Long-Term Visual Outcomes for Small Uveal Melanoma Staged T1 Treated by Proton Beam Radiotherapy

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Visual Acuity Outcomes
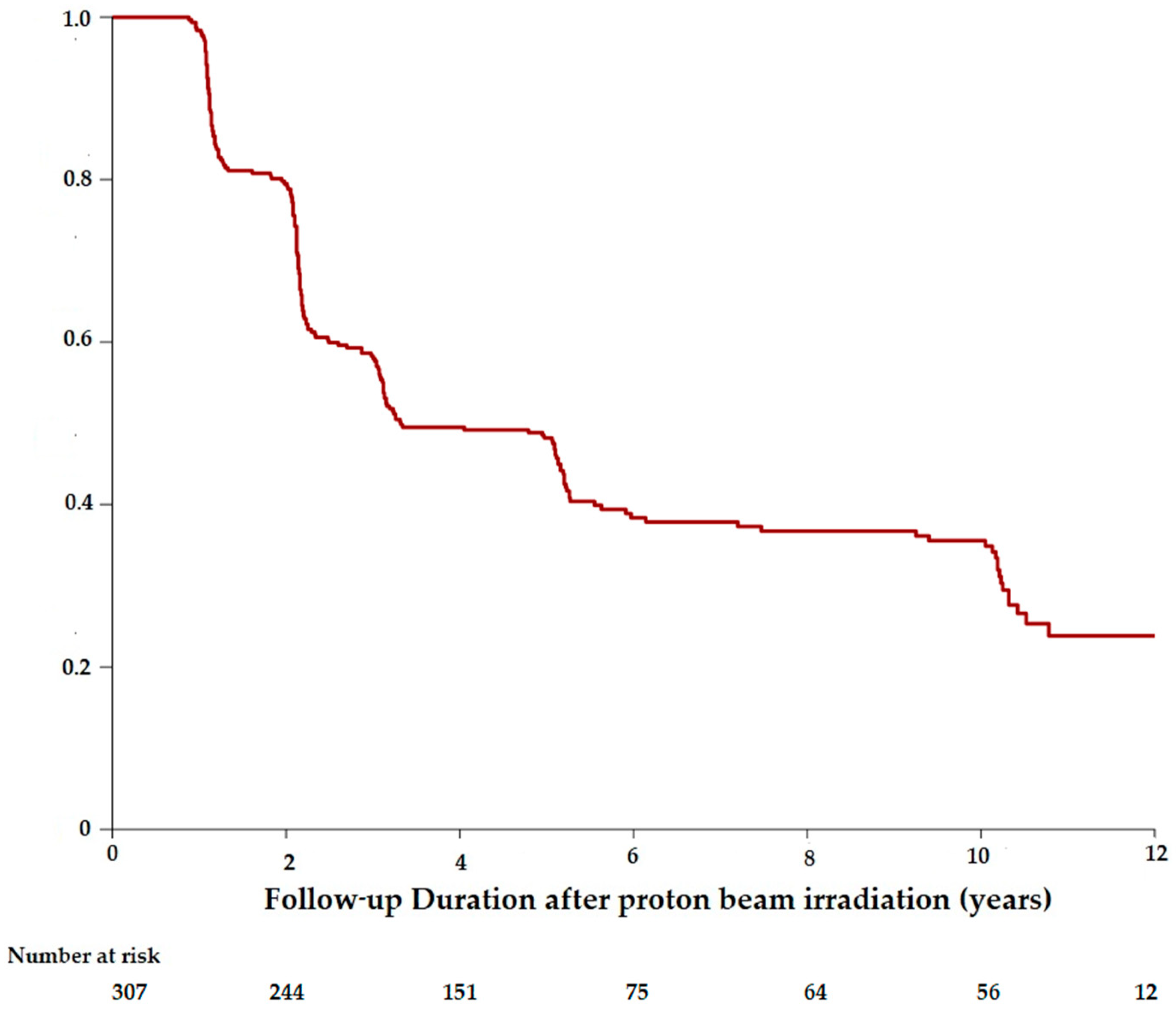
3.1.1. Visual Outcomes in the Cohort
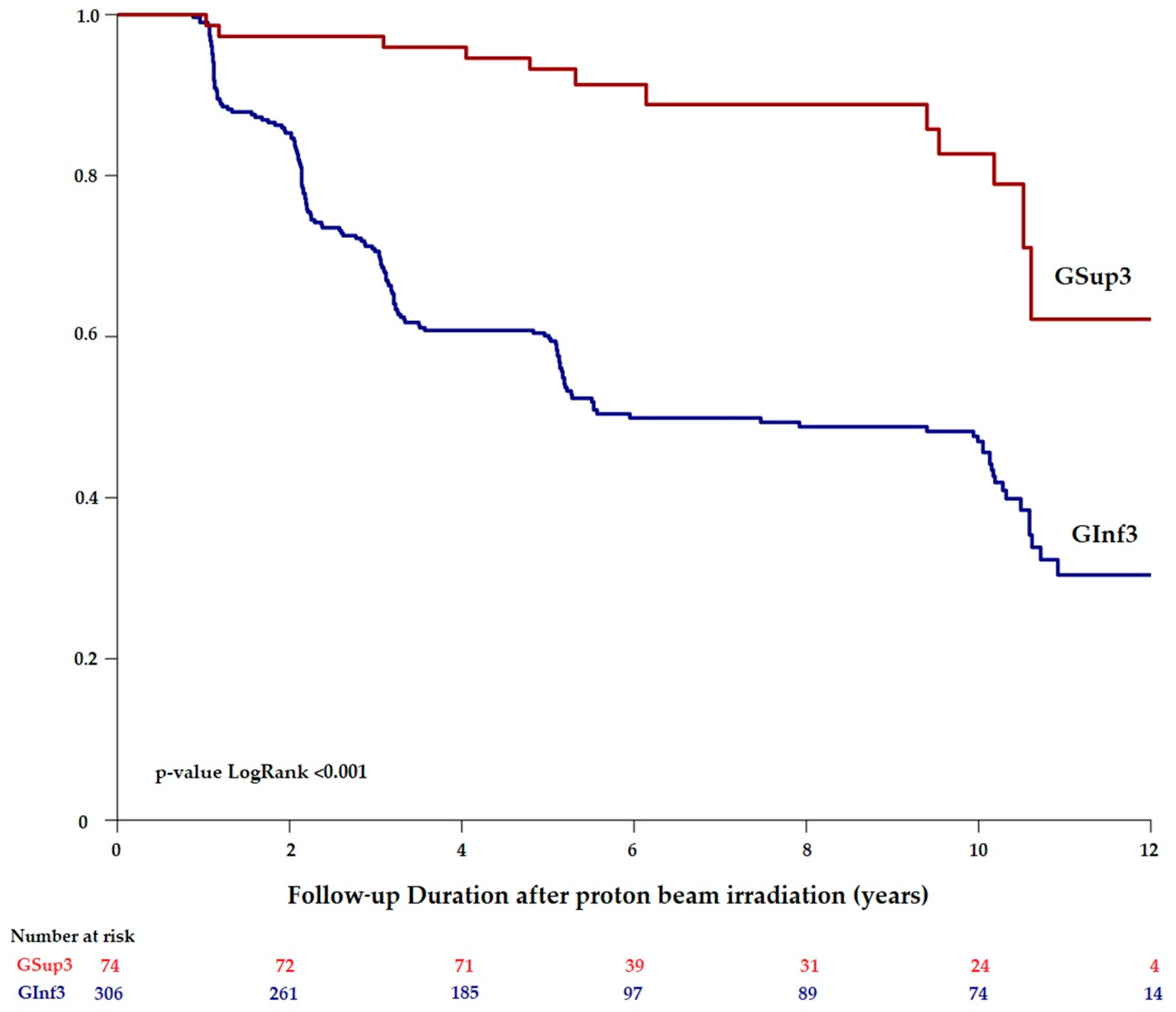
3.1.2. Visual Outcomes in Gsup3 and in GInf3
3.2. Risk Factors Associated with Vision Loss after Irradiation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Damato, B. Ocular treatment of choroidal melanoma in relation to the prevention of metastatic death A personal view. Prog. Retin. Eye Res. 2018, 66, 187–199. [Google Scholar] [PubMed]
- Desjardins, L.; Lumbroso-Le, R.L.; Levy-Gabriel, C.; Cassoux, N.; Dendale, R.; Mazal, A.; Delacroix, S.; Sastre, X.; Plancher, C.; Asselain, B. Treatment of uveal melanoma by accelerated proton beam. Dev. Ophthalmol. 2012, 49, 41–57. [Google Scholar] [PubMed]
- Dendale, R.; Lumbroso-Le, R.L.; Noel, G.; Feuvret, L.; Levy, C.; Delacroix, S.; Meyer, A.; Nauraye, C.; Mazal, A.; Mammar, H.; et al. Proton beam radiotherapy for uveal melanoma: results of Curie Institut-Orsay proton therapy center (ICPO). Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 780–787. [Google Scholar] [PubMed]
- Shields, C.L.; Sioufi, K.; Srinivasan, A.; Nicola, M.; Masoomian, B.; Barna, L.E.; Bekerman, V.P.; Say, E.A.T.; Mashayekhi, A.; Emrich, J.; et al. Visual Outcome and Millimeter Incremental Risk of Metastasis in 1780 Patients with Small Choroidal Melanoma Managed by Plaque Radiotherapy. JAMA Ophthalmol. 2018, 136, 1325–1333. [Google Scholar] [PubMed]
- Lane, A.M.; Kim, I.K.; Gragoudas, E.S. Proton irradiation for peripapillary and parapapillary melanomas. Arch. Ophthalmol. 2011, 129, 1127–1130. [Google Scholar] [PubMed]
- Kim, I.K.; Lane, A.M.; Egan, K.M.; Munzenrider, J.; Gragoudas, E.S. Natural history of radiation papillopathy after proton beam irradiation of parapapillary melanoma. Ophthalmology 2010, 117, 1617–1622. [Google Scholar] [PubMed]
- Seibel, I.; Cordini, D.; Hager, A.; Tillner, J.; Riechardt, A.I.; Heufelder, J.; Davids, A.M.; Rehak, M.; Joussen, A.M. Predictive risk factors for radiation retinopathy and optic neuropathy after proton beam therapy for uveal melanoma. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 1787–1792. [Google Scholar] [PubMed]
- Riechardt, A.I.; Cordini, D.; Willerding, G.D.; Georgieva, I.; Weber, A.; Seibel, I.; Lakotka, N.; Bechrakis, N.E.; Foerster, M.H.; Moser, L.; et al. Proton beam therapy of parapapillary choroidal melanoma. Am. J. Ophthalmol. 2014, 157, 1258–1265. [Google Scholar] [PubMed]
- Groenewald, C.; Konstantinidis, L.; Damato, B. Effects of radiotherapy on uveal melanomas and adjacent tissues. Eye (Lond) 2013, 27, 163–171. [Google Scholar]
- Papakostas, T.D.; Lane, A.M.; Morrison, M.; Gragoudas, E.S.; Kim, I.K. Long-term Outcomes After Proton Beam Irradiation in Patients with Large Choroidal Melanomas. JAMA Ophthalmol. 2017, 135, 1191–1196. [Google Scholar]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual; Springer Nature: Basel, Switzerland, 2017; pp. 1–1024. [Google Scholar]
- Damato, B.; Kacperek, A.; Chopra, M.; Campbell, I.R.; Errington, R.D. Proton beam radiotherapy of choroidal melanoma: The Liverpool-Clatterbridge experience. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 1405–1411. [Google Scholar] [PubMed]
- Gragoudas, E.; Li, W.; Goitein, M.; Lane, A.M.; Munzenrider, J.E.; Egan, K.M. Evidence-based estimates of outcome in patients irradiated for intraocular melanoma. Arch. Ophthalmol. 2002, 120, 1665–1671. [Google Scholar] [PubMed]
- Gragoudas, E.S.; Lane, A.M.; Munzenrider, J.; Egan, K.M.; Li, W. Long-term risk of local failure after proton therapy for choroidal/ciliary body melanoma. Trans. Am. Ophthalmol. Soc. 2002, 100, 43–48. [Google Scholar] [PubMed]
- Gragoudas, E.S. The Bragg peak of proton beams for treatment of uveal melanoma. Int. Ophthalmol. Clin. 1980, 20, 123–133. [Google Scholar]
- Lane, A.M.; Kim, I.K.; Gragoudas, E.S. Long-term Risk of Melanoma-Related Mortality for Patients with Uveal Melanoma Treated with Proton Beam Therapy. JAMA Ophthalmol. 2015, 133, 792–796. [Google Scholar]
- Vavvas, D.; Kim, I.; Lane, A.M.; Chaglassian, A.; Mukai, S.; Gragoudas, E. Posterior uveal melanoma in young patients treated with proton beam therapy. Retina 2010, 30, 1267–1271. [Google Scholar]
- Patel, A.V.; Lane, A.M.; Morrison, M.A.; Trofimov, A.V.; Shih, H.A.; Gragoudas, E.S.; Kim, I.K. Visual Outcomes after Proton Beam Irradiation for Choroidal Melanomas Involving the Fovea. Ophthalmology 2016, 123, 369–377. [Google Scholar]
- Schönfeld, S.; Cordini, D.; Riechardt, A.I.; Seibel, I.; Willerding, G.; Bechrakis, N.E.; Moser, L.; Joussen, A.M. Proton beam therapy leads to excellent local control rates in choroidal melanoma in the intermediate fundus zone. Am. J. Ophthalmol. 2014, 158, 1184–1191. [Google Scholar]
- Seddon, J.M.; Gragoudas, E.S.; Egan, K.M.; Glynn, R.J.; Munzenrider, J.E.; Austin-Seymour, M.; Goitein, M.; Verhey, L.; Urie, M.; Koehler, A. Uveal melanomas near the optic disc or fovea. Visual results after proton beam irradiation. Ophthalmology 1987, 94, 354–361. [Google Scholar]
- Char, D.H. The management of small choroidal melanomas. Surv. Ophthalmol. 1978, 22, 377–386. [Google Scholar]
- Seddon, J.M.; Gragoudas, E.S.; Polivogianis, L.; Hsieh, C.C.; Egan, K.M.; Goitein, M.; Verhey, L.; Munzenrider, J.; Austin-Seymour, M.; Urie, M. Visual outcome after proton beam irradiation of uveal melanoma. Ophthalmology 1986, 93, 666––674. [Google Scholar]
- Shields, C.L.; Shields, J.A.; Cater, J.; Gündüz, K.; Miyamoto, C.; Micaily, B.; Brady, L.W. Plaque radiotherapy for uveal melanoma: Long-term visual outcome in 1106 consecutive patients. Arch. Ophthalmol. 2000, 118, 1219–1228. [Google Scholar] [PubMed]
- Matet, A.; Daruich, A.; Zografos, L. Radiation Maculopathy After Proton Beam Therapy for Uveal Melanoma: Optical Coherence Tomography Angiography Alterations Influencing Visual Acuity. Invest. Ophthalmol. Vis. Sci. 2017, 58, 3851–3861. [Google Scholar] [PubMed]
- Sellam, A.; Coscas, F.; Lumbroso-Le Rouic, L.; Dendale, R.; Lupidi, M.; Coscas, G.; Desjardins, L.; Cassoux, N. Optical Coherence Tomography Angiography of Macular Features After Proton Beam Radiotherapy for Small Choroidal Melanoma. Am. J. Ophthalmol. 2017, 181, 12–19. [Google Scholar] [PubMed]
- Veverka, K.K.; AbouChehade, J.E.; Iezzi, R.; Pulido, J.S. Noninvasive Grading of Radiation Retinopathy: The Use of Optical Coherence Tomography Angiography. Retina 2015, 35, 2400–2410. [Google Scholar] [PubMed]
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [PubMed]
- Shields, C.L.; Kaliki, S.; Furuta, M.; Fulco, E.; Alarcon, C.; Shields, J.A. American Joint Committee on Cancer Classification of Uveal Melanoma (Anatomic Stage) Predicts Prognosis in 7,731 Patients: The 2013 Zimmerman Lecture. Ophthalmology 2015, 122, 1180–1186. [Google Scholar] [PubMed]
- Boldt, H.C.; Binkley, E. Treating Small Choroidal Melanoma: Smaller Is Better. JAMA Ophthalmol. 2018, 136, 1333–1334. [Google Scholar]
- Factors predictive of growth and treatment of small choroidal melanoma: COMS Report No.5. The Collaborative Ocular Melanoma Study Group. Arch. Ophthalmol. 1997, 115, 1537–1544.
- Shields, C.L.; Demirci, H.; Materin, M.A.; Marr, B.P.; Mashayekhi, A.; Shields, J.A. Clinical factors in the identification of small choroidal melanoma. Can. J. Ophthalmol. 2004, 39, 351–357. [Google Scholar]
- Shields, C.L.; Shields, J.A.; Kiratli, H.; De Potter, P.; Cater, J.R. Risk factors for growth and metastasis of small choroidal melanocytic lesions. Trans. Am. Ophthalmol. Soc. 1995, 93, 259–275. [Google Scholar] [PubMed]
- Augsburger, J.J.; Schroeder, R.P.; Territo, C.; Gamel, J.W.; Shields, J.A. Clinical parameters predictive of enlargement of melanocytic choroidal lesions. Br. J. Ophthalmol. 1989, 73, 911–917. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value | Range or Percentage |
|---|---|---|
| Sex, no., % | ||
| Female | 220 | |
| Male | 204 | |
| Eye, no., % | ||
| Right | 226 | |
| Left | 198 | |
| Tumor dimension, median (range), mm | ||
| Basal tumor diameter | 8.8 | |
| Tumor thickness | 2.8 | |
| Distance, mean (range), mm | ||
| To optic disc | 3.3 | |
| To fovea | 2.6 | |
| Ocular location of the tumor, no., % | ||
| Tumor invaded ciliary body | 6 | |
| Tumor touching optic disc | 45 | |
| Non applicable | 373 | |
| Ocular location of the tumor, no., % | ||
| Ante equatorial location | 11 | |
| Equatorial location | 30 | |
| Post equatorial Location | 383 | |
| Documented growth, no., % | 141 | 33.3% |
| Initial Findings, no., % | ||
| Initial Extra scleral spread | 1 | |
| Initial retinal detachment | 54 | |
| Initial macular edema | 15 | |
| Intravitreal hemorrhage | 2 | |
| Amelanotic tumor (partially or totally unpigmented) | 73 | |
| Characteristics | Patients | Percentage |
|---|---|---|
| Patient status, no., % | ||
| Alive | 385 | |
| Dead from all-cause mortality | 39 | |
| T1UM with metastatic disease, no., % | ||
| Initial UM metastasis | 0 | |
| Patients with UM metastases during 5-year follow-up | 12 | |
| Patients without metastases | 412 | |
| Metastases location, no., % | ||
| Liver metastases | 11 | |
| Multisystemic metastases (liver, lungs, skin) | 1 |
| Patients | Hazard Ratio | 95% Confidence Interval (95%CI) | |
|---|---|---|---|
| Age (years) | |||
| ≤60 | 243 | 1 | |
| >60 | 165 | 1.75 | (1.28; 2.38) |
| Documented growth | |||
| Yes | 133 | 1 | |
| No | 275 | 0.6 | (0.43; 0.83) |
| Distance to fovea-optic disc | |||
| <3 mm (GInf3) | 306 | 1 | |
| ≥3 mm (GSup3) | 74 | 0.29 | (0.16; 0.54) |
| Initial visual acuity (Snellen scale) | |||
| <20/40 | 155 | 1 | |
| ≥20/40 | 250 | 0.45 | (0.33; 0.62) |
| Tumor touching optic disc | |||
| No | 359 | 1 | |
| Yes | 42 | 1.62 | (1.06; 2.49) |
| Initial retinal detachment | |||
| No | 355 | 1 | |
| Yes | 52 | 0.87 | (0.55; 1.38) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toutée, A.; Angi, M.; Dureau, S.; Lévy-Gabriel, C.; Rouic, L.L.-L.; Dendale, R.; Desjardins, L.; Cassoux, N. Long-Term Visual Outcomes for Small Uveal Melanoma Staged T1 Treated by Proton Beam Radiotherapy. Cancers 2019, 11, 1047. https://doi.org/10.3390/cancers11081047
Toutée A, Angi M, Dureau S, Lévy-Gabriel C, Rouic LL-L, Dendale R, Desjardins L, Cassoux N. Long-Term Visual Outcomes for Small Uveal Melanoma Staged T1 Treated by Proton Beam Radiotherapy. Cancers. 2019; 11(8):1047. https://doi.org/10.3390/cancers11081047
Chicago/Turabian StyleToutée, Adélaïde, Martina Angi, Sylvain Dureau, Christine Lévy-Gabriel, Livia Lumbroso-Le Rouic, Rémi Dendale, Laurence Desjardins, and Nathalie Cassoux. 2019. "Long-Term Visual Outcomes for Small Uveal Melanoma Staged T1 Treated by Proton Beam Radiotherapy" Cancers 11, no. 8: 1047. https://doi.org/10.3390/cancers11081047
APA StyleToutée, A., Angi, M., Dureau, S., Lévy-Gabriel, C., Rouic, L. L.-L., Dendale, R., Desjardins, L., & Cassoux, N. (2019). Long-Term Visual Outcomes for Small Uveal Melanoma Staged T1 Treated by Proton Beam Radiotherapy. Cancers, 11(8), 1047. https://doi.org/10.3390/cancers11081047