Evaluation of Second-Line Anti-VEGF after First-Line Anti-EGFR Based Therapy in RAS Wild-Type Metastatic Colorectal Cancer: The Multicenter “SLAVE” Study

 , , , , , , , , ,
, , , , , , , , ,  , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Eligibility
2.2. Study Design
2.3. Molecular Profile Assessment
2.4. Statistical Analysis
3. Results
3.1. Patients Characteristics
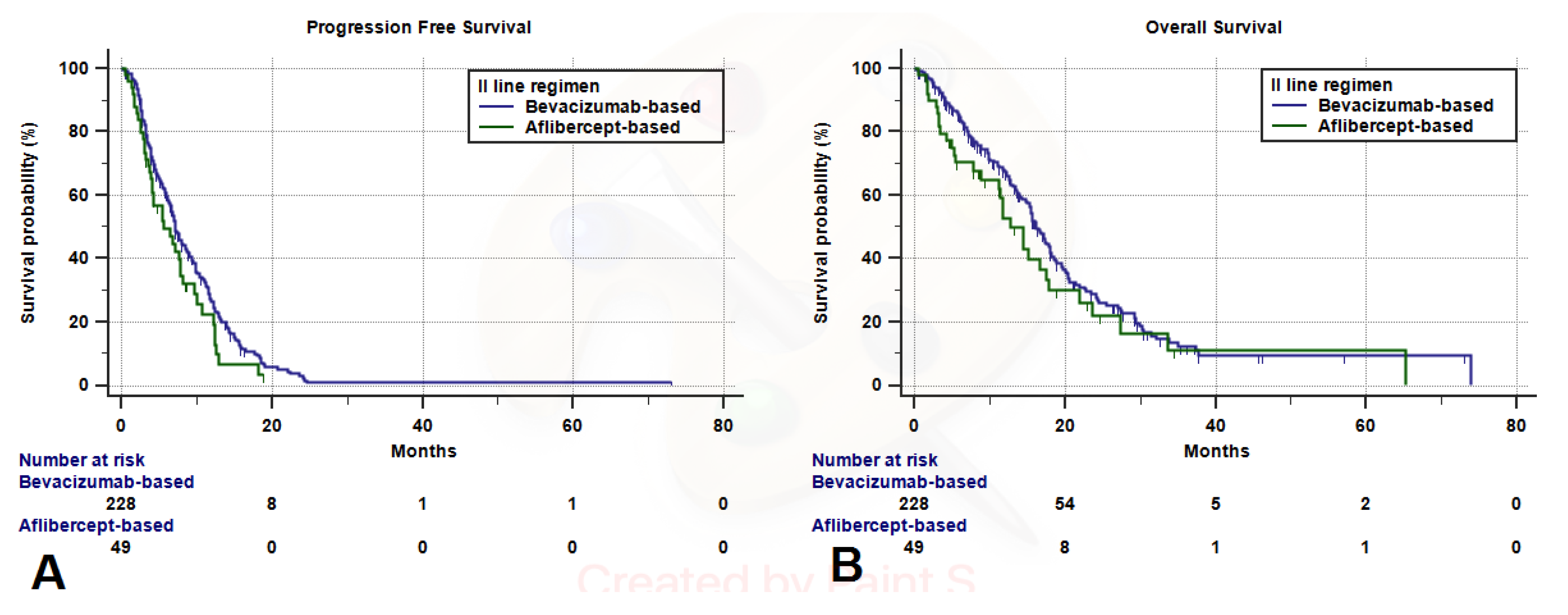
3.2. Clinical Outcomes Analysis
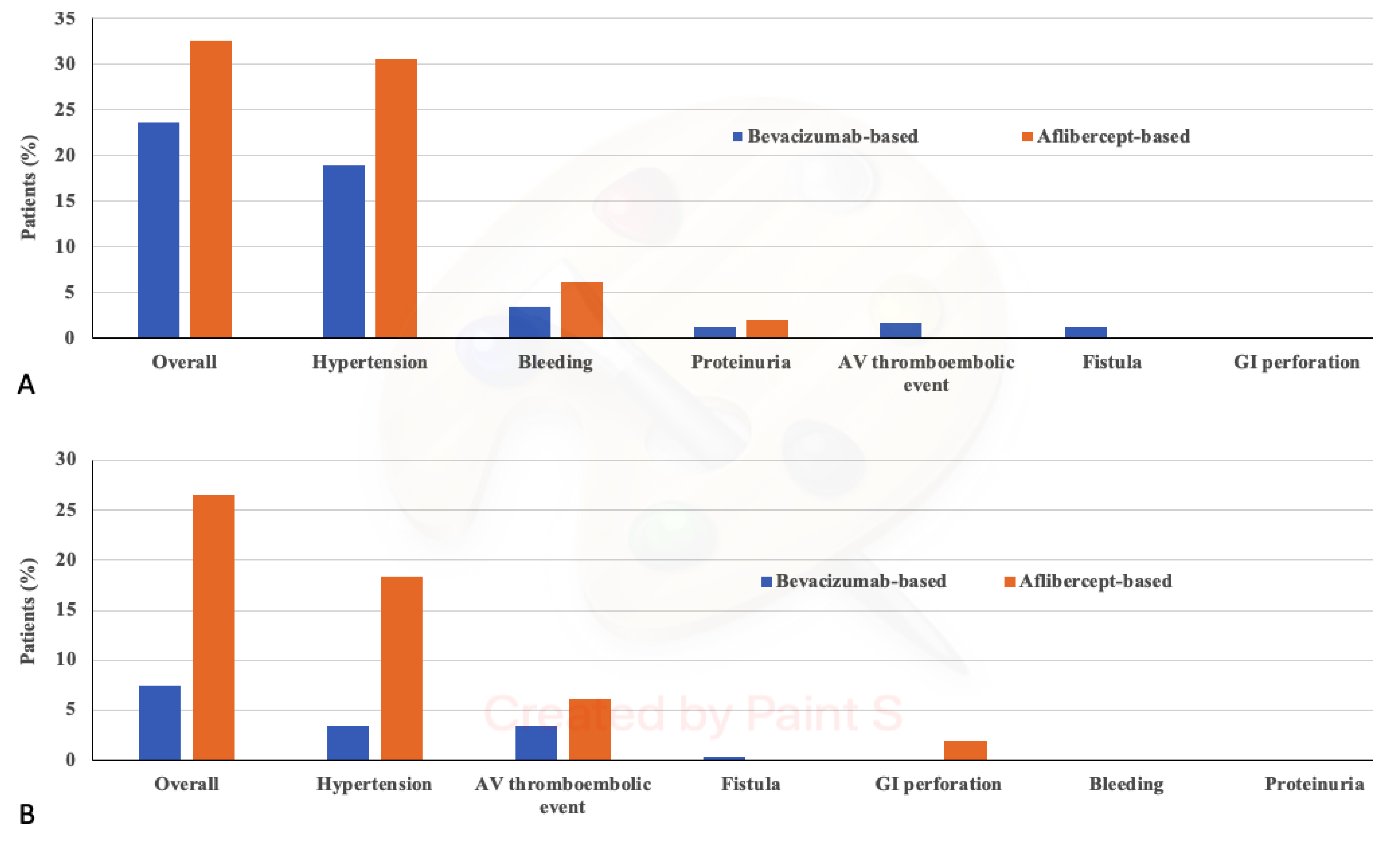
3.3. Toxicity Analysis
3.4. Maintenance Regimens and Post-Progression Treatments
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cremolini, C.; Schirripa, M.; Antoniotti, C.; Moretto, R.; Salvatore, L.; Masi, G.; Falcone, A.; Loupakis, F. First-line chemotherapy for mCRC—A review and evidence-based algorithm. Nat. Rev. Clin. Oncol. 2015, 12, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Cannita, K.; Parisi, A.; Baldi, P.L.; Venditti, O.; D’Orazio, C.; Dal Mas, A.; Calvisi, G.; Giordano, A.V.; Vicentini, V.; et al. Weekly alternate intensive regimen FIrB/FOx in metastatic colorectal cancer patients: An update from clinical practice. Onco Targets Ther. 2019, 12, 2159–2170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modest, D.P.; Pant, S.; Sartore-Bianchi, A. Treatment sequencing in metastatic colorectal cancer. Eur. J. Cancer 2019, 109, 70–83. [Google Scholar] [CrossRef]
- Temraz, S.; Mukherji, D.; Shamseddine, A. Sequencing of treatment in metastatic colorectal cancer: Where to fit the target. World J. Gastroenterol. 2014, 20, 1993. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012, 487, 330. [CrossRef] [Green Version]
- Amado, R.G.; Wolf, M.; Peeters, M.; van Cutsem, E.; Siena, S.; Freeman, D.J.; Juan, T.; Sikorski, R.; Suggs, S.; Radinsky, R.; et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 1626–1634. [Google Scholar] [CrossRef]
- Karapetis, C.S.; Khambata-Ford, S.; Jonker, D.J.; O’Callaghan, C.J.; Tu, D.; Tebbutt, N.C.; Simes, R.J.; Chalchal, H.; Shapiro, J.D.; Robitaille, S.; et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N. Engl. J. Med. 2008, 359, 1757–1765. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, V.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; Seipelt, G.; et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): A randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1065–1075. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Oliner, K.S.; Siena, S.; Tabernero, J.; Burkes, R.; Barugel, M.; Humblet, Y.; Bodoky, G.; Cunningham, D.; Jassem, J.; et al. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N. Engl. J. Med. 2013, 369, 1023–1034. [Google Scholar] [CrossRef] [Green Version]
- Martinelli, E.; Ciardiello, D.; Martini, G.; Troiani, T.; Cardone, C.; Vitiello, P.P.; Normanno, N.; Rachiglio, A.M.; Maiello, E.; Latiano, T.; et al. Implementing anti-epidermal growth factor receptor (EGFR) therapy in metastatic colorectal cancer: Challenges and future perspectives. Ann. Oncol. 2020, 31, 30–40. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Giantonio, B.J.; Catalano, P.J.; Meropol, N.J.; O’Dwyer, P.J.; Mitchell, E.P.; Alberts, S.R.; Schwartz, M.A.; Benson, A.B., III. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: Results from the Eastern Cooperative Oncology Group Study E3200. J. Clin. Oncol. 2007, 25, 1539–1544. [Google Scholar] [CrossRef]
- Bennouna, J.; Sastre, J.; Arnold, D.; Österlund, P.; Greil, R.; Van Cutsem, E.; von Moos, R.; Viéitez, J.M.; Bouché, O.; Borg, C.; et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): A randomized phase 3 trial. Lancet Oncol. 2013, 14, 29–37. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Tabernero, J.; Lakomy, R.; Prenen, H.; Prausová, J.; Macarulla, T.; Ruff, P.; van Hazel, G.A.; Moiseyenko, V.; Ferry, D.; et al. Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J. Clin. Oncol. 2012, 30, 3499–3506. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Pazdur, R. Endpoints for assessing drug activity in clinical trials. Oncologist 2008, 13 (Suppl. 2), 19–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woolley, K.K. How Variables Uncorrelated with the Dependent Variable Can Actually Make Excellent Predictors: The Important Suppressor Variable Case. Southwest Educational Research Association Annual Meeting Proceedings. 1997. Available online: https://eric.ed.gov/?id=ED407420 (accessed on 29 March 2020).
- Thompson, F.T.; Levine, D.U. Examples of Easily Explainable Suppressor Variables in Multiple Regression Research. Mult. Linear Regres. Viewp. 1997, 24, 11–13. [Google Scholar]
- Stopping Stepwise: Why Stepwise Selection Is Bad and What you Should Use Instead. Available online: https://towardsdatascience.com/stopping-stepwise-why-stepwise-selection-is-bad-and-what-you-should-use-instead-90818b3f52df (accessed on 29 March 2020).
- Köhne, C.H.; Grothey, A.; Bokemeyer, C.; Bontke, N.; Aapro, M. Chemotherapy in elderly patients with colorectal cancer. Ann Oncol. 2001, 12, 435–442. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, G.; He, J.; Ren, S.; Wu, F.; Zhang, J.; Wang, F. Gender differences in colorectal cancer survival: A meta-analysis. Int. J. Cancer 2017, 141, 1942–1949. [Google Scholar] [CrossRef]
- Wang, J.; Li, S.; Liu, Y.; Zhang, C.; Li, H.; Lai, B. Metastatic patterns and survival outcomes in patients with stage IV colon cancer: A population-based analysis. Cancer Med. 2020, 9, 361–373. [Google Scholar] [CrossRef] [Green Version]
- Grassadonia, A.; Di Marino, P.; Ficorella, C.; Cortellini, A.; Cannita, K.; Parisi, A.; Gamucci, T.; Zoratto, F.; Vici, P.; Barba, M.; et al. Impact of primary tumor location in patients with RAS wild-type metastatic colon cancer treated with first-line chemotherapy plus anti-EGFR or anti-VEGF monoclonal antibodies: A retrospective multicenter study. J. Cancer 2019, 10, 5926–5934. [Google Scholar] [CrossRef] [PubMed]
- Bianco, R.; Rosa, R.; Damiano, V.; Daniele, G.; Gelardi, T.; Garofalo, S.; Tarallo, V.; De Falco, S.; Melisi, D.; Benelli, R.; et al. Vascular endothelial growth factor receptor-1 contributes to resistance to anti-epidermal growth factor receptor drugs in human cancer cells. Clin. Cancer Res. 2008, 14, 5069–5080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viloria-Petit, A.; Crombet, T.; Jothy, S.; Hicklin, D.; Bohlen, P.; Schlaeppi, J.M.; Rak, J.; Kerbel, R.S. Acquired resistance to the antitumor effect of epidermal growth factor receptorblocking antibodies in vivo: A role for altered tumor angiogenesis. Cancer Res. 2001, 61, 5090–6101. [Google Scholar] [PubMed]
- Angelucci, A.; Delle Monache, S.; Cortellini, A.; Di Padova, M.; Ficorella, C. “Vessels in the Storm”: Searching for prognostic and predictive angiogenic factors in colorectal cancer. Int. J. Mol. Sci. 2018, 19, 299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delle Monache, S.; Cortellini, A.; Parisi, A.; Pulcini, F.; Martellucci, S.; Mei, C.; Danubio, M.E.; Mattei, V.; Angelucci, A.; Ficorella, C. Expression of pro-angiogenic factors as potential biomarkers in experimental models of colon cancer. J. Cancer Res. Clin. Oncol. 2020. [Google Scholar] [CrossRef]
- Modest, D.P.; Stintzing, S.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; et al. Impact of subsequent therapies on outcome of the FIRE-3/AIO KRK0306 trial: First-line therapy with FOLFIRI plus cetuximab or bevacizumab in patients with KRAS wild-type tumors in metastatic colorectal cancer. J. Clin. Oncol. 2015, 33, 3718–3726. [Google Scholar] [CrossRef]
- Arnold, D.; Lueza, B.; Douillard, J.Y.; Peeters, M.; Lenz, H.J.; Venook, A.; Heinemann, V.; Van Cutsem, E.; Pignon, J.P.; Tabernero, J.; et al. Prognostic and predictive value of primary tumor side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef]
- Hasegawa, H.; Taniguchi, H.; Mitani, S.; Masuishi, T.; Komori, A.; Narita, Y.; Kadowaki, S.; Ura, T.; Ando, M.; Yatabe, Y.; et al. Efficacy of second-line bevacizumab-containing chemotherapy for patients with metastatic colorectal cancer following first-line treatment with an anti-epidermal growth factor receptor antibody. Oncology 2017, 92, 205–212. [Google Scholar] [CrossRef]
- Lam, K.O.; Lee, V.H.; Liu, R.K.; Leung, T.W.; Kwong, D.L. Bevacizumab-containing regimens after cetuximab failure in Kras wild-type metastatic colorectal carcinoma. Oncol. Lett. 2013, 5, 637–640. [Google Scholar] [CrossRef]
- Vera, R.; Mata, E.; González, E.; Juez, I.; Alonso, V.; Iranzo, P.; Martínez, N.P.; López, C.; Cabrera, J.M.; Safont, M.J.; et al. Is aflibercept an optimal treatment for wt RAS mCRC patients after progression to first line containing anti-EGFR? Int. J. Colorectal Dis. 2020, 35, 739–746. [Google Scholar] [CrossRef]
- Feo, L.; Polcino, M.; Nash, G.M. Resection of the Primary Tumor in Stage IV Colorectal Cancer: When Is It Necessary? Surg. Clin. N. Am. 2017, 97, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; Petrelli, F.; Coinu, A.; Di Bartolomeo, M.; Borgonovo, K.; Maggi, C.; Cabiddu, M.; Iacovelli, R.; Bossi, I.; Lonati, V.; et al. Predictive role of BRAF mutations in patients with advanced colorectal cancer receiving cetuximab and panitumumab: A meta-analysis. Eur. J. Cancer 2015, 51, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.; Kopetz, S.; Tie, J.; Gibbs, P.; Jiang, Z.Q.; Lieu, C.H.; Agarwal, A.; Maru, D.M.; Sieber, O.; Desai, J. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer 2011, 117, 4623–4632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubicka, S.; Greil, R.; André, T.; Bennouna, J.; Sastre, J.; Van Cutsem, E.; von Moos, R.; Osterlund, P.; Reyes-Rivera, I.; Müller, T.; et al. Bevacizumab plus chemotherapy continued beyond first progression in patients with metastatic colorectal cancer previously treated with bevacizumab plus chemotherapy: ML18147 study KRAS subgroup findings. Ann. Oncol. 2013, 24, 2342–2349. [Google Scholar] [CrossRef] [PubMed]
- Wirapati, P.; Pomella, V.; Vandenbosch, B.; Kerr, P.; Maiello, E.; Jeffery Grahame, M.; Curca, R.D.; Karthaus, M.; Bridgewater, J.A.; Mihailov, A.C.; et al. VELOUR trial biomarkers update: Impact of RAS, BRAF, and sidedness on aflibercept activity. Ann. Oncol. 2017, 28 (Suppl. 3), iii151–iii152. [Google Scholar] [CrossRef]
- Holash, J.; Davis, S.; Papadopoulos, N.; Croll, S.D.; Ho, L.; Russell, M.; Boland, P.; Leidich, R.; Hylton, D.; Burova, E.; et al. VEGF-Trap: A VEGF blocker with potent antitumor effects. Proc. Natl. Acad. Sci. USA 2002, 99, 11393–11398. [Google Scholar] [CrossRef] [Green Version]
- Tabernero, J.; Yoshino, T.; Cohn, A.L.; Obermannova, R.; Bodoky, G.; Garcia-Carbonero, R.; Ciuleanu, T.E.; Portnoy, D.C.; Van Cutsem, E.; Grothey, A.; et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): A randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 2015, 16, 499–508. [Google Scholar]
- Chibaudel, B.; Bonnetain, F.; Tournigand, C.; de Larauze, M.H.; de Gramont, A.; Laurent-Puig, P.; Paget, J.; Hadengue, A.; Notelet, D.; Benetkiewicz, M.; et al. STRATEGIC-1: A multiple-lines, randomized, open-label GERCOR phase III study in patients with unresectable wild-type RAS metastatic colorectal cancer. BMC Cancer 2015, 15, 496. [Google Scholar] [CrossRef]
- Ziranu, P.; Demurtas, L.; Puzzoni, M.; Loupakis, F.; Daniele, B.; Rimassa, L.; Bilancia, D.; Lonardi, S.; Avallone, A.; Pella, N.; et al. The DISTINCTIVE study: A biologically enriched phase II study of seconD-line folfiri/aflIbercept in proSpecTIvely stratified, anti-EGFR resistaNt, metastatic coloreCTal cancer patIents with RAS Validated wild typE status-Trial in progress. Ann. Oncol. 2018, 29 (Suppl. 5), mdy151–mdy290. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Overall N (%) | Bevacizumab-Based N (%) | Aflibercept-Based N (%) | |
|---|---|---|---|---|
| 277 (100) | 228 (82.3) | 49 (17.7) | p Value | |
| Age Median (years) Range (years) Elderly (≥70) | 64.5 29–84 90 (32.5) | 65.5 30–84 76 (33.3) | 63 29–81 14 (28.6) | 0.5192 |
| Sex Male Female | 168 (60.6) 109 (39.4) | 139 (61.0) 89 (39.0) | 29 (59.2) 20 (40.8) | 0.8172 |
| ECOG-PS 0 1 2 | 147 (53.1) 116 (41.9) 14 (5.0) | 118 (51.7) 100 (43.9) 10 (4.4) | 29 (59.2) 16 (32.6) 4 (8.2) | 0.6953 # |
| N° of metastatic sites 1 ≥2 | 93 (33.6) 184 (66.4) | 74 (32.5) 154 (67.5) | 19 (38.8) 30 (61.2) | 0.3963 |
| Sideness Right-side Left-side/Rectum | 71 (25.6) 206 (74.4) | 58 (25.4) 170 (74.6) | 13 (26.5) 36 (73.5) | 0.8740 |
| Primary tumor resection Yes No | 204 (73.6) 73 (26.4) | 180 (78.9) 48 (21.1) | 24 (49.0) 25 (51.0) | <0.0001 |
| BRAF Wild-type V600E mutated Not-V600E mutated NA | 249 (89.9) 3 (1.1) 1 (0.4) 24 (8.6) | 204 (89.5) 2 (0.9) 1 (0.4) 21 (9.2) | 45 (91.8) 1 (2.0) 0 (0.0) 3 (6.2) | 0.4027 # |
| MMR/MSI Proficient/wild-type Deficient/mutated NA | 96 (34.7) 5 (1.8) 176 (63.5) | 80 (35.1) 5 (2.2) 143 (62.7) | 16 (32.7) 0 (0) 33 (67.3) | 0.6361 # |
| I-line treatment FOLFIRI-Cetuximab FOLFOX-Cetuximab FOLFOX-Panitumumab FOLFIRI-Panitumumab mFOLFOXIRI-anti-EGFR 5-FU/Cape-anti-EGFR | 142 (51.3) 19 (6.8) 92 (33.2) 5 (1.8) 11 (4.0) 8 (2.9) | 140 (61.4) 15 (6.6) 51 (22.4) 5 (2.2) 9 (3.9) 8 (3.5) | 2 (4.1) 4 (8.1) 41 (83.7) 0 (0) 2 (4.1) 0 (0) | <0.0001 # |
| II-line chemotherapy backbone FOLFOX/XELOX FOLFIRI FOLFOXIRI 5-FU/Cape | 128 (46.2) 122 (44.1) 2 (0.7) 25 (9.0) | 128 (56.1) 73 (32.0) 2 (0.9) 25 (11.0) | 0 (0) 49 (100) 0 (0) 0 (0) | 0.0148 # |
| OBJECTIVE RESPONSE RATE | ||||||
|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||||
| Variable (Comparator) | Responses-Ratio | ORR (95% CI) | p-Value | Coeff. | St. Err. | p-Value |
| Overall | 68/264 | 25.8 (20.0–32.6) | - | - | - | - |
| II Line regimen Bevacizumab-based Aflibercept-based | 56/218 12/46 | 25.7 (19.4–33.3) 26.1 (13.4–45.6) | 0.9553 | 0.0126 | 0.3762 | 0.9733 |
| ECOG-PS 0 1 2 | 39/141 26/111 3/12 | 27.7 (19.7-37.8) 23.4 (15.3–34.3) 25.0 (5.1–73.1) | 0.7458 | –0.0996 | 0.2564 | 0.6976 |
| No. of metastatic sites 1 site ≥2 sites | 29/89 39/175 | 32.6 (21.8–46.8) 22.3 (15.8–30.5) | 0.0710 | –0.4905 | 0.3010 | 0.1032 |
| Sex Female Male | 30/103 38/161 | 29.1 (19.6–41.6) 23.6 (16.7–32.4) | 0.3177 | 0.2497 | 0.2899 | 0.3891 |
| Age Elderly Non-elderly | 24/86 44/178 | 27.9 (17.9–41.5) 24.7 (17.9–33.2) | 0.5798 | 0.0945 | 0.3219 | 0.7639 |
| Sideness Right-side Left-side | 23/66 45/198 | 34.8 (22.1–52.3) 22.7 (16.6–30.4) | 0.0516 | 0.5516 | 0.3219 | 0.0866 |
| PROGRESSION FREE SURVIVAL | ||
|---|---|---|
| Univariate Analysis | Multivariate Analysis | |
| VARIABLE | HR (95% CI); p-Value | HR (95% CI); p-Value |
| II Line regimen Aflibercept-based vs. Bevacizumab-based | 1.34 (0.95–1.89); p = 0.0932 | 1.44 (1.02–2.03); p = 0.0399 |
| ECOG-PS Continuous | 1.44 (1.15–1.82); p = 0.0013 | 1.36 (1.07–1.72); p = 0.0107 |
| No. of metastatic sites ≥2 sites vs. 1 site | 1.68 (1.27–2.21); p = 0.0002 | 1.56 (1.18–2.08); p = 0.0019 |
| Sex Female vs. Male | 0.92 (0.71–1.20); p = 0.5564 | 0.91 (0.70–1.19); p = 0.5184 |
| Age Non-elderly vs. Elderly | 0.99 (0.75–1.31); p = 0.9725 | 0.94 (0.70–1.26); p = 0.6950 |
| Sideness Right-side vs. Left-side | 0.79 (0.59–1.06); p = 0.1224 | 0.87 (0.64–1.18); p = 0.3785 |
| OVERALL SURVIVAL | ||
|---|---|---|
| Univariate Analysis | Multivariate Analysis | |
| VARIABLE | HR (95% CI); p-Value | HR (95% CI); p-Value |
| II Line regimen Aflibercept-based vs. Bevacizumab-based | 1.31 (0.89–1.93); p = 0.1600 | 1.47 (0.99–2.17); p = 0.0503 |
| ECOG-PS Continuous | 1.98 (1.53–2.57); p < 0.0001 | 1.81 (1.38–2.37); p < 0.0001 |
| No. of metastatic sites ≥ 2 sites vs. 1 site | 2.17 (1.56–3.03); p < 0.0001 | 1.90 (1.35–2.67); p = 0.0002 |
| Sex Female vs. Male | 0.72 (0.53–0.98); p = 0.0390 | 0.80 (0.59–1.09); p = 0.1727 |
| Age Non-elderly vs. Elderly | 1.10 (0.81–1.48); p = 0.5316 | 0.98 (0.72–1.35); p = 0.9411 |
| Sideness Right-side vs. Left-side | 0.94 (0.68–1.30); p = 0.7295 | 0.99 (0.71–1.38); p = 0.9582 |
| Overall N (277) | Bevacizumab-Based N (228) | Aflibercept-Based N (49) | ||||
|---|---|---|---|---|---|---|
| Adverse Events (AE) | G1–G2 N (%) | G3–G4 N (%) | G1–G2 N (%) | G3-G4 N (%) | G1–G2 N (%) | G3–G4 N (%) |
| VEGF inhibitors class-specific | 70 (25.3) | 29 (10.5) | 54 (23.7) | 17 (7.5) | 16 (32.7) | 13 (26.5) |
| Hypertension | 58 (82.9) | 17 (58.6) | 43 (79.6) | 8 (47.1) | 15 (93.8) | 9 (69.2) |
| AV thromboembolic event | 4 (5.7) | 11 (37.9) | 4 (7.4) | 8 (47.1) | 0 (0) | 3 (23.1) |
| Bleeding | 11 (15.7) | 0 (0) | 8 (14.8) | 0 (0) | 3 (18.8) | 0 (0) |
| Fistula | 3 (4.3) | 1 (3.4) | 3 (5.6) | 1 (5.9) | 0 (0) | 0 (0) |
| GI perforation | 0 (0) | 1 (3.4) | 0 (0) | 0 (0) | 0 (0) | 1 (7.7) |
| Proteinuria | 3 (4.3) | 1 (3.4) | 3 (5.6) | 0 (0) | 1 (6.3) | 0 (0) |
| Hematologic | 67 (29.4) | 16 (5.8) | 56 (24.6) | 7 (3.1) | 11 (22.4) | 9 (18.4) |
| Leukopenia | 8 (11.9) | 3 (18.7) | 7 (12.5) | 1 (14.3) | 1 (11.1) | 2 (20) |
| Neutropenia | 37 (55.2) | 13 (81.2) | 32 (57.1) | 5 (71.4) | 5 (55.6) | 8 (80) |
| Anemia | 47 (70.1) | 4 (25.0) | 40 (71.4) | 3 (42.9) | 7 (77.8) | 1 (10) |
| Thrombocytopenia | 29 (43.3) | 1 (6.2) | 21 (37.5) | 1 (14.3) | 8 (88.9) | 0 (0) |
| Non hematologic | 112 (40.4) | 14 (5.1) | 83 (36.4) | 10 (4.4) | 29 (59.2) | 4 (8.2) |
| Asthenia | 46 (41.1) | 3 (21.4) | 31 (37.3) | 2 (12.5) | 15 (50.0) | 1 (20) |
| Anorexia | 16 (14.3) | 0 (0) | 10 (12.0) | 0 (0) | 6 (20) | 0 (0) |
| Diarrhea | 60 (53.6) | 5 (35.7) | 40 (48.2) | 3 (25.0) | 20 (66.7) | 2 (40) |
| Nausea | 33 (29.5) | 2 (14.3) | 24 (28.9) | 2 (25.0) | 9 (30.0) | 0 (0) |
| Vomiting | 7 (6.2) | 1 (7.1) | 4 (4.8) | 1 (12.5) | 3 (10) | 0 (0) |
| Mucositis/stomatitis | 33 (29.5) | 2 (14.3) | 21 (25.3) | 1 (12.5) | 12 (40) | 1 (20) |
| HFS | 9 (8.0) | 1 (7.1) | 8 (9.6) | 1 (12.5) | 1 (3.3) | 0 (0) |
| Overall Population N (%) | Bevacizumab-Based N (%) | Aflibercept-Based N (%) | p-Value | |
|---|---|---|---|---|
| Characteristic | 277 (100) | 228 (82.3) | 49 (17.7) | |
| II-line maintenance treatment | 76 (27.4) | 67 (29.4) | 9 (18.4) | 0.2236 |
| 5-FU/Cape + antiangiogenic | 63 (22.7) | 56 (24.6) | 7 (14.3) | |
| Antiangiogenic alone | 10 (3.6) | 8 (3.5) | 2 (4.1) | |
| 5-FU/Cape alone | 3 (1.1) | 3 (1.3) | 0 (0) | |
| II-line discontinued | 236 (85.2) | 196 (86.0) | 40 (81.6) | 0.8425 |
| Cause of discontinuation | ||||
| Disease Progression | 193 (81.8) | 161 (82.1) | 32 (80.0) | |
| Toxicity | 25 (10.6) | 18 (9.2) | 7 (17.5) | |
| Patient rest/refusal | 10 (4.2) | 9 (4.6) | 1 (2.5) | |
| Palliative surgery or locoregional treatments | 8 (3.4) | 8 (4.1) | 0 (0) | |
| III-line treatment | 160 (67.8) ¥ | 136 (69.4) ¥ | 24 (60.0) ¥ | 0.5930 |
| Regorafenib | 57 (35.6) | 47 (34.6) | 10 (41.7) | |
| Trifluridine-tipiracil | 15 (9.4) | 12 (8.8) | 3 (12.5) | |
| Other (CT or Clinical Trial) | 48 (30.0) | 45 (33.1) | 3 (12.5) | |
| Anti-EGFR retreatment | 40 (25.0) | 32 (23.5) | 8 (33.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisi, A.; Cortellini, A.; Cannita, K.; Venditti, O.; Camarda, F.; Calegari, M.A.; Salvatore, L.; Tortora, G.; Rossini, D.; Germani, M.M.; et al. Evaluation of Second-Line Anti-VEGF after First-Line Anti-EGFR Based Therapy in RAS Wild-Type Metastatic Colorectal Cancer: The Multicenter “SLAVE” Study. Cancers 2020, 12, 1259. https://doi.org/10.3390/cancers12051259
Parisi A, Cortellini A, Cannita K, Venditti O, Camarda F, Calegari MA, Salvatore L, Tortora G, Rossini D, Germani MM, et al. Evaluation of Second-Line Anti-VEGF after First-Line Anti-EGFR Based Therapy in RAS Wild-Type Metastatic Colorectal Cancer: The Multicenter “SLAVE” Study. Cancers. 2020; 12(5):1259. https://doi.org/10.3390/cancers12051259
Chicago/Turabian StyleParisi, Alessandro, Alessio Cortellini, Katia Cannita, Olga Venditti, Floriana Camarda, Maria Alessandra Calegari, Lisa Salvatore, Giampaolo Tortora, Daniele Rossini, Marco Maria Germani, and et al. 2020. "Evaluation of Second-Line Anti-VEGF after First-Line Anti-EGFR Based Therapy in RAS Wild-Type Metastatic Colorectal Cancer: The Multicenter “SLAVE” Study" Cancers 12, no. 5: 1259. https://doi.org/10.3390/cancers12051259