Functional Outcomes after Local Salvage Therapies for Radiation-Recurrent Prostate Cancer Patients: A Systematic Review

 ,
,  ,
,  , ,
, ,
Abstract
:Simple Summary
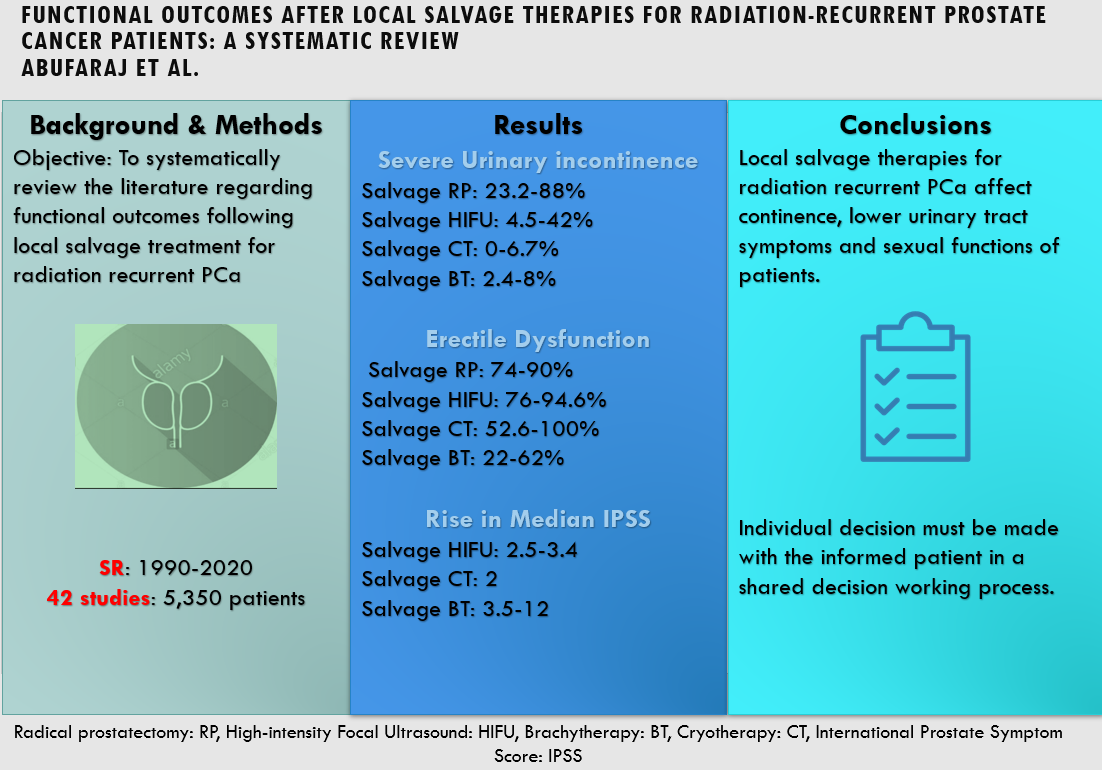
Abstract

1. Introduction
2. Materials and Methods
Evidence Acquisition
3. Evidence Synthesis
3.1. Study Selection
3.2. Study Characteristics
3.3. Urinary Incontinence
3.4. Erectile Dysfunction
3.5. Urinary Obstruction
3.6. Additional Outcomes
4. Risk of Bias Assessment
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pishgar, F.; Ebrahimi, H.; Moghaddam, S.S.; Fitzmaurice, C.; Amini, E. Global, Regional and National Burden of Prostate Cancer, 1990 to 2015: Results from the Global Burden of Disease Study 2015. J. Urol. 2018, 199, 1224–1232. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Mariotto, A.B.; Yabroff, K.R.; Shao, Y.; Feuer, E.J.; Brown, M.L. Projections of the Cost of Cancer Care in the United States: 2010 –2020. J. Natl. Cancer Inst. 2011, 103, 117–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, J.W.; Drumm, M.R.; Efstathiou, J.A.; Paly, J.J.; Niemierko, A.; Ancukiewicz, M.; Talcott, J.A.; Clark, J.A.; Zietman, A.L. Long-term quality of life after definitive treatment for prostate cancer: Patient-reported outcomes in the second posttreatment decade. Cancer Med. 2017, 6, 1827–1836. [Google Scholar] [CrossRef] [Green Version]
- Burt, L.M.; Shrieve, D.C.; Tward, J.D. Factors influencing prostate cancer patterns of care: An analysis of treatment variation using the SEER database. Adv. Radiat. Oncol. 2018, 3, 170–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walz, J.; Gallina, A.; Perrotte, P.; Jeldres, C.; Trinh, Q.D.; Hutterer, G.C.; Traumann, M.; Ramirez, A.; Shariat, S.F.; McCormack, M.; et al. Clinicians are poor raters of life-expectancy before radical prostatectomy or definitive radiotherapy for localized prostate cancer. BJU Int. 2007, 100, 1254–1258. [Google Scholar] [CrossRef] [PubMed]
- Lawrentschuk, N.; Trottier, G.; Kuk, C.; Zlotta, A.R. Role of surgery in high-risk localized prostate cancer. Curr. Oncol. 2010, 17, 387–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shariat, S.F.; Kattan, M.W.; Vickers, A.J.; Karakiewicz, P.I.; Scardino, P.T. Critical review of prostate cancer predictive tools. Futur. Oncol. 2009, 5, 1555–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, P.J.; Zietman, A.L. Dose-Escalated Radiotherapy for Prostate Cancer Is the Sky the Limit? JAMA Oncol. 2015, 1, 883–884. [Google Scholar] [CrossRef]
- Dearnaley, D.P.; Jovic, G.; Syndikus, I.; Khoo, V.; Cowan, R.A.; Graham, J.D.; Aird, E.G.; Bottomley, D.; Huddart, R.A.; Jose, C.C.; et al. Escalated-dose versus control-dose conformal radiotherapy for prostate cancer: Long-term results from the MRC RT01 randomised controlled trial. Lancet Oncol. 2014, 15, 464–473. [Google Scholar] [CrossRef] [Green Version]
- Zietman, A.L.; Bae, K.; Slater, J.D.; Shipley, W.U.; Efstathiou, J.A.; Coen, J.J.; Bush, D.A.; Lunt, M.; Spiegel, D.Y.; Skowronski, R.; et al. Randomized Trial Comparing Conventional-Dose With High-Dose Conformal Radiation Therapy in Early-Stage Adenocarcinoma of the Prostate: Long-Term Results From Proton Radiation Oncology Group/American College of Radiology 95-09. J. Clin. Oncol. 2014, 28, 1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steele, E.M.; Holmes, J.A. A review of salvage treatment options for disease progression after radiation therapy for localized prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 582–598. [Google Scholar] [CrossRef] [Green Version]
- Zdrojowy, R.; Dembowski, J.; Małkiewicz, B.; Tupikowski, K.; Krajewski, W. Salvage local therapy for radiation-recurrent prostate cancer where are we? Cent. Eur. J. Urol. 2016, 69, 264–270. [Google Scholar]
- Gandaglia, G.; Abdollah, F.; Schiffmann, J.; Trudeau, V.; Shariat, S.F.; Kim, S.P.; Perrotte, P.; Montorsi, F.; Briganti, A.; Trinh, Q.; et al. Distribution of metastatic sites in patients with prostate cancer: A population-based analysis. Prostate 2014, 74, 210–216. [Google Scholar] [CrossRef]
- Abufaraj, M.; Grubmüller, B.; Zeitlinger, M.; Kramer, G.; Seitz, C.; Haitel, A.; Baltzer, P.; Hacker, M.; Wadsak, W.; Pfaff, S.; et al. Prospective evaluation of the performance of [68Ga]Ga-PSMA-11 PET/CT(MRI) for lymph node staging in patients undergoing superextended salvage lymph node dissection after radical prostatectomy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2169–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, N.N.; Unger, P.; Crawford, E.D.; Stock, R.G. Diagnosis and management of local recurrence after low-dose-rate brachytherapy. Brachytherapy 2015, 14, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Leventis, A.K.; Shariat, S.F.; Slawin, K.M. Local recurrence after radical prostatectomy: Correlation of US features with prostatic fossa biopsy findings. Radiology 2001, 219, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.K.; Sadetsky, N.; Konety, B.R.; Resnick, M.I.; Carroll, P.R. Treatment failure after primary and salvage therapy for prostate cancer: Likelihood, patterns of care, and outcomes. Cancer 2008, 112, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Chade, D.C.; Eastham, J.; Graefen, M.; Hu, J.C.; Karnes, R.J.; Klotz, L.; Montorsi, F.; Poppel, H.V.; Scardino, P.T.; Shariat, S.F. Cancer Control and Functional Outcomes of Salvage Radical Prostatectomy for Radiation-recurrent Prostate Cancer: A Systematic Review of the Literature. Eur. Urol. 2012, 61, 961–971. [Google Scholar] [CrossRef]
- Chade, D.C.; Shariat, S.F.; Cronin, A.M.; Savage, C.J.; Karnes, R.J.; Blute, M.L.; Briganti, A.; Montorsi, F.; Poel, H.G.; Poppel, H.V.; et al. Salvage radical prostatectomy for radiation-recurrent prostate cancer: A multi-institutional collaboration. Eur. Urol. 2011, 60, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D.; et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Ingelman-Sundberg, A.; Ulmsten, U. Surgical Treatment of Female Urinary Stress Incontinence. In Contributions to Gynecology and Obstetrics; Karger: Basel, Switzerland, 1983; pp. 51–69. Available online: https://www.karger.com/Article/FullText/407974 (accessed on 14 November 2020).
- National Institutes of Health (NIH). National Cancer Institute. Common Terminology Criteria for Adverse Events v4.02 (CTCAE). US Department of Health and Human Services. 2009. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/Archive/CTCAE_4.02_2009-09-15_QuickReference_8.5x11.pdf (accessed on 16 December 2020).
- National Institutes of Health (NIH). National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) v3.0. US Department of Health and Human Services Version. 2006. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf (accessed on 16 December 2020).
- National Institutes of Health. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 2014. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 14 November 2020).
- Mohler, J.L.; Halabi, S.; Ryan, S.T.; Al-Daghmin, A.; Sokoloff, M.H.; Steinberg, G.D.; Sanford, B.L.; Eastham, J.A.; Walther, P.J.; Morris, M.J.; et al. Management of recurrent prostate cancer after radiotherapy: Long-term results from CALGB 9687 (Alliance), a prospective multi-institutional salvage prostatectomy series. Prostate Cancer Prostatic Dis. 2019, 22, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Seabra, D.; Faria, E.; Dauster, B.; Rodrigues, G.; Fava, G. Critical analysis of salvage radical prostatectomy in the management of radioresistant prostate cancer. Int. Braz. J. Urol. 2009, 35, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, B.J.; Saliken, J.C.; Ernst, D.S.; Weber, B.; Robinson, J.W.; Brasher, P.M.A.; Rose, M.; Rewcastle, J. Role of transrectal ultrasound guided salvage cryosurgery for recurrent prostate carcinoma after radiotherapy. Prostate Cancer Prostatic Dis. 2005, 8, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Van Son, M.J.; Peters, M.; Moerland, M.A.; Lagendijk, J.J.W.; Eppinga, W.S.C.; Shah, T.T.; Ahmed, H.U.; Zyp, J.R. MRI-Guided Ultrafocal Salvage High-Dose-Rate Brachytherapy for Localized Radiorecurrent Prostate Cancer: Updated Results of 50 Patients. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Kollmeier, M.A.; Pei, X.; Kan, C.C.; Cohen, G.N.; Donat, S.M.; Cox, B.W.; Zelefsky, M.J. A Phase II study of salvage high-dose-rate brachytherapy for the treatment of locally recurrent prostate cancer after definitive external beam radiotherapy. Brachytherapy 2014, 13, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, T.A.; Chin, J.; Mcleod, D.; Barkin, J.; Pantuck, A.; Marks, L.S. High Intensity Focused Ultrasound for Radiorecurrent Prostate Cancer: A North American Clinical Trial. J. Urol. 2018, 199, 133–139. [Google Scholar] [CrossRef]
- Shah, T.T.; Peters, M.; Kanthabalan, A.; McCartan, N.; Fatola, Y.; Van Der, V.; Van Zyp, J.; Vulpen, M.V.; Freeman, A.; Moore, C.M.; et al. PSA nadir as a predictive factor for biochemical disease-free survival and overall survival following whole-gland salvage HIFU following radiotherapy failure. Prostate Cancer Prostatic Dis. 2016, 19, 311–316. [Google Scholar] [CrossRef]
- Baco, E.; Gelet, A.; Crouzet, S.; Rud, E.; Rouvière, O.; Tonoli-Catez, H.; Berge, V.; Chapelon, J.; Eggesbø, H.B. Hemi salvage high-intensity focused ultrasound (HIFU) in unilateral radiorecurrent prostate cancer: A prospective two-centre study. BJU Int. 2014, 114, 532–540. [Google Scholar] [CrossRef] [Green Version]
- Crouzet, S.; Murat, F.J.; Pommier, P.; Poissonnier, L.; Pasticier, G.; Rouviere, O.; Chapelon, J.; Rabilloud, M.; Belot, A.; Mège-Lechevallier, F.; et al. Locally recurrent prostate cancer after initial radiation therapy: Early salvage high-intensity focused ultrasound improves oncologic outcomes. Radiother. Oncol. 2012, 105, 198–202. [Google Scholar] [CrossRef]
- Hostiou, T.; Gelet, A.; Chapelon, J.Y.; Rouvière, O.; Mège-Lechevalier, F.; Lafon, C.; Tonoli-Catez, H.; Badet, L.; Crouzet, S. Salvage high-intensity focused ultrasound for locally recurrent prostate cancer after low-dose-rate brachytherapy: Oncological and functional outcomes. BJU Int. 2019, 124, 746–757. [Google Scholar] [CrossRef] [PubMed]
- Berge, V.; Baco, E.; Karlsen, S.J. A prospective study of salvage high-intensity focused ultrasound for locally radiorecurrent prostate cancer: Early results. Scand. J. Urol. Nephrol. 2010, 44, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.; Ahmed, S.; Kastner, C.; Davies, J. Salvage cryotherapy for recurrent prostate cancer after radiation failure: A prospective case series of the first 100 patients. BJU Int. 2007, 100, 760–764. [Google Scholar] [CrossRef] [PubMed]
- Clarke, H.S.; Eskridge, M.R.; El-Zawahry, A.M.; Keane, T.E. Salvage cryosurgical ablation of the prostate for local recurrence after radiation therapy: Improved outcomes utilizing a capromab pendetide scan and biopsy algorithm. Can. J. Urol. 2007, 14, 24–27. [Google Scholar] [PubMed]
- Robinson, J.W.; Donnelly, B.J.; Coupland, K.; Siever, J.E.; Saliken, J.C.; Scott, C.; Brasher, P.M.A.; Ernst, D.S. Quality of life 2 years after salvage cryosurgery for the treatment of local recurrence of prostate cancer after radiotherapy. Urol. Oncol. Semin. Orig. Investig. 2006, 24, 472–486. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.F.; Sebo, T.J.; Blute, M.L.; Zincke, H. Salvage surgery for radiorecurrent prostate cancer: Contemporary outcomes. J. Urol. 2005, 173, 1156–1160. [Google Scholar] [CrossRef]
- Devos, B.; Al Hajj Obeid, W.; Andrianne, C.; Diamand, R.; Peltier, A.; Everaerts, W.; Poppel, H.V.; Velthoven, R.V.; Joniau, S. Salvage high-intensity focused ultrasound versus salvage radical prostatectomy for radiation-recurrent prostate cancer: A comparative study of oncological, functional, and toxicity outcomes. World J. Urol. 2019, 37, 1507–1515. [Google Scholar] [CrossRef]
- Murat, F.J.; Poissonnier, L.; Rabilloud, M.; Belot, A.; Bouvier, R.; Rouviere, O.; Chapelon, J.; Gelet, A. Mid-term Results Demonstrate Salvage High-Intensity Focused Ultrasound (HIFU) as an Effective and Acceptably Morbid Salvage Treatment Option for Locally Radiorecurrent Prostate Cancer. Eur. Urol. 2009, 55, 640–649. [Google Scholar]
- Crook, J.M.; Zhang, P.; Pisansky, T.M.; Trabulsi, E.J.; Amin, M.B.; Bice, W.; Morton, G.; Pervez, N.; Vigneault, E.; Catton, C.; et al. A Prospective Phase 2 Trial of Transperineal Ultrasound-Guided Brachytherapy for Locally Recurrent Prostate Cancer After External Beam Radiation Therapy (NRG Oncology/RTOG-0526). Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 335–343. [Google Scholar] [CrossRef]
- Ahmed, H.U.; Cathcart, P.; Chalasani, V.; Williams, A.; McCartan, N.; Freeman, A.; Kirkham, A.; Allen, C.; Chin, J.; Emberton, M. Whole-gland salvage high-intensity focused ultrasound therapy for localized prostate cancer recurrence after external beam radiation therapy. Cancer 2012, 118, 3071–3078. [Google Scholar] [CrossRef] [Green Version]
- Crouzet, S.; Blana, A.; Murat, F.J.; Pasticier, G.; Brown, S.C.W.; Conti, G.N.; Ganzer, R.; Chapet, O.; Gelet, A.; Chaussy, C.G.; et al. Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy: Multi-institutional analysis of 418 patients. BJU Int. 2017, 119, 896–904. [Google Scholar] [CrossRef] [Green Version]
- Berge, V.; Baco, E.; Dahl, A.A.; Karlsen, S.J. Health-related quality of life after salvage high-intensity focused ultrasound (HIFU) treatment for locally radiorecurrent prostate cancer. Int. J. Urol. 2011, 18, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Kalna, G.; Ismail, M.; Birrell, F.; Asterling, S.; McCartney, E.; Greene, D.; Davies, J.; Leung, H.Y. Prostate Gland Lengths and Iceball Dimensions Predict Micturition Functional Outcome Following Salvage Prostate Cryotherapy in Men with Radiation Recurrent Prostate Cancer. PLoS ONE 2013, 8, e069243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Ruckle, H.C.; Schlaifer, A.E.; El-Shafei, A.; Yu, C.; Jones, J.S. The Effect of Androgen Deprivation Therapy Before Salvage Whole-gland Cryoablation After Primary Radiation Failure in Prostate Cancer Treatment. Urology 2015, 85, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, K.M.; Billia, M.; Al-Zahrani, A.; Williams, A.; Goodman, C.; Arifin, A.; Violette, P.; Bauman, G.; Chin, J.L. Long-Term Oncologic Outcomes of Salvage Cryoablation for Radio-Recurrent Prostate Cancer. J. Urol. 2016, 196, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.H.; Elshafei, A.; Agarwal, G.; Ruckle, H.; Pow-Sang, J.; Jones, J.S. Salvage focal prostate cryoablation for locally recurrent prostate cancer after radiotherapy: Initial results from the cryo on-line data registry. Prostate 2015, 75, 1–7. [Google Scholar] [CrossRef]
- De Castro Abreu, A.L.; Bahn, D.; Leslie, S.; Shoji, S.; Silverman, P.; Desai, M.M.; Gill, I.; Ukimura, O. Salvage focal and salvage total cryoablation for locally recurrent prostate cancer after primary radiation therapy. BJU Int. 2013, 112, 298–307. [Google Scholar] [CrossRef]
- Pisters, L.L.; Rewcastle, J.C.; Donnelly, B.J.; Lugnani, F.M.; Katz, A.E.; Jones, J.S. Salvage Prostate Cryoablation: Initial Results From the Cryo On-Line Data Registry. J. Urol. 2008, 180, 559–564. [Google Scholar] [CrossRef]
- Ng, C.K.; Moussa, M.; Downey, D.B.; Chin, J.L. Salvage Cryoablation of the Prostate: Followup and Analysis of Predictive Factors for Outcome. J. Urol. 2007, 178, 1253–1257. [Google Scholar] [CrossRef]
- Henríquez López, I.; González-San Segundo, C.; Vegas, J.O.; Gutierrez, C.; Hervas, A.; Cabeza Rodriguez, M.Á.; Albarrán, J.V.; Villalba, S.R.; Gonzalez, A.; Pardo, G.S.; et al. Salvage brachytherapy for locally-recurrent prostate cancer after radiation therapy: A comparison of efficacy and toxicity outcomes with high-dose rate and low-dose rate brachytherapy. Radiother. Oncol. 2019, 141, 156–163. [Google Scholar]
- Kollmeier, M.A.; McBride, S.; Taggar, A.; Anderson, E.; Lin, M.; Pei, X.; Weiji, S.; Voros, L.; Cohen, G.; Yamada, Y.; et al. Salvage brachytherapy for recurrent prostate cancer after definitive radiation therapy: A comparison of low-dose-rate and high-dose-rate brachytherapy and the importance of prostate-specific antigen doubling time. Brachytherapy 2017, 16, 1091–1098. [Google Scholar] [CrossRef]
- Siddiqui, K.M.; Billia, M.; Williams, A.; Alzahrani, A.; Chin, J.L. Comparative morbidity of ablative energy-based salvage treatments for radio-recurrent prostate cancer. J. Can. Urol. Assoc. 2015, 9, 325–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanthabalan, A.; Peters, M.; Van Vulpen, M.; McCartan, N.; Hindley, R.G.; Emara, A.; Moore, C.M.; Arya, M.; Emberton, M.; Ahmed, H.U. Focal salvage high-intensity focused ultrasound in radiorecurrent prostate cancer. BJU Int. 2017, 120, 246–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bomers, J.G.R.; Overduin, C.G.; Jenniskens, S.F.M.; Cornel, E.B.; van Lin, E.N.J.T.; Sedelaar, J.P.M.; Fütterer, J.J. Focal Salvage MR Imaging–Guided Cryoablation for Localized Prostate Cancer Recurrence after Radiotherapy: 12-Month Follow-up. J. Vasc. Interv. Radiol. 2020, 31, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.P.; ElShafei, A.; Aminsharifi, A.; Khalifa, A.O.; Polascik, T.J. Salvage Focal Cryotherapy Offers Similar Short-term Oncologic Control and Improved Urinary Function Compared With Salvage Whole Gland Cryotherapy for Radiation-resistant or Recurrent Prostate Cancer. Clin. Genitourin. Cancer 2020, 18, e260–e265. [Google Scholar] [CrossRef]
- Safavy, S.; Jabaji, R.B.; Lu, S.M.; Slezak, J.M.; Cosmatos, H.A.; Williams, S.G.; Finley, D.S. Salvage Cryoablation for Radiorecurrent Prostate Cancer: Initial Experience at a Regional Health Care System. Perm. J. 2019, 23, 1–5. [Google Scholar]
- Gotto, G.T.; Yunis, L.H.; Vora, K.; Eastham, J.A.; Scardino, P.T.; Rabbani, F. Impact of Prior Prostate Radiation on Complications After Radical Prostatectomy. J. Urol. 2010, 184, 136–142. Available online: https://pubmed.ncbi.nlm.nih.gov/20478594/ (accessed on 17 October 2020). [CrossRef]
- Stephenson, A.J.; Scardino, P.T.; Bianco, F.J.; DiBlasio, C.J.; Fearn, P.A.; Eastham, J.A. Morbidity and functional outcomes of salvage radical prostatectomy for locally recurrent prostate cancer after radiation therapy. J. Urol. 2004, 172, 2239–2243. [Google Scholar] [CrossRef]
- Cespedes, R.D.; Pisters, L.L.; Von Eschenbach, A.C.; McGuire, E.J. Long-term followup of incontinence and obstruction after salvage cryosurgical ablation of the prostate: Results in 143 patients. J. Urol. 1997, 157, 237–240. [Google Scholar] [CrossRef]
- Boissier, R.; Sanguedolce, F.; Territo, A.; Gaya, J.; Huguet, J.; Rodriguez-Faba, O.; Regis, F.; Gallioli, A.; Vedovo, F.; Martinez, C.; et al. Partial salvage cryoablation of the prostate for local recurrent prostate cancer after primary radiotherapy: Step-by-step technique and outcomes. Urol. Video J. 2020, 7, 100040. [Google Scholar] [CrossRef]
- Mottet, P.N.; Cornford, R.C.N.; van den Bergh, E.; Briers, M.; De Santis, S.; Fanti, S.; Gillessen, J.; Grummet, A.M.; Henry, T.B.; Lam, M.D.; et al. EAU Guidelines: Prostate Cancer | Uroweb. European Association of Urology. 2020. Available online: https://uroweb.org/guideline/prostate-cancer/#4 (accessed on 17 October 2020).
- Gomez-veiga, F.; Mari, A.; Alvarez, L.; Rodriguez, I.; Fernandez, C.; Pertega, S.; Pertega, S.; Candal, A. Brachytherapy for the treatment of recurrent prostate cancer after radiotherapy or radical prostatectomy. BJUI Suppl. 2012, 109, 17–21. [Google Scholar] [CrossRef]
- Philippou, Y.; Parker, R.A.; Volanis, D.; Gnanapragasam, V.J.; Catto, J. Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus Nonsurgical Therapies for Radiorecurrent Prostate Cancer: A Meta–Regression Analysis. Eur. Urol. Focus 2016, 2, 158–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Name | Study Type | Location | Sample Size | Primary Treatment | Androgen Deprivation Therapy | Salvage Modality | Reported Outcomes |
|---|---|---|---|---|---|---|---|
| Surgical | |||||||
| Mohler 2019 [26] | Prospective | USA | 41 | 58.5%: EBRT 26.8%: BT 14.6%: Combined | 22%: after recurrence | RP | Continence Potency |
| Devos 2019 (a) [41] | Retrospective | Belgium | 25 | 68%: EBRT 32%: BT | 36%: N-AD | RP | Continence |
| Seabra 2009 [27] | Prospective | Brazil | 42 | EBRT | - | RP | Continence Potency |
| Ward 2005 [40] | Retrospective | USA | 138 (49: 1967–1990) (89: 1990–2001) | 92%: EBRT 7.2%: BT 0.8%: Combined | 38%: N-AD 61%: AD | RP | Continence |
| HIFU | |||||||
| Hostiou 2019 [35] | Prospective maintenance, Retrospective analysis | France | 50 | BT | 16%: at biochemical failure | HIFU | Continence Potency IPSS IIEF QOL (EORTC QLC-28) |
| Devos 2019 (b) [41] | Retrospective | Belgium | 27 | EBRT | 31%: N-AD | HIFU | |
| Crouzet 2017 [45] | Retrospective | France | 418 | EBRT | none within 3 months of HIFU | HIFU | Continence |
| Jones 2018 [31] | Prospective trial | USA | 100 | EBRT | none within 3 months of HIFU | HIFU | Continence Potency |
| Kanthabalan 2017 [57] | Retrospective | UK | 150 | 96.7%: EBRT 3.3%: EBRT + BT | 45.3%: pre-salvage | HIFU | Continence IIEF |
| Shah 2016 [32] | Prospective | UK | 50 | EBRT | 52%: after biochemical failure | HIFU | Continence IIEF |
| Siddiqui 2015 (a) [56] | Retrospective | UK | 65 | 93.8%: EBRT 6.2%: BT | 21%: AD | HIFU | Continence IIEF |
| Baco 2014 [33] | Prospective | France & Norway | 48 | 95.8%: EBRT 4.2%: BT | 22.9%: N-AD | HIFU | Continence IPSS IIEF ICS (A) ICS (B) EORTC QLC-30 |
| Crouzet 2012 [34] | Prospective | France | 290 | EBRT | 50%: prior to HIFU | HIFU | Continence |
| Berge 2011 [46] | Retrospective | Norway | 61 | EBRT | 19% | HIFU | UCLA-PCI |
| Ahmed 2011 [44] | Retrospective | Canada and UK | 84 | EBRT | 35.4%: N-AD | HIFU | Continence IPSS IIEF RAND-SF 36 |
| Berge 2010 [36] | Prospective | Norway | 46 | EBRT | 17.4%: N-AD | HIFU | Continence Potency |
| Murat 2009 [42] | Retrospective | France | 167 | EBRT | 56.8%: post primary therapy or AD | HIFU | Continence |
| Cryotherapy | |||||||
| Bomers 2020 [58] | Retrospective | Netherlands | 62 | 64.5%: EBRT 33.9%: BT 1.6%: Combined | prior use: 37.1% | MR imaging–guided CT | IPSS IIEF |
| Tan 2020 (a) [59] | Retrospective | COLD registry | 385 | 75%: EBRT 16%: BT 9%: Combined | 26.4% | Focal CT: 72 patients | Continence Potency |
| Tan 2020 (b) [59] | Retrospective | COLD registry | 385 | 75%: EBRT 16%: BT 9%: Combined | 31.3%: prior to salvage | Total CT: 313 patients | |
| Safavy 2019 [60] | Retrospective | USA | 75 | 77.3%: EBRT 21.3%: BT 1.3%: missing | 25.3%: were subjected to ADT | CT | Continence |
| Siddiqui 2016 [49] | Retrospective | Canada | 157 | EBRT or EBRT + BT or BT | 71%: prior to salvage | CT | Continence |
| Li 2015 [48] | Retrospective | COLD registry | 740 | Radiotherapy | 34.3%: prior to salvage | CT | Continence Potency |
| Siddiqui 2015 (b) [56] | Retrospective | UK | 65 | 97%: EBRT3%: BT | 13%: AD | CT 1995–1998 | |
| Siddiqui 2015 (c) [56] | Retrospective | UK | 65 | EBRT | 18%: AD | CT 2002–2004 | |
| Li 2014 [50] | Retrospective | COLD registry | 91 | 25: BT 44: EBRT 3: Combined | 35.2%: N-AD | CT | Continence Potency |
| Ahmad 2013 [47] | Retrospective | UK | 283 | Radiotherapy | - | CT | Continence Potency |
| De Castro Abreu 2013 (a) [51] | Retrospective | USA | 25 | 44%: EBRT 32%: Proton beam 20%: BT 4%: BT + EBRT | none during study period before recurrence | Focal CT, UL | Continence Potency |
| De Castro Abreu 2013 (b) [51] | Retrospective | USA | 25 | 44%: EBRT 20%: Proton beam 28%: BT 8%: BT + EBRT | none during study period before recurrence | Total CT, BL | |
| Pisters 2008 [52] | Retrospective | USA | 279 | 78.1%: EBRT 11.5%: BT 7.2%: Combined 3.2%: unknown | 50.9%: prior to salvage | CT | Continence |
| Ismail 2007 [37] | Prospective case series | UK | 100 | Radiotherapy | 46%: N-AD | CT | Continence PotencyIPSS |
| Ng 2007 [53] | Retrospective | USA | 187 | 97.9%: EBRT 1.6%: BT 0.5%: Combined | 32%: started ADT due to disease progression | CT | Continence |
| Clarke 2007 [38] | Prospective | USA | 47 | EBRT or BT or both | - | CT | Continence |
| Robinson 2006 [39] | Prospective PHASE II study | Canada | 46 | EBRT | 26.1%: pre cryosurgery 15.2% post crysurgery | CT | Potency UCLA-PCI |
| Donnelly 2005 [28] | Prospective | Canada | 46 | EBRT | 6.5%: AD | Ultrasound-guided CT | Continence Potency |
| Brachytherapy | |||||||
| van Son 2020 [29] | Prospective | Netherlands | 50 | 50%: EBRT 50%: BT | 8%: N-AD 14%: AD | BT | Continence Potency IPSS IIEF |
| Crook 2019 [43] | Retrospective | Canada | 92 | EBRT | 16%: at study entry | BT | Continence |
| Lopez 2019 (a) [54] | Retrospective | Spain | 73 | EBRT or BT | 29%: AD | HDR BT | Continence |
| Lopez 2019 (b) [54] | Retrospective | Spain | 44 | EBRT or BT | 18%: AD | LDR BT | |
| Kollmeier 2017 [55] | Retrospective | USA | 98 | 87.8%: EBRT 10.2%: BT 2%: Combined | 45%: at salvage | 37.8%: LDR BT 62.2%: HDR BT | Continence IPSS |
| Yamada 2014 [30] | Prospective PHASE II study | USA | 42 | EBRT | 43%: N-AD | BT | Continence IPSS IIEF |
| Author and Year of Publication | Functional Outcomes Sample | Incontinence Rate (General) | Mild UI ¥ | Severe UI £ |
|---|---|---|---|---|
| Surgery | ||||
| Mohler 2019 [26] | 40 (6 months) 34 (12 months) 32 (24 months) 24 (36 months) | - | - | 88% 85% 63% 42% |
| Devos 2019 (a) | 25 | 56% | 28% | 28% |
| Seabra 2009 [27] | 42 | 72% | - | 72% |
| Ward 2005 [40] | 130 | 48% | At least 20% ** | Less than 28% ** |
| HIFU | ||||
| Hostiou 2019 [35] | 50 | - | 14% | 42% |
| Devos 2019 (b) | 27 | 22% | 11% | 11% |
| Crouzet 2017 [45] | 388 | 49% | 33% | 16% |
| Jones 2018 [31] | 100 | 47% | 18% | 29% |
| Kanthabalan 2017 [57] | 48 | 22% * | - | - |
| Shah 2016 [32] | 26 | 31% * | - | - |
| Siddiqui 2015 (a) [56] | 65 | 7.50% | 3% | 4.5% |
| Baco 2014 [33] | 48 | 25.30% | 17% | 8.3% |
| Crouzet 2012 [34] | 290 | 46% | 37% | 16.8% |
| Berge 2011 [46] | 61 | - | 44% | 16% |
| Ahmed 2012 [44] | 84 | 38% | N/A § | N/A |
| Berge 2010 [36] | 35 | 60.7% | 43.4% | 17.3% |
| Murat 2009 [42] | 167 | 49.50% | 40% | 9.5% |
| Cryotherapy | ||||
| Bomers 2020 [58] | 44 | 3.2% | - | 3.2% |
| Tan 2020 (a) ₡ [59] | 72 | 9.30% | N/A | N/A |
| Tan 2020 (b) ₡ [59] | 313 | 15.10% | N/A | N/A |
| Safavy 2019 [60] | 75 | 25.30% * | - | - |
| Siddiqui 2016 [49] | 157 | 48% | 44% | 4% |
| Li 2015 [48] | 740 | No pre-SC ADT: 33.3% * With pre-SC ADT: 23.3% * | - | - |
| Siddiqui 2015 (b) [56] | 65 | 52% | 49% | 3% |
| Siddiqui 2015 (c) [56] | 65 | 37.50% | 31% | 6.5% |
| Li 2014 [50] | 91 | 5.50% * | - | - |
| Ahmad 2013 [47] | 283 | 12% * | - | - |
| De Castro Abreu 2013 (a) [51] | 25 | 0% * | - | - |
| De Castro Abreu 2013 (b) [51] | 25 | 13% * | - | - |
| Pisters 2008 [52] | 137 | 10.20% * | - | - |
| Ismail 2007 [37] | 100 | 13% | Less than 7% ** | At least 6% ** |
| Ng 2007 [53] | 187 | 40% + | 37% | 3% |
| Clarke 2007 [38] | 47 | 0% | 0% | 0% |
| Donnelly 2005 [28] | 46 | 6.50% | N/A | N/A |
| Brachytherapy | ||||
| Van Son 2020 [29] | 50 | 8% | - | 8% |
| Crook 2019 [43] | 87 | 4.6% | - | 4.6% |
| Henríquez López 2019 (a) [54] | 73 | 26.70% * | - | - |
| Henríquez López 2019 (b) [54] | 44 | 4.50% * | - | - |
| Kollmeier 2017 [55] | 98 | 11% * | - | - |
| Yamada 2014 [30] | 42 | 2.40% | - | 2.4% |
| Author and Year of Publication | Functional Outcomes Follow-Up Sample | Pre-op ED Rate | Post-op ED Rate | Follow-Up Time for EF (Months) |
|---|---|---|---|---|
| Surgical | ||||
| Mohler 2019 [26] | 40 at 3 months 40 at 6 months 24 at 36 months | 32% [38] | 90% at 3 months 78% at 6 months 25% at 36 months | - |
| Seabra 2009 [27] | 42 | - | 74% | - |
| HIFU | ||||
| Hostiou 2019 A [35] | 50 | 50% | 76% | 12 |
| Jones 2018 [31] | 100 | 53% | 88% | 12 |
| Kanthabalan 2017 B [57] | 48 | - | - | - |
| Shah 2016 A [32] | 26 | - | - | - |
| Siddiqui 2015 (a) [56] | 65 | - | - | - |
| Baco 2014 B [33] | 48 | - | - | - |
| Ahmed 2012 B [44] | 84 | - | - | - |
| Berge 2010 [36] | 37 | 78.8% [33] | 94.6% | - |
| Cryotherapy | ||||
| Bomers 2020 B [58] | 44 | - | - | - |
| Tan 2020 (a) ¥ [59] | 72 | - | 52.60% | 12 |
| Tan 2020 (b) ¥ [59] | 313 | - | 59.60% | 12 |
| Li 2015 [48] | 740 | - | No pre-SC ADT: 71.3% With pre-SC ADT: 84.5% | 12 |
| Li 2014 [50] | 91 | 70% | 85% | - |
| Ahmad 2013 [47] | 283 | - | 83% | - |
| De Castro Abreu 2013 (a) [51] | 25 | 72% | 92% | - |
| De Castro Abreu 2013 (b) [51] | 25 | 84% | 100% | - |
| Ismail 2007 [37] | 63 | - | 86% | - |
| Robinson 2006 [39] | 40 | 67.90% | 86.20% | 24 |
| Donnelly 2005 [28] | 46 | 72% | 84.90% | 6 |
| Brachytherapy | ||||
| Van Son 2020 B [29] | 50 | 18% grade III | 40% grade III 22% grade II | - |
| Yamada 2014 [30] | 42 | - | - | - |
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 * | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ahmad 2013 [47] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | N/A | 1 | 1 | 11 |
| Ahmed 2011 [44] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 0 | 1 | 8 |
| Baco 2014 [33] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 1 | 0 | 9 |
| Berge 2010 [36] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 1 | 0 | 9 |
| Berge 2011 [46] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 10 |
| Bomers 2020 [58] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 10 |
| Clarke 2007 [38] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | N/A | 1 | 1 | 9 |
| Crook 2019 [43] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 10 |
| Crouzet 2012 [34] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 9 |
| Crouzet 2017 [45] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 9 |
| De castro Abreu 2013 [51] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | N/A | 1 | 0 | 8 |
| Devos 2019 (HIFU) [41] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 0 | 8 |
| Devos 2019 (RP) [41] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | N/A | 0 | 1 | N/A | 1 | 0 | 7 |
| Donnelly 2005 [28] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | N/A | 1 | 0 | 7 |
| Hostiou 2019 [35] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | N/A | 1 | 1 | 11 |
| Ismail 2007 [37] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 10 |
| Jones 2018 [31] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 1 | 0 | 8 |
| Kanthabalan 2017 [57] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 0 | 1 | 10 |
| Kollmeier 2017 [55] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 8 |
| Li 2014 [50] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | N/A | 1 | 1 | 8 |
| Li 2015 [48] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | N/A | 1 | 1 | 10 |
| Lopez 2019 [54] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | N/A | 1 | 1 | 11 |
| Mohler 2019 [26] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | N/A | N/A | 0 | 0 | N/A | 1 | 0 | 7 |
| Murat 2009 [42] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 9 |
| NG 2007 [53] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | N/A | 1 | 1 | 8 |
| Pisters 2008 [52] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 0 | 0 | 8 |
| Robinson 2006 [39] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 0 | 9 |
| Safavy 2019 [60] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 0 | 10 |
| Seabra 2009 [27] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | N/A | N/A | 0 | 0 | N/A | 1 | 0 | 6 |
| Shah 2016 [32] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | N/A | 0 | 1 | 10 |
| Siddiqui 2015 [56] | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | N/A | 1 | 0 | 7 |
| Siddiqui 2016 [49] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 9 |
| Tan 2020 [59] | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | N/A | 1 | 1 | 10 |
| Van Son 2020 [29] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 1 | 10 |
| Ward 2005 [40] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | N/A | N/A | 0 | 1 | N/A | 1 | 1 | 8 |
| Yamada 2014 [30] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | N/A | 1 | 0 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abufaraj, M.; Siyam, A.; Ali, M.R.; Suarez-Ibarrola, R.; Yang, L.; Foerster, B.; Shariat, S.F. Functional Outcomes after Local Salvage Therapies for Radiation-Recurrent Prostate Cancer Patients: A Systematic Review. Cancers 2021, 13, 244. https://doi.org/10.3390/cancers13020244
Abufaraj M, Siyam A, Ali MR, Suarez-Ibarrola R, Yang L, Foerster B, Shariat SF. Functional Outcomes after Local Salvage Therapies for Radiation-Recurrent Prostate Cancer Patients: A Systematic Review. Cancers. 2021; 13(2):244. https://doi.org/10.3390/cancers13020244
Chicago/Turabian StyleAbufaraj, Mohammad, Abdelmuez Siyam, Mustafa Rami Ali, Rodrigo Suarez-Ibarrola, Lin Yang, Beat Foerster, and Shahrokh F. Shariat. 2021. "Functional Outcomes after Local Salvage Therapies for Radiation-Recurrent Prostate Cancer Patients: A Systematic Review" Cancers 13, no. 2: 244. https://doi.org/10.3390/cancers13020244