar] [CrossRef]
- Kim, Y.; Rho, J.; Quan, Y.H.; Choi, B.H.; Han, K.N.; Kim, H.K.; Choi, Y.H. Simultaneous visualization of pulmonary nodules and intersegmental planes on fluorescent images in pulmonary segmentectomy. Eur. J. Cardio-Thorac. Surg. 2020, 58, i77–i84. [Google Scholar] [CrossRef]
- Rho, J.; Lee, J.W.; Quan, Y.H.; Choi, B.H.; Shin, B.K.; Han, K.N.; Kim, B.M.; Choi, Y.H.; Yong, H.S.; Kim, H.K. Fluorescent and Iodized Emulsion for Preoperative Localization of Pulmonary Nodules. Ann. Surg. 2021, 273, 989–996. [Google Scholar] [CrossRef]
- Gotoh, K.; Yamada, T.; Ishikawa, O.; Takahashi, H.; Eguchi, H.; Yano, M.; Ohigashi, H.; Tomita, Y.; Miyamoto, Y.; Imaoka, S. A novel image-guided surgery of hepatocellular carcinoma by indocyanine green fluorescence imaging navigation. J. Surg. Oncol. 2009, 100, 75–79. [Google Scholar] [CrossRef]
- Keating, J.; Tchou, J.; Okusanya, O.; Fisher, C.; Batiste, R.; Jiang, J.; Kennedy, G.; Nie, S.; Singhal, S. Identification of breast cancer margins using intraoperative near-infrared imaging. J. Surg. Oncol. 2016, 113, 508–514. [Google Scholar] [CrossRef]
- Predina, J.D.; Keating, J.; Newton, A.; Corbett, C.; Xia, L.; Shin, M.; Frenzel Sulyok, L.; Deshpande, C.; Litzky, L.; Nie, S.; et al. A clinical trial of intraoperative near-infrared imaging to assess tumor extent and identify residual disease during anterior mediastinal tumor resection. Cancer 2019, 125, 807–817. [Google Scholar] [CrossRef]
- Quan, Y.H.; Xu, R.; Choi, B.H.; Rho, J.; Lee, J.H.; Han, K.N.; Choi, Y.H.; Kim, B.M.; Kim, H.K. Fluorescence Imaging-Guided Identification of Thymic Masses Using Low-Dose Indocyanine Green. Ann. Surg. Oncol. 2022, 29, 4476–4485. [Google Scholar] [CrossRef]
- Rho, J.; Quan, Y.H.; Choi, B.H.; Han, K.N.; Kim, B.M.; Choi, Y.H.; Kim, H.K. Near-infrared fluorescent imaging with indocyanine green in rabbit and patient specimens of esophageal cancer. J. Thorac. Dis. 2021, 13, 6314–6322. [Google Scholar] [CrossRef] [PubMed]
- Souzaki, R.; Kawakubo, N.; Matsuura, T.; Yoshimaru, K.; Koga, Y.; Takemoto, J.; Shibui, Y.; Kohashi, K.; Hayashida, M.; Oda, Y.; et al. Navigation surgery using indocyanine green fluorescent imaging for hepatoblastoma patients. Pediatr. Surg. Int. 2019, 35, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Keating, J.; Singhal, S. Novel Methods of Intraoperative Localization and Margin Assessment of Pulmonary Nodules. Semin. Thorac. Cardiovasc. Surg. 2016, 28, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Madajewski, B.; Judy, B.F.; Mouchli, A.; Kapoor, V.; Holt, D.; Wang, M.D.; Nie, S.; Singhal, S. Intraoperative near-infrared imaging of surgical wounds after tumor resections can detect residual disease. Clin. Cancer Res. 2012, 18, 5741–5751. [Google Scholar] [CrossRef] [Green Version]
- Okusanya, O.T.; Holt, D.; Heitjan, D.; Deshpande, C.; Venegas, O.; Jiang, J.; Judy, R.; DeJesus, E.; Madajewski, B.; Oh, K.; et al. Intraoperative near-infrared imaging can identify pulmonary nodules. Ann. Thorac. Surg. 2014, 98, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Teng, C.W.; Cho, S.S.; Singh, Y.; De Ravin, E.; Somers, K.; Buch, L.; Brem, S.; Singhal, S.; Delikatny, E.J.; Lee, J.Y.K. Second window ICG predicts gross-total resection and progression-free survival during brain metastasis surgery. J. Neurosurg. 2021, 135, 1–10. [Google Scholar] [CrossRef]
- Jiang, J.X.; Keating, J.J.; Jesus, E.M.; Judy, R.P.; Madajewski, B.; Venegas, O.; Okusanya, O.T.; Singhal, S. Optimization of the enhanced permeability and retention effect for near-infrared imaging of solid tumors with indocyanine green. Am. J. Nucl. Med. Mol. Imaging 2015, 5, 390–400. [Google Scholar]
- Kim, H.K.; Quan, Y.H.; Choi, B.H.; Park, J.H.; Han, K.N.; Choi, Y.; Kim, B.M.; Choi, Y.H. Intraoperative pulmonary neoplasm identification using near-infrared fluorescence imaging. Eur. J. Cardio-Thorac. Surg. 2016, 49, 1497–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, F.; Kozak, K.R.; Imaizumi, S.; Gao, F.; Amneus, M.W.; Grijalva, V.; Ng, C.; Wagner, A.; Hough, G.; Farias-Eisner, G.; et al. Apolipoprotein A-I (apoA-I) and apoA-I mimetic peptides inhibit tumor development in a mouse model of ovarian cancer. Proc. Natl. Acad. Sci. USA 2010, 107, 19997–20002. [Google Scholar] [CrossRef]
- Quan, Y.H.; Oh, C.H.; Jung, D.; Lim, J.Y.; Choi, B.H.; Rho, J.; Choi, Y.; Han, K.N.; Kim, B.M.; Kim, C.; et al. Evaluation of Intraoperative Near-Infrared Fluorescence Visualization of the Lung Tumor Margin With Indocyanine Green Inhalation. JAMA Surg. 2020, 155, 732–740. [Google Scholar] [CrossRef]
- Choi, B.H.; Young, H.S.; Quan, Y.H.; Rho, J.; Eo, J.S.; Han, K.N.; Choi, Y.H.; Hyun Koo, K. Real-time computed tomography fluoroscopy-guided solitary lung tumor model in a rabbit. PLoS ONE 2017, 12, e0179220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawakita, N.; Takizawa, H.; Kondo, K.; Sakiyama, S.; Tangoku, A. Indocyanine Green Fluorescence Navigation Thoracoscopic Metastasectomy for Pulmonary Metastasis of Hepatocellular Carcinoma. Ann. Thorac. Cardiovasc. Surg. 2016, 22, 367–369. [Google Scholar] [CrossRef] [Green Version]
- Newton, A.D.; Predina, J.D.; Corbett, C.J.; Frenzel-Sulyok, L.G.; Xia, L.; Petersson, E.J.; Tsourkas, A.; Nie, S.; Delikatny, E.J.; Singhal, S. Optimization of Second Window Indocyanine Green for Intraoperative Near-Infrared Imaging of Thoracic Malignancy. J. Am. Coll. Surg. 2019, 228, 188–197. [Google Scholar] [CrossRef]
- Azari, F.; Kennedy, G.; Zhang, K.; Bernstein, E.; Chang, A.; Nadeem, B.; Segil, A.; Desphande, C.; Delikatny, J.; Kucharczuk, J.; et al. Effects of Light-absorbing Carbons in Intraoperative Molecular Imaging-Guided Lung Cancer Resections. Mol. Imaging Biol. 2023, 25, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Onda, N.; Kimura, M.; Yoshida, T.; Shibutani, M. Preferential tumor cellular uptake and retention of indocyanine green for in vivo tumor imaging. Int. J. Cancer 2016, 139, 673–682. [Google Scholar] [CrossRef]
- Predina, J.D.; Newton, A.; Corbett, C.; Xia, L.; Sulyok, L.F.; Shin, M.; Deshpande, C.; Litzky, L.; Barbosa, E.; Low, P.S.; et al. Localization of Pulmonary Ground-Glass Opacities with Folate Receptor-Targeted Intraoperative Molecular Imaging. J. Thorac. Oncol. 2018, 13, 1028–1036. [Google Scholar] [CrossRef] [Green Version]
- Azari, F.; Kennedy, G.; Bernstein, E.; Delikatny, J.; Lee, J.Y.K.; Kucharczuk, J.; Low, P.S.; Singhal, S. Evaluation of OTL38-Generated Tumor-to-Background Ratio in Intraoperative Molecular Imaging-Guided Lung Cancer Resections. Mol. Imaging Biol. 2023, 25, 85–96. [Google Scholar] [CrossRef]
- de Valk, K.S.; Deken, M.M.; Handgraaf, H.J.; Bhairosingh, S.S.; Bijlstra, O.D.; van Esdonk, M.J.; Terwisscha van Scheltinga, A.G.; Valentijn, A.R.P.; March, T.L.; Vuijk, J. First-in-human assessment of cRGD-ZW800-1, a zwitterionic, integrin-targeted, near-infrared fluorescent peptide in colon carcinoma. Clin. Cancer Res. 2020, 26, 3990–3998. [Google Scholar] [CrossRef]
- Zhu, S.; Tian, R.; Antaris, A.L.; Chen, X.; Dai, H. Near-Infrared-II Molecular Dyes for Cancer Imaging and Surgery. Adv. Mater. 2019, 31, e1900321. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Z.; Li, Y.; Hu, D.; Min, T.; Gao, D.; Ni, J.S.; Zhang, P.; Wang, Y.; Liu, X.; Li, K.; et al. Centimeter-Deep NIR-II Fluorescence Imaging with Nontoxic AIE Probes in Nonhuman Primates. Research 2020, 2020, 4074593. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Wang, D.; Tang, B.Z. NIR-II AIEgens: A Win-Win Integration towards Bioapplications. Angew.Chem. Int. Ed. 2021, 60, 7476–7487. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, N.S.; Simon, H.; Kleinjan, G.H.; Engelen, T.; Bunschoten, A.; Welling, M.M.; Tijink, B.M.; Horenblas, S.; Chambron, J.; van Leeuwen, F.W.B. First-in-human evaluation of a hybrid modality that allows combined radio- and (near-infrared) fluorescence tracing during surgery. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Bugby, S.L.; Lees, J.E.; Perkins, A.C. Hybrid intraoperative imaging techniques in radioguided surgery: Present clinical applications and future outlook. Clin. Transl. Imaging 2017, 5, 323–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 51 |
|---|---|
| Mean age (Range) | 65 ± 10 (38–81) |
| Gender (%) | |
| Female | 19 (35%) |
| Male | 32 (65%) |
| Tumor location (%) | |
| RUL | 11 (22%) |
| RML | 4 (8%) |
| RLL | 12 (25%) |
| LUL | 13 (25%) |
| LLL | 11 (20%) |
| Surgical procedure (VATS or Robotic) (%) | |
| Wedge resection | 3 (8%) |
| Segmentectomy | 5 (8%) |
| Lobectomy | 42 (82%) |
| Pneumonectomy | 1 (2%) |
| Mean tumor size, cm (Range) | 2.8 ± 1.5 (0.7–7) |
| Histologic diagnosis, (%) | |
| Adenocarcinoma | 31 (61%) |
| Squamous cell carcinoma | 16 (31%) |
| Sarcoma | 2 (4%) |
| Neuroendocrine carcinoma | 2 (4%) |
| p-TNM stage (%) | |
| T1N0M0 | 14 (27%) |
| T2N0M0 | 23 (45%) |
| T3N0M0 | 6 (12%) |
| T1N1M0 | 2 (4%) |
| T2N1M0 | 4 (8%) |
| T4N1M0 | 1 (2%) |
| T2N2M0 | 1 (2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, O.H.; Choi, B.H.; Rho, J.; Kim, K.; Lee, J.H.; Lee, J.; Kim, B.-M.; Kim, H.K. Optimization of Indocyanine Green for Intraoperative Fluorescent Image-Guided Localization of Lung Cancer; Analysis Based on Solid Component of Lung Nodule. Cancers 2023, 15, 3643. https://doi.org/10.3390/cancers15143643
Jeon OH, Choi BH, Rho J, Kim K, Lee JH, Lee J, Kim B-M, Kim HK. Optimization of Indocyanine Green for Intraoperative Fluorescent Image-Guided Localization of Lung Cancer; Analysis Based on Solid Component of Lung Nodule. Cancers. 2023; 15(14):3643. https://doi.org/10.3390/cancers15143643
Chicago/Turabian StyleJeon, Ok Hwa, Byeong Hyeon Choi, Jiyun Rho, Kyungsu Kim, Jun Hee Lee, Jinhwan Lee, Beop-Min Kim, and Hyun Koo Kim. 2023. "Optimization of Indocyanine Green for Intraoperative Fluorescent Image-Guided Localization of Lung Cancer; Analysis Based on Solid Component of Lung Nodule" Cancers 15, no. 14: 3643. https://doi.org/10.3390/cancers15143643