
ADAM17—A Potential Blood-Based Biomarker for Detection of Early-Stage Ovarian Cancer

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
- (i)
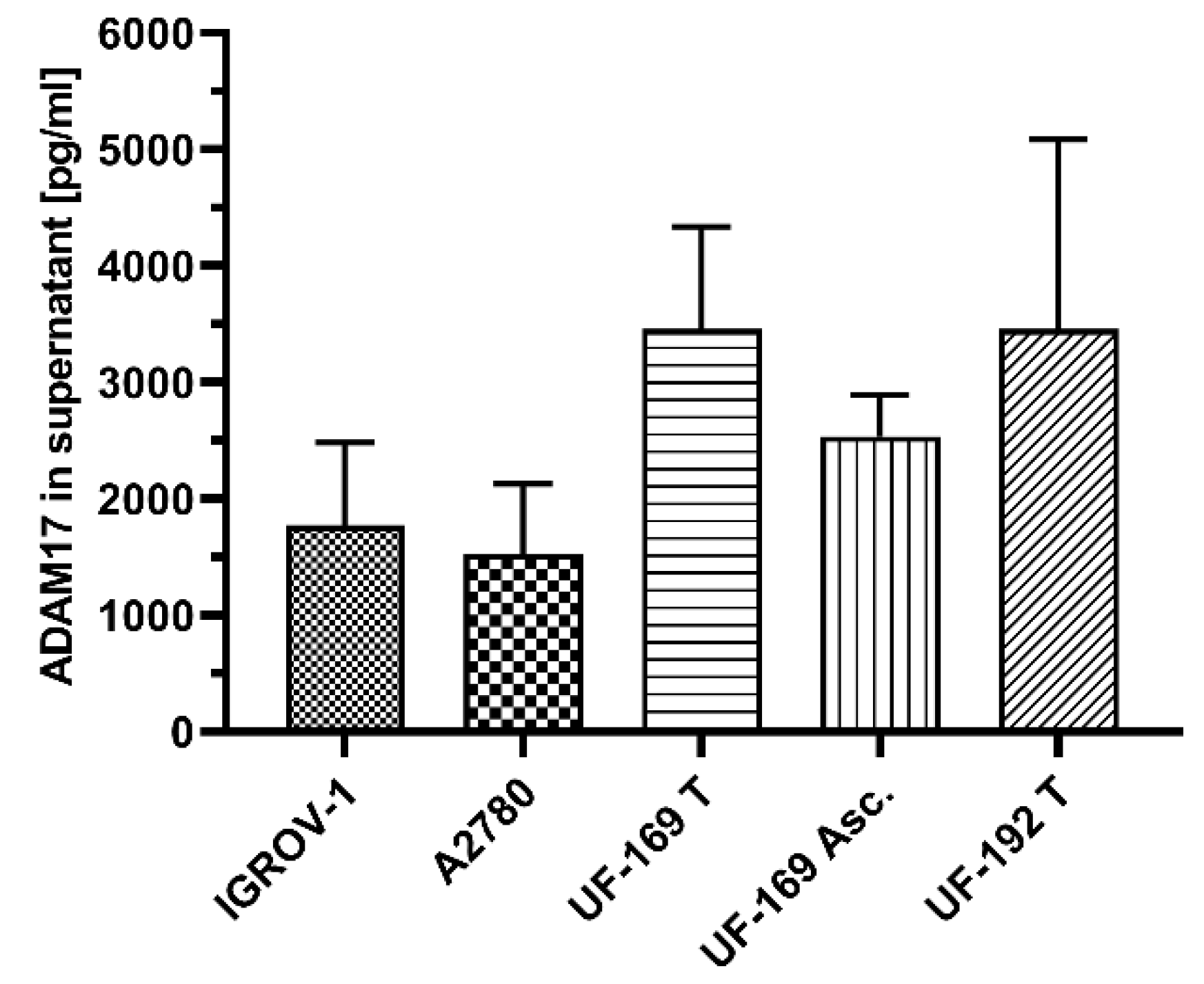
- ADAM17 is released by ovarian cancer cell lines and patient-derived cells into the culture supernatant
- (ii)
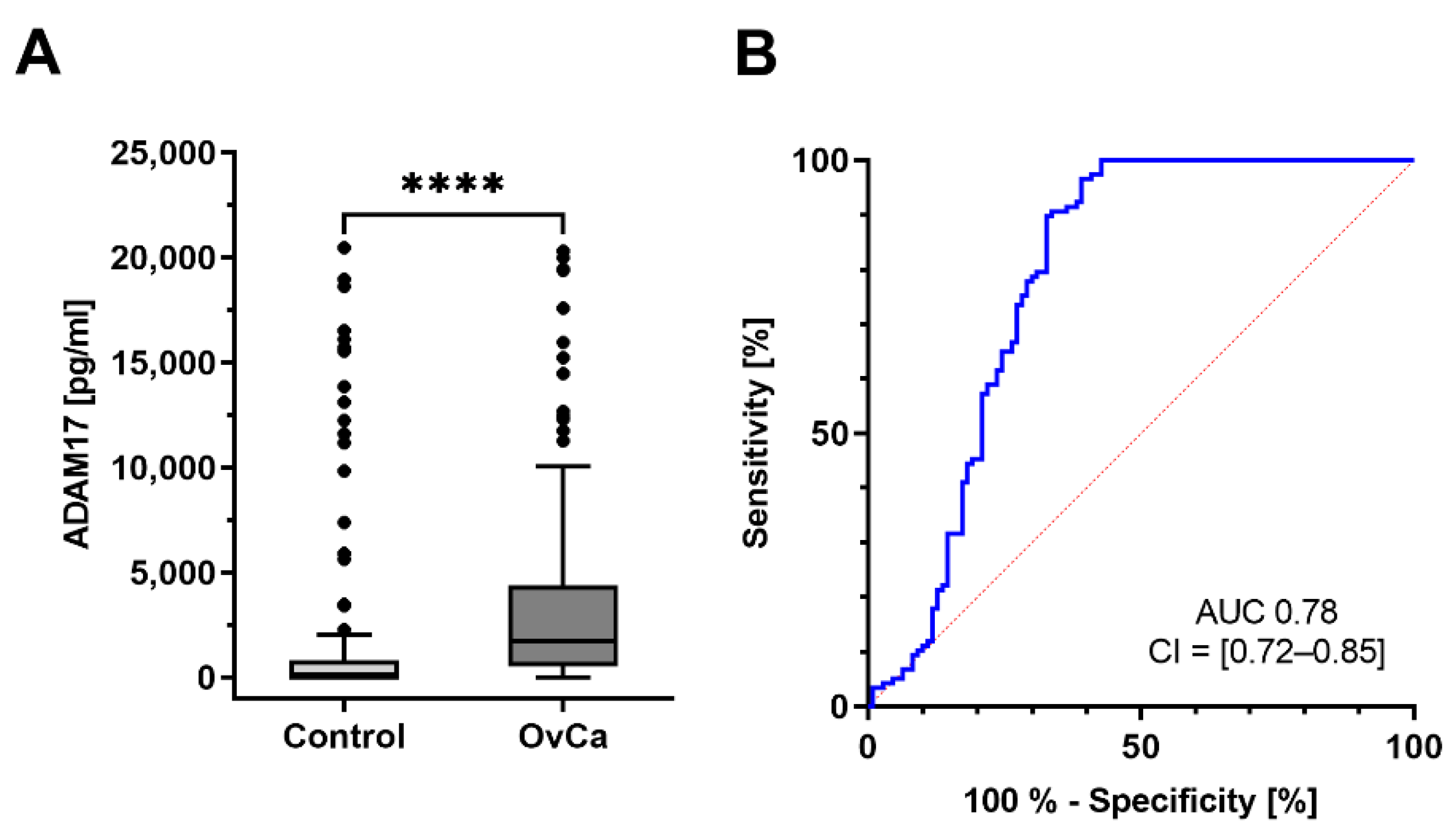
- ADAM17 is differentially detectable in serum samples of ovarian cancer patients compared to healthy controls
- (iii)
- ADAM17 has clinical relevance e.g., in terms of blood-based detection of early-stage ovarian cancer
2. Materials and Methods
2.1. Ethics Statement
2.2. Cell Culture
2.3. Primary Cells and Ascites Fluids
2.4. ADAM17 ELISA
2.5. Cell Lyses, Westernblot and Densitometry
2.6. Patient Characteristics und Serum Samples
2.7. Statistics
3. Results
3.1. ADAM17 Is Detectable in Culture Supernatants of Ovarian Cancer Cell Lines and Patient Derived Tumor Cells
3.2. ADAM17 Is Detectable in Serum and Corresponding Ascites of Ovarian Cancer Patients
3.3. ADAM17 a Novel Marker for Early Detection of Ovarian Cancer?
3.3.1. Early-Stage Patients Have Higher ADAM17 Serum Levels
3.3.2. ADAM17 Is Highly Expressed in the Endometrioid Subtype
3.3.3. Higher ADAM17 Level Predicts Optimal Primary Tumor Debulking
3.4. Comparison between ADAM17 and CA-125
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vargas, A.N. Natural history of ovarian cancer. Ecancermedicalscience 2014, 8, 465. [Google Scholar] [CrossRef]
- Davidson, B.; Tropé, C.G. Ovarian cancer: Diagnostic, biological and prognostic aspects. Women’s Health 2014, 10, 519–533. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Bristow, R.E.R.; Tomacruz, R.; Armstrong, D.K.; Trimble, E.; Montz, F.; Koppitsch, C.M.S.; Chang, S.J.; Bristow, R.E.R.; Chi, D.S.; Cliby, W.A.; et al. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the paltinum era: A meta-analysis. Eur. J. Cancer 2009, 20, 1248–1259. [Google Scholar] [CrossRef]
- Kainz, C. [Early detection and preoperative diagnosis of ovarian carcinoma]. Wien. Med. Wochenschr. 1996, 146, 2–7. [Google Scholar] [PubMed]
- Jacobs, I.; Bast, R.C. The CA 125 tumour-associated antigen: A review of the literature. Hum. Reprod. 1989, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Quentmeier, A.; Schlag, P.; Geisen, H.P.; Schmidt-Gayk, H. Evaluation of Ca 12-5 as a tumor marker for gastric and colo-rectal cancer in comparison to CEA and Ca 19-9. Eur. J. Surg. Oncol. 1987, 13, 197–201. [Google Scholar] [PubMed]
- Kabawat, S.E.; Bast, R.C.; Bhan, A.K.; Welch, W.R.; Knapp, R.C.; Colvin, R.B. Tissue distribution of a coelomic-epithelium-related antigen recognized by the monoclonal antibody OC125. Int. J. Gynecol. Pathol. 1983, 2, 275–285. [Google Scholar] [CrossRef]
- Cramer, D.W.; Bast, R.C.; Berg, C.D.; Diamandis, E.P.; Godwin, A.K.; Hartge, P.; Lokshin, A.E.; Lu, K.H.; McIntosh, M.W.; Mor, G.; et al. Ovarian cancer biomarker performance in prostate, lung, colorectal, and ovarian cancer screening trial specimens. Cancer Prev. Res. 2011, 4, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Molina, R.; Escudero, J.M.; Augé, J.M.; Filella, X.; Foj, L.; Torné, A.; Lejarcegui, J.; Pahisa, J. HE4 a novel tumour marker for ovarian cancer: Comparison with CA 125 and ROMA algorithm in patients with gynaecological diseases. Tumour Biol. 2011, 32, 1087–1095. [Google Scholar] [CrossRef] [Green Version]
- Huhtinen, K.; Suvitie, P.; Hiissa, J.; Junnila, J.; Huvila, J.; Kujari, H.; Setälä, M.; Härkki, P.; Jalkanen, J.; Fraser, J.; et al. Serum HE4 concentration differentiates malignant ovarian tumours from ovarian endometriotic cysts. Br. J. Cancer 2009, 100, 1315–1319. [Google Scholar] [CrossRef]
- Romagnolo, C.; Leon, A.E.; Fabricio, A.S.C.; Taborelli, M.; Polesel, J.; Del Pup, L.; Steffan, A.; Cervo, S.; Ravaggi, A.; Zanotti, L.; et al. HE4, CA125 and risk of ovarian malignancy algorithm (ROMA) as diagnostic tools for ovarian cancer in patients with a pelvic mass: An Italian multicenter study. Gynecol. Oncol. 2016, 141, 303–311. [Google Scholar] [CrossRef]
- Sahin, U.; Blobel, C.P. Ectodomain shedding of the EGF-receptor ligand epigen is mediated by ADAM17. FEBS Lett. 2007, 581, 41–44. [Google Scholar] [CrossRef] [Green Version]
- Richards, F.M.; Tape, C.J.; Jodrell, D.I.; Murphy, G. Anti-tumour effects of a specific anti-ADAM17 antibody in an ovarian cancer model in vivo. PLoS ONE 2012, 7, e40597. [Google Scholar] [CrossRef] [Green Version]
- Hedemann, N.; Rogmans, C.; Sebens, S.; Wesch, D.; Reichert, M.; Schmidt-Arras, D.; Oberg, H.-H.; Pecks, U.; van Mackelenbergh, M.; Weimer, J.; et al. ADAM17 inhibition enhances platinum efficiency in ovarian cancer. Oncotarget 2018, 9, 16043–16058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabre-Lafay, S.; Monville, F.; Garrido-Urbani, S.; Berruyer-Pouyet, C.; Ginestier, C.; Reymond, N.; Finetti, P.; Sauvan, R.; Adélaïde, J.; Geneix, J.; et al. Nectin-4 is a new histological and serological tumor associated marker for breast cancer. BMC Cancer 2007, 7, 73. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, P.C.; Boylan, K.L.M.; Walcheck, B.; Heinze, R.; Geller, M.A.; Argenta, P.A.; Skubitz, A.P.N. Ectodomain shedding of the cell adhesion molecule Nectin-4 in ovarian cancer is mediated by ADAM10 and ADAM17. J. Biol. Chem. 2017, 292, 6339–6351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGowan, P.M.; McKiernan, E.; Bolster, F.; Ryan, B.M.; Hill, A.D.K.; Mcdermott, E.W.; Evoy, D.; O’Higgins, N.; Crown, J.; Duffy, M.J. ADAM-17 predicts adverse outcome in patients with breast cancer. Ann. Oncol. 2008, 19, 1075–1081. [Google Scholar] [CrossRef]
- Umemura, M.; Isozaki, T.; Ishii, S.; Seki, S.; Oguro, N.; Miura, Y.; Miwa, Y.; Nakamura, M.; Inagaki, K.; Kasama, T. Reduction of serum ADAM17 level accompanied with decreased cytokines after abatacept therapy in patients with rheumatoid arthritis. Int. J. Biomed. Sci. 2014, 10, 229–235. [Google Scholar]
- Kermarrec, N.; Selloum, S.; Plantefeve, G.; Chosidow, D.; Paoletti, X.; Lopez, A.; Mantz, J.; Desmonts, J.M.; Gougerot-Pocidalo, M.A.; Chollet-Martin, S. Regulation of peritoneal and systemic neutrophil-derived tumor necrosis factor-α release in patients with severe peritonitis: Role of tumor necrosis factor-α converting enzyme cleavage. Crit. Care Med. 2005, 33, 1359–1364. [Google Scholar] [CrossRef] [PubMed]
- Walkiewicz, K.; Strzelczyk, J.; Waniczek, D.; Biernacki, K.; Muc-Wierzgoń, M.; Copija, A.; Nowakowska-Zajdel, E. Adamalysines as biomarkers and a potential target of therapy in colorectal cancer patients: Preliminary results. Dis. Markers 2019, 2019, 5035234. [Google Scholar] [CrossRef]
- Zhang, T.; Zhu, W.; Huang, M.; Fan, R.; Chen, X. Prognostic value of ADAM17 in human gastric cancer. Med. Oncol. 2012, 29, 2684–2690. [Google Scholar] [CrossRef]
- Yunusova, N.V.; Patysheva, M.R.; Molchanov, S.V.; Zambalova, E.A.; Grigor’eva, A.E.; Kolomiets, L.A.; Ochirov, M.O.; Tamkovich, S.N.; Kondakova, I.V. Metalloproteinases at the surface of small extrcellular vesicles in advanced ovarian cancer: Relationships with ascites volume and peritoneal canceromatosis index. Clin. Chim. Acta 2019, 494, 116–122. [Google Scholar] [CrossRef]
- Tanaka, Y.; Miyamoto, S.; Suzuki, S.O.; Oki, E.; Yagi, H.; Sonoda, K.; Yamazaki, A.; Mizushima, H.; Maehara, Y.; Mekada, E.; et al. Clinical significance of heparin-binding epidermal growth factor-like growth factor and a disintegrin and metalloprotease 17 expression in human ovarian cancer. Clin. Cancer Res. 2005, 11, 4783–4792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Weimer, J.; von Wurmb-Schwark, N.; Fredrik, R.; Arnold, N.; Schem, C. Alteration of STR profiles in ovarian carcinoma cells during primary culture. Arch. Gynecol. Obstet. 2016, 294, 369–376. [Google Scholar] [CrossRef]
- Trad, A.; Hedemann, N.; Shomali, M.; Pawlak, V.; Grötzinger, J.; Lorenzen, I. Development of sandwich ELISA for detection and quantification of human and murine a disintegrin and metalloproteinase17. J. Immunol. Methods 2011, 371, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Kurbacher, C.M.; Korn, C.; Dexel, S.; Schween, U.; Kurbacher, J.A.; Reichelt, R.; Arenz, P.N. Isolation and culture of ovarian cancer cells and cell lines. Methods Mol. Biol. 2011, 731, 161–180. [Google Scholar] [CrossRef] [PubMed]
- Lieb, W.; Jacobs, G.; Wolf, A.; Richter, G.; Gaede, K.I.; Schwarz, J.; Arnold, N.; Böhm, R.; Buyx, A.; Cascorbi, I.; et al. Linking pre-existing biorepositories for medical research: The PopGen 2.0 Network. J. Community Genet. 2019, 10, 523–530. [Google Scholar] [CrossRef] [Green Version]
- Lorenzen, I.; Lokau, J.; Korpys, Y.; Oldefest, M.; Flynn, C.M.; Künzel, U.; Garbers, C.; Freeman, M.; Grötzinger, J.; Düsterhöft, S. Control of ADAM17 activity by regulation of its cellular localisation. Sci. Rep. 2016, 6, 35067. [Google Scholar] [CrossRef]
- Scheff, N.N.; Ye, Y.; Bhattacharya, A.; MacRae, J.; Hickman, D.N.; Sharma, A.K.; Dolan, J.C.; Schmidt, B.L. Tumor necrosis factor alpha secreted from oral squamous cell carcinoma contributes to cancer pain and associated inflammation. Pain 2017, 158, 2396–2409. [Google Scholar] [CrossRef]
- Schlöndorff, J.; Becherer, J.D.; Blobel, C.P. Intracellular maturation and localization of the tumour necrosis factor alpha convertase (TACE). Biochem. J. 2000, 347, 131. [Google Scholar] [CrossRef] [PubMed]
- Groth, E.; Pruessmeyer, J.; Babendreyer, A.; Schumacher, J.; Pasqualon, T.; Dreymueller, D.; Higashiyama, S.; Lorenzen, I.; Grötzinger, J.; Cataldo, D.; et al. Stimulated release and functional activity of surface expressed metalloproteinase ADAM17 in exosomes. Biochim. Biophys. Acta Mol. Cell Res. 2016, 1863, 2795–2808. [Google Scholar] [CrossRef]
- Belotti, D.; Calcagno, C.; Garofalo, A.; Caronia, D.; Riccardi, E.; Giavazzi, R.; Taraboletti, G. Vascular endothelial growth factor stimulates organ-specific host matrix metalloproteinase-9 expression and ovarian cancer invasion. Mol. Cancer Res. 2008, 6, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Koyama, S. Coordinate cell-surface expression of matrix metalloproteinases and their inhibitors on cancer-associated myofibroblasts from malignant ascites in patients with gastric carcinoma. J. Cancer Res. Clin. Oncol. 2005, 131, 809–814. [Google Scholar] [CrossRef] [PubMed]
- DeRycke, M.S.; Pambuccian, S.E.; Gilks, C.B.; Kalloger, S.E.; Ghidouche, A.; Lopez, M.; Bliss, R.L.; Geller, M.A.; Argenta, P.A.; Harrington, K.M.; et al. Nectin 4 overexpression in ovarian cancer tissues and serum. Am. J. Clin. Pathol. 2010, 134, 835–845. [Google Scholar] [CrossRef]
- Link, T.; Passek, S.; Wimberger, P.; Frank, K.; Vassileva, Y.D.; Kramer, M.; Kuhlmann, J.D. Serum calretinin as an independent predictor for platinum resistance and prognosis in ovarian cancer. Int. J. Cancer 2020, 146, 2608–2618. [Google Scholar] [CrossRef] [Green Version]
- Cragun, J.M. Screening for ovarian cancer. Cancer Control. 2011, 18, 16–21. [Google Scholar] [CrossRef]
- Saftig, P.; Reiss, K. The “A disintegrin and metalloproteases” ADAM10 and ADAM17: Novel drug targets with therapeutic potential? Eur. J. Cell Biol. 2011, 90, 527–535. [Google Scholar] [CrossRef]
- Sahin, U.; Weskamp, G.; Kelly, K.; Zhou, H.-M.; Higashiyama, S.; Peschon, J.; Hartmann, D.; Saftig, P.; Blobel, C.P. Distinct roles for ADAM10 and ADAM17 in ectodomain shedding of six EGFR ligands. J. Cell Biol. 2004, 164, 769–779. [Google Scholar] [CrossRef] [Green Version]
- Kenny, P.A. TACE: A new target in epidermal growth factor receptor dependent tumors. Differentiation 2007, 75, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Peschon, J.J. An Essential Role for Ectodomain Shedding in Mammalian Development. Science 1998, 282, 1281–1284. [Google Scholar] [CrossRef]
- McGowan, P.M.; Ryan, B.M.; Hill, A.D.K.; McDermott, E.; O’Higgins, N.; Duffy, M.J. ADAM-17 expression in breast cancer correlates with variables of tumor progression. Clin. Cancer Res. 2007, 13, 2335–2343. [Google Scholar] [CrossRef] [Green Version]
- Tapia, V.M.; Amtmann, N.; Gabler, F.; Selman, A.; Vega, M.; Romero, C. ADAM17 Expression is increased in epithelial ovarian carcinoma. Biol. Reprod. 2011, 85, 748. [Google Scholar] [CrossRef]
- Sinnathamby, G.; Zerfass, J.; Hafner, J.; Block, P.; Nickens, Z.; Hobeika, A.; Secord, A.A.; Lyerly, H.K.; Morse, M.A.; Philip, R. ADAM metallopeptidase domain 17 (ADAM17) is naturally processed through major histocompatibility complex (MHC) class I molecules and is a potential immunotherapeutic target in breast, ovarian and prostate cancers. Clin. Exp. Immunol. 2011, 163, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Scharfenberg, F.; Helbig, A.; Sammel, M.; Benzel, J.; Schlomann, U.; Peters, F.; Wichert, R.; Bettendorff, M.; Schmidt-Arras, D.; Rose-John, S.; et al. Degradome of soluble ADAM10 and ADAM17 metalloproteases. Cell. Mol. Life Sci. 2020, 77, 331–350. [Google Scholar] [CrossRef]
- Mongaret, C.; Alexandre, J.; Thomas-Schoemann, A.; Bermudez, E.; Chéreau, C.; Nicco, C.; Goldwasser, F.; Weill, B.; Batteux, F.; Lemare, F. Tumor invasion induced by oxidative stress is dependent on membrane ADAM 9 protein and its secreted form. Int. J. Cancer 2011, 129, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Hampel, H.; Blennow, K.; Lista, S.; Levey, A.; Tang, B.; Li, R.; Shen, Y. Increased plasma TACE activity in subjects with mild cognitive impairment and patients with Alzheimer’s disease. J. Alzheimers Dis. 2014, 41, 877–886. [Google Scholar] [CrossRef] [Green Version]
- Conrad, C.; Dorzweiler, K.; Thanisch, M.; Bartsch, J.; Strik, H.M. P13.03 Profiling protease activities in cerebrospinal fluids: A novel method for detection of neoplastic meningitis? Neuro. Oncol. 2017, 19, iii101. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Magenheimer, B.S.; Xia, S.; Johnson, T.; Wallace, D.P.; Calvet, J.P.; Li, R. A tumor necrosis factor-α-mediated pathway promoting autosomal dominant polycystic kidney disease. Nat. Med. 2008, 14, 863–868. [Google Scholar] [CrossRef] [Green Version]
- Poersch, A.; Grassi, M.L.; Carvalho, V.P.; de Lanfredi, G.P.; Palma, C.d.S.; Greene, L.J.; de Sousa, C.B.; Carrara, H.H.A.; Candido dos Reis, F.J.; Faça, V.M. A proteomic signature of ovarian cancer tumor fluid identified by highthroughput and verified by targeted proteomics. J. Proteomics 2016, 145, 226–236. [Google Scholar] [CrossRef]
- Carbotti, G.; Orengo, A.M.; Mezzanzanica, D.; Bagnoli, M.; Brizzolara, A.; Emionite, L.; Puppo, A.; Centurioni, M.G.; Bruzzone, M.; Marroni, P.; et al. Activated leukocyte cell adhesion molecule soluble form: A potential biomarker of epithelial ovarian cancer is increased in type II tumors. Int. J. Cancer 2013, 132, 2597–2605. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.G.; Stewart, M.E.; Altman, D.G.; Gabra, H.; Smyth, J.F. A prognostic model for ovarian cancer. Br. J. Cancer 2001, 85, 944–952. [Google Scholar] [CrossRef] [Green Version]
- Fures, R.; Bukovic, D.; Hodek, B.; Klaric, P.; Herman, R.; Grubisic, G. Preoperative tumor marker CA125 levels in relation to epithelial ovarian cancer stage. Coll. Antropol. 1999, 138, 378–383. [Google Scholar] [CrossRef] [Green Version]
- Welander, C.E. What do CA 125 and other antigens tell us about ovarian cancer biology? Acta Obstet. Gynecol. Scand. Suppl. 1992, 155, 85–93. [Google Scholar] [CrossRef]
- Tholander, B.; Taube, A.; Lindgren, A.; Sjöberg, O.; Stendahl, U.; Kiviranta, A.; Hallman, K.; Holm, L.; Weiner, E.; Tamsen, L. Pretreatment serum levels of CA-125, carcinoembryonic antigen, tissue polypeptide antigen, and placental alkaline phosphatase in patients with ovarian carcinoma: Influence of histological type, grade of differentiation, and clinical stage of disease. Gynecol. Oncol. 1990, 39, 16–25. [Google Scholar] [CrossRef]
- Griffiths, C. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma: Seminar on ovarian cancer. J. Natl Cancer Inst. Monogr. 1975, 42, 101–104. [Google Scholar]
- Gonzalez, A.; Vizoso, F.; Vázquez, J.; Ruibal, A.; Balibrea, J.L. Clinical significance of preoperative serum levels of CA 125 and TAG-72 in ovarian carcinoma. Int. J. Biol. Markers 1997, 12, 112–117. [Google Scholar] [CrossRef]
- Rossi, A.C.; Di Vagno, G.; Cormio, G.; Cazzolla, A.; Stefanelli, S.; D’Elia, E.; Selvaggi, L. A retrospective study of preoperative CA 125 levels in 82 patients with ovarian cancer. Arch. Gynecol. Obstet. 2004, 269, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Ganss, R. Tumor stroma fosters neovascularization by recruitment of progenitor cells into the tumor bed. J. Cell. Mol. Med. 2006, 10, 857–865. [Google Scholar] [CrossRef]
- Schauer, I.G.; Sood, A.K.; Mok, S.; Liu, J. Cancer-associated fibroblasts and their putative role in potentiating the initiation and development of epithelial ovarian cancer. Neoplasia 2011, 13, 393–405. [Google Scholar] [CrossRef] [Green Version]
- Cury, P.M.; de Carvalho, M.B.; Dias-Neto, E.; Figueiredo, D.L.A.; Fukuyama, E.E.; Góis-Filho, J.F.; Leopoldino, A.M.; Mamede, R.C.M.; Michaluart-Junior, P.; Moyses, R.A.; et al. Genomics and proteomics approaches to the study of cancer-stroma interactions. BMC Med. Genom. 2010, 3, 14. [Google Scholar] [CrossRef] [Green Version]
- Romee, R.; Lenvik, T.; Wang, Y.; Walcheck, B.; Verneris, M.R.; Miller, J.S. ADAM17, a novel metalloproteinase, mediates CD16 and CD62L shedding in human NK cells and modulates IFNγ responses. Blood 2011, 118, 2184. [Google Scholar] [CrossRef]
- Nishiwada, S.; Sho, M.; Yasuda, S.; Shimada, K.; Yamato, I.; Akahori, T.; Kinoshita, S.; Nagai, M.; Konishi, N.; Nakajima, Y. Nectin-4 expression contributes to tumor proliferation, angiogenesis and patient prognosis in human pancreatic cancer. J. Exp. Clin. Cancer Res. 2015, 34, 30. [Google Scholar] [CrossRef]
- Tsujioka, H.; Yotsumoto, F.; Hikita, S.; Ueda, T.; Kuroki, M.; Miyamoto, S. Targeting the heparin-binding epidermal growth factor-like growth factor in ovarian cancer therapy. Curr. Opin. Obstet. Gynecol. 2011, 23, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.Q.; Kim, B.G.; Kang, S.; Choi, Y.P.; Yoon, J.H.; Cho, N.H. Human breast cancer-associated fibroblasts enhance cancer cell proliferation through increased TGF-α cleavage by ADAM17. Cancer Lett. 2013, 336, 240–246. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Parameter | Characteristics | |||
|---|---|---|---|---|
| Histology | Serous | Endometrioid | Clear-cell | Others |
| 84 | 18 | 6 | 9 | |
| Grading | Low | High | ||
| 3 | 101 | |||
| FIGO | I | II | III | IV |
| 21 | 6 | 77 | 16 | |
| Resection of the tumor | R0 | R1 | ||
| 79 | 47 | |||
| Age | Mean 60.6 +/10.8 years | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogmans, C.; Kuhlmann, J.D.; Hugendieck, G.; Link, T.; Arnold, N.; Weimer, J.P.; Flörkemeier, I.; Rambow, A.-C.; Lieb, W.; Maass, N.; et al. ADAM17—A Potential Blood-Based Biomarker for Detection of Early-Stage Ovarian Cancer. Cancers 2021, 13, 5563. https://doi.org/10.3390/cancers13215563
Rogmans C, Kuhlmann JD, Hugendieck G, Link T, Arnold N, Weimer JP, Flörkemeier I, Rambow A-C, Lieb W, Maass N, et al. ADAM17—A Potential Blood-Based Biomarker for Detection of Early-Stage Ovarian Cancer. Cancers. 2021; 13(21):5563. https://doi.org/10.3390/cancers13215563
Chicago/Turabian StyleRogmans, Christoph, Jan Dominik Kuhlmann, Gerrit Hugendieck, Theresa Link, Norbert Arnold, Jörg Paul Weimer, Inken Flörkemeier, Anna-Christina Rambow, Wolfgang Lieb, Nicolai Maass, and et al. 2021. "ADAM17—A Potential Blood-Based Biomarker for Detection of Early-Stage Ovarian Cancer" Cancers 13, no. 21: 5563. https://doi.org/10.3390/cancers13215563