1. Introduction
Noninvasive imaging techniques such as electrical impedance tomography (EIT) are valuable tools for medical applications. EIT is used to image the electrical conductivity of tissues in the human body. EIT usage was first suggested in the 1970s [
1]. Despite its relatively low cost, safety, and high temporal resolution, EIT has not been as widely adopted as other medical imaging methods, such as magnetic resonance imaging (MRI) and computed tomography (CT) [
2,
3].
The applications of functional EIT include pulmonary investigations [
4], cardiac and gastrointestinal tract monitoring, breast cancer screening, and functional brain imaging [
5]. Multiple devices have been introduced for clinical research [
6], mainly in applications with functional imaging, such as bedside lung monitoring. Other applications, such as temperature estimation where accurate quantitative conductivity (or change in conductivity) reconstruction is needed, are more challenging compared with those in which only the volume with high dielectric change must be reconstructed.
One of the main challenges in EIT is that image reconstruction from measured voltages is an ill-posed problem [
7]. Changes in the whole domain correspond to an infinite number of degrees of freedom (DOF) that must be reconstructed from a limited number of electrode measurements. Nevertheless, knowledge about distribution smoothness adds constraints, and regularization methods can be employed to facilitate reconstruction. Another issue with EIT is that impedances are affected by the entire volume rather than a single slice. Therefore, 2D reconstructions are merely an approximation of the real 3D problem [
8]. While linearization methods combined with prior knowledge about the conductivity distribution and difference imaging have been used to further improve image reconstruction, the problem is nonlinear. Nonlinear reconstruction methods are more sensitive to inaccuracies in electrode models and positions. The literature on reconstruction algorithms for EIT [
9] suggests that linear reconstruction methods should be combined with nonlinear iterative approaches to improve overall accuracy. From an instrumentation perspective, measurement noise, electrode positioning accuracy, signal generation, and sensing techniques impact overall EIT quality [
10]. Further advances in EIT require improvements in both instrumentation and image reconstruction. Improvements are especially needed for applications that require the quantitative imaging of conductivity.
A potential application of EIT is in hyperthermic oncology. Hyperthermia (HT) therapy aims to selectively heat tumor tissue to temperatures ranging from 40 °C to 45 °C for a duration of about one hour. It is typically used as an adjuvant to radio- and/or chemotherapy in cancer treatment. In the case of deep-seated tumors, selective heating is usually achieved through coherent interference of electromagnetic (EM) energy from multiple radiating elements [
11]. A significant challenge is noninvasive temperature monitoring in deep-seated tissue. The achieved temperature is difficult to predict, but it is important for tracking the achieved thermal dose in the tumor and avoiding potential treatment-limiting hotspots in healthy tissue. Treatment planning [
12,
13], which involves patient-specific EM simulation, optimization of energy deposition, and thermal prediction of the treatment, has been introduced as a tool for improving the prediction of thermal distribution. However, high uncertainty about the actual temperatures (e.g., due to perfusion changes during treatment) remains [
14,
15,
16]. Research progress has been made in noninvasive monitoring using magnetic resonance thermometry (MRT) [
17], but the accuracy of measurement is susceptible to patient movements, magnetic field drift over time, and limited sensitivity in fatty tissues, among others. In addition, the cost associated with MRT and the integration complexity with HT are high [
18]. Alternatively, EIT can offer a low-cost, low-complexity solution for estimating temperature increases and perfusion changes during HT treatment.
Temperature elevation impacts tissue conductivity in two different ways. First, temperature changes the conductivity of intra- and extracellular fluids, which can be modeled by a linear relationship and described by a temperature coefficient (
)—the ratio of relative conductivity increases per degree centigrade. Second, in tissues in which thermoregulation-induced perfusion changes (e.g., vasodilatory response) are high, fluid flow in the extracellular environment increases, resulting in additional tissue conductivity change. At lower frequencies, current flows mainly in the extracellular region, whereas at higher frequencies, current flow is more uniform across all tissue compartments. Multifrequency EIT is considered as a method to distinguish changes in conductivity directly related to temperature (i.e.,
-related part) from changes in conductivity due to perfusion increase [
19]. Earlier studies have achieved temperature estimation accuracies ranging from 1.5 °C to 5 °C [
20]. The results of these and other studies [
21,
22,
23,
24,
25] suggest that to enable clinical EIT for HT and ablation treatment monitoring, improvements in conductivity reconstruction and temperature estimation are essential and consequently require accurate models of temperature-induced conductivity changes and the ability to distinguish temperature-related changes from tissue changes or damage-related changes, both permanent and temporary.
Recently, there has been increased interest and progress in applying EIT as a monitoring tool for thermal ablation, both in experimental and simulation studies [
26,
27,
28,
29], which motivates revisiting EIT for HT monitoring. New tools for EIT simulations have been introduced [
30,
31], and the computational power has increased considerably. Additionally, developments in tissue segmentation [
32], combined with knowledge about tissue properties [
33], enable the simulation of patient-specific treatment scenarios. Similarly, more realistic anatomical models can be used to perform sensitivity analyzes to improve the design of instruments. Most experimental studies in EIT are performed in tanks with simple geometrical shapes and few objects with different conductivities; hence, results cannot directly be translated to real human application. Since human anatomy is highly heterogeneous and geometrically complex, accurate representation in a model requires high resolution and many discretization elements. Notably, higher resolution negatively impacts reconstruction accuracy since total error minimization involves residuum minimization for more degrees of freedom, while the number of voltage electrode measurements remains the same [
34].
Accurate temperature and/or perfusion estimation requires accurate knowledge about the relationship between temperature and conductivity, in addition to accurate conductivity imaging. In this paper, we focus on the achievable EIT reconstruction accuracy by using existing tools, such as electrical impedance tomography and diffuse optical tomography reconstruction (EIDORS) [
31]), in conjunction with high-resolution anatomical models [
35]. We aim to exploit HT treatment planning-based prior information and investigate the reconstruction of conductivity changes in the range expected for the given application. We also identify potential practical issues specific to hyperthermic oncology and their impact on the accuracy of conductivity change reconstruction to further improve temperature estimation.
2. Materials and Methods
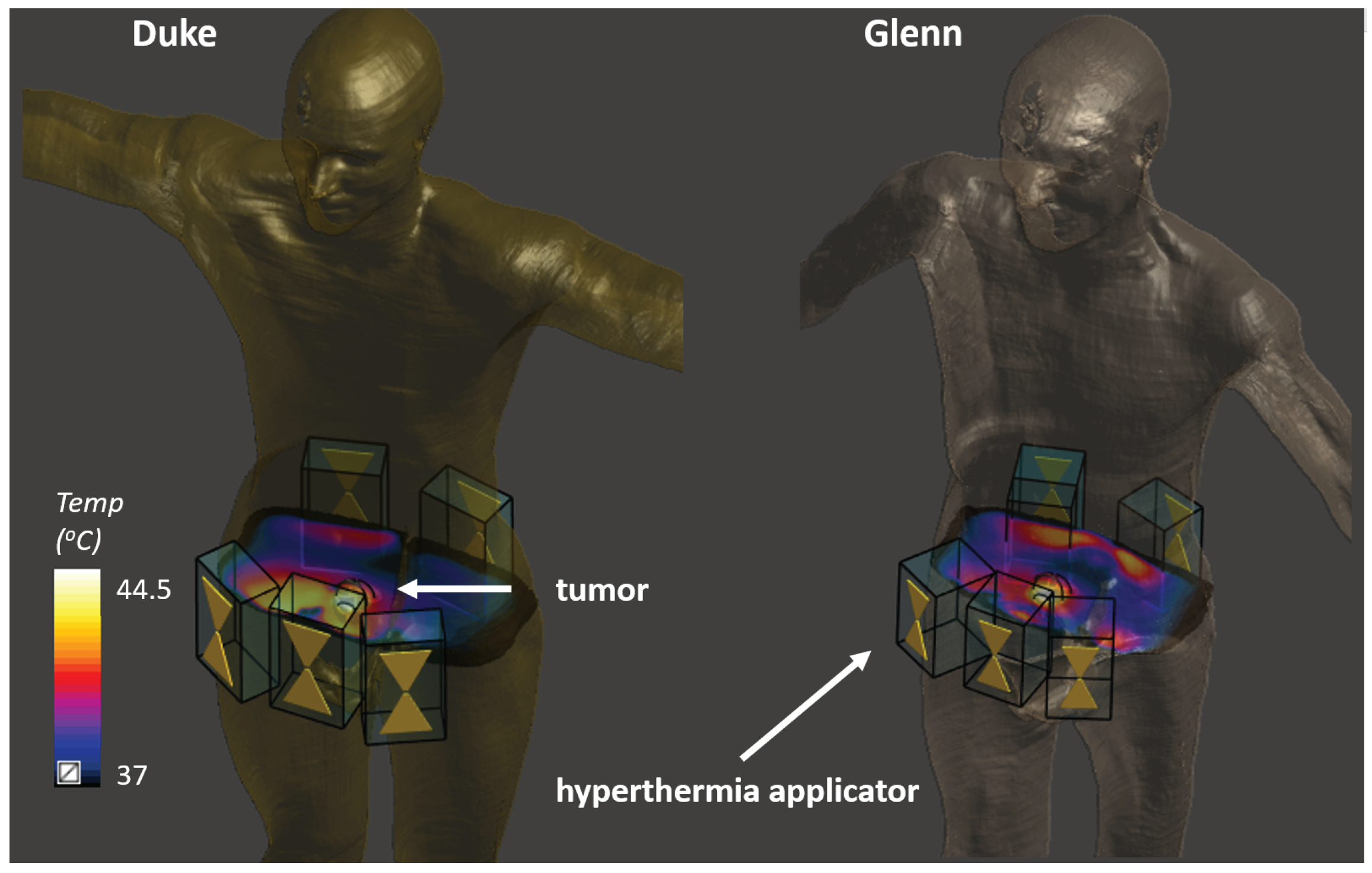
To investigate the potential application of EIT in HT treatment planning and treatment monitoring, we performed simulations using the Virtual Population (ViP) Duke (age: 34, height: 1.77 m, BMI: 22.4 kg/m
2) and Glenn (age: 84, height: 1.73 m, BMI: 20.4 kg/m
2) anatomical models [
35]. Two anatomical models were used to assess the impact of intersubject variability, as well as the importance of using personalized reference models. The models were discretized using a tetrahedral mesh in EIDORS v3.9. We first describe single iteration reconstruction using EIDORS. In
Section 2.2, we present novel reconstruction approaches capable of overcoming the limitations of existing methods in our application of interest, their implementation, and the investigation scenarios. While considering the high heterogeneity of the human body, we then determined if the reconstruction accuracy improved when using a tissue-dependent penalty (TiD) parameter. A sensitivity analysis regarding the location and size of the simulated region was also performed.
In difference imaging, a reference model with an initial conductivity assignment is required. The measured changes in the electrode voltages are used to reconstruct the changes in conductivity from the reference model. As reference patient models may display anatomical segmentation inaccuracies, we investigated their impact on the reconstruction accuracy by considering a scenario where a volume outside the prior region, i.e., the volume, where an increased sensitivity is achieved by applying a penalty value [
36], exhibited a large deviation (
) from the reference model conductivity (
).
Noise in the measurement acquisition chain is also present in practical implementations. We assessed the impact of different electrode voltage noise levels (signal-to-noise ratio, SNR) on reconstruction accuracy using different reconstruction parameter values.
Finally, a realistic bladder tumor HT treatment scenario was considered as an EIT application case, using the two anatomical models (different body shapes and heating patterns). The clinical value of treatment planning-based EIT and the importance of personalizing the reference model were also assessed.
2.1. Single Iteration Reconstruction
EIDORS includes multiple algorithms for two- and three-dimensional (2D/3D) image reconstruction. In this study, we used difference imaging reconstruction on a 3D body. Single iteration reconstruction assumes small variations in conductivity, for which the relationship between voltage and conductivity can be approximated linearly as follows:
where
is the Jacobian,
is the difference of the actual conductivity distribution and the reference value,
is a vector with electrode voltage differences of the actual measurement to the reference measurement, and
n is the measurement noise. Regularization techniques are used to solve this problem [
36,
37,
38]. We used the one-step linear Gauss–Newton method to estimate
by minimizing the sum of quadratic norms for:
The solution of the above formulation is:
To reduce computational time by decreasing the size of the matrix to be inverted,
B can be rewritten as follows:
where
and
. Effectively,
R is a diagonal regularization matrix scaled with the sensitivity of each element and
is a regularization parameter.
represents difference imaging EIT with identical channels. Two important and frequently used parameters in the reconstruction are the hyperparameter (
) and the penalty parameter. When known changes are likely to occur in a smaller subdomain, a penalty parameter is used to implement an increased sensitivity in this region:
, for
i in the subdomain. More details about derivations can be found in existing publications [
36,
37,
39].
2.2. Pipeline and Simulation Setup
The ViP Duke model comprised of tissue properties from the IT’IS tissue database [
33] was imported into EIDORS. Only a 20 cm portion of the torso (620 k elements) was used for further analysis.
Using difference imaging, we exploited prior information about the geometry and the conductivity distribution. Hence, we focused on reconstructing the conductivity change (
):
where reference conductivity (baseline for EIT difference reconstruction) is
.
is the function to solve the inverse problem using
v and
from the electrode voltages calculated from solving the forward problem or from current injection measurements for
, respectively
. The actual conductivity change (
) is referred to as “modified conductivity”, since a range of conductivity change configurations will be created by modifying the reference conductivity to investigate difference image reconstruction scenarios.
HT treatment planning workflows already include a tissue segmentation step. The segmented anatomical model can be assigned tissue properties, while considering the EIT frequency, to establish the reference model.
Difference imaging reconstruction is less sensitive to the modeling of the electrodes and contact impedance, as we assume the same conditions are present in both reference and additional measurements of the model to be reconstructed [
9,
40]. Therefore, we did not investigate the impact of the electrode parameters in this study; however, changes in the contact quality in experimental measurements will affect the reconstruction accuracy.
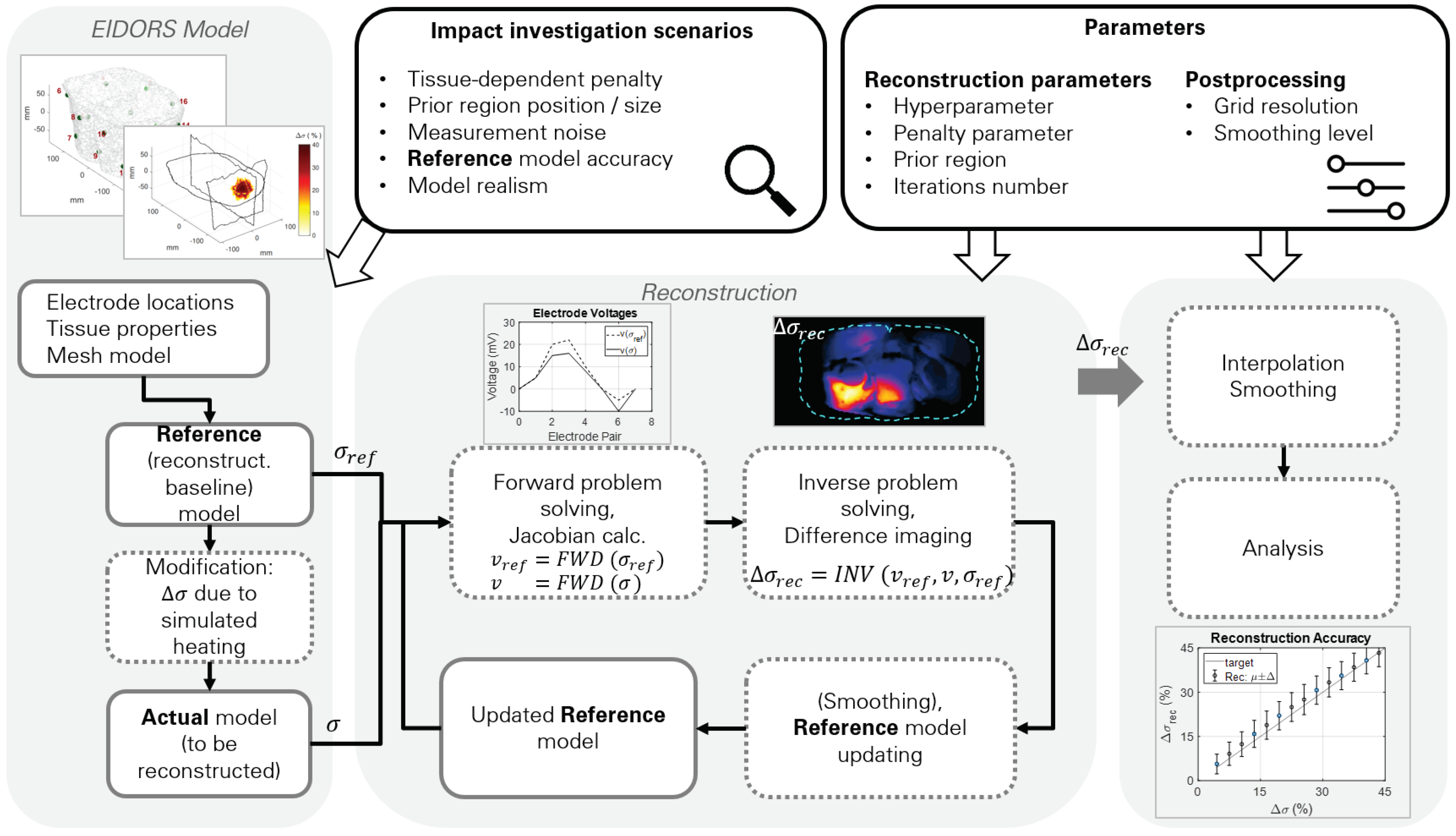
The reconstruction pipeline used in this study is shown in
Figure 1. The reference model includes the tissue conductivity assignments. In nonablative HT treatment, the target region can reach temperatures of up to 45 °C. In addition to the direct temperature-related conductivity change contribution modeled with temperature coefficients (∼2%/°C),
can also change due to perfusion changes, thus altering the tissue extracellular fluid distribution. From the reference model, modified models were created by changing the tissue conductivity by up to 40%, a level similar to the experimental measurement study by Gersing [
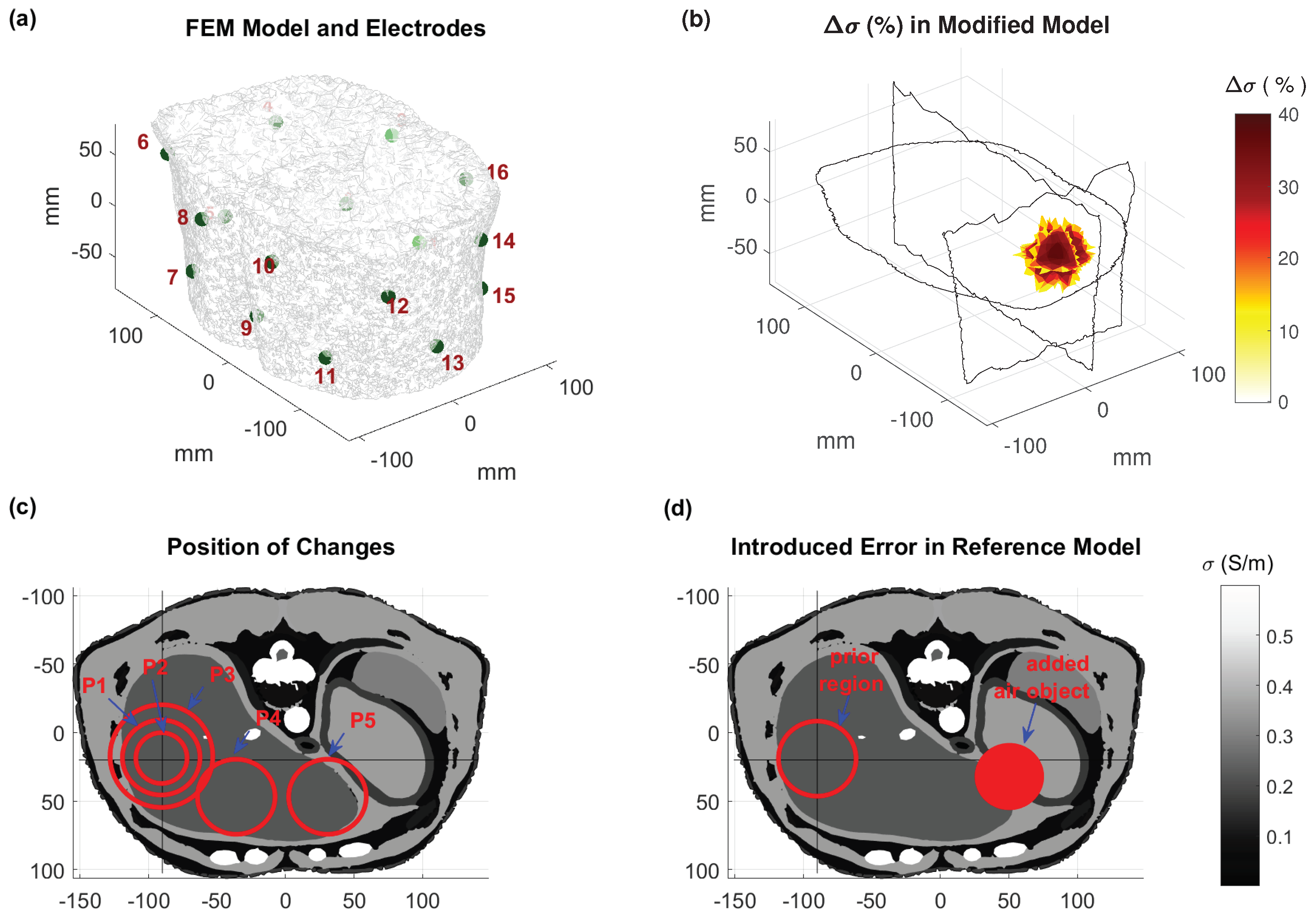
25]. The reference conductivity was multiplied by a 3D Gaussian shape mimicking heating during an HT treatment, as shown in
Figure 2. At the end of the simulation pipeline, we compared the reconstructed model conductivity with the modified model conductivity.
For current injection and measurement, we positioned electrodes in single nodes, distributed as two rows of eight electrodes to form an interleaved arrangement. Current injection was applied transversely through single pairs (1–8, 2–9, etc.) and the voltage difference was calculated in all adjacent pairs (
,
, etc.) except for the electrodes used for current injection. Injecting currents through transversal, nonadjacent electrodes increases the current density, and hence, the sensitivity of EIT to changes in deeper tissues. Theoretically, a larger number of electrodes should improve the reconstruction accuracy. However, for the same injected current, which is limited by safety considerations, the voltage difference of more densely placed electrodes will be lower and, in practice, we will obtain more voltage measurements with lower SNR. An additional drawback of using numerous electrodes is the increased computational reconstruction effort. The torso model and electrode placements used in this study are shown in
Figure 2.
In HT applications, the prior region can be determined either from the volume with highest HT power deposition or from a preliminary thermal simulation, which does not have to exactly reproduce the real patient tissue parameters. Although prior regions improve reconstruction by focusing on changes in a smaller volume, changes outside the prior region may be attributed to changes inside the region.
Simulations were interpolated to a structured rectilinear grid. A spatial averaging filter (cubic volume of 1.2 cm edge length) was applied to (%), mimicking the expected smoothness of the heat distribution in tissue. Finally, the reconstruction accuracy across different tissues was analyzed.
2.3. Investigation Scenarios
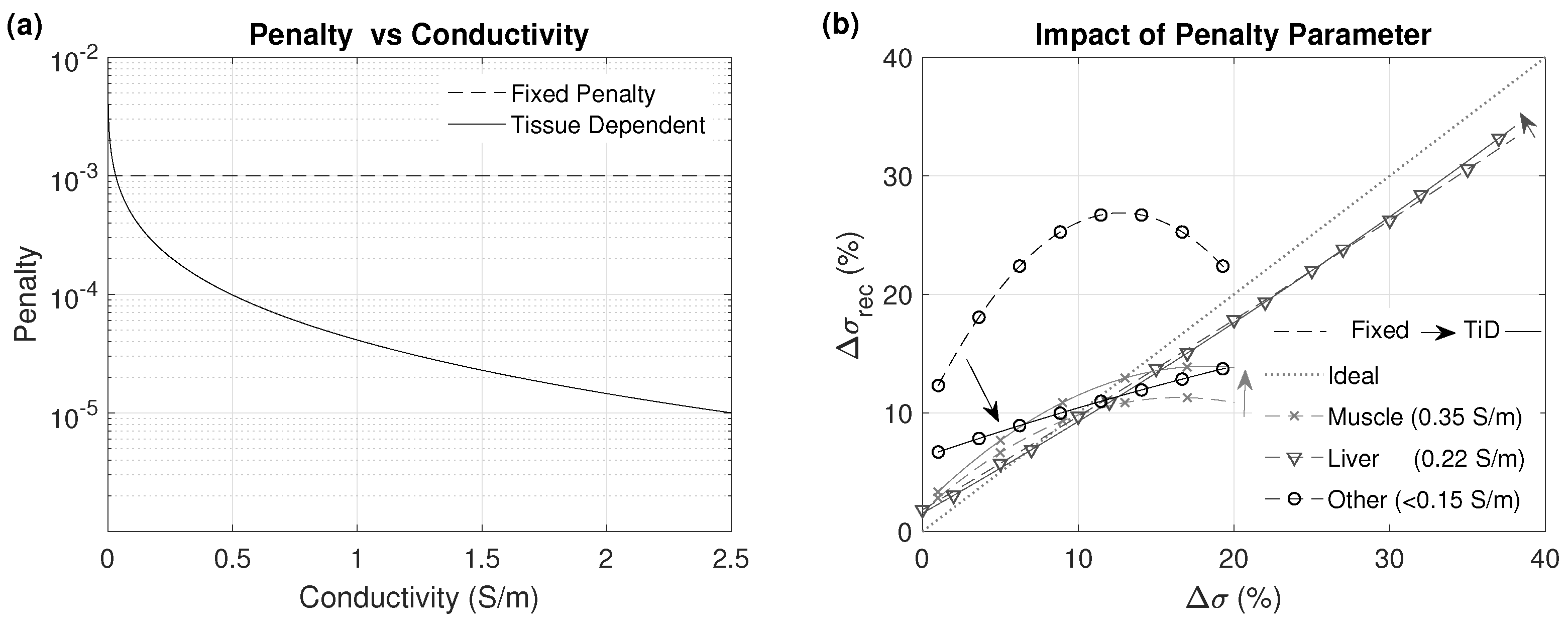
2.3.1. Tissue-Dependent Penalty
As the human body is highly heterogeneous, a wide range of low frequency values can be found, from close to 0 S/m (internal air) to over 0.36 S/m (muscle) and 3 S/m (urine). The prior region can encompass a multitude of tissues covering a broad range, which makes adequate change detection throughout the entire range without overestimation or underestimation challenging. Information from the reference model allows for the use of tissue-dependent penalty values, as constant penalty changes in low tissues are overestimated and changes in tissues with high , such as muscle, are underestimated, since the reconstruction algorithm minimizes the overall electrode voltage differences. In this study, we compared the reconstruction accuracy in different tissues when using a constant penalty value versus a tissue-dependent penalty in a single iteration reconstruction without applying any averaging or smoothing filter.
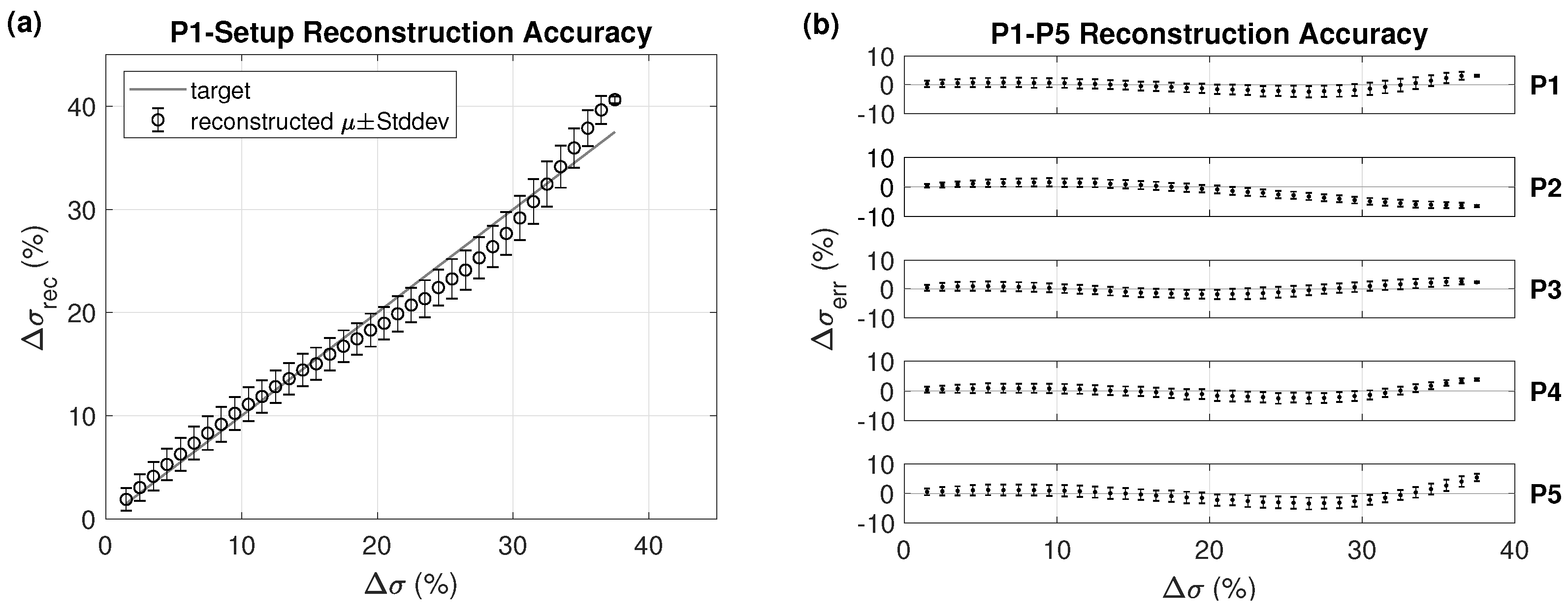
2.3.2. Region Location and Size
It is necessary to compare the reconstruction accuracy for different heating locations and sizes. The size of the region where the conductivity was changed should correspond to the typical extent of focused heating in HT treatment. For the first investigated location, spherical heating regions of different diameters were considered. A simulated heating was applied to a spherical region, as illustrated in
Figure 2, by multiplying the conductivity inside the sphere with
(
r: radial distance,
cm, peak
-increase of 40%). Depending on the location, the region can contain more than one tissue type. The modified regions are shown in
Table 1 and illustrated in
Figure 2. In these scenarios, we assumed that the prior region is perfectly known, and corresponds to the heated region.
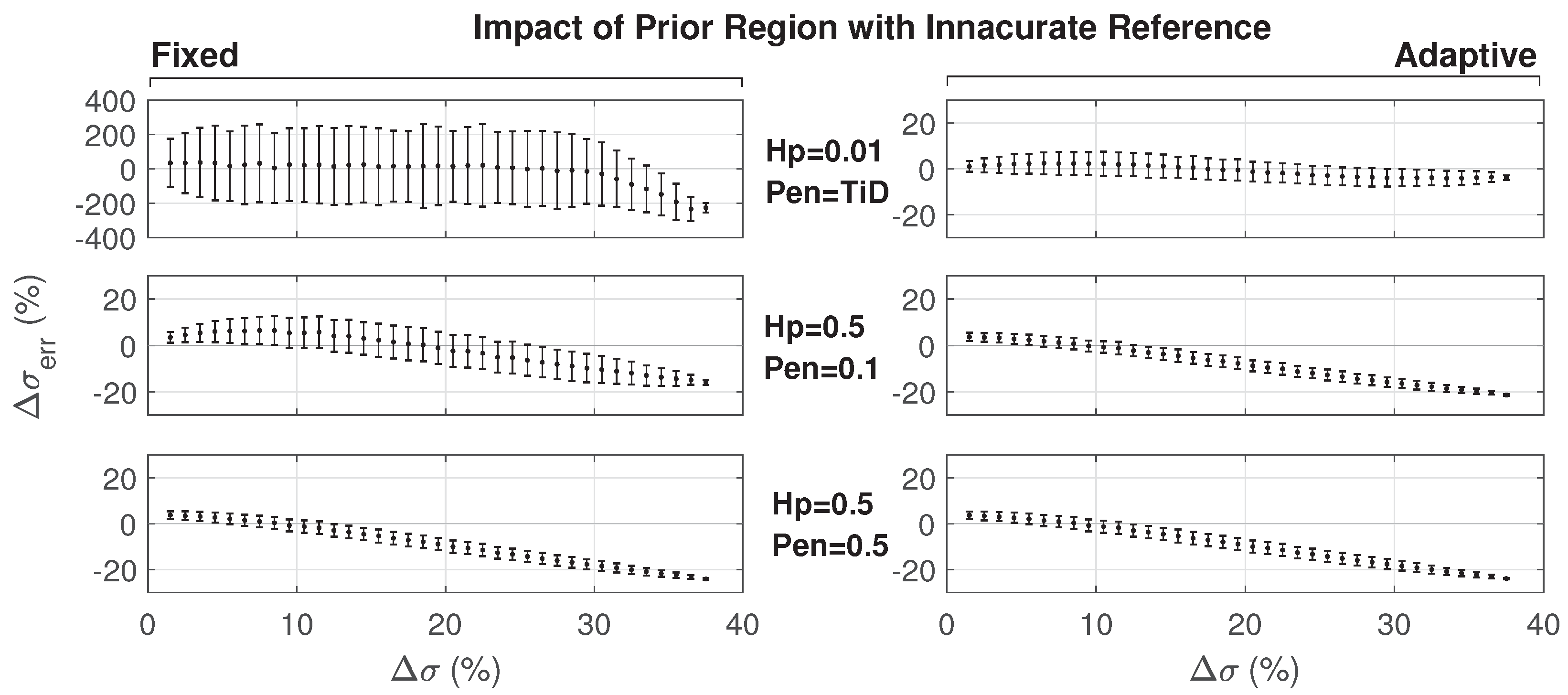
2.3.3. Impact of Inaccurate Reference Model
The reconstruction is sensitive to the accuracy of the reference model. Even if the reference model is accurate at the beginning of the treatment, organ shifts and air movement in the bowels can occur during the treatment, since the HT treatment duration is relatively long. We simulated such a scenario, where in addition to the changes due to the simulated heating, the modified model included a spherical region with a 50 mm diameter and
= 0 S/m (same as air), as illustrated in
Figure 2. The setup corresponds to P1 (
Table 1), such that results can be compared with the ideal case of an accurate reference model (see
Section 2.4 and
Section 3.3.1 regarding the impact of not using a personalized reference anatomy).
In addition to the iterative approach with a fixed prior region, we also introduced an adaptive prior region approach. An initial mask was obtained by reconstructing the conductivity change without prior region and thresholding locations, where a high change was obtained. Subsequently, the mask was used as a prior region and a relatively relaxed penalty value of 0.1 was assigned before obtaining an adapted or more focal mask. On the basis of the obtained reconstruction, three additional reconstruction iterations with a stricter penalty value were performed in the usual manner. This adaptive approach increased the reconstruction sensitivity to changes outside of the classic prior region. Both the change in the simulated heated region and the unexpected change outside the prior region were simultaneously reconstructed. To achieve this, five (1 + 1 + 3) iterations instead of three were required.
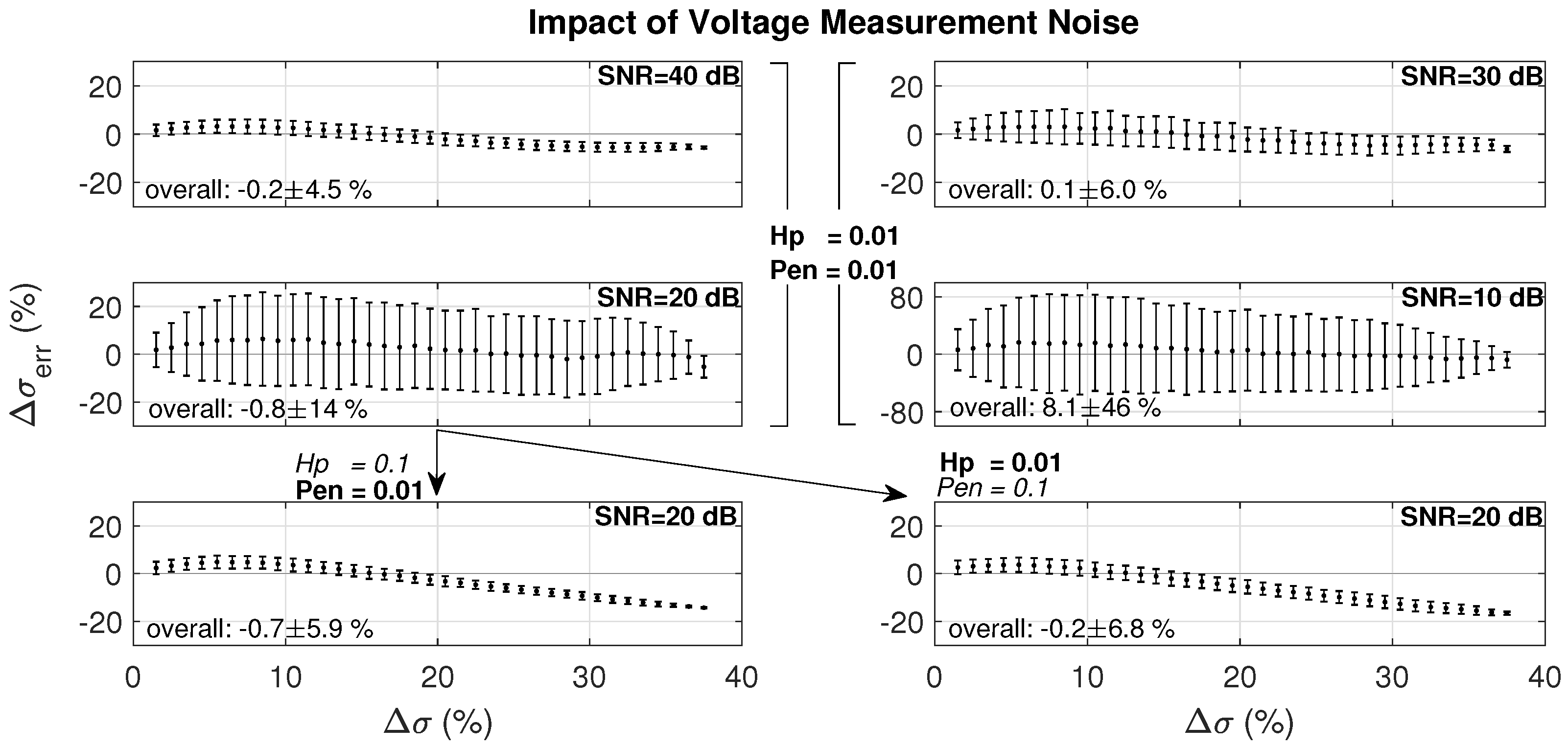
2.3.4. Voltage Measurement Noise
The reconstruction problem is ill-conditioned. Minor voltage differences in the electrode measurements can lead to large changes in estimated conductivity. As a result, electrode voltage measurement noise is expected to significantly corrupt the reconstruction quality. Here, we investigated its impact on the conductivity reconstruction in the Duke anatomical model with a large number of mesh elements. Specifically, we assessed the impact of the noise level by adding noise with different SNR levels in setup P1. A noisy voltage vector (
) was generated by adding noise to the electrode voltages (
v) from the forward problem solution of the modified model (
).
where
n is zero mean white Gaussian noise with standard deviation
. The SNR is calculated as follows:
where
.
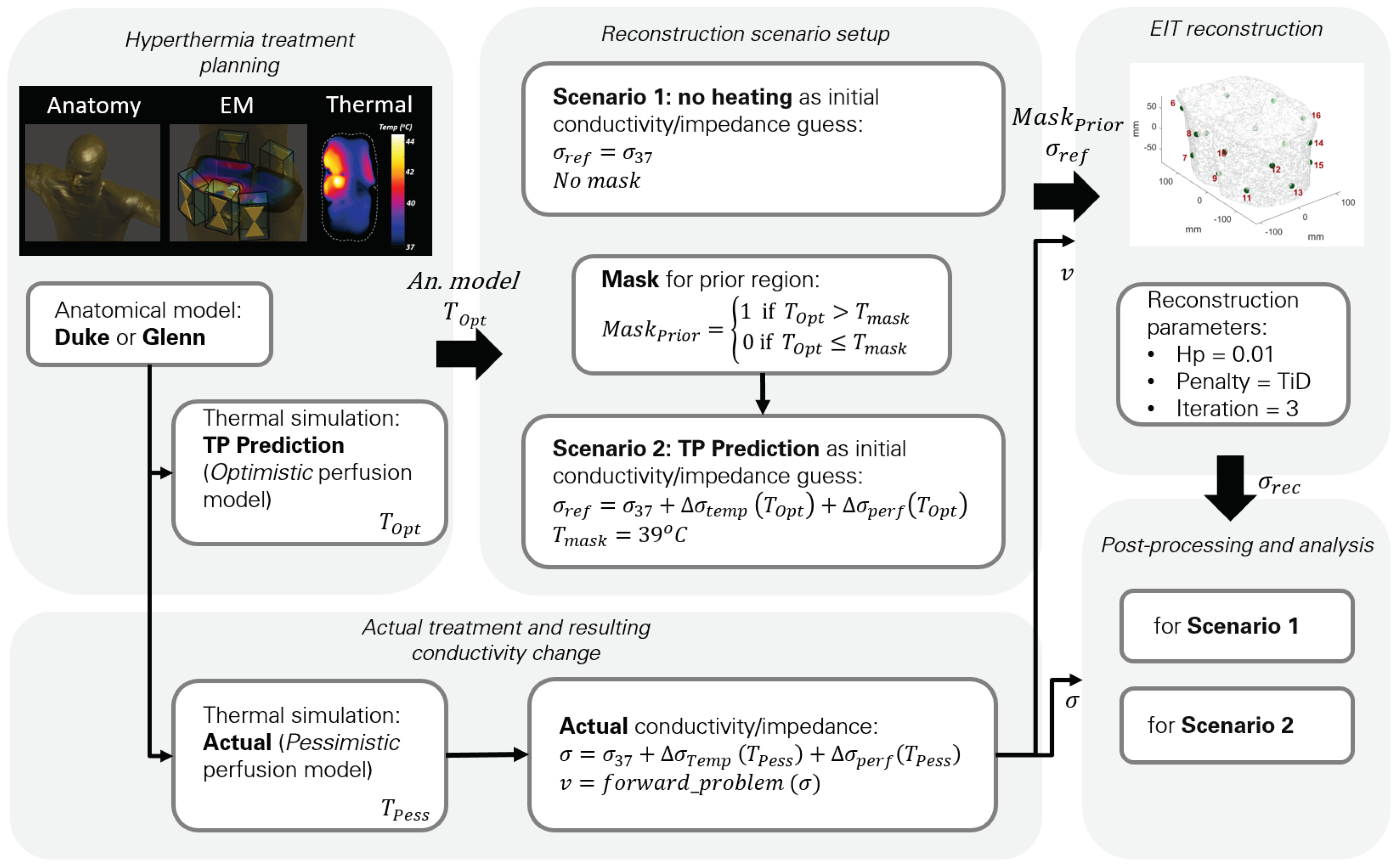
2.4. Simulated HT Treatment Reconstruction
In this part of the study, we used a setup that mimicked the targeting of a bladder tumor using locoregional HT, where heat was delivered to a larger region encompassing the tumor (see
Figure 3). This scenario provides increased realism and avoids the simplifying symmetries of the previous sections.
The procedure for the simulation was as follows:
We performed two thermal simulations of a one-hour treatment (
and
) using the same specific absorption rate (SAR) distribution. The Pennes bioheat equation (PBE) [
41] with temperature-dependent perfusion models was used for the thermal simulations (see Equation (
8)). The applied power level was the same in both cases, but the temperature-dependent perfusion models for muscle, fat, and tumor tissues were different (see
Figure 4), to illustrate the impact of perfusion uncertainty;
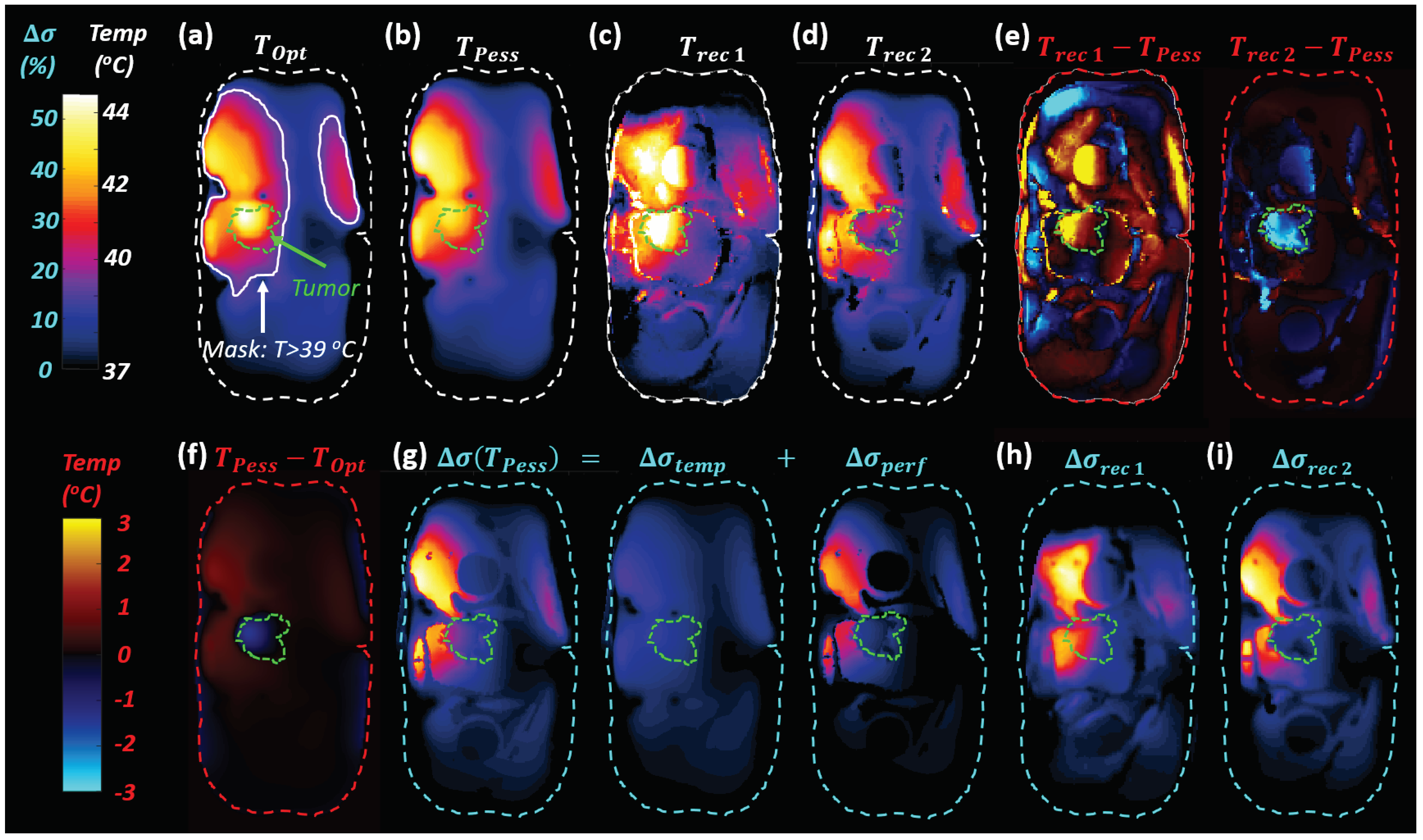
We translated the temperature increase to a modified conductivity map, which included a component directly related to temperature () and a perfusion-related indirect component ();
We reconstructed and analyzed the changes in conductivity based on the “ground truth” temperature simulation (), using the conductivity at 37 °C as the reference model (Scenario 1) or the conductivity for the “planned” (Scenario 2). The reconstructed conductivity was then converted into a reconstructed temperature estimation map.
The procedure is illustrated in
Figure 5.
The PBE couples thermal diffusion with a heat-sink term that is proportional to the local perfusion and to the difference between the local tissue temperature (
) at time
t and the arterial blood temperature (
):
where
represents density (kg/m
3),
c is the specific heat capacity (J/kg°C),
k is the thermal conductivity (J/(s·m·°C)),
is the perfusion rate (kg/(s·m
3)),
is the density of blood,
is the specific heat capacity of blood,
is the metabolic heat generation rate (J/(s·m
3)), and
is the electromagnetic power deposition.
can be temperature dependent to account for vasodilation.
2.4.1. Change in Conductivity Due to Temperature Increase
The change in conductivity during a HT treatment can be modeled with two components:
where the change in conductivity directly due to the increase in temperature (
) is
, with the temperature coefficient
(we assume
= 2%/°C in all tissues).
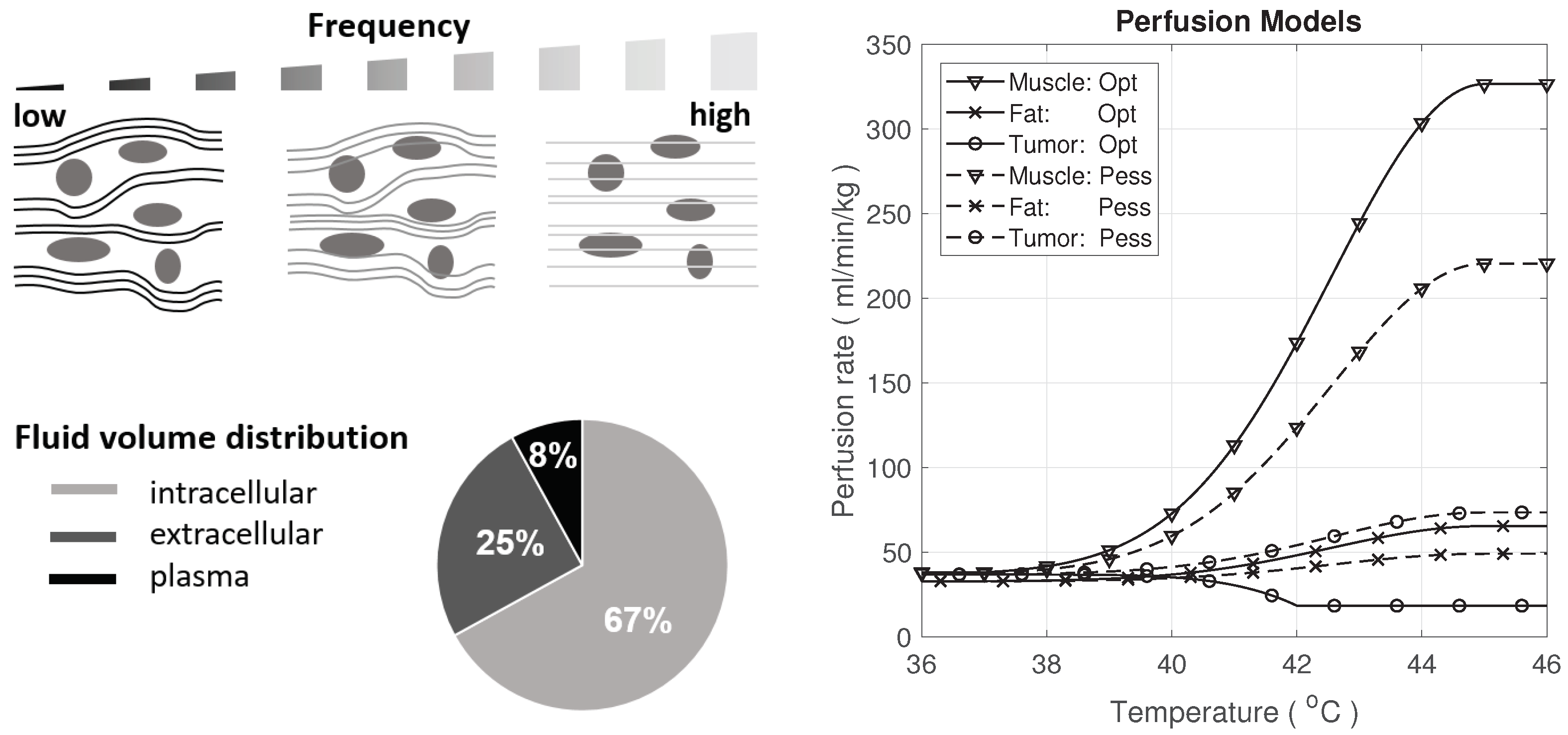
The conductivity change due to perfusion depends on the tissue as well as the frequency. At lower frequencies (kHz, LF), current flows mainly in the extracellular compartment, whereas at higher frequencies (MHz, HF), current flow tends to be more uniform across all tissue (see
Figure 4).
For the purpose of this study, a simple model representing the difference between high and low frequency EIT and perfusion effects was constructed. Large uncertainties were associated with the temperature dependence of the perfusion
. However, as long as the model reproduced the general magnitude and behavior in terms of perfusion impact on conductivity and heating, it did not affect the generality of the study conclusions. To model the different frequencies, we neglected other dispersive effects and assumed that:
and
where
and
are the LF and HF conductance, respectively.
,
,
, correspond to intracellular, extracellular (without the blood plasma), and plasma conductance. We used the average human body volume ratio of these compartments from [
42], as illustrated in
Figure 4, as the conductance ratio between compartments to model the perfusion impact on conductance. Actual values are tissue-dependent.
The change in perfusion affects the total conductance by changing the relative contributions of the three compartments; therefore, the plasma volume increases as the perfusion increases. Assuming that the relative tissue volume change related to a perfusion increase is small and the plasma conductivity is the principal contributor to the overall conductivity, we obtain:
where
is the plasma volume change due to perfusion, and
is the relative perfusion change.
is the relative amount of plasma prior to heating, which is taken uniformly as 8% (see
Figure 4), while in reality it varies across tissues and individuals. The
accounts for the plasma volume prior to heating, which is already included in the
term. The square root approximates the relationship between blood vessel cross-sectional area and perfusion increase and is obtained under the assumption of a constant pressure drive and laminar flow [
44].
Perfusion-related changes were considered for muscle, fat, and tumor tissues, particularly for prominent tissues with strong temperature dependence of perfusion and an important impact on the predicted temperature, using the two perfusion models shown in
Figure 4, according to [
14]. Tumor perfusion has a high associated uncertainty [
14] due to irregular vascularization.
Disentangling Temperature and Perfusion
Distinguishing from to identify temperature and perfusion changes is not the subject of this paper. However, a possible approach is provided here:
, where
and
. If
is known at two frequencies for a tissue of interest (in this study, we assumed
= 24% and
= 8% for all tissues), we obtain
and
The former can be used to estimate
, while the latter can be used to obtain
(either using the
estimated using Equation (
13), or
from the simulation, or neglecting the term
in Equation (
14)). In practice,
and
might not be known, as the exact form of the temperature and perfusion dependences likely deviates from Equation (
12), and the reconstructed
and
contain reconstruction errors. For a brief analysis of the latter, see
Section 3.3.2.
2.4.2. Reconstruction Scenarios
Temperature predictions have uncertainties; hence, the need for online monitoring of temperature during treatment. Here, we assumed that a temperature distribution (
) corresponds to the actual thermal treatment administered to a patient with a bladder tumor. Using the equations and assumptions above, we calculated the actual conductivity change corresponding to
and the corresponding EIT voltages were used for reconstruction. Two scenarios were considered: one without previous knowledge and one with an imperfect thermal simulation-based treatment plan. In Scenario 1 (see
Figure 5), we reconstructed conductivity changes using the values at 37 °C (no heating applied) as the reference conductivity. In Scenario 2, temperature distributions from simulations using
were used to define the prior region for reconstruction; the incorrect perfusion information was used to introduce uncertainty similar to expected outcomes in a real treatment. Despite not using accurate perfusion values, Scenario 2 provided a better starting point than Scenario 1 for the reconstruction, as the conductivity difference to be reconstructed is smaller.
In both scenarios, we determined the prior region by thresholding at a temperature above a temperature threshold (). For Scenario 2, a of 39 °C was used, whereas for Scenario 1, no mask is applied. In Scenario 1, we expected changes in the whole volume, whereas in Scenario 2, the prior region was smaller, as differences were more localized. Suitable temperature thresholds were identified by studying the resulting reconstruction accuracy in a range of setups. Higher thresholds prevent the reconstruction outside the masked volume, resulting in an overall increased error, while lower thresholds lead to underestimation of tumor heating, as the impedance changes are attributed to a larger region.
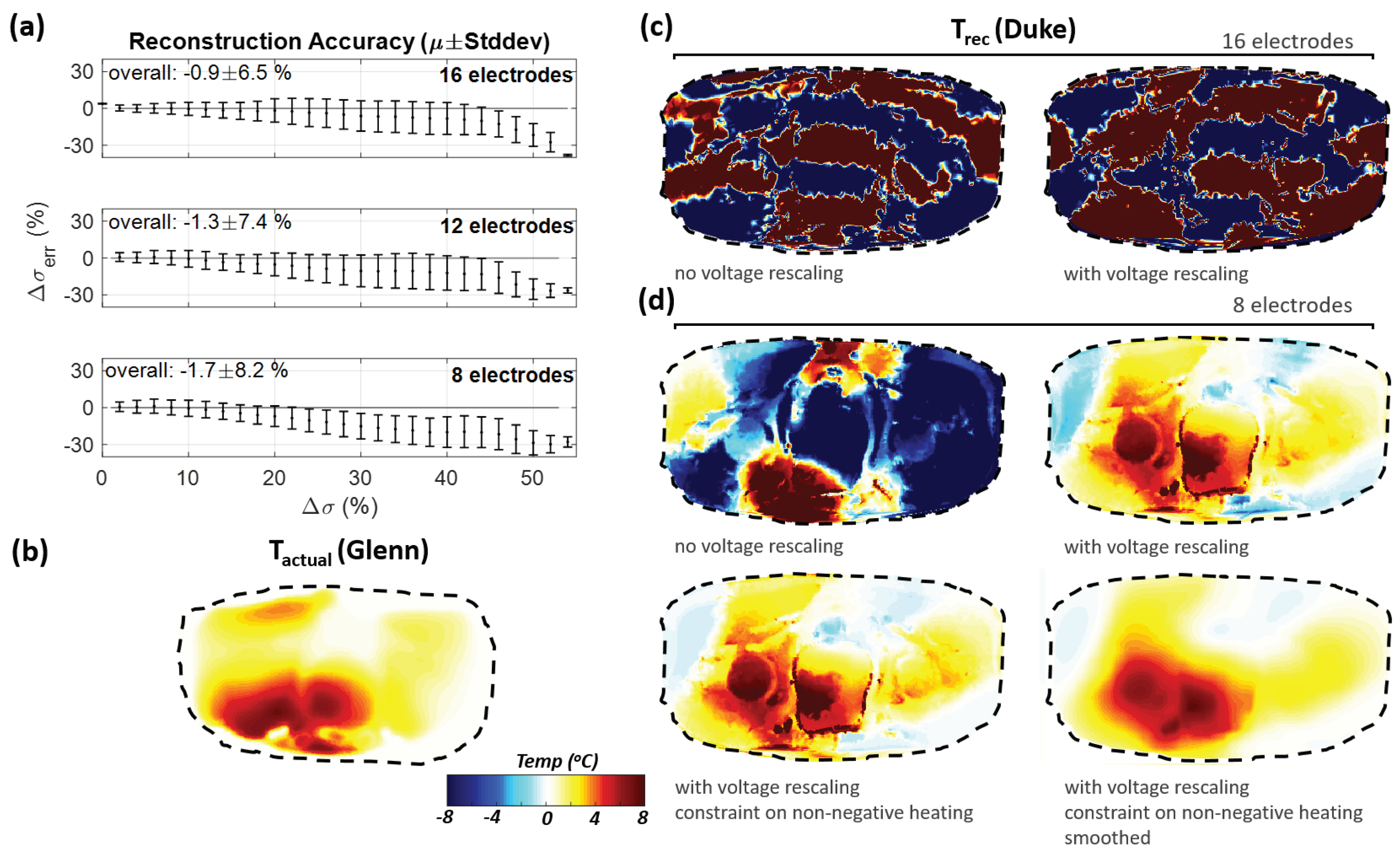
To investigate the importance of using personalized reference models, reconstruction was performed again using the Duke reference model, but with a simulated HT treatment measurement of Glenn (similar element placement, same steering parameters). As reconstruction with 16 elements was unsuccessful (see
Section 3.3.1), eight-element reconstruction was investigated further. Subsequently, changes in anatomy (Glenn has a smaller cross-section area than Duke) were compensated by rescaling the voltages with the ratio of the voltages prior to heating. The additional constraint of demanding a positive temperature increase was imposed by zeroing all negative conductivity changes prior to each reconstruction iteration (note: negative conductivity changes cannot be excluded completely, e.g., due to geometry changes during treatment or perfusion redistribution; performing the reconstruction step after zeroing does allow to account for some of that). Finally, the expected temperature distribution smoothness was mimicked by convolution with a Gaussian filter (radius: 1 cm; chosen based on the characteristic lengths of the PBE Green’s function in muscle, bone, fat, and tumor at the initial temperature).
For the analysis of the reconstruction accuracy, the conductivity change in the heated reference model was compared with the conductivity change in the reconstruction.
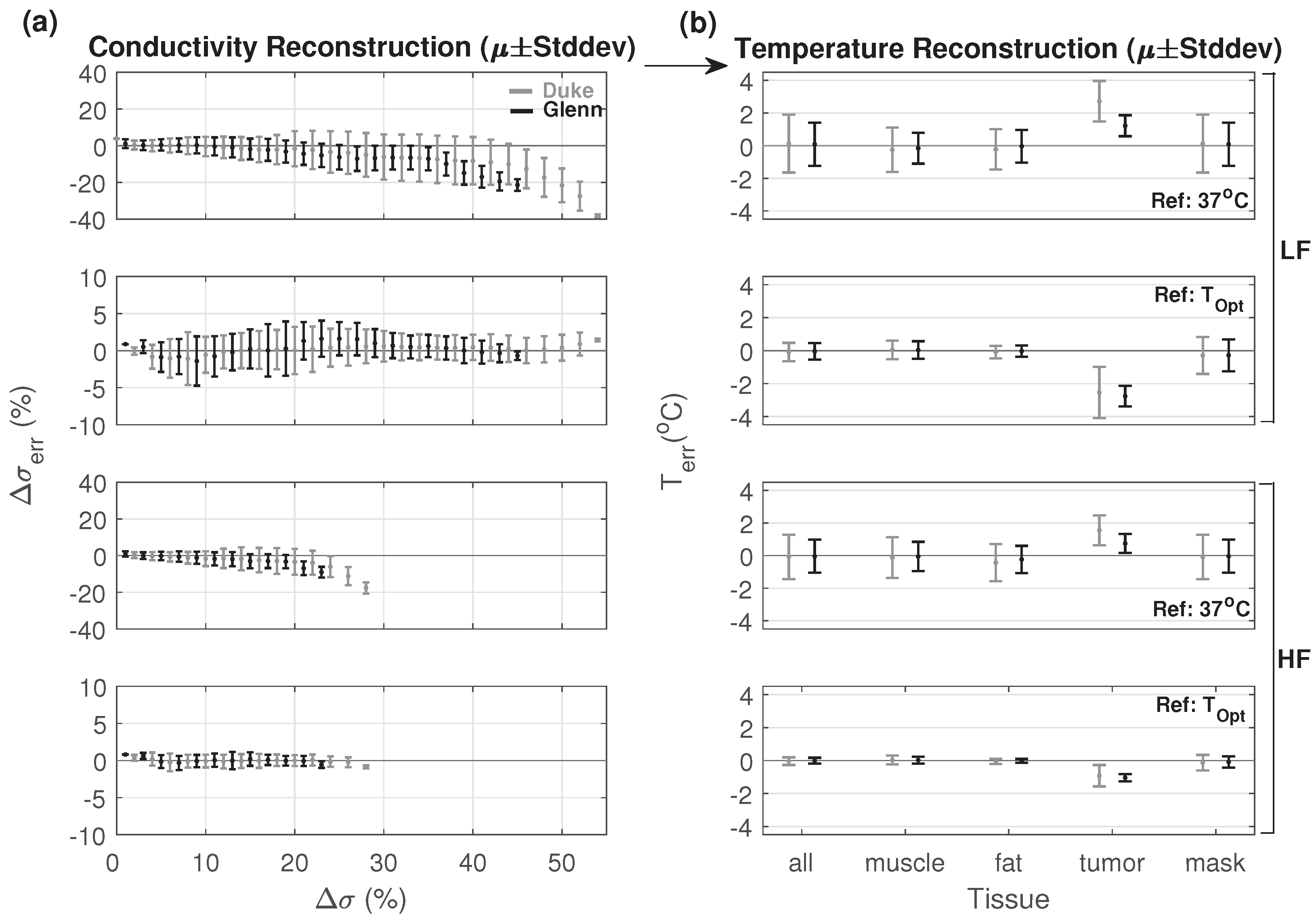
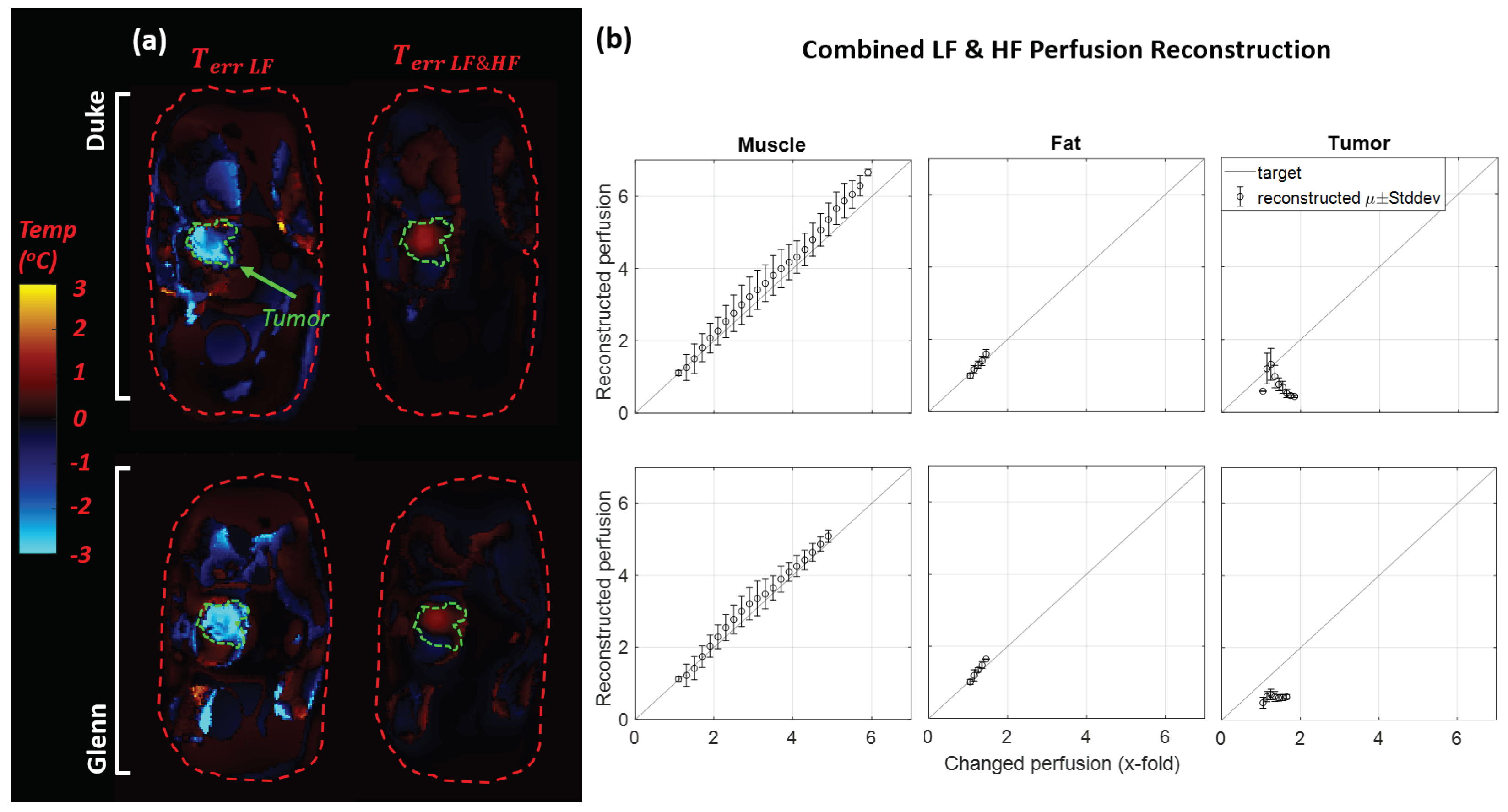
Both the LF and the HF EIT cases were simulated. In the LF case, the contribution of perfusion to the conductivity change is higher. Thus, the same temperature distribution resulted in a higher total change in conductivity. Ultimately, EIT at multiple frequencies was used to distinguish conductivity changes related to from indirect conductivity changes related to perfusion changes and to monitor both the temperature and the perfusion distribution. In this study, we focused on the feasibility of conductivity reconstruction, and only briefly considered multifrequency EIT-enabled contribution separation.
4. Discussion
In this study, we investigated the potential application of EIT as a low-cost, noninvasive technique for HT treatment monitoring.
For estimation accuracy, if only changes in conductivity associated with are considered, a 2% deviation from the actual conductivity leads to 1 °C error in temperature. Due to the presence of perfusion-related conductivity changes, the total conductivity sensitivity to temperature is higher, which can facilitate temperature mapping, if accurate information about the temperature dependence of perfusion is provided. However, the relation between the conductivity error and the temperature or perfusion estimation error becomes more complex. In the absence of well-known temperature–perfusion relationships, distinguishing between perfusion and temperature changes using multifrequency EIT is crucial. To simultaneously map perfusion and temperature changes, the use of more than two measurement frequencies and postprocessing techniques should be further investigated, considering the limited accuracy of conductivity map reconstruction and the limited knowledge about .
Using a tissue-dependent penalty along with adaptive prior regions are key to achieving conductivity mapping in highly heterogeneous anatomical models. Information from thermal simulations can be used to further improve the accuracy, as shown in the simulated HT treatment scenario. Under ideal conditions, reconstruction in a simulated HT treatment achieves a mean deviation in the order of 1 °C (see
Figure 11) in the heated domain. Having a good reference model is important, and a priori personalized models should be used. When using a nonspecific anatomical reference, fewer measurement electrodes should be used and voltages should be rescaled based on preheating measurements. An extreme scenario was investigated to assess local reference model inaccuracies (e.g., passing air bubble). Regarding local reference model inaccuracies (e.g., passing air bubble), an extreme scenario was investigated. We found that using adaptive prior regions in combination with a tissue-dependent penalty successfully enabled reconstruction. Nonablative HT is a relatively long treatment (∼40–60 min) and the heating time constant is in the order of minutes. Therefore, changes during treatment, except for body movements, occur slowly compared with the potential voltage acquisition speed. Continuous monitoring can be combined with continuous prior region adaptation to handle slow tissue environment changes and to adapt the reference model.
Measurement noise is problematic as the number of cells in the model to be reconstructed is large compared to the number of voltage measurements.
Figure 9 illustrates the quantifiable impact of SNR on the reconstruction error from 40 dB to 10 dB SNR, while keeping the same reconstruction parameters results in an increase of the reconstruction error by an order of magnitude. The SNR can be improved by averaging multiple acquisitions, and voltage measurements with poor SNR should be detected.
The combination of HT treatment planning with EIT has multiple advantages: Treatment planning typically includes imaging and segmentation for personalized treatment optimization, and a personalized reference model is important for the reconstruction. Electromagnetic and thermal simulations from HT planning can be used in EIT to determine the region where changes in conductivity are expected and which can serve as a prior region. A good reference model for the heated state also facilitates reconstruction (smaller ). In turn, EIT-reconstructed changes in conductivity converted to perfusion/temperature changes can be used for an online adaptation of the treatment plan and of the applied parameters.
For the simulated HT scenarios with the Duke and Glenn ViP models, additional investigations were performed that are not presented in this paper due to space constraints. The following parameters were varied: masking threshold level (37–40 °C), hyperparameter value (0.0001–1), and the number of electrodes (8–32) and electrode rows (2–4). The masking threshold affects the reconstruction of regions with relatively high changes that are left outside the mask, if too high, or the accuracy of high temperature region reconstruction, if too low. The impact of the hyperparameter is dependent on the masking threshold and the mask and penalty values; however, in most of the cases, 0.01 was considered a good choice. Increasing both the number of rows and electrodes did not yield significant improvements compared to two rows with 16 electrodes and resulted in smaller voltage differences between nearby electrodes, making the system more susceptible to noise and measurement uncertainty in practical implementations.
Table 4 lists study limitations that should be considered.
5. Conclusions
In this study, we investigated the feasibility of EIT difference imaging for detecting conductivity changes during HT therapy. Realistic scenarios were considered for the practical implementation of EIT in HT monitoring. We implemented an iterative reconstruction in which the reference model was updated for each iteration. The results suggest that a single iteration may be sufficient if there are only small changes.
By using highly heterogeneous anatomical models, we showed that a tissue-dependent penalty parameter improves reconstruction accuracy throughout the modeled volume. We also showed that reconstruction performance has no apparent dependence on the location and extent of the heated region when placing heated spheres with sizes typical of HT heating volumes in relevant torso treatment locations.
Simulated HT treatment with realistic heating patterns revealed large errors in the reconstruction, mainly due to conductivity changes within most of the volume. Using simulated treatment plans as references yields better reconstructions, despite modeling-inherent inaccuracies (e.g., of the tissue parameters). A personalized reference model is thus required; however, a nonspecific reference model can be used if the number of electrodes is reduced and a rescaling of voltages based on preheating measurements is performed.
In view of real-world limitations, we considered the impact of voltage measurement noise and strong localized inaccuracies in the reference model (large air bubble). Both can lead to significant errors, if reconstruction parameters for ideal conditions (no noise, accurate reference model) are used. However, important improvements can be achieved by relaxing reconstruction parameters and introducing prior region adaptation in the reconstruction.
For the successful application of EIT to monitor temperature and perfusion during HT therapy, all factors contributing to the deterioration of the accuracy must be addressed and mitigated. Essentially, accurate reference models (geometry and conductivity) and accurate impedance measurements are required. The results indicate that a temperature estimation accuracy in the order of 1 °C is achievable under the considered conditions and assumptions based on the novel methodologies in this study (iterative reconstruction with adaptive prior regions, planning-based references, measurement-based reweighting, tissue-dependent penalties, and positive heating constraints). The achievable mapping accuracy will depend on how well multifrequency EIT measurements can be leveraged to distinguish direct temperature-related impedance changes from changes caused by perfusion adaptation.
As a next step, experimental realization and validation of the presented approach is required. Initial work could focus on the reconstruction of heating distributions when applying HT ex vivo, where perfusion changes are irrelevant and measurement access is better. Subsequent work would then shift to in vivo situations and rely on strategically placed thermometry catheters, or information from MR thermometry and MR perfusion mapping. Compatibility issues associated with the presence of EIT electrodes during HT application must be considered.


 ,
, 















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}