Multimodal Assessment Shows a Mostly Preserved Cognitive Status in Incidentally Discovered Low Grade Gliomas: A Single Institution Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Neuropsychological Data
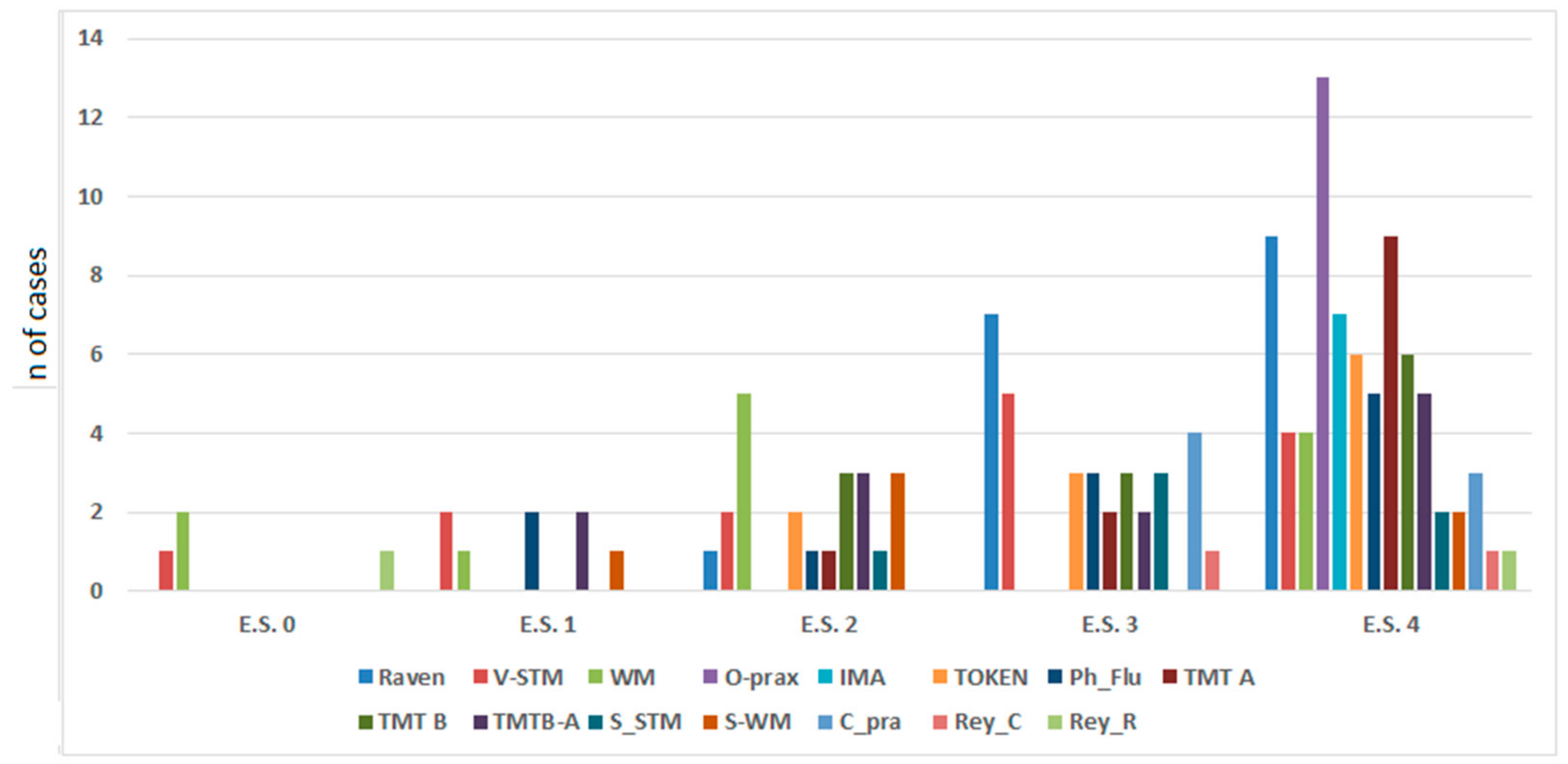
2.1.1. Below the Normal Range Performances
2.1.2. Borderline Performances
2.1.3. Correlation between Patients’ Equivalent Score and Molecular Class
2.2. MRI Structural Data
2.2.1. Preoperative Tumor Volume
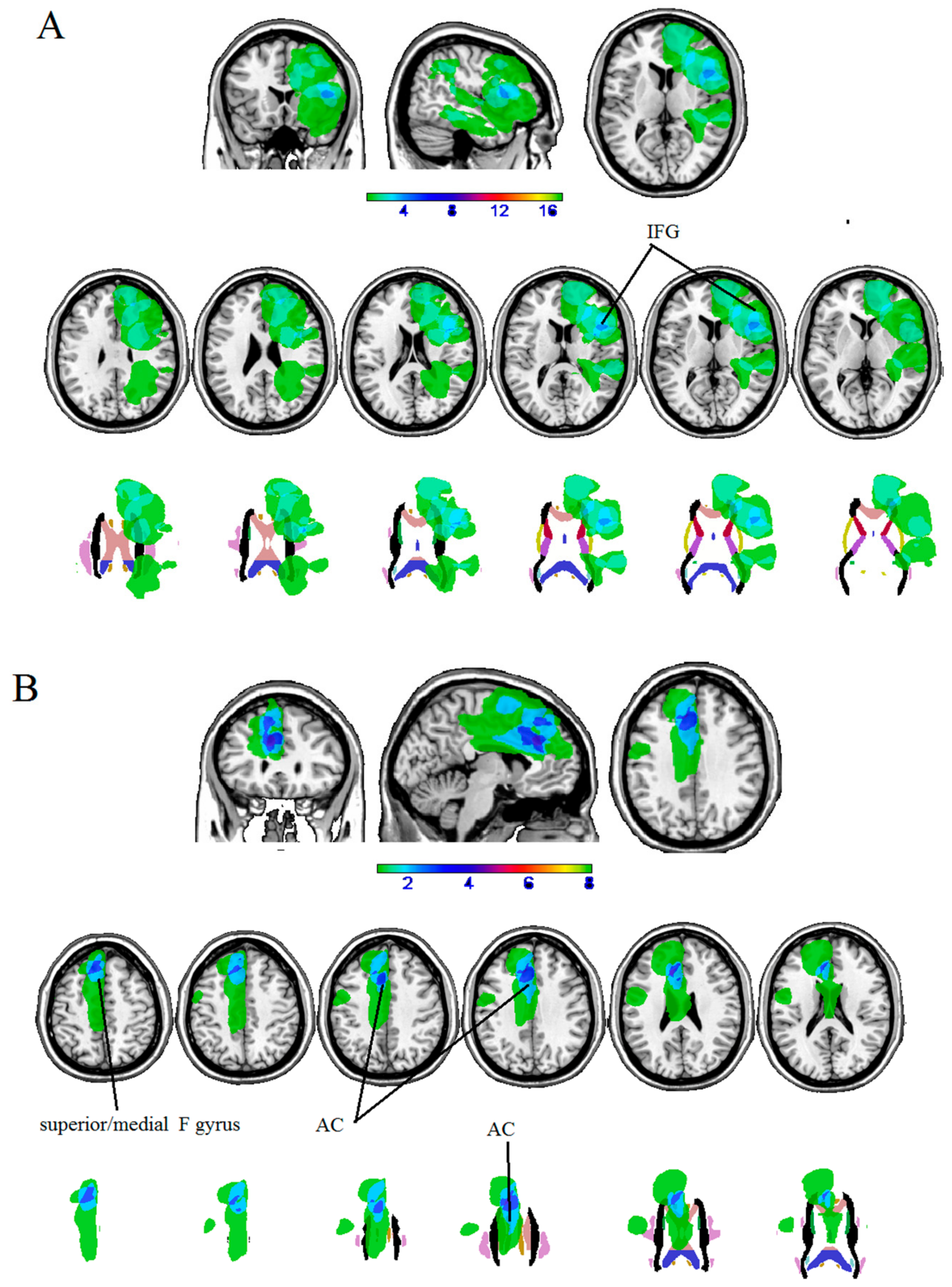
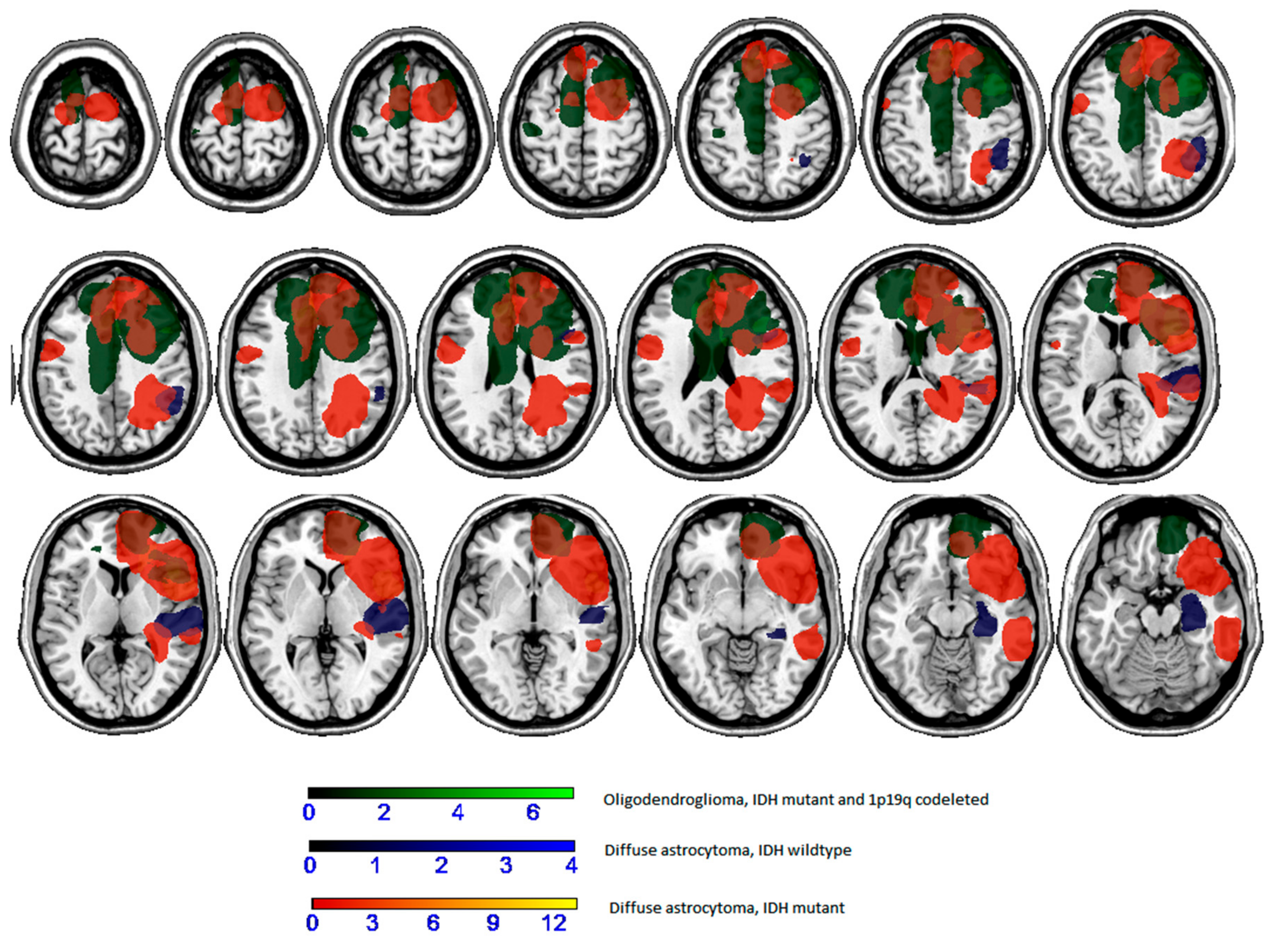
2.2.2. Maximum Lesion Overlap
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Neuropsychological Evaluation
4.3. MRI Structural Data
4.4. Histological and Molecular Analysis
4.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pallud, J.; Fontaine, D.; Duffau, H.; Mandonnet, E.; Sanai, N.; Taillandier, L.; Peruzzi, P.; Guillevin, R.; Bauchet, L.; Bernier, V.; et al. Natural history of incidental World Health Organization grade II gliomas. Ann. Neurol. 2010, 68, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Potts, M.B.; Smith, J.S.; Molinaro, A.M.; Berger, M.S. Natural history and surgical management of incidentally discovered low-grade gliomas. J. Neurosurg. 2012, 116, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Opoku-Darko, M.; Lang, S.T.; Artindale, J.; Cairncross, J.G.; Sevick, R.J.; Kelly, J.J.P. Surgical management of incidentally discovered diffusely infiltrating low-grade glioma. J. Neurosurg. 2018, 129, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.H.; Madhavan, K.; Heros, D.; Raper, D.M.; Iorgulescu, J.B.; Lally, B.E.; Komotar, R.J. The management of incidental low-grade gliomas using magnetic resonance imaging: Systematic review and optimal treatment paradigm. Neurosurg. Focus 2011, 31, E12. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, T.S.; Grant, R.; Gilbert, M.R.; Lee, J.W.; Norden, A.D. Epilepsy in glioma patients: Mechanisms, management, and impact of anticonvulsant therapy. Neuro-Oncol. 2016, 18, 779–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ius, T.; Pauletto, G.; Isola, M.; Gregoraci, G.; Budai, R.; Lettieri, C.; Eleopra, R.; Fadiga, L.; Skrap, M. Surgery for insular low-grade glioma: Predictors of postoperative seizure outcome. J. Neurosurg. 2014, 120, 12–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudà, R.; Trevisan, E.; Soffietti, R. Epilepsy and brain tumors. Curr. Opin. Oncol. 2010, 22, 611–620. [Google Scholar] [CrossRef]
- Skrap, M.; Mondani, M.; Tomasino, B.; Weis, L.; Budai, R.; Pauletto, G.; Eleopra, R.; Fadiga, L.; Ius, T. Surgery of insular non-enhancing Gliomas: Volumetric analysis of tumoral resection, clinical outcome and survival in a consecutive series of 66 cases. Neurosurgery 2012, 70, 1081–1093. [Google Scholar] [CrossRef] [Green Version]
- Van Breemen, M.S.; Wilms, E.B.; Vecht, C.J. Epilepsy in patients with brain tumours: Epidemiology, mechanisms, and management. Lancet Neurol. 2007, 6, 421–430. [Google Scholar] [CrossRef]
- Weller, M.; Stupp, R.; Wick, W. Epilepsy meets cancer: When, why, and what to do about it? Lancet Oncol. 2012, 13, e375–e382. [Google Scholar] [CrossRef] [Green Version]
- Eskandary, H.; Sabba, M.; Khajehpour, F.; Eskandari, M. Incidental findings in brain computed tomography scans of 3000 head trauma patients. Surg. Neurol. 2005, 63, 550–553. [Google Scholar] [CrossRef] [PubMed]
- Jakola, A.S.; Myrmel, K.S.; Kloster, R.; Torp, S.H.; Lindal, S.; Unsgård, G.; Solheim, O. Comparison of a strategy favoring early surgical resection vs a strategy favoring watchful waiting in low-grade gliomas. JAMA 2012, 308, 1881–1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochereau, J.; Herbet, G.; Rigau, V.; Duffau, H. Acute progression of untreated incidental WHO Grade II glioma to glioblastoma in an asymptomatic patient. J. Neurosurg. 2016, 124, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Cochereau, J.; Herbet, G.; Duffau, H. Patients with incidental WHO grade II glioma frequently suffer from neuropsychological disturbances. Acta Neurochir. (Wien) 2016, 158, 305–312. [Google Scholar] [CrossRef]
- Duffau, H. Long-term outcomes after supratotal resection of diffuse low-grade gliomas: A consecutive series with 11-year follow-up. Acta Neurochir. (Wien) 2016, 158, 51–58. [Google Scholar] [CrossRef]
- Ius, T.; Cesselli, D.; Isola, M.; Pauletto, G.; Tomasino, B.; D’Auria, S.; Bagatto, D.; Pegolo, E.; Beltrami, A.P.; di Loreto, C.; et al. Incidental Low-Grade Gliomas: Single-Institution Management Based on Clinical, Surgical, and Molecular Data. Neurosurgery 2019, nyz114. [Google Scholar] [CrossRef]
- Lima, G.L.; Duffau, H. Is there a risk of seizures in “preventive” awake surgery for incidental diffuse low-grade gliomas? J. Neurosurg. 2015, 122, 1397–1405. [Google Scholar] [CrossRef]
- Lima, G.L.; Zanello, M.; Mandonnet, E.; Taillandier, L.; Pallud, J.; Duffau, H. Incidental diffuse low-grade gliomas: From early detection to preventive neuro-oncological surgery. Neurosurg. Rev. 2016, 39, 377–384. [Google Scholar] [CrossRef]
- Lima, G.L.O.; Dezamis, E.; Corns, R.; Rigaux-Viode, O.; Moritz-Gasser, S.; Roux, A.; Duffau, H.; Pallud, J. Surgical resection of incidental diffuse gliomas involving eloquent brain areas. Rationale, functional, epileptological and oncological outcomes. Neurochirurgie 2017, 63, 250–258. [Google Scholar] [CrossRef]
- Pallud, J.; Mandonnet, E. Incidental low-grade gliomas. J. Neurosurg. 2013, 118, 702–704. [Google Scholar] [CrossRef]
- Zhang, Z.Y.; Chan, A.K.; Ng, H.K.; Ding, X.J.; Li, Y.X.; Shi, Z.F.; Zhu, W.; Zhong, P.; Wang, Y.; Mao, Y.; et al. Surgically treated incidentally discovered low-grade gliomas are mostly IDH mutated and 1p19q co-deleted with favorable prognosis. Int. J. Clin. Exp. Pathol. 2014, 7, 8627–8636. [Google Scholar] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh Inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Capitani, E.; Laiacona, M. Aging and psychometric diagnosis of intellective impairment: Some considerations on test scores and their use. Dev. Neuropsychol 1988, 4, 325–330. [Google Scholar] [CrossRef]
- Weber, F.; Knopf, H. Incidental findings in magnetic resonance imaging of the brains of healthy young men. J. Neurol. Sci. 2006, 240, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Sanai, N.; Berger, M.S. Glioma extent of resection and its impact on patient outcome. Neurosurgery 2008, 62, 753–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, M.; Duffau, H.; Hamer, P.C.D.W. Cognition and resective surgery for diffuse infiltrative glioma: An overview. J. Neurooncol. 2012, 108, 309–318. [Google Scholar] [CrossRef] [Green Version]
- Basso, A.; Capitani, E.; Laiacona, M. Raven’s coloured progressive matrices: Normative values on 305 adult normal controls. Funct. Neurol. 1987, 2, 189–194. [Google Scholar]
- Crepaldi, D.; Aggujaro, S.; Arduino, L.S.; Zonca, G.; Ghirardi, G.; Inzaghi, M.G.; Colombo, M.; Chierchia, G.; Luzzatti, C. Noun-verb dissociation in aphasia: The role of imageability and functional locus of the lesion. Neuropsychologia 2006, 44, 73–89. [Google Scholar] [CrossRef]
- Miceli, G.; Laudanna, A.; Burani, C.; Capasso, R. Batteria per l’Analisi dei Deficit Afasici: BADA [BADA: A Battery for the Assessment of Aphasic Disorders]; CEPSAG: Roma, Italy, 1994. [Google Scholar]
- Gamboz, N.; Coluccia, E.; Iavarone, A.; Brandimonte, M.A. Normative data for the Pyramids and Palm Trees Test in the elderly Italian population. Neurol. Sci. 2009, 30, 453–458. [Google Scholar] [CrossRef]
- De Renzi, E.; Piezcuro, A.; Vignolo, L.A. Oral Apraxia and Aphasia. Cortex 1966, 2, 50–73. [Google Scholar] [CrossRef]
- Tessari, A.; Toraldo, A.; Lunardelli, A.; Zadini, A.; Rumiati, R.I. Prova standardizzata per la diagnosi del disturbo aprassico ideomotorio selettivo perntipo di gesto e tipo di effettore. Ricerche di Psicologia 2011, 3, 311–339. [Google Scholar]
- De Renzi, E.; Faglioni, P. Normative data and screening power of a shortened version of the Token Test. Cortex 1978, 14, 41–49. [Google Scholar] [CrossRef]
- Monaco, M.; Costa, A.; Caltagirone, C.; Carlesimo, G.A. Erratum to: Forward and backward span for verbal and visuo-spatial data: Standardization and normative data from an Italian adult population. Neurol. Sci. 2015, 36, 345–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail making test: Normative values from 287 normal adult controls. Ital. J. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Novelli, G.P.C.; Papagno, C.; Capitani, E.; Laiacona, M.; Vallar, G.; Cappa, S.F. Tre test clinici di ricerca e produzione lessicale.Taratura su soggetti normali. Archivio di Psicologia Neurologia e Psichiatria 1996, 47, 477–505. [Google Scholar]
- Mondini, S.; Mapelli, D.; Vestri, A.; Arcara, G.; Bisiacchi, P.S. Esame Neuropsicologico Breve 2; Raffaello Cortina Editore: Milan, Italy, 2011. [Google Scholar]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. Rey-Osterrieth complex figure: Normative values in an Italian population sample. Neurol. Sci. 2002, 22, 443–447. [Google Scholar] [CrossRef]
- Orsini, A.; Laicardi, C. WAIS-R. Contributo alla Taratura Italiana; Giunti Os: Florence, Italy, 1997. [Google Scholar]
- Wilson, B.A.; Cockburn, J.; Halligan, P.W. Behavioral Inattention Test (BIT); Thames Valley Test Company: London, UK, 1987. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| H | P# | WHO_2016 | Age | Ed | Site Surgery | H | V |
|---|---|---|---|---|---|---|---|
| LH | 1 | Diffuse astrocytoma, IDH mutant | 42 | 13 | F | 10 | |
| LH | 2 | Oligodendroglioma, IDH mutant and 1p/19q co-del | 40 | 13 | F | 100 | 18 |
| LH | 3 | Diffuse astrocytoma, IDH wildtype | 29 | 13 | F | 8 | |
| LH | 4 | Diffuse astrocytoma, IDH mutant | 20 | 13 | F | 100 | 12 |
| LH | 5 | Oligodendroglioma IDH mutant, 1p19q co-del | 52 | 13 | F | 100 | 26 |
| LH | 6 | Diffuse astrocytoma, IDH mutant | 25 | 13 | F | −100 | 15 |
| LH | 7 | Diffuse astrocytoma, IDH wildtype | 20 | 13 | T | 100 | 32 |
| LH | 8 | Diffuse astrocytoma, IDH mutant | 32 | 8 | F | 100 | 40 |
| LH | 9 | Diffuse astrocytoma, IDH mutant | 61 | 18 | T | 100 | 12 |
| LH | 10 | Diffuse astrocytoma, IDH wildtype | 46 | 11 | T | 50 | 12 |
| LH | 11 | Diffuse astrocytoma, IDH mutant | 40 | 16 | F | 100 | 34 |
| LH | 12 | Diffuse astrocytoma, IDH wildtype | 29 | 13 | P | 100 | 16 |
| LH | 13 | Diffuse astrocytoma, IDH mutant | 32 | 17 | P | 100 | 10 |
| LH | 14 | Oligodendroglioma, IDH mutant and 1p/19q co-del | 48 | 13 | F | 100 | 12 |
| LH | 15 | Diffuse astrocytoma, IDH mutant | 28 | 11 | T | 100 | 10 |
| LH | 16 | Oligodendroglioma IDH mutant, 1p19q co-del | 52 | 13 | F | 83 | 5 |
| RH | 1 | Diffuse astrocytoma, IDH mutant | 30 | 18 | F | 100 | 18 |
| RH | 2 | Oligodendroglioma, IDH mutant and 1p/19q co-del | 35 | 18 | F | 100 | 22 |
| RH | 3 | Diffuse astrocytoma, IDH mutant | 26 | 17 | F | 14 | |
| RH | 4 | Diffuse astrocytoma, IDH mutant | 30 | 18 | F | 100 | 18 |
| RH | 5 | Diffuse astrocytoma, IDH mutant | 71 | 8 | F | 100 | 8 |
| RH | 6 | Diffuse astrocytoma, IDH mutant | 45 | 8 | F | 100 | 27 |
| RH | 7 | Oligodendroglioma, IDH mutant and 1p/19q co-del | 49 | 13 | F | 100 | 8 |
| RH | 8 | Oligodendroglioma, IDH mutant and 1p/19q co-del | 25 | 13 | F | 100 | 10 |
| Reason to Perform MRI | Number of Cases |
|---|---|
| Headache * | 4 |
| Otolaryngology disorders ^ | 3 |
| Mental confusion | 1 |
| Hearing disturbance | 2 |
| Sensitive disorders ^ | 6 |
| Dizziness | 2 |
| Other | 2 |
| Neuropsychological Evaluation | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intelligence | Memory | Praxis | Language | Executive Functions | Memory | Visuo-Spatial | Psychomotor Speed | |||||||||||||
| H | P# | RAVEN | V_STM | WM | O_prax | IMA | V_comp | N_nam | V_nam | Ph_Flu | TMT A | TMT B | TMTB-A | S_STM | S_WM | C_pra | Clock | Bit_St | Line_bis | Dig_Sym |
| LH | 1 | 35 | 5,6 | 2,6 | 19,75 | Na | 32,5 | 29 | 23 | 26 | 32 | 135 | 117 | Na | Na | Na | Na | Na | Na | Na |
| LH | 2 | 33 | 5,6 | 3,6 | 19,75 | 72 | 33,5 | 30 | 28 | 31 | 23 | 76 | 53 | Na | Na | Na | Na | Na | Na | Na |
| LH | 3 | 32 | 5,5 | 4,5 | 19,75 | Na | 33,5 | 30 | 28 | 62 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 4 | 33 | 8,4 | 3,4 | 19,75 | 72 | 33,5 | 28 | 28 | 45 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 5 | Na | 3,6 | 3,6 | 19,75 | 71 | 29,8 | 29 | 24 | 40 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 6 | 31 | 5,4 | 4,4 | 19,75 | 72 | 33,5 | 29 | 28 | 20 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 7 | 26 | 4,4 | 2,4 | Na | 72 | 33,5 | 30 | 28 | 49 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 8 | 27 | 4,7 | 3,8 | 19,75 | 72 | 34,8 | 29 | 27 | 20 | 33 | 93 | 65 | Na | Na | Na | Na | Na | Na | Na |
| LH | 9 | 34 | 5,8 | 4,7 | 20 | 72 | 31,5 | Na | 28 | 49 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 10 | 34 | Na | Na | 19,75 | 72 | 33,5 | 30 | 28 | 34 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 11 | 31 | 7,5 | 4,4 | 19,75 | 72 | 32,8 | 29 | 28 | 29 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 12 | Na | Na | Na | 19,75 | 72 | 33,5 | 30 | 27 | 40 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 13 | 30 | 4,4 | 3,3 | 19,75 | Na | 32,8 | 28 | 27 | 34 | 46 | 137 | 180 | Na | Na | Na | Na | Na | Na | Na |
| LH | 14 | 33 | 4,8 | 3,7 | 19,75 | Na | 34 | 29 | 27 | 29 | 25 | 92 | 67 | Na | Na | Na | Na | Na | Na | Na |
| LH | 15 | Na | 5,4 | Na | 19,75 | Na | Na | 23 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| LH | 16 | Na | 7 | Na | 19,75 | Na | Na | 28 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na |
| RH | 1 | 28 | Na | Na | Na | Na | Na | Na | Na | Na | 37 | 125 | 88 | Na | Na | 12 | 10 | 53 | 9 | Na |
| RH | 2 | 32 | Na | Na | Na | Na | Na | Na | Na | Na | 51 | 113 | 62 | 6,4 | 3,5 | 12 | 10 | 52 | Na | 62 |
| RH | 3 | 32 | Na | Na | Na | Na | Na | Na | Na | Na | 44 | 141 | 96 | 5,3 | 5,4 | 12 | 10 | Na | 9 | 47 |
| RH | 4 | 30 | Na | Na | Na | Na | Na | Na | Na | Na | 61 | 156 | 95 | 5,3 | 3,4 | 12 | 10 | 54 | 9 | 46 |
| RH | 5 | 30 | Na | Na | Na | Na | Na | Na | Na | Na | 27 | 26 | -1 | 4,4 | 4,3 | 13 | 10 | 52 | 9 | 50 |
| RH | 6 | 28 | Na | Na | Na | Na | Na | Na | Na | Na | 31 | 70 | 39 | 4,9 | 3,7 | 13 | 10 | 54 | 9 | 48 |
| RH | 7 | 36 | Na | Na | Na | Na | Na | Na | Na | Na | 27 | 53 | 26 | 5,7 | 4,8 | 13 | 10 | Na | 9 | 57 |
| RH | 8 | 28 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | 8,5 | 54 | Na | Na |
| H | P# | Au_N_Comp | Au_V_comp | P&P | W_Read | Pw_Read | W_Rep | Pw_Rep | W_Wri | Pw_Wri | Phon_Disc | Au_lex-dec | Vis_lex-dec | Rey_C | Rey_R | BIT Let |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LH | 1 | 40 | 20 | Na | 45 | 45 | 45 | 20 | 15 | 25 | 60 | 88 | 99 | Na | Na | Na |
| LH | 2 | Na | Na | Na | 45 | 45 | 45 | 35 | 25 | 25 | 60 | 80 | 80 | Na | Na | Na |
| LH | 3 | 40 | 20 | 50 | 45 | 45 | 45 | 35 | 25 | 25 | 60 | 80 | 80 | Na | Na | Na |
| LH | 4 | 40 | 20 | 49 | 45 | 45 | 45 | 35 | 25 | 25 | 60 | 79 | 77 | Na | Na | Na |
| LH | 9 | 40 | 20 | 49 | Na | 45 | 45 | 35 | 25 | 25 | 60 | 80 | 80 | Na | Na | Na |
| LH | 11 | 40 | 20 | 48 | 45 | 45 | 45 | 35 | 25 | 25 | 60 | 80 | 80 | Na | Na | Na |
| LH | 13 | 40 | 20 | 48 | 45 | 45 | 45 | 35 | 25 | 25 | 60 | 80 | 80 | Na | Na | Na |
| RH | 3 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | 33 | 24 | Na |
| RH | 4 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | 35 |
| RH | 5 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | 36 |
| RH | 6 | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | Na | 35 | 5,3 | 36 |
| Area | Hemisphere | MNI | % Overlap | ||
|---|---|---|---|---|---|
| x | y | z | |||
| Inferior Frontal Gyrus (opercular) | LH | −46 | 15 | 13 | 23.52% |
| Anterior cingulate | RH | 9 | 35 | 27 | 50% |
| Superior medial gyrus | EH | 9 | 36 | 50 | 37.5% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarracino, I.; Ius, T.; Pegolo, E.; Cesselli, D.; Skrap, M.; Tomasino, B. Multimodal Assessment Shows a Mostly Preserved Cognitive Status in Incidentally Discovered Low Grade Gliomas: A Single Institution Study. Cancers 2020, 12, 156. https://doi.org/10.3390/cancers12010156
Guarracino I, Ius T, Pegolo E, Cesselli D, Skrap M, Tomasino B. Multimodal Assessment Shows a Mostly Preserved Cognitive Status in Incidentally Discovered Low Grade Gliomas: A Single Institution Study. Cancers. 2020; 12(1):156. https://doi.org/10.3390/cancers12010156
Chicago/Turabian StyleGuarracino, Ilaria, Tamara Ius, Enrico Pegolo, Daniela Cesselli, Miran Skrap, and Barbara Tomasino. 2020. "Multimodal Assessment Shows a Mostly Preserved Cognitive Status in Incidentally Discovered Low Grade Gliomas: A Single Institution Study" Cancers 12, no. 1: 156. https://doi.org/10.3390/cancers12010156