
Tumor Margin Contains Prognostic Information: Radiomic Margin Characteristics Analysis in Lung Adenocarcinoma Patients


 , ,
, ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
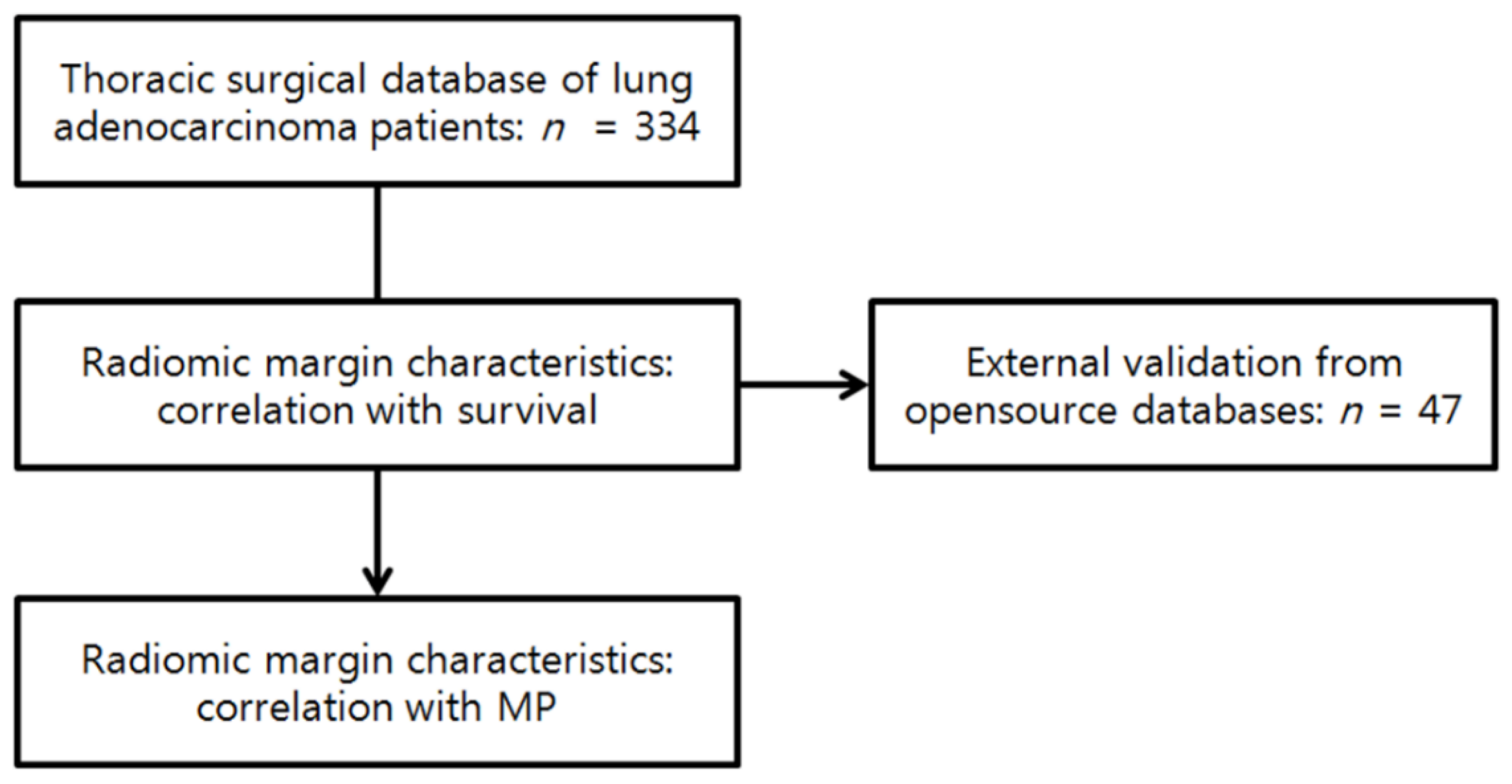
2.1. Patients
2.2. Pathology Review
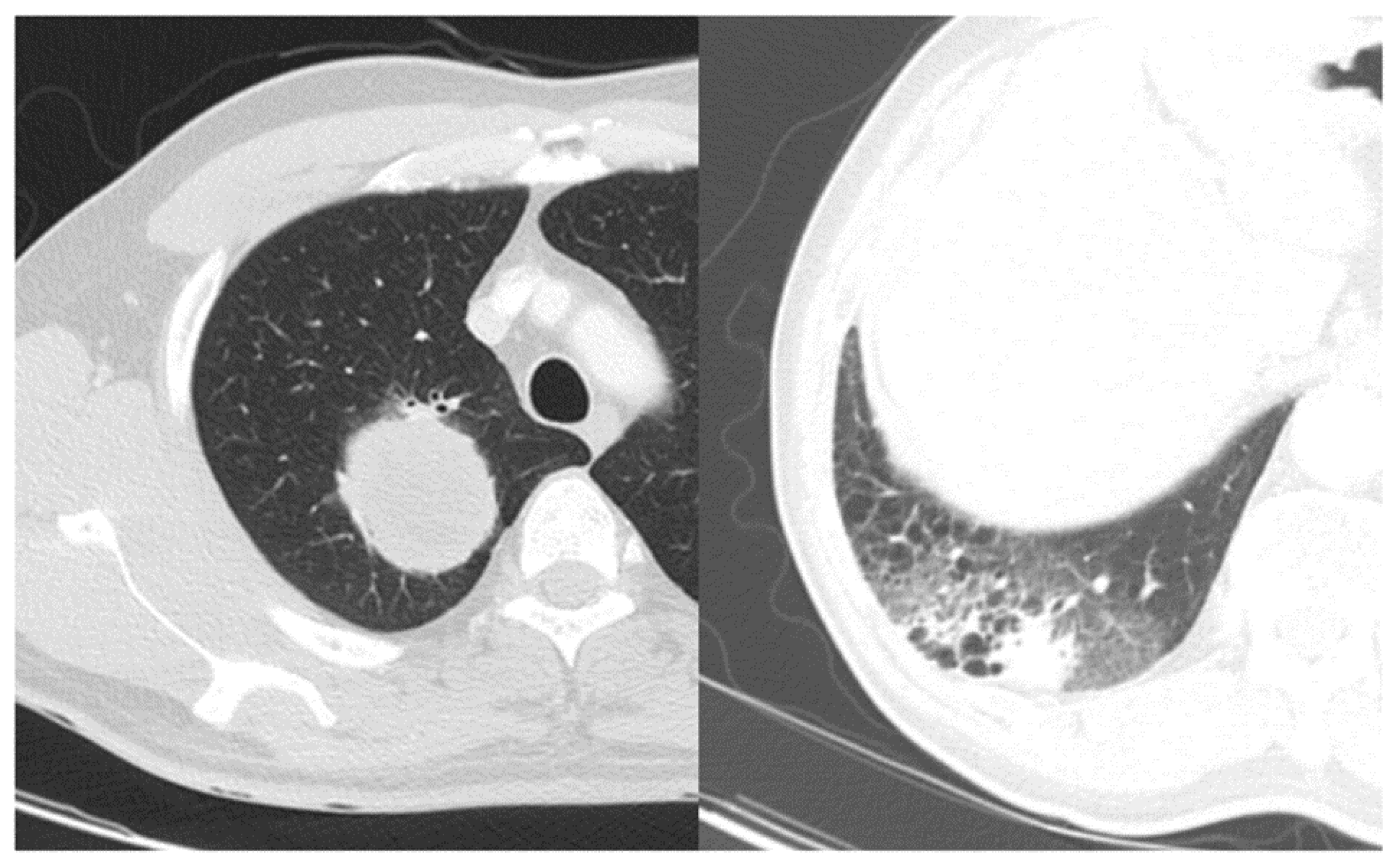
2.3. Features of Radiomic Margin Characteristics
2.4. Statistical Analysis
3. Results
3.1. Stability of Radiomic Margin Characteristics
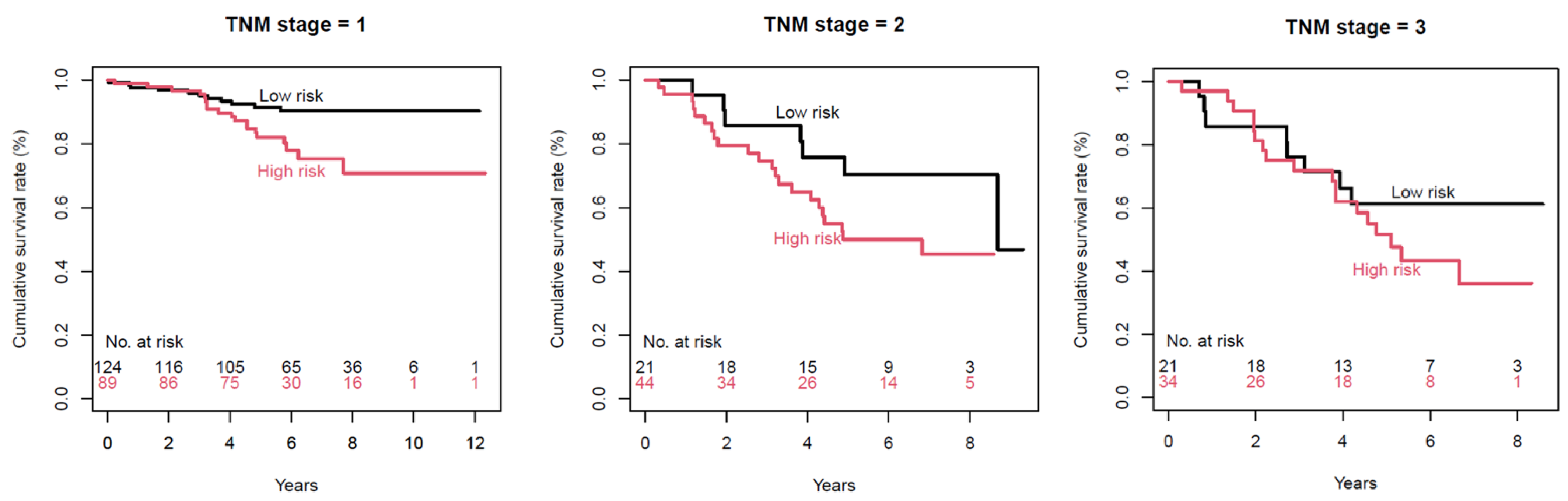
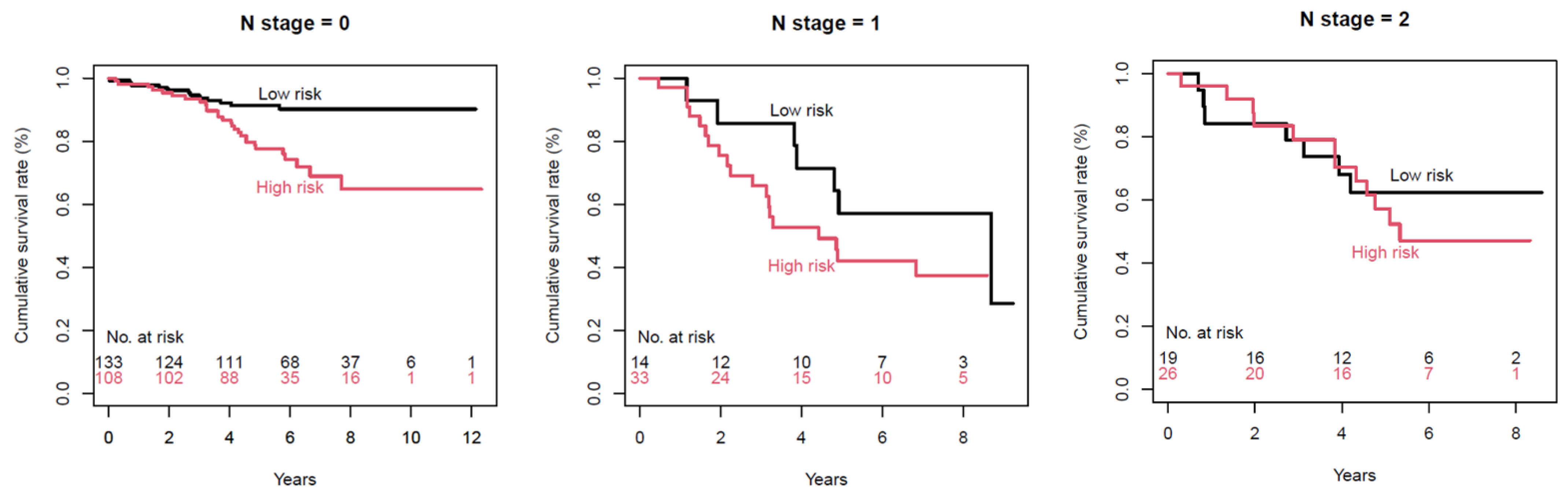
3.2. Association with Survival
3.3. External Validation of Survival
3.4. Association with the MP Pattern
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balkwill, F.R.; Capasso, M.; Hagemann, T. The tumor microenvironment at a glance. J. Cell Sci. 2012, 125, 5591–5596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanahan, D.; Coussens, L.M. Accessories to the crime: Functions of cells recruited to the tumor microenvironment. Cancer Cell 2012, 21, 309–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quail, D.F.; Joyce, J.A. Microenvironmental regulation of tumor progression and metastasis. Nat. Med. 2013, 19, 1423–1437. [Google Scholar] [CrossRef]
- Wu, T.; Dai, Y. Tumor microenvironment and therapeutic response. Cancer Lett. 2017, 387, 61–68. [Google Scholar] [CrossRef]
- Hui, L.; Chen, Y. Tumor microenvironment: Sanctuary of the devil. Cancer Lett. 2015, 368, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Roh, M.S.; Lee, J.I.; Choi, P.J.; Hong, Y.S. Relationship between micropapillary component and micrometastasis in the regional lymph nodes of patients with stage I lung adenocarcinoma. Histopathology 2004, 45, 580–586. [Google Scholar] [CrossRef]
- Carter, B.W.; Halpenny, D.F.; Ginsberg, M.S.; Papadimitrakopoulou, V.A.; de Groot, P.M. Immunotherapy in Non-Small Cell Lung Cancer Treatment: Current Status and the Role of Imaging. J. Thorac. Imaging 2017, 32, 300–312. [Google Scholar] [CrossRef]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Lee, G.; Park, H.; Sohn, I.; Lee, S.H.; Song, S.H.; Kim, H.; Lee, K.S.; Shim, Y.M.; Lee, H.Y. Comprehensive Computed Tomography Radiomics Analysis of Lung Adenocarcinoma for Prognostication. Oncologist 2018, 23, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.Y.; Lee, S.W.; Lee, K.S.; Jeong, J.Y.; Choi, J.Y.; Kwon, O.J.; Song, S.H.; Kim, E.Y.; Kim, J.; Shim, Y.M. Role of CT and PET Imaging in Predicting Tumor Recurrence and Survival in Patients with Lung Adenocarcinoma: A Comparison with the International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society Classification of Lung Adenocarcinoma. J. Thorac. Oncol. 2015, 10, 1785–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganeshan, B.; Goh, V.; Mandeville, H.C.; Ng, Q.S.; Hoskin, P.J.; Miles, K.A. Non-small cell lung cancer: Histopathologic correlates for texture parameters at CT. Radiology 2013, 266, 326–336. [Google Scholar] [CrossRef]
- Ganeshan, B.; Panayiotou, E.; Burnand, K.; Dizdarevic, S.; Miles, K. Tumour heterogeneity in non-small cell lung carcinoma assessed by CT texture analysis: A potential marker of survival. Eur. Radiol. 2012, 22, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Win, T.; Miles, K.A.; Janes, S.M.; Ganeshan, B.; Shastry, M.; Endozo, R.; Meagher, M.; Shortman, R.I.; Wan, S.; Kayani, I.; et al. Tumor heterogeneity and permeability as measured on the CT component of PET/CT predict survival in patients with non-small cell lung cancer. Clin. Cancer Res. 2013, 19, 3591–3599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grove, O.; Berglund, A.E.; Schabath, M.B.; Aerts, H.J.; Dekker, A.; Wang, H.; Velazquez, E.R.; Lambin, P.; Gu, Y.; Balagurunathan, Y.; et al. Quantitative computed tomographic descriptors associate tumor shape complexity and intratumor heterogeneity with prognosis in lung adenocarcinoma. PLoS ONE 2015, 10, e0118261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yip, S.S.F.; Liu, Y.; Parmar, C.; Li, Q.; Liu, S.; Qu, F.; Ye, Z.; Gillies, R.J.; Aerts, H. Associations between radiologist-defined semantic and automatically computed radiomic features in non-small cell lung cancer. Sci. Rep. 2017, 7, 3519. [Google Scholar] [CrossRef]
- Lee, G.; Lee, H.Y.; Jeong, J.Y.; Han, J.; Cha, M.J.; Lee, K.S.; Kim, J.; Shim, Y.M. Clinical impact of minimal micropapillary pattern in invasive lung adenocarcinoma: Prognostic significance and survival outcomes. Am. J. Surg. Pathol. 2015, 39, 660–666. [Google Scholar] [CrossRef]
- Maeda, R.; Isowa, N.; Onuma, H.; Miura, H.; Harada, T.; Touge, H.; Tokuyasu, H.; Kawasaki, Y. Lung adenocarcinomas with micropapillary components. Gen. Thorac. Cardiovasc. Surg. 2009, 57, 534–539. [Google Scholar] [CrossRef]
- Miyoshi, T.; Satoh, Y.; Okumura, S.; Nakagawa, K.; Shirakusa, T.; Tsuchiya, E.; Ishikawa, Y. Early-stage lung adenocarcinomas with a micropapillary pattern, a distinct pathologic marker for a significantly poor prognosis. Am. J. Surg. Pathol. 2003, 27, 101–109. [Google Scholar] [CrossRef]
- Nitadori, J.; Bograd, A.J.; Kadota, K.; Sima, C.S.; Rizk, N.P.; Morales, E.A.; Rusch, V.W.; Travis, W.D.; Adusumilli, P.S. Impact of micropapillary histologic subtype in selecting limited resection vs lobectomy for lung adenocarcinoma of 2cm or smaller. J. Natl. Cancer Inst. 2013, 105, 1212–1220. [Google Scholar] [CrossRef] [PubMed]
- Bains, S.; Eguchi, T.; Warth, A.; Yeh, Y.C.; Nitadori, J.I.; Woo, K.M.; Chou, T.Y.; Dienemann, H.; Muley, T.; Nakajima, J.; et al. Procedure-Specific Risk Prediction for Recurrence in Patients Undergoing Lobectomy or Sublobar Resection for Small (</=2 cm) Lung Adenocarcinoma: An International Cohort Analysis. J. Thorac. Oncol. 2019, 14, 72–86. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Yang, J.; Lu, M. Micropapillary Predominant Lung Adenocarcinoma in Stage IA Benefits from Adjuvant Chemotherapy. Ann. Surg. Oncol. 2020, 27, 2051–2060. [Google Scholar] [CrossRef]
- Song, S.H.; Park, H.; Lee, G.; Lee, H.Y.; Sohn, I.; Kim, H.S.; Lee, S.H.; Jeong, J.Y.; Kim, J.; Lee, K.S.; et al. Imaging Phenotyping Using Radiomics to Predict Micropapillary Pattern within Lung Adenocarcinoma. J. Thorac. Oncol. 2017, 12, 624–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Subashi, E.; Yin, F.F.; Chang, Z. Dynamic fractal signature dissimilarity analysis for therapeutic response assessment using dynamic contrast-enhanced MRI. Med. Phys. 2016, 43, 1335–1347. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.; Grossmann, P.; Tan, Y.; Oxnard, G.R.; Rizvi, N.; Schwartz, L.H.; Zhao, B. Defining a Radiomic Response Phenotype: A Pilot Study using targeted therapy in NSCLC. Sci. Rep. 2016, 6, 33860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennon, F.E.; Cianci, G.C.; Cipriani, N.A.; Hensing, T.A.; Zhang, H.J.; Chen, C.T.; Murgu, S.D.; Vokes, E.E.; Vannier, M.W.; Salgia, R. Lung cancer-a fractal viewpoint. Nat. Rev. Clin. Oncol. 2015, 12, 664–675. [Google Scholar] [CrossRef] [Green Version]
- Altorki, N.K.; Markowitz, G.J.; Gao, D.; Port, J.L.; Saxena, A.; Stiles, B.; McGraw, T.; Mittal, V. The lung microenvironment: An important regulator of tumour growth and metastasis. Nat. Rev. Cancer 2019, 19, 9–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, T.; Tomoda, Y.; Watanabe, H.; Nakata, H.; Kasai, T.; Hashimoto, H.; Kodate, M.; Osaki, T.; Yasumoto, K. Peripheral lung adenocarcinoma: Correlation of thin-section CT findings with histologic prognostic factors and survival. Radiology 2001, 220, 803–809. [Google Scholar] [CrossRef]
- O’Donovan, P.B. The radiologic appearance of lung cancer. Oncology (Williston Park) 1997, 11, 1387–1402, discussion 1402–1404. [Google Scholar] [PubMed]
- Zwirewich, C.V.; Vedal, S.; Miller, R.R.; Muller, N.L. Solitary pulmonary nodule: High-resolution CT and radiologic-pathologic correlation. Radiology 1991, 179, 469–476. [Google Scholar] [CrossRef]
- Takashima, S.; Maruyama, Y.; Hasegawa, M.; Yamanda, T.; Honda, T.; Kadoya, M.; Sone, S. Prognostic significance of high-resolution CT findings in small peripheral adenocarcinoma of the lung: A retrospective study on 64 patients. Lung Cancer 2002, 36, 289–295. [Google Scholar] [CrossRef]
- Wang, H.; Schabath, M.B.; Liu, Y.; Berglund, A.E.; Bloom, G.C.; Kim, J.; Stringfield, O.; Eikman, E.A.; Klippenstein, D.L.; Heine, J.J.; et al. Semiquantitative Computed Tomography Characteristics for Lung Adenocarcinoma and Their Association With Lung Cancer Survival. Clin. Lung Cancer 2015, 16, e141–e163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, K.A.; Ganeshan, B.; Hayball, M.P. CT texture analysis using the filtration-histogram method: What do the measurements mean? Cancer Imaging 2013, 13, 400–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weidner, N.; Semple, J.P.; Welch, W.R.; Folkman, J. Tumor angiogenesis and metastasis--correlation in invasive breast carcinoma. N. Engl. J. Med. 1991, 324, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Meert, A.P.; Paesmans, M.; Martin, B.; Delmotte, P.; Berghmans, T.; Verdebout, J.M.; Lafitte, J.J.; Mascaux, C.; Sculier, J.P. The role of microvessel density on the survival of patients with lung cancer: A systematic review of the literature with meta-analysis. Br. J. Cancer 2002, 87, 694–701. [Google Scholar] [CrossRef] [Green Version]
- Parra, E.R.; Behrens, C.; Rodriguez-Canales, J.; Lin, H.; Mino, B.; Blando, J.; Zhang, J.; Gibbons, D.L.; Heymach, J.V.; Sepesi, B.; et al. Image Analysis-based Assessment of PD-L1 and Tumor-Associated Immune Cells Density Supports Distinct Intratumoral Microenvironment Groups in Non-small Cell Lung Carcinoma Patients. Clin. Cancer Res. 2016, 22, 6278–6289. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef] [Green Version]
- Miyoshi, T.; Shirakusa, T.; Ishikawa, Y.; Iwasaki, A.; Shiraishi, T.; Makimoto, Y.; Iwasaki, H.; Nabeshima, K. Possible mechanism of metastasis in lung adenocarcinomas with a micropapillary pattern. Pathol. Int. 2005, 55, 419–424. [Google Scholar] [CrossRef]
- Kadota, K.; Nitadori, J.; Sima, C.S.; Ujiie, H.; Rizk, N.P.; Jones, D.R.; Adusumilli, P.S.; Travis, W.D. Tumor Spread through Air Spaces is an Important Pattern of Invasion and Impacts the Frequency and Location of Recurrences after Limited Resection for Small Stage I Lung Adenocarcinomas. J. Thorac. Oncol. 2015, 10, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [Green Version]
- Warth, A.; Muley, T.; Kossakowski, C.A.; Goeppert, B.; Schirmacher, P.; Dienemann, H.; Weichert, W. Prognostic Impact of Intra-alveolar Tumor Spread in Pulmonary Adenocarcinoma. Am. J. Surg. Pathol. 2015, 39, 793–801. [Google Scholar] [CrossRef] [Green Version]
- Chao, L.; Yi-Sheng, H.; Yu, C.; Li-Xu, Y.; Xin-Lan, L.; Dong-Lan, L.; Jie, C.; Yi-Lon, W.; Hui, L.Y. Relevance of EGFR mutation with micropapillary pattern according to the novel IASLC/ATS/ERS lung adenocarcinoma classification and correlation with prognosis in Chinese patients. Lung Cancer 2014, 86, 164–169. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Shape | LoG Filtering | 2D Shape | Fractal-Based |
|---|---|---|---|---|
| Total number of features in each category | 7 | 63 | 3 | 3 |
| Range of ICC | 0.904–0.994 | 0.607–1.000 | 0.868–0.958 | 0.935–0.955 |
| Number of features with ICC ≥0.8 | 7 (100%) | 61 (96.8%) | 3 (100%) | 3 (100%) |
| Number of features with ICC 0.6–0.799 | 0 (0%) | 2 (3.2%) | 0 (0%) | 0 (0%) |
| Selected Variables | Reference | p-Value | OR | 95% CI |
|---|---|---|---|---|
| MP (Predominant cell non-solid) | 0.022 | 1.959 | 1.100–3.490 | |
| MP (Predominant cell is solid) | 0.010 | 2.539 | 1.253–5.148 | |
| Moderately differentiated | Well-differentiated | 0.023 | 3.946 | 1.208–12.890 |
| Poorly differentiated | Well-differentiated | 0.036 | 4.110 | 1.098–15.389 |
| Sex | Male | 0.035 | 1.669 | 1.036–2.688 |
| Age | <0.001 | 1.047 | 1.021–1.073 | |
| Size | 0.019 | 1.219 | 1.034–1.438 | |
| Convexity | 0.004 | 0.078 | 0.013–0.447 | |
| LoG Kurtosis 3 | 0.034 | 1.085 | 1.006–1.170 | |
| Roundness factor | 0.009 | 2.384 | 1.246–4.561 |
| Selected Variables | Reference | p-Value | OR | 95% CI |
|---|---|---|---|---|
| MP (Predominant cell non-solid) | 0.018 | 1.985 | 1.122–3.512 | |
| MP (Predominant cell is solid) | 0.006 | 2.730 | 1.335–5.583 | |
| Moderately differentiated | Well-differentiated | 0.045 | 3.317 | 1.026–10.731 |
| Poorly differentiated | Well-differentiated | 0.074 | 3.299 | 0.891–12.214 |
| Sex | Male | 0.033 | 1.677 | 1.043–2.698 |
| Age | <0.001 | 1.048 | 1.023–1.073 | |
| Size | 0.004 | 1.228 | 1.066–1.414 |
| Variable | p-Value | OR | 95% CI |
|---|---|---|---|
| (Intercept) | 0.059 | ||
| Sphericity value | 0.033 | 0.071 | 0.006–0.813 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, G.; Park, H.; Lee, H.Y.; Ahn, J.H.; Sohn, I.; Lee, S.-H.; Kim, J. Tumor Margin Contains Prognostic Information: Radiomic Margin Characteristics Analysis in Lung Adenocarcinoma Patients. Cancers 2021, 13, 1676. https://doi.org/10.3390/cancers13071676
Lee G, Park H, Lee HY, Ahn JH, Sohn I, Lee S-H, Kim J. Tumor Margin Contains Prognostic Information: Radiomic Margin Characteristics Analysis in Lung Adenocarcinoma Patients. Cancers. 2021; 13(7):1676. https://doi.org/10.3390/cancers13071676
Chicago/Turabian StyleLee, Geewon, Hyunjin Park, Ho Yun Lee, Joong Hyun Ahn, Insuk Sohn, Seung-Hak Lee, and Jhingook Kim. 2021. "Tumor Margin Contains Prognostic Information: Radiomic Margin Characteristics Analysis in Lung Adenocarcinoma Patients" Cancers 13, no. 7: 1676. https://doi.org/10.3390/cancers13071676