

Risk Factors, Prevalence, and Outcomes of Invasive Fungal Disease Post Hematopoietic Cell Transplantation and Cellular Therapies: A Retrospective Monocenter Real-Life Analysis
 , , ,
, , ,  , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cohort and Study Design
2.2. Statistics
3. Results
3.1. Study Population
3.2. Antifungal Prophylaxis and Patient Evaluation
3.3. Incidence and Characteristics of IFD
3.4. Independent Risk Factors for IFD
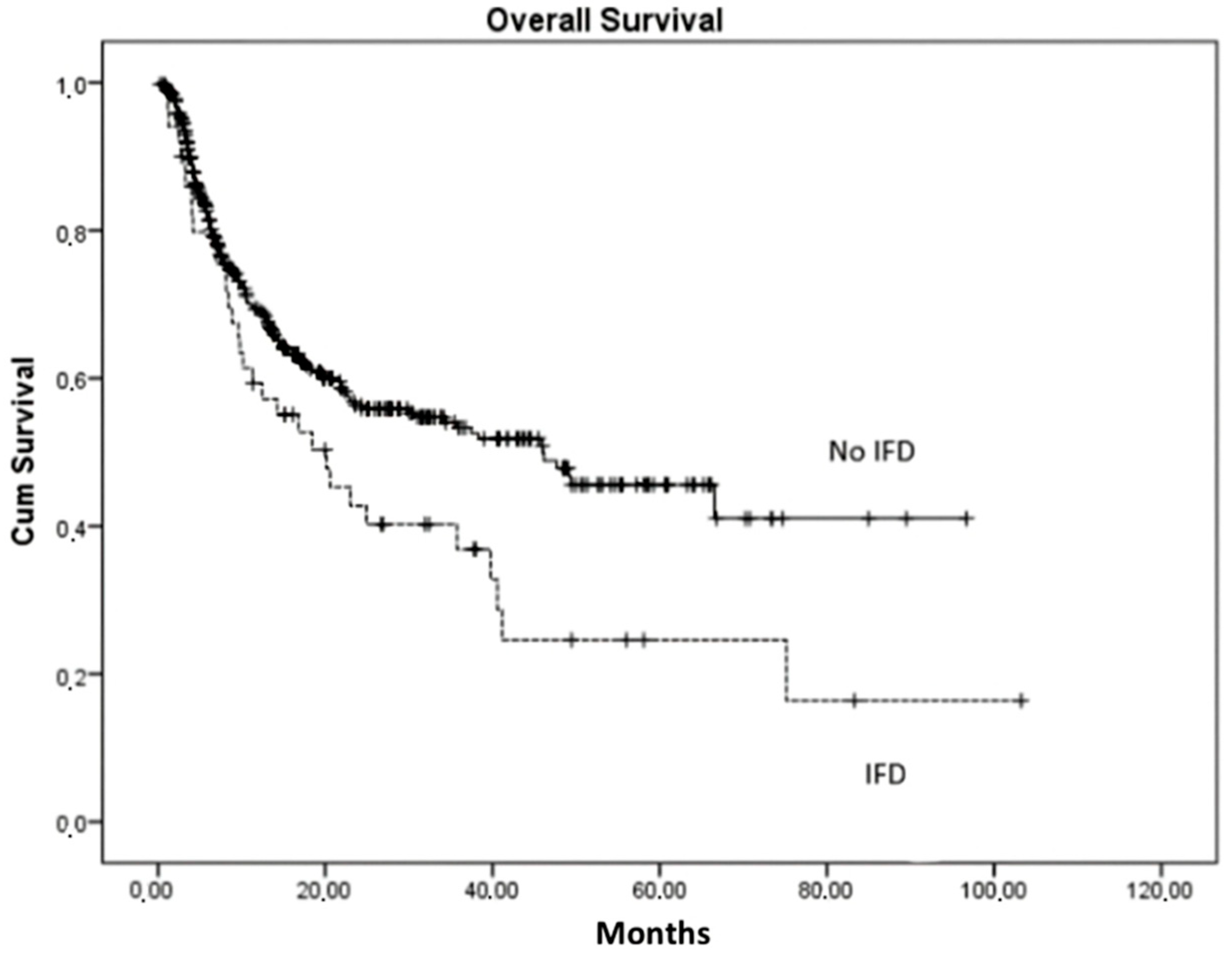
3.5. Overall Survival (OS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gyurkocza, B.; Rezvani, A.; Storb, R.F. Allogeneic Hematopoietic Cell Transplantation: The State of the Art. Expert Rev. Hematol. 2010, 3, 285–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copelan, E.A.; Chojecki, A.; Lazarus, H.M.; Avalos, B.R. Allogeneic Hematopoietic Cell Transplantation; the Current Renaissance. Blood Rev. 2019, 34, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Caocci, G.; Orofino, M.G.; Vacca, A.; Piroddi, A.; Piras, E.; Addari, M.C.; Caria, R.; Pilia, M.P.; Origa, R.; Moi, P.; et al. Long-Term Survival of Beta Thalassemia Major Patients Treated with Hematopoietic Stem Cell Transplantation Compared with Survival with Conventional Treatment. Am. J. Hematol. 2017, 92, 1303–1310. [Google Scholar] [CrossRef] [Green Version]
- Palumbo, A.; Cavallo, F.; Gay, F.; Di Raimondo, F.; Ben Yehuda, D.; Petrucci, M.T.; Pezzatti, S.; Caravita, T.; Cerrato, C.; Ribakovsky, E.; et al. Autologous Transplantation and Maintenance Therapy in Multiple Myeloma. N. Engl. J. Med. 2014, 371, 895–905. [Google Scholar] [CrossRef]
- Rodríguez-Lozano, F.J.; Oñate-Sánchez, R.; Gonzálvez-García, M.; Vallés-Bergadá, M.; Martínez, C.M.; Revilla-Nuin, B.; Guerrero-Gironés, J.; Moraleda, J.M.; García-Bernal, D. Allogeneic Bone Marrow Mesenchymal Stem Cell Transplantation in Tooth Extractions Sites Ameliorates the Incidence of Osteonecrotic Jaw-like Lesions in Zoledronic Acid-Treated Rats. J. Clin. Med. 2020, 9, 1649. [Google Scholar] [CrossRef] [PubMed]
- Wingard, J.R. Infections in Allogeneic Bone Marrow Transplant Recipients. Semin. Oncol. 1993, 20, 80–87. [Google Scholar]
- Wingard, J.R.; Hsu, J.; Hiemenz, J.W. Hematopoietic Stem Cell Transplantation: An Overview of Infection Risks and Epidemiology. Infect. Dis. Clin. N. Am. 2010, 24, 257–272. [Google Scholar] [CrossRef]
- Small, T.N.; Papadopoulos, E.B.; Boulad, F.; Black, P.; Castro-Malaspina, H.; Childs, B.H.; Collins, N.; Gillio, A.; George, D.; Jakubowski, A.; et al. Comparison of Immune Reconstitution after Unrelated and Related T-Cell-Depleted Bone Marrow Transplantation: Effect of Patient Age and Donor Leukocyte Infusions. Blood 1999, 93, 467–480. [Google Scholar] [CrossRef]
- Ferdjallah, A.; Young, J.A.H.; MacMillan, M.L. A Review of Infections After Hematopoietic Cell Transplantation Requiring PICU Care: Transplant Timeline Is Key. Front. Pediatr. 2021, 9, 634449. [Google Scholar] [CrossRef]
- Tomblyn, M.; Chiller, T.; Einsele, H.; Gress, R.; Sepkowitz, K.; Storek, J.; Wingard, J.R.; Young, J.A.H.; Boeckh, M.A. Guidelines for Preventing Infectious Complications among Hematopoietic Cell Transplantation Recipients: A Global Perspective. Biol. Blood Marrow Transplant. 2009, 15, 1143–1238. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Romero, F.A.; Taur, Y.; Sadelain, M.; Brentjens, R.J.; Hohl, T.M.; Seo, S.K. Cytokine Release Syndrome Grade as a Predictive Marker for Infections in Patients with Relapsed or Refractory B-Cell Acute Lymphoblastic Leukemia Treated with Chimeric Antigen Receptor T Cells. Clin. Infect. Dis. 2018, 67, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Wudhikarn, K.; Palomba, M.L.; Pennisi, M.; Garcia-Recio, M.; Flynn, J.R.; Devlin, S.M.; Afuye, A.; Silverberg, M.L.; Maloy, M.A.; Shah, G.L.; et al. Infection during the First Year in Patients Treated with CD19 CAR T Cells for Diffuse Large B Cell Lymphoma. Blood Cancer J. 2020, 10, 79. [Google Scholar] [CrossRef]
- Hill, J.A.; Li, D.; Hay, K.A.; Green, M.L.; Cherian, S.; Chen, X.; Riddell, S.R.; Maloney, D.G.; Boeckh, M.; Turtle, C.J. Infectious Complications of CD19-Targeted Chimeric Antigen Receptor-Modified T-Cell Immunotherapy. Blood 2018, 131, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Wingard, J.R. The Changing Face of Invasive Fungal Infections in Hematopoietic Cell Transplant Recipients. Curr. Opin. Oncol. 2005, 17, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Wingard, J.R. Fungal Infections after Bone Marrow Transplant. Biol. Blood Marrow Transplant. 1999, 5, 55–68. [Google Scholar] [CrossRef] [Green Version]
- Kontoyiannis, D.P.; Wessel, V.C.; Bodey, G.P.; Rolston, K.V.I. Zygomycosis in the 1990s in a Tertiary-Care Cancer Center. Clin. Infect. Dis. 2000, 30, 851–856. [Google Scholar] [CrossRef] [Green Version]
- Schuster, M.G.; Cleveland, A.A.; Dubberke, E.R.; Kauffman, C.A.; Avery, R.K.; Husain, S.; Paterson, D.L.; Silveira, F.P.; Chiller, T.M.; Benedict, K.; et al. Infections in Hematopoietic Cell Transplant Recipients: Results from the Organ Transplant Infection Project, a Multicenter, Prospective, Cohort Study. Open Forum Infect. Dis. 2017, 4, ofx050. [Google Scholar] [CrossRef] [Green Version]
- Kontoyiennis, D.P.; Marr, K.A.; Park, B.J.; Alexander, B.D.; Anaissie, E.J.; Walsh, T.J.; Ito, J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; et al. Prospective Surveillance for Invasive Fungal Infections in Hematopoietic Stem Cell Transplant Recipients, 2001–2006: Overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin. Infect. Dis. 2010, 50, 1091–1100. [Google Scholar] [CrossRef]
- Cobo, F.; Lara-Oya, A.; Rodríguez-Granger, J.; Sampedro, A.; Aliaga-Martínez, L.; Navarro-Marí, J.M. Infections caused by Scedosporium/Lomentospora species: Clinical and microbiological findings in 21 cases. Med. Mycol. 2018, 56, 917–925. [Google Scholar] [CrossRef]
- Husain, S.; Muñoz, P.; Forrest, G.; Alexander, B.D.; Somani, J.; Brennan, K.; Wagener, M.M.; Singh, N. Infections Due to Scedosporium Apiospermum and Scedosporium Prolificans in Transplant Recipients: Clinical Characteristics and Impact of Antifungal Agent Therapy on Outcome. Clin. Infect. Dis. 2005, 40, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Maertens, J.A.; Girmenia, C.; Brüggemann, R.J.; Duarte, R.F.; Kibbler, C.C.; Ljungman, P.; Racil, Z.; Ribaud, P.; Slavin, M.A.; Cornely, O.A.; et al. European Guidelines for Primary Antifungal Prophylaxis in Adult Haematology Patients: Summary of the Updated Recommendations from the European Conference on Infections in Leukaemia. J. Antimicrob. Chemother. 2018, 73, 3221–3230. [Google Scholar] [CrossRef] [PubMed]
- Marr, K.A.; Bow, E.; Chiller, T.; Maschmeyer, G.; Ribaud, P.; Segal, B.; Steinbach, W.; Wingard, J.R.; Nucci, M. Fungal Infection Prevention after Hematopoietic Cell Transplantation. Bone Marrow Transplant. 2009, 44, 483–487. [Google Scholar] [CrossRef]
- Los-Arcos, I.; Iacoboni, G.; Aguilar-Guisado, M.; Alsina-Manrique, L.; Díaz de Heredia, C.; Fortuny-Guasch, C.; García-Cadenas, I.; García-Vidal, C.; González-Vicent, M.; Hernani, R.; et al. Recommendations for Screening, Monitoring, Prevention, and Prophylaxis of Infections in Adult and Pediatric Patients Receiving CAR T-Cell Therapy: A Position Paper. Infection 2021, 49, 215–231. [Google Scholar] [CrossRef] [PubMed]
- Peter Donnelly, J.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, J.; Teh, B.W.; Micklethwaite, K.; Slavin, M. Azole Antifungals and New Targeted Therapies for Hematological Malignancy. Curr. Opin. Infect. Dis. 2019, 32, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus Voriconazole for Primary Treatment of Invasive Mould Disease Caused by Aspergillus and Other Filamentous Fungi (SECURE): A Phase 3, Randomised-Controlled, Non-Inferiority Trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef]
- Cornely, O.A.; Duarte, R.F.; Haider, S.; Chandrasekar, P.; Helfgott, D.; Jiménez, J.L.; Candoni, A.; Raad, I.; Laverdiere, M.; Langston, A.; et al. Phase 3 Pharmacokinetics and Safety Study of a Posaconazole Tablet Formulation in Patients at Risk for Invasive Fungal Disease. J. Antimicrob. Chemother. 2016, 71, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Teh, B.W.; Yeoh, D.K.; Haeusler, G.M.; Yannakou, C.K.; Fleming, S.; Lindsay, J.; Slavin, M.A.; Chang, C.C.; Blyth, C.C.; Chen, S.C.A.; et al. Consensus Guidelines for Antifungal Prophylaxis in Haematological Malignancy and Haemopoietic Stem Cell Transplantation, 2021. Intern. Med. J. 2021, 51, 67–88. [Google Scholar] [CrossRef]
- Sakellari, I.; Mallouri, D.; Gavriilaki, E.; Batsis, I.; Kaliou, M.; Constantinou, V.; Papalexandri, A.; Lalayanni, C.; Vadikolia, C.; Athanasiadou, A.; et al. Survival Advantage and Comparable Toxicity in Reduced-Toxicity Treosulfan-Based versus Reduced-Intensity Busulfan-Based Conditioning Regimen in Myelodysplastic Syndrome and Acute Myeloid Leukemia Patients after Allogeneic Hematopoietic Cell Transplantatio. Biol. Blood Marrow Transplant. 2017, 23, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Sakellari, I.; Batsis, I.; Bousiou, Z.; Mallouri, D.; Constantinou, V.; Gavriilaki, E.; Smias, C.; Yannaki, E.; Kaloyannidis, P.; Papaioannou, G.; et al. The Role of Low-Dose Anti-Thymocyte Globulin as Standard Prophylaxis in Mismatched and Matched Unrelated Hematopoietic Peripheral Stem Cell Transplantation for Hematologic Malignancies. Clin. Lymphoma Myeloma Leuk. 2017, 17, 658–666. [Google Scholar] [CrossRef]
- Sakellari, I.; Gavriilaki, E.; Chatziioannou, K.; Papathanasiou, M.; Mallouri, D.; Batsis, I.; Bousiou, Z.; Bouziana, S.; Constantinou, V.; Douka, V.; et al. Long-Term Outcomes of Total Body Irradiation plus Cyclophosphamide versus Busulfan plus Cyclophosphamide as Conditioning Regimen for Acute Lymphoblastic Leukemia: A Comparative Study. Ann. Hematol. 2018, 97, 1987–1994. [Google Scholar] [CrossRef]
- Alexander, B.D.; Lamoth, F.; Heussel, C.P.; Prokop, C.S.; Desai, S.R.; Morrissey, C.O.; Baddley, J.W. Guidance on Imaging for Invasive Pulmonary Aspergillosis and Mucormycosis: From the Imaging Working Group for the Revision and Update of the Consensus Definitions of Fungal Disease from the EORTC/MSGERC. Clin. Infect. Dis. 2021, 72, S79–S88. [Google Scholar] [CrossRef]
- Sorror, M.L.; Maris, M.B.; Storb, R.; Baron, F.; Sandmaier, B.M.; Maloney, D.G.; Storer, B. Hematopoietic Cell Transplantation (HCT)-Specific Comorbidity Index: A New Tool for Risk Assessment before Allogeneic HCT. Blood 2005, 106, 2912–2919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glucksberg, H.; Storb, R.; Fefer, A.; Buckner, C.D.; Neiman, P.E.; Clift, R.A.; Lerner, K.G.; Thomas, E.D. Clinical Manifestations of Graft-versus-Host Disease in Human Recipients of Marrow from HL-A-Matched Sibling Donors. Transplantation 1974, 18, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software “EZR” for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Vora, S.B.; Waghmare, A.; Englund, J.A.; Qu, P.; Gardner, R.A.; Hill, J.A. Infectious Complications Following CD19 Chimeric Antigen Receptor T-Cell Therapy for Children, Adolescents, and Young Adults. Open Forum Infect. Dis. 2020, 7, ofaa121. [Google Scholar] [CrossRef] [Green Version]
- Little, J.S.; Aleissa, M.M.; Beluch, K.; Gonzalez-Bocco, I.H.; Marty, F.M.; Manne-Goehler, J.; Koo, S.; Hammond, S.P.; Jacobson, C.A. Low Incidence of Invasive Fungal Disease Following CD19 Chimeric Antigen Receptor T-Cell Therapy for Non-Hodgkin Lymphoma. Blood Adv. 2022, 6, 4821–4830. [Google Scholar] [CrossRef]
- Cordeiro, A.; Bezerra, E.D.; Hirayama, A.V.; Hill, J.A.; Wu, Q.V.; Voutsinas, J.; Sorror, M.L.; Turtle, C.J.; Maloney, D.G.; Bar, M. Late Events after Treatment with CD19-Targeted Chimeric Antigen Receptor Modified T Cells. Biol. Blood Marrow Transplant. 2020, 26, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Kurosawa, M.; Yonezumi, M.; Hashino, S.; Tanaka, J.; Nishio, M.; Kaneda, M.; Ota, S.; Koda, K.; Suzuki, N.; Yoshida, M.; et al. Epidemiology and Treatment Outcome of Invasive Fungal Infections in Patients with Hematological Malignancies. Int. J. Hematol. 2012, 96, 748–757. [Google Scholar] [CrossRef]
- Jantunen, E.; Salonen, J.; Juvonen, E.; Koivunen, E.; Siitonen, T.; Lehtinen, T.; Kuittinen, O.; Leppä, S.; Anttila, V.J.; Itälä, M.; et al. Invasive Fungal Infections in Autologous Stem Cell Transplant Recipients: A Nation-Wide Study of 1188 Transplanted Patients. Eur. J. Haematol. 2004, 73, 174–178. [Google Scholar] [CrossRef]
- Morgan, J.; Wannemuehler, K.A.; Marr, K.A.; Hadley, S.; Kontoyiannis, D.P.; Walsh, T.J.; Fridkin, S.K.; Pappas, P.G.; Warnock, D.W. Incidence of Invasive Aspergillosis Following Hematopoietic Stem Cell and Solid Organ Transplantation: Interim Results of a Prospective Multicenter Surveillance Program. Med. Mycol. 2005, 43, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Pagano, L.; Caira, M.; Nosari, A.; Van Lint, M.T.; Candoni, A.; Offidani, M.; Aloisi, T.; Irrera, G.; Bonini, A.; Picardi, M.; et al. Fungal Infections in Recipients of Hematopoietic Stem Cell Transplants: Results of the SEIFEM B-2004 Study—Sorveglianza Epidemiologica Infezioni Fungine Nelle Emopatie Maligne. Clin. Infect. Dis. 2007, 45, 1161–1170. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, A.; McLaughlin, L.; Wang, C.; Srivastava, D.K.; Shook, D.R.; Leung, W.; Hayden, R.T. Early Infections after Autologous Hematopoietic Stem Cell Transplantation in Children and Adolescents: The St. Jude Experience. Transpl. Infect. Dis. 2014, 16, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marr, K.A.; Carter, R.A.; Crippa, F.; Wald, A.; Corey, L. Epidemiology and Outcome of Mould Infections in Hematopoietic Stem Cell Transplant Recipients. Clin. Infect. Dis. 2002, 34, 909–917. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Meng, F.; Han, M.; Zhang, X.; Yu, L.; Huang, H.; Wu, D.; Ren, H.; Wang, C.; Shen, Z.; et al. Epidemiology, Management, and Outcome of Invasive Fungal Disease in Patients Undergoing Hematopoietic Stem Cell Transplantation in China: A Multicenter Prospective Observational Study. Biol. Blood Marrow Transplant. 2015, 21, 1117–1126. [Google Scholar] [CrossRef] [Green Version]
- Chu, S.; McCormick, T.S.; Lazarus, H.M.; Leal, L.O.; Ghannoum, M.A. Invasive Fungal Disease and the Immunocompromised Host Including Allogeneic Hematopoietic Cell Transplant Recipients: Improved Understanding and New Strategic Approach with Sargramostim. Clin. Immunol. 2021, 228, 108731. [Google Scholar] [CrossRef] [PubMed]
- Omer, A.K.; Ziakas, P.D.; Anagnostou, T.; Coughlin, E.; Kourkoumpetis, T.; McAfee, S.L.; Dey, B.R.; Attar, E.; Chen, Y.B.; Spitzer, T.R.; et al. Risk Factors for Invasive Fungal Disease after Allogeneic Hematopoietic Stem Cell Transplantation: A Single Center Experience. Biol. Blood Marrow Transplant. 2013, 19, 1190–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atoui, A.; Omeirat, N.; Fakhreddine, O.; El Alam, R.; Kanafani, Z.; Dalle, I.A.; Bazarbachi, A.; El-Cheikh, J.; Kanj, S.S. The Use of Voriconazole as Primary Prophylaxis for Invasive Fungal Infections in Patients Undergoing Allogeneic Stem Cell Transplantation: A Single Center’s Experience. J. Fungi 2021, 7, 925. [Google Scholar] [CrossRef]
- Mikulska, M.; Raiola, A.M.; Bruno, B.; Furfaro, E.; Van Lint, M.T.; Bregante, S.; Ibatici, A.; Del Bono, V.; Bacigalupo, A.; Viscoli, C. Risk Factors for Invasive Aspergillosis and Related Mortality in Recipients of Allogeneic SCT from Alternative Donors: An Analysis of 306 Patients. Bone Marrow Transplant. 2009, 44, 361–370. [Google Scholar] [CrossRef]
- Dvorak, C.C.; Steinbach, W.J.; Brown, J.M.Y.; Agarwal, R. Risks and Outcomes of Invasive Fungal Infections in Pediatric Patients Undergoing Allogeneic Hematopoietic Cell Transplantation. Bone Marrow Transplant. 2005, 36, 621–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakellari, I.; Gavriilaki, E.; Kaliou, M.; Mallouri, D.; Batsis, I.; Yannaki, E.; Smias, C.; Sotiropoulos, D.; Tsorlini, E.; Anagnostopoulos, A. Candida Is an Emerging Pathogen beyond the Neutropenic Period of Allogeneic Hematopoietic Cell Transplantation. Clin. Transplant. 2017, 31. [Google Scholar] [CrossRef] [PubMed]
- Lionakis, M.S.; Lewis, R.E.; Kontoyiannis, D.P. Breakthrough Invasive Mold Infections in the Hematology Patient: Current Concepts and Future Directions. Clin. Infect. Dis. 2018, 67, 1621–1630. [Google Scholar] [CrossRef] [PubMed]
- Harrison, N.; Mitterbauer, M.; Tobudic, S.; Kalhs, P.; Rabitsch, W.; Greinix, H.; Burgmann, H.; Willinger, B.; Presterl, E.; Forstner, C. Incidence and Characteristics of Invasive Fungal Diseases in Allogeneic Hematopoietic Stem Cell Transplant Recipients: A Retrospective Cohort Study. BMC Infect. Dis. 2015, 15, 584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.M.; Pei, X.Y.; Luo, Y.; Tan, Y.M.; Tie, R.X.; He, J.S.; Zheng, W.Y.; Zhang, J.; Cai, Z.; Lin, M.F.; et al. Invasive Fungal Infection in Allogeneic Hematopoietic Stem Cell Transplant Recipients: Single Center Experiences of 12 Years. J. Zhejiang Univ. Sci. B 2015, 16, 796–804. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Kim, K.; Jang, J.H.; Kim, S.J.; Kim, W.S.; Chung, D.R.; Kang, C.I.; Peck, K.R.; Jung, C.W. Randomized Trial of Micafungin versus Fluconazole as Prophylaxis against Invasive Fungal Infections in Hematopoietic Stem Cell Transplant Recipients. J. Infect. 2016, 73, 496–505. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | AlloHCT with IFD (n = 52) | AlloHCT Recipients without IFD (n = 421) | p-Value |
|---|---|---|---|
| Hematological disease, n | 0.324 | ||
| AML | 26 | 216 | |
| ALL | 18 | 87 | |
| MDS | 4 | 32 | |
| CML | 2 | 25 | |
| NHL | 1 | 32 | |
| PMF | 1 | 19 | |
| Other | 10 | ||
| Type of donor, n | 0.012 | ||
| Graft from a matched sibling donor | 10 | 232 | |
| Graft from a matched unrelated donor | 31 | 164 | |
| Graft from an alternative donor | 11 | 25 | |
| HCT, n | 0.127 | ||
| HCT in complete remission in CR | 41 | 369 | |
| HCT in active disease | 11 | 52 |
| IFD | Possible | Probable | Proven |
|---|---|---|---|
| Patients (n) | 31 | 11 | 10 |
| Median post-transplantation day | 112 | 154 | 226 |
| Positive Galactomannan (n) | 0 | 5 | 3 |
| Positive cultures (n) | 0 | 6 | 7 |
| Histopathological evidence | 0 | 0 | 3 |
| Second IFD episode (n) | 0 | 1 | 2 |
| Bacterial Infections | Patients (n) | Viral Infections | Patients (n) |
|---|---|---|---|
| Blood | Blood CMV EBV Influenza A | 8 9 1 | |
| Staphyloccocus hominis | 1 | ||
| Staphylococcus haemolyticus | 1 | ||
| Enteroccus faecium | 1 | ||
| Pseudomonas aeruginosa | 2 | ||
| Klebsiella pneumoniae | 2 | ||
| Eserichia coli | 1 | ||
| Sphingomonas paucimobilis | 1 | ||
| Sputum | |||
| Enterococcus faecium | 1 | ||
| Klebsiella pneumoniae | 3 | ||
| Pseudomonas aeruginosa | 3 | ||
| Pneumocystis jirovecii | 1 | ||
| Stools | |||
| Klebsiella pneumoniae | 2 | ||
| Urine | |||
| Klebsiella pneumoniae | 1 | ||
| 20 | 17 * |
| Fungal Infections | Patients (n) |
|---|---|
| Candida spp. | 9 |
| Fusarium | 2 |
| Aspergillus | 2 |
| Mucormycosis | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavriilaki, E.; Dolgyras, P.; Dimou-Mpesikli, S.; Poulopoulou, A.; Evangelidis, P.; Evangelidis, N.; Demosthenous, C.; Zachrou, E.; Siasios, P.; Mallouri, D.; et al. Risk Factors, Prevalence, and Outcomes of Invasive Fungal Disease Post Hematopoietic Cell Transplantation and Cellular Therapies: A Retrospective Monocenter Real-Life Analysis. Cancers 2023, 15, 3529. https://doi.org/10.3390/cancers15133529
Gavriilaki E, Dolgyras P, Dimou-Mpesikli S, Poulopoulou A, Evangelidis P, Evangelidis N, Demosthenous C, Zachrou E, Siasios P, Mallouri D, et al. Risk Factors, Prevalence, and Outcomes of Invasive Fungal Disease Post Hematopoietic Cell Transplantation and Cellular Therapies: A Retrospective Monocenter Real-Life Analysis. Cancers. 2023; 15(13):3529. https://doi.org/10.3390/cancers15133529
Chicago/Turabian StyleGavriilaki, Eleni, Panagiotis Dolgyras, Sotiria Dimou-Mpesikli, Aikaterini Poulopoulou, Paschalis Evangelidis, Nikolaos Evangelidis, Christos Demosthenous, Evangelia Zachrou, Panagiotis Siasios, Despina Mallouri, and et al. 2023. "Risk Factors, Prevalence, and Outcomes of Invasive Fungal Disease Post Hematopoietic Cell Transplantation and Cellular Therapies: A Retrospective Monocenter Real-Life Analysis" Cancers 15, no. 13: 3529. https://doi.org/10.3390/cancers15133529