
An Automatic Detection and Localization of Mammographic Microcalcifications ROI with Multi-Scale Features Using the Radiomics Analysis Approach

 ,
,  , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Related Works
2.1. Mammography Characterization through Conventional Machine Learning Models
2.2. Mammography Characterization through Conventional Deep Learning Models
3. Materials and Methods
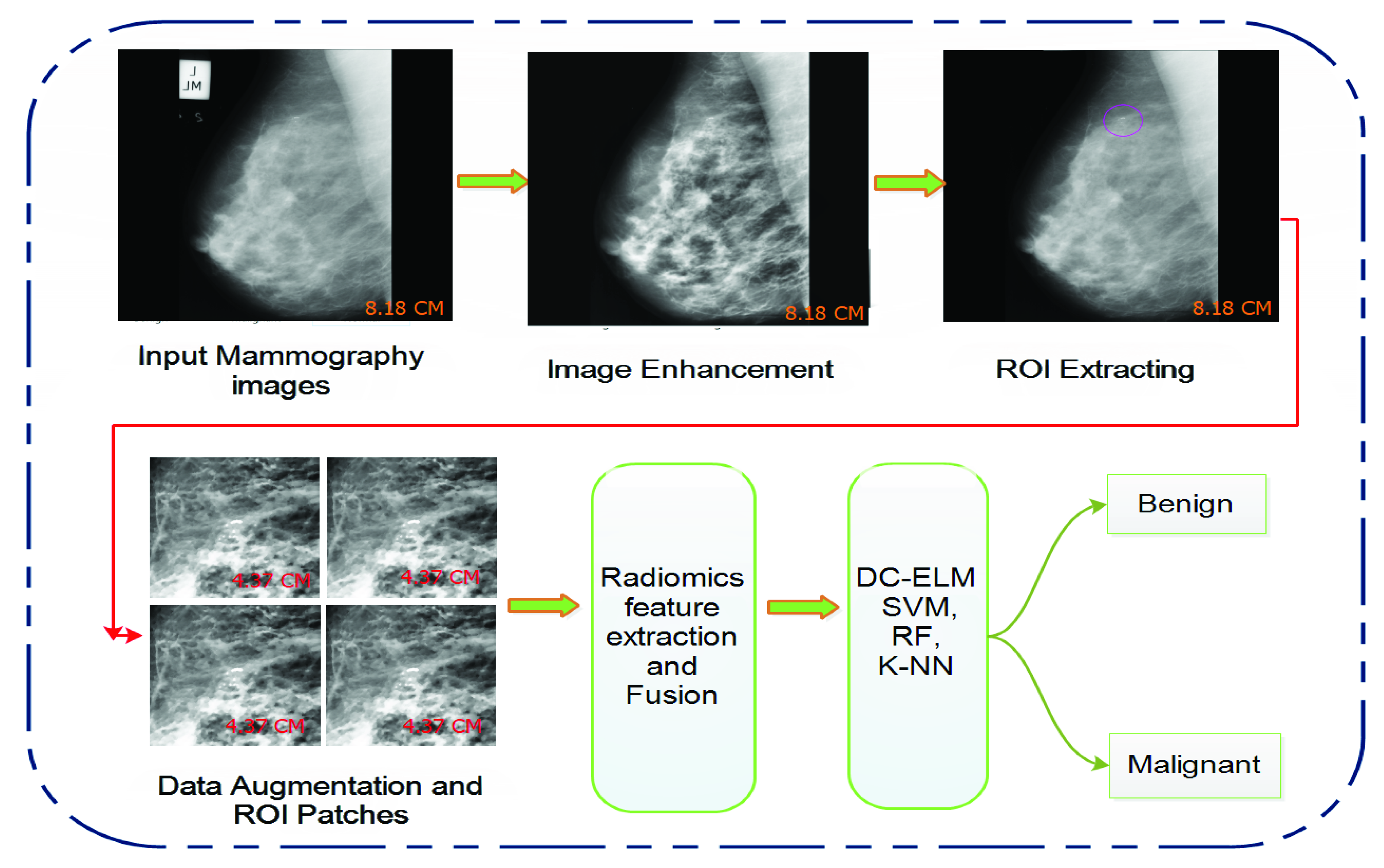
- We created an efficient strategy for identifying and categorizing MC mammograms using a radiomics analysis approach. It is easy to implement, convincing, well-defined, and overcomes small and large feature search space optimization issues.
- The optimum feature collections from the input data were achieved using wavelet analysis, which suppresses redundant and superfluous characteristics and prioritizes feature significance.
- This study combined wavelet transform and the top-hat operator to filter out seed regions of calcification spots, resulting in a significant reduction in false detection and improved detection accuracy.
- The effectiveness of the proposed feature learning model is compared to that of existing strategies. The mammogram dataset was validated using well-established clinical validation techniques.
3.1. Dataset
3.2. Image Preprocessing and Data Augmentation
3.3. Wavelet Analysis
3.4. Mathematical Morphology
3.5. Top-Hat Algorithm
3.6. Radiomics Based Proposed Method

3.7. Standard Classifiers
3.8. Performance Measures
4. Results and Analysis
4.1. Microcalcification-Based ROI Detection and Segmentation
4.2. Microcalcification-Based Feature Extraction and Classification
4.3. Comparative Analysis with Conventional Studies
5. Discussions
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahmood, T.; Li, J.; Pei, Y.; Akhtar, F.; Imran, A.; Rehman, K.U. A Brief Survey on Breast Cancer Diagnostic With Deep Learning Schemes Using Multi-Image Modalities. IEEE Access 2020, 8, 165779–165809. [Google Scholar] [CrossRef]
- Ginsburg, O.; Yip, C.H.; Brooks, A.; Cabanes, A.; Caleffi, M.; Dunstan Yataco, J.A.; Gyawali, B.; McCormack, V.; McLaughlin de Anderson, M.; Mehrotra, R.; et al. Breast cancer early detection: A phased approach to implementation. Cancer 2020, 126, 2379–2393. [Google Scholar] [CrossRef] [PubMed]
- Maitra, I.K.; Nag, S.; Bandyopadhyay, S.K. Technique for preprocessing of digital mammogram. Comput. Methods Progr. Biomed. 2012, 107, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Balleyguier, C.; Ayadi, S.; Van Nguyen, K.; Vanel, D.; Dromain, C.; Sigal, R. BIRADS classification in mammogram. Eur. J. Radiol. 2007, 61, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Liberman, L.; Menell, J.H. Breast imaging reporting and data system (BI-RADS). Radiol. Clin. 2002, 40, 409–430. [Google Scholar] [CrossRef]
- Hadi, Q.; Masroor, I.; Hussain, Z. Mammographic Criteria for Determining the Diagnostic Accuracy of Microcalcifications in the Detection of Malignant Breast Lesions. Cureus 2019, 11, e5919. [Google Scholar] [CrossRef] [Green Version]
- Diyana, W.M.; Besar, R. Automated methods in clustered microcalcifications detection module of a CAD system. J. Mech. Med. Biol. 2003, 3, 247–260. [Google Scholar] [CrossRef]
- Lee, S.J.; Chen, T.; Yu, L.; Lai, C.H. Image classification based on the boost convolutional neural network. IEEE Access 2018, 6, 12755–12768. [Google Scholar] [CrossRef]
- Panda, R.N.; Panigrahi, B.K.; Patro, M.R. Feature extraction for classification of microcalcifications and mass lesions in mammograms. IJCSNS Int. J. Comput. Sci. Netw. Secur. 2009, 9, 255–265. [Google Scholar]
- Chen, Y.; Zhang, Q.; Wu, Y.; Liu, B.; Wang, M.; Lin, Y. Fine-tuning ResNet for breast cancer classification from mammogram. In The International Conference on Healthcare Science and Engineering; Springer: Berlin/Heidelberg, Germany, 2018; pp. 83–96. [Google Scholar]
- Craft, M.; Bicknell, A.M.; Hazan, G.J.; Flegg, K.M. Microcalcifications detected as an abnormality on screening mammogram: Outcomes and followup over a five-year period. Int. J. Breast Cancer 2013, 2013, 458540. [Google Scholar] [CrossRef]
- Li, M.; Zhu, L.; Zhou, G.; He, J.; Jiang, Y.; Chen, Y. Predicting the pathological status of mammographic microcalcifications via a radiomics approach. Intell. Med. 2021, 1, 1–8. [Google Scholar]
- Elezaby, M.; Li, G.; Bhargavan-Chatfield, M.; Burnside, E.S.; DeMartini, W.B. ACR BI-RADS assessment category 4 subdivisions in diagnostic mammogram: Utilization and outcomes in the national mammogram database. Radiology 2018, 287, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Xu, Z. Feature extraction by PCA and diagnosis of breast tumors using SVM with DE-based parameter tuning. Int. J. Mach. Learn. Cybern. 2019, 10, 591–601. [Google Scholar] [CrossRef]
- Jiang, Y.; Metz, C.E.; Nishikawa, R.M.; Schmidt, R.A. Comparison of independent double readings and computer-aided diagnosis (CAD) for the diagnosis of breast calcifications. Acad. Radiol. 2006, 13, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.T.; Lim, V.; Vu, H.X.; Chim, R.; Weise, E.; Liu, J.; Bradley, W.G.; Comstock, C.E. Improved cancer detection using artificial intelligence: A retrospective evaluation of missed cancers on mammogram. J. Digit. Imaging 2019, 32, 625–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valvano, G.; Santini, G.; Martini, N.; Ripoli, A.; Iacconi, C.; Chiappino, D.; Della Latta, D. Convolutional neural networks for the segmentation of microcalcification in mammogram imaging. J. Healthc. Eng. 2019, 2019, 9360941. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Huang, Q.; Rong, W.; Song, Y.; Li, J.; Wang, J.; Chen, J.; Li, L. Breast microcalcification diagnosis using deep convolutional neural network from digital mammograms. Comput. Math. Methods Med. 2019, 2019, 2717454. [Google Scholar] [CrossRef] [PubMed]
- Gallardo-Caballero, R.; García-Orellana, C.; García-Manso, A.; González-Velasco, H.; Macías-Macías, M. Independent component analysis to detect clustered microcalcification breast cancers. Sci. World J. 2012, 2012, 540457. [Google Scholar] [CrossRef] [Green Version]
- Lei, C.q.; Wei, W.; Liu, Z.y.; Xiong, Q.Q.; Yang, C.Q.; Zhu, T.; Zhang, L.L.; Yang, M.; Tian, J.; Wang, K. Radiomics analysis for pathological classification prediction in BI-RADS category 4 mammographic calcifications. J. Clin. Oncol. 2019, 37, 1–8. [Google Scholar] [CrossRef]
- Morin, O.; Vallières, M.; Jochems, A.; Woodruff, H.C.; Valdes, G.; Braunstein, S.E.; Wildberger, J.E.; Villanueva-Meyer, J.E.; Kearney, V.; Yom, S.S.; et al. A deep look into the future of quantitative imaging in oncology: A statement of working principles and proposal for change. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1074–1082. [Google Scholar] [CrossRef]
- Wang, J.; Yang, X.; Cai, H.; Tan, W.; Jin, C.; Li, L. Discrimination of breast cancer with microcalcifications on mammogram by deep learning. Sci. Rep. 2016, 6, 27327. [Google Scholar] [CrossRef] [PubMed]
- Beham, M.P.; Tamilselvi, R.; Roomi, S.M.; Nagaraj, A. Accurate Classification of Cancer in Mammogram Images. In Innovations in Electronics and Communication Engineering; Springer: Berlin/Heidelberg, Germany, 2019; pp. 71–77. [Google Scholar]
- Obaidullah, S.M.; Ahmed, S.; Gonçalves, T.; Rato, L. RMID: A novel and efficient image descriptor for mammogram mass classification. In Proceedings of the Information Technology, Systems Research and Computational Physics, Cracow, Poland, 2–5 July 2018; pp. 229–240. [Google Scholar]
- Sun, D.; Wang, M.; Li, A. A multimodal deep neural network for human breast cancer prognosis prediction by integrating multi-dimensional data. IEEE/ACM Trans. Comput. Biol. Bioinform. 2018, 16, 841–850. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Martins, L.; Junior, G.B.; Silva, A.C.; de Paiva, A.C.; Gattass, M. Detection of masses in digital mammograms using K-means and support vector machine. ELCVIA Electron. Lett. Comput. Vis. Image Anal. 2009, 1, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Loizidou, K.; Skouroumouni, G.; Nikolaou, C.; Pitris, C. An automated breast micro-calcification detection and classification technique using temporal subtraction of mammograms. IEEE Access 2020, 8, 52785–52795. [Google Scholar] [CrossRef]
- Gaikwad, V.J. Detection of breast cancer in mammogram using support vector machine. Int. J. Sci. Eng. Res. 2015, 10, 19–21. [Google Scholar]
- Chakraborty, J.; Midya, A.; Mukhopadhyay, S.; Rangayyan, R.M.; Sadhu, A.; Singla, V.; Khandelwal, N. Computer-aided detection of mammographic masses using hybrid region growing controlled by multilevel thresholding. J. Med. Biol. Eng. 2019, 39, 352–366. [Google Scholar] [CrossRef]
- Liu, N.; Qi, E.S.; Xu, M.; Gao, B.; Liu, G.Q. A novel intelligent classification model for breast cancer diagnosis. Inf. Process. Manag. 2019, 56, 609–623. [Google Scholar] [CrossRef]
- Elmoufidi, A.; El Fahssi, K.; Jai-Andaloussi, S.; Sekkaki, A.; Gwenole, Q.; Lamard, M. Anomaly classification in digital mammogram based on multiple-instance learning. IET Image Process. 2018, 12, 320–328. [Google Scholar] [CrossRef]
- Wang, Z.; Li, M.; Wang, H.; Jiang, H.; Yao, Y.; Zhang, H.; Xin, J. Breast cancer detection using extreme learning machine based on feature fusion with CNN deep features. IEEE Access 2019, 7, 105146–105158. [Google Scholar] [CrossRef]
- Soulami, K.B.; Saidi, M.N.; Tamtaoui, A. A cad system for the detection of abnormalities in the mammograms using the metaheuristic algorithm particle swarm optimization (pso). In International Symposium on Ubiquitous Networking; Springer: Berlin/Heidelberg, Germany, 2016; pp. 505–517. [Google Scholar]
- Guan, Y.; Wang, X.; Li, H.; Zhang, Z.; Chen, X.; Siddiqui, O.; Nehring, S.; Huang, X. Detecting Asymmetric Patterns and Localizing Cancers on Mammograms. Patterns 2020, 1, 100106. [Google Scholar] [CrossRef]
- Rouhi, R.; Jafari, M. Classification of benign and malignant breast tumors based on hybrid level set segmentation. Expert Syst. Appl. 2016, 46, 45–59. [Google Scholar] [CrossRef]
- Rizzi, M.; D’Aloia, M.; Castagnolo, B. Computer aided detection of microcalcifications in digital mammograms adopting a wavelet decomposition. Integr. Comput.-Aided Eng. 2009, 16, 91–103. [Google Scholar] [CrossRef]
- Yu, S.N.; Huang, Y.K. Detection of microcalcifications in digital mammograms using combined model-based and statistical textural features. Expert Syst. Appl. 2010, 37, 5461–5469. [Google Scholar] [CrossRef]
- Papadopoulosa, A.; Fotiadisb, D.I.; Likasb, A. An automatic microcalcification detection system based on a hybrid neural network classifier. Artif. Intell. Med. 2002, 25, 149–167. [Google Scholar] [CrossRef] [Green Version]
- Elter, M.; Held, C. Semiautomatic segmentation for the computer aided diagnosis of clustered microcalcifications. Proc. SPIE Int. Soc. Opt. Eng. 2008, 6915, 691524. [Google Scholar]
- Suckling, J.P. The mammographic image analysis society digital mammogram database. Dig. Mammo 1994, 1, 375–386. [Google Scholar]
- Mahmood, T.; Li, J.; Pei, Y.; Akhtar, F.; Jia, Y.; Khand, Z.H. Breast Mass Detection and Classification Using Deep Convolutional Neural Networks for Radiologist Diagnosis Assistance. In Proceedings of the 2021 IEEE 45th Annual Computers, Software, and Applications Conference (COMPSAC), Madrid, Spain, 12–16 July 2021; pp. 1918–1923. [Google Scholar]
- Wang, Z.; Xin, J.; Zhang, Q.; Gao, S.; Ma, C.; Ren, J.; Zhang, H.; Qian, W.; Zhu, W.; Zhang, X.; et al. Breast microcalcifications detection based on fusing features with DTCWT. J. X-ray Sci. Technol. 2020, 28, 197–218. [Google Scholar] [CrossRef]
- Al-Masni, M.A.; Al-Antari, M.A.; Park, J.M.; Gi, G.; Kim, T.Y.; Rivera, P.; Valarezo, E.; Choi, M.T.; Han, S.M.; Kim, T.S. Simultaneous detection and classification of breast masses in digital mammograms via a deep learning YOLO-based CAD system. Comput. Methods Programs Biomed. 2018, 157, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Pang, W.; Xu, Q.; Liang, M. Mammographic image classification with deep fusion learning. Sci. Rep. 2020, 10, 14361. [Google Scholar] [CrossRef]
- Ting, F.F.; Tan, Y.J.; Sim, K.S. Convolutional neural network improvement for breast cancer classification. Expert Syst. Appl. 2019, 120, 103–115. [Google Scholar] [CrossRef]
- Malar, E.; Kandaswamy, A.; Chakravarthy, D.; Dharan, A.G. A novel approach for detection and classification of mammographic microcalcifications using wavelet analysis and extreme learning machine. Comput. Biol. Med. 2012, 42, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Liu, X.; Han, Y.; Qi, C. License plate location algorithm based on edge detection and morphology. In Proceedings of the 2012 7th International Forum on Strategic Technology (IFOST), Tomsk, Russia, 18–21 September 2012; pp. 1–4. [Google Scholar] [CrossRef]
- Shrivastava, N.; Bharti, J. Breast tumor detection and classification based on density. Multimed. Tools Appl. 2020, 79, 26467–26487. [Google Scholar] [CrossRef]
- Linguraru, M.G.; Marias, K.; English, R.; Brady, M. A biologically inspired algorithm for microcalcification cluster detection. Med. Image Anal. 2006, 10, 850–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.; Yao, B.; Wason, A. A genetic algorithm design for microcalcification detection and classification in digital mammograms. Comput. Med. Imaging Gr. 2007, 31, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Melekoodappattu, J.G.; Subbian, P.S. Automated breast cancer detection using hybrid extreme learning machine classifier. J. Am. Intell. Hum. Comput. 2020, 1–10. [Google Scholar] [CrossRef]
- Melekoodappattu, J.G.; Subbian, P.S. A hybridized ELM for automatic micro calcification detection in mammogram images based on multi-scale features. J. Med Syst. 2019, 43, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, T.; Li, J.; Pei, Y.; Akhtar, F. An Automated In-Depth Feature Learning Algorithm for Breast Abnormality Prognosis and Robust Characterization from Mammography Images Using Deep Transfer Learning. Biology 2021, 10, 859. [Google Scholar] [CrossRef]
- Ali, A.A.; Mishra, S.; Dappuri, B. Breast cancer classification using tetrolet transform based energy features and K-nearest neighbor classifier. In Recent Trends and Advances in Artificial Intelligence and Internet of Things; Springer: Berlin/Heidelberg, Germany, 2020; pp. 39–46. [Google Scholar]
- Fadil, R.; Jackson, A.; Abou El Majd, B.; El Ghazi, H.; Kaabouch, N. Classification of Microcalcifications in Mammograms using 2D Discrete Wavelet Transform and Random Forest. In Proceedings of the 2020 IEEE International Conference on Electro Information Technology (EIT), Chicago, IL, USA, 31 July–1 August 2020; pp. 353–359. [Google Scholar]
- Keras Deep Learning Library for Image Data Preprocessing. Available online: https://keras.io/api/preprocessing/image/imagedatagenerator-class.html (accessed on 23 September 2021).
- Goudarzi, M.; Maghooli, K. Extraction of fuzzy rules at different concept levels related to image features of mammogram for diagnosis of breast cancer. Biocybern. Biomed. Eng. 2018, 38, 1004–1014. [Google Scholar] [CrossRef]
- Shi, P.; Zhong, J.; Rampun, A.; Wang, H. A hierarchical pipeline for breast boundary segmentation and calcification detection in mammograms. Comput. Biol. Med. 2018, 96, 178–188. [Google Scholar] [CrossRef]
- Polesel, A.; Ramponi, G.; Mathews, V.J. Adaptive unsharp masking for contrast enhancement. In Proceedings of the International Conference on Image Processing, Washington, DC, USA, 26–29 October 1997; Volume 1, pp. 267–270. [Google Scholar]
- Wang, J.; Yang, Y. A context-sensitive deep learning approach for microcalcification detection in mammograms. Pattern Recognit. 2018, 78, 12–22. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Category | Benign Images | Malignant Images | Total Images |
|---|---|---|---|
| Images | 536 | 432 | 968 |
| Training set | 429 | 346 | 775 |
| Validation set | 107 | 86 | 193 |
| Sr | Augmentation Techniques | Performance Values |
|---|---|---|
| 1 | Rotation | 45°, 90°, 135°, 180°, 270°, 360° |
| 2 | Sharpen (lightness value) | 0.5, 1, 1.5, 2 |
| 3 | Crop and Pad | 0.25 |
| 4 | Shear (axis value) | 10° (X-axis and Y-axis) |
| 5 | Flipping | Top, Bottom, Left, Right |
| 6 | Gaussian Blur (Sigma value) | 0.25, 0.5, 1, 2 |
| 7 | Horizontal and Vertical Shift | 0.2 |
| Configuration | Values |
|---|---|
| Batch Size | 32 |
| Learning Rate | 0.001 |
| Epochs | 90 |
| Steps per epochs | 100 |
| Weight Decay | 0.00005 |
| Dropout | 0.5 |
| Momentum | 0.9 |
| Optimization function | Adam |
| Classifiers | Accuracy | Loss | F-Score | Recall | Precision | Specificity | Sensitivity | AUC |
|---|---|---|---|---|---|---|---|---|
| RF | 0.83 | 0.37 | 0.85 | 0.81 | 0.82 | 0.78 | 0.83 | 0.83 (CI = 75–90) |
| K-NN | 0.79 | 0.38 | 0.77 | 0.73 | 0.79 | 0.76 | 0.79 | 0.79 (CI = 71–86) |
| SVM | 0.93 | 0.08 | 0.91 | 0.90 | 0.93 | 0.91 | 0.93 | 0.85 (CI = 78–91) |
| Proposed Method | 0.98 | 0.06 | 0.98 | 0.93 | 0.94 | 0.97 | 0.98 | 0.90 (CI = 84–95) |
| Authors | Challenges | Approaches Used | Database | ACC | SEN |
|---|---|---|---|---|---|
| [10] | Automatic MC classification | ResNet | DDSM | 0.931 | 0.938 |
| [18] | Characterization of MC cluster | Deep CNN | Private | 0.89 | 0.86 |
| [19] | Detection of MC cluster | ICA | DDSM | N/A | 0.81 |
| [22] | MC segmentation and classification | SVM, KNN | Private | 0.87 | 0.93 |
| [25] | Detection of breast cancer | Deep CNN | Private | 0.82 | 0.50 |
| [31] | MC’s ROI segmentation and classification | MIL | MIAS | N/A | 0.94 |
| [35] | Recognize and segment the breast tumor | MLP, SVM | MIAS | 0.89 | 0.83 |
| [39] | Mass detection and diagnosis | SVM | MIAS | 0.93 | N/A |
| [48] | Automatic segmentation of MC | SGR | DDSM | 0.91 | N/A |
| [60] | MC detection based on surround tissue | Context-Sensitive DNN | FFDM | N/A | 0.87 |
| Proposed | Detection and classification of MC | DC-ELM, SVM | MIAS | 0.98 | 0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmood, T.; Li, J.; Pei, Y.; Akhtar, F.; Imran, A.; Yaqub, M. An Automatic Detection and Localization of Mammographic Microcalcifications ROI with Multi-Scale Features Using the Radiomics Analysis Approach. Cancers 2021, 13, 5916. https://doi.org/10.3390/cancers13235916
Mahmood T, Li J, Pei Y, Akhtar F, Imran A, Yaqub M. An Automatic Detection and Localization of Mammographic Microcalcifications ROI with Multi-Scale Features Using the Radiomics Analysis Approach. Cancers. 2021; 13(23):5916. https://doi.org/10.3390/cancers13235916
Chicago/Turabian StyleMahmood, Tariq, Jianqiang Li, Yan Pei, Faheem Akhtar, Azhar Imran, and Muhammad Yaqub. 2021. "An Automatic Detection and Localization of Mammographic Microcalcifications ROI with Multi-Scale Features Using the Radiomics Analysis Approach" Cancers 13, no. 23: 5916. https://doi.org/10.3390/cancers13235916