Arytenoid Fixation in Laryngeal Cancer: Radiological Pictures and Clinical Correlations with Respect to Conservative Treatments

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Radiologic Assessment
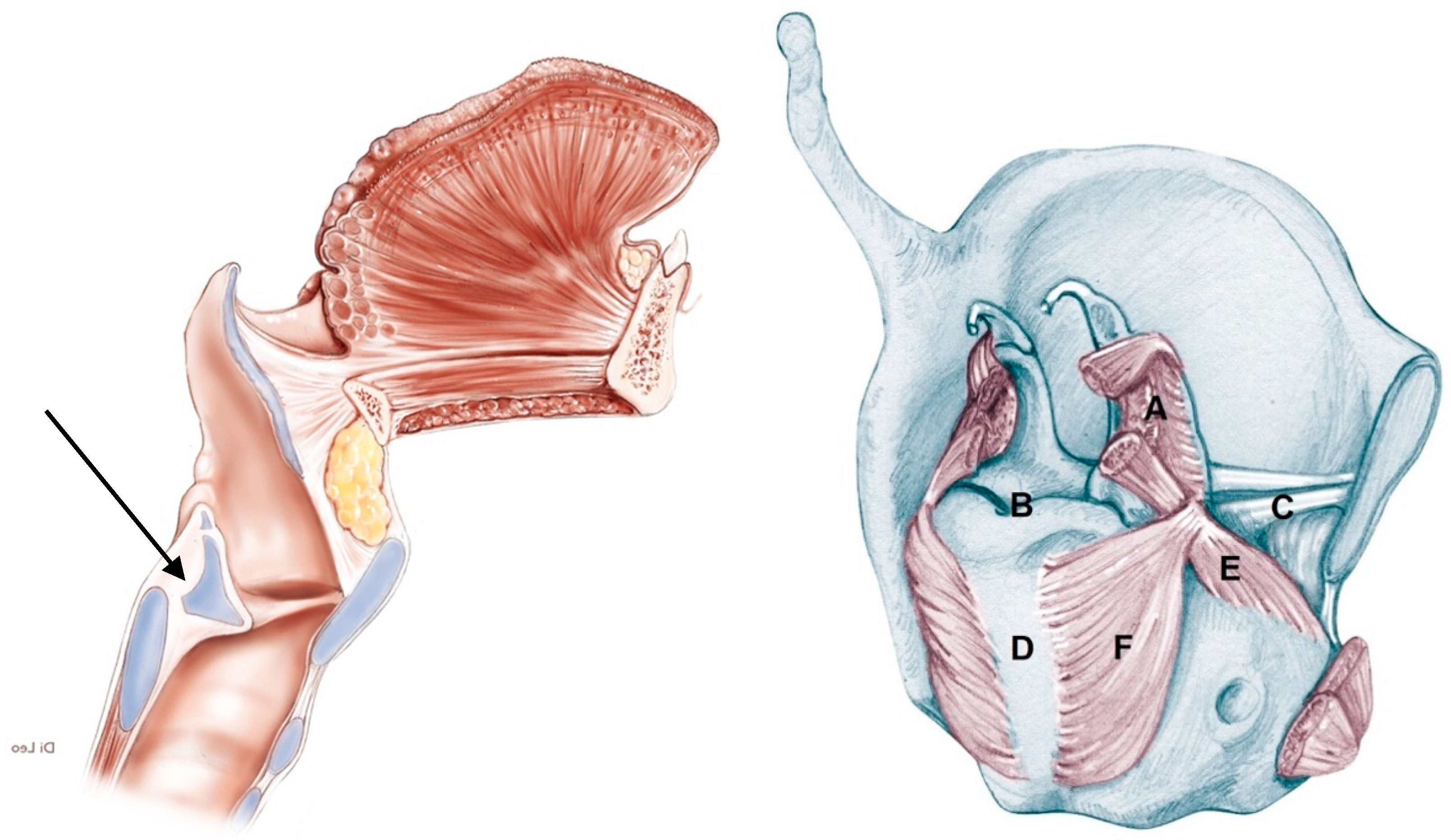
2.3. Pattern of Arytenoid Fixation
- 1)
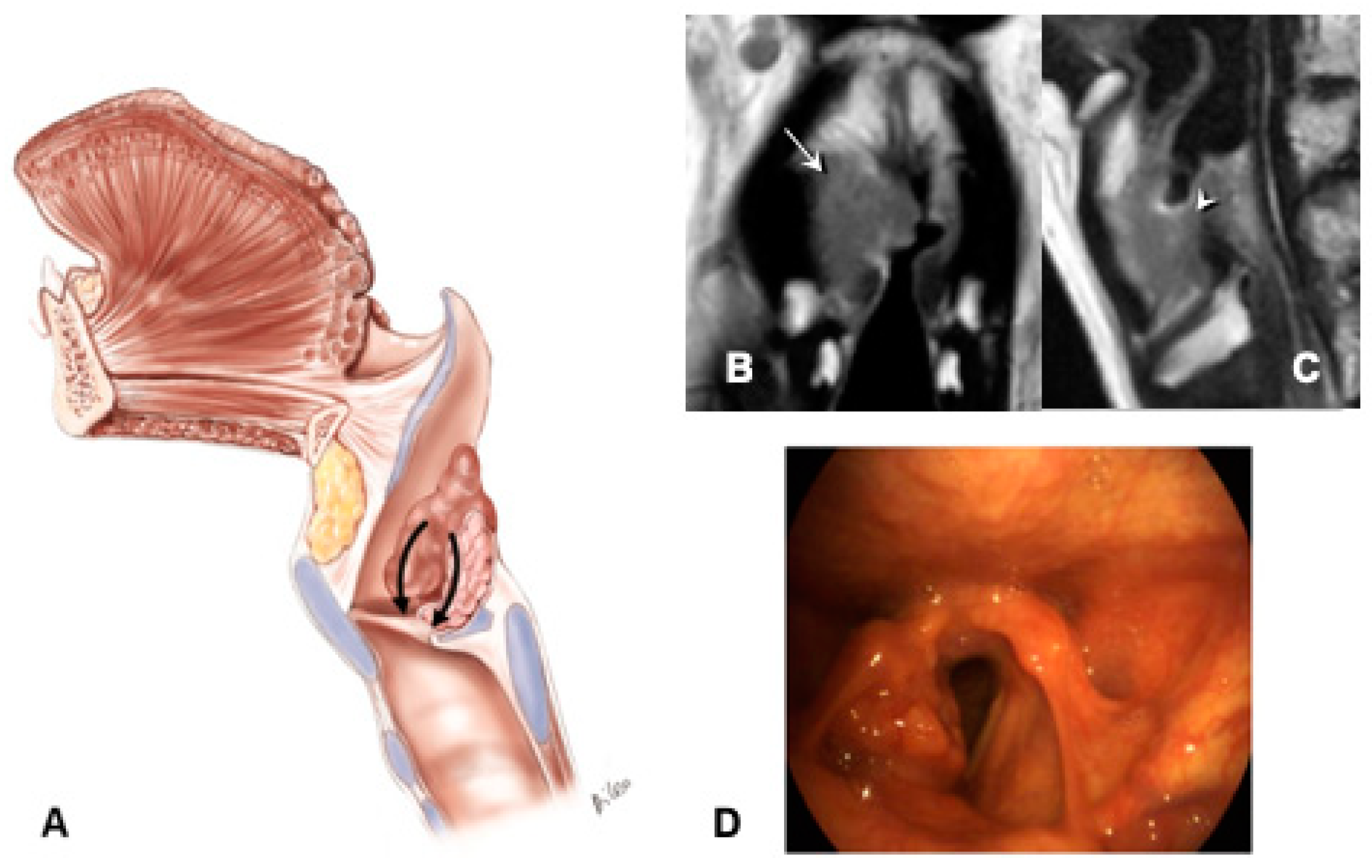
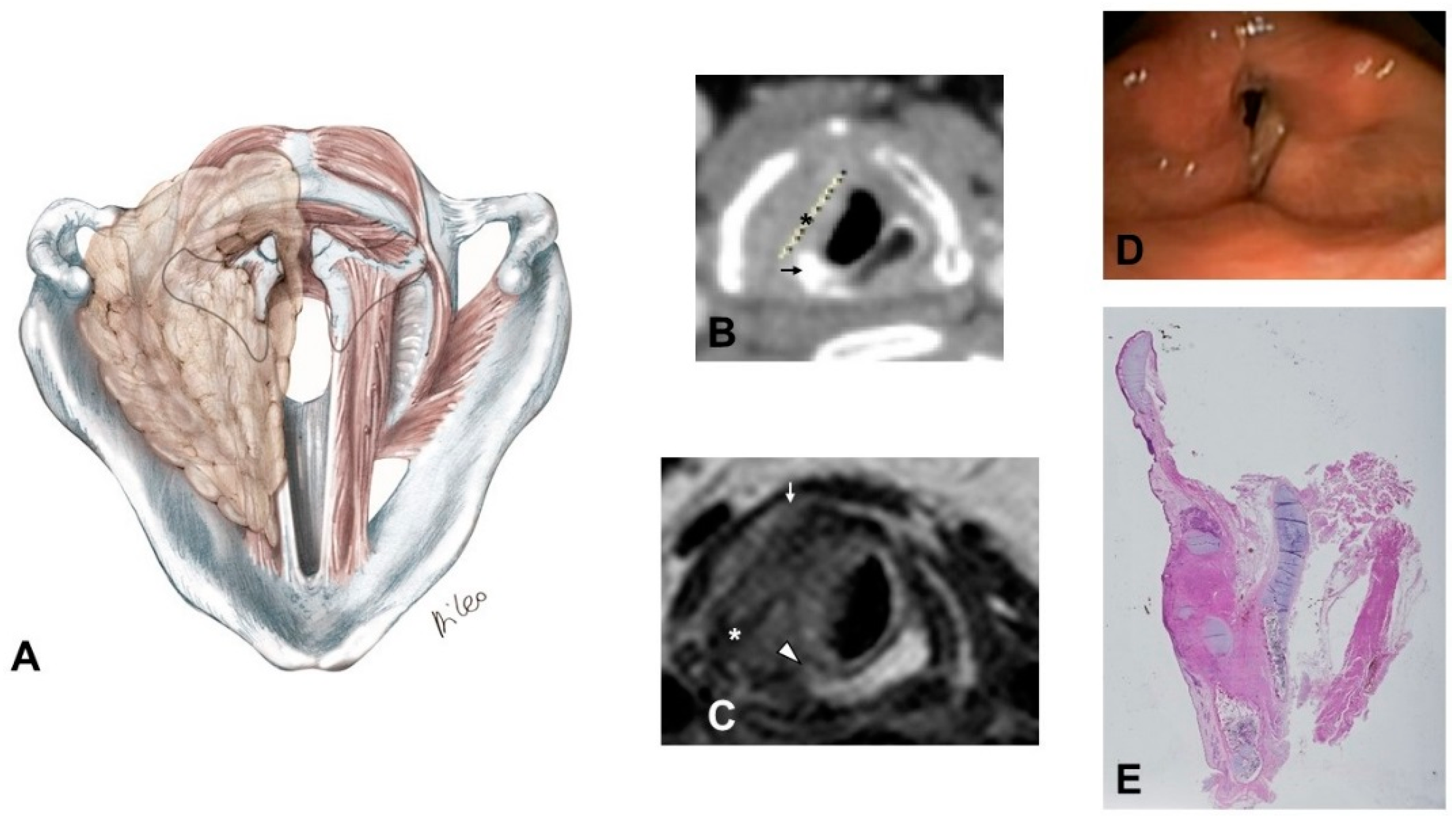
- Supraglottic carcinoma encasing the arytenoid from above with its fixation due to weight effect, without direct involvement of the CAU (Figure 2):
- –
- The tumor infiltrates the superior paraglottic space (SPGS) and the thyro-arytenoid muscle (TAM) without direct involvement of the crico-arytenoid unit (CAU), with evaluation of the following radiological parameters: superior paraglottic space (SPGS), TAM, inferior paraglottic space (IPGS), crico-arytenoid joint (CAJ) and cricoid plate.
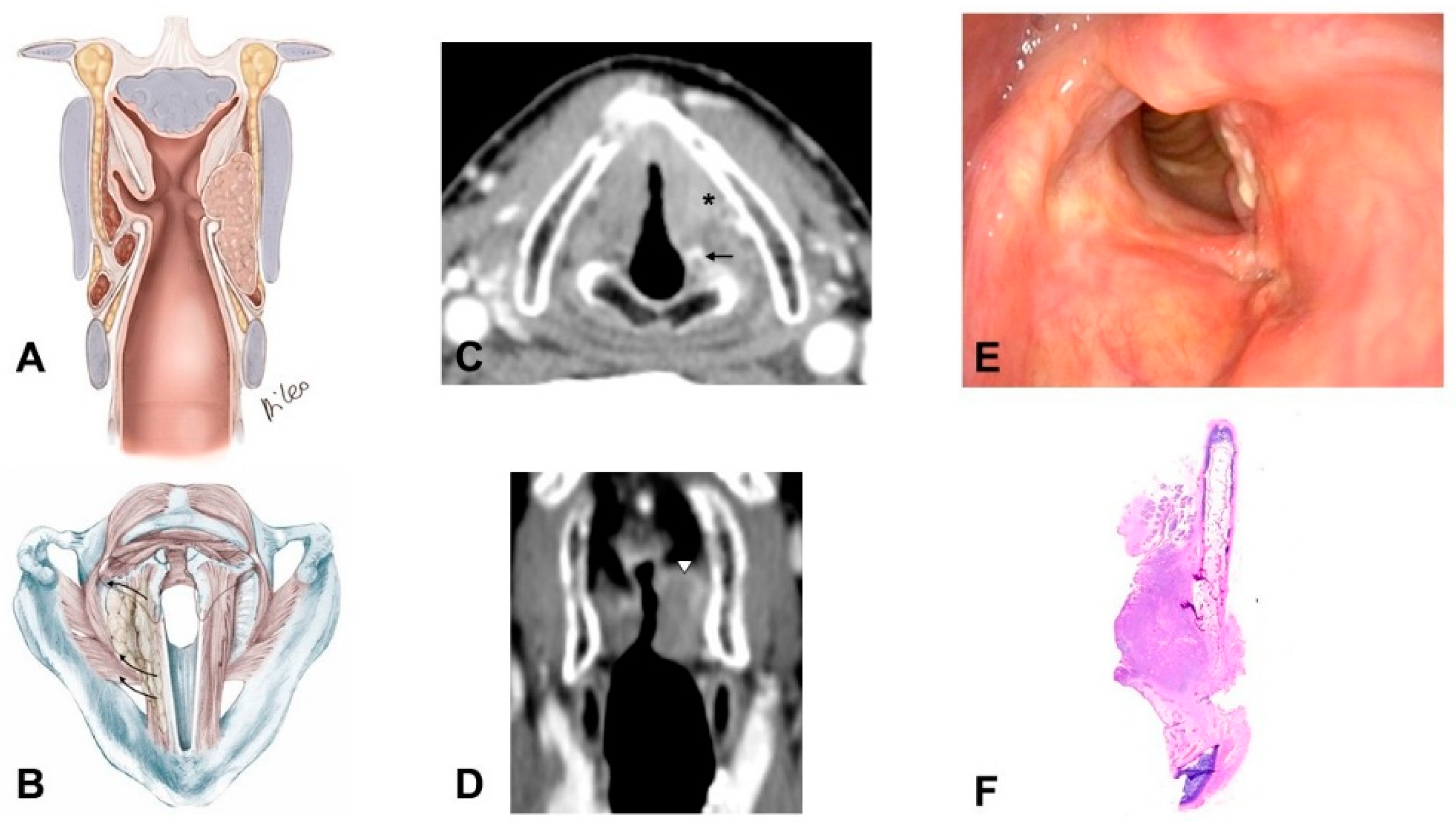
- 2)
- Glottic carcinoma involving the IPGS and extending toward the CAU, medially contained by the conus elasticus and laterally by the thyroid wing (Figure 3):
- –
- The tumor extends in part to the SPGS becoming transglottic.
- –
- It involves TAM, IPGS, thyro-arytenoid space and/or posterior crico-thyroid space and blocks the arytenoid laterally corresponding to the lateral crico-arytenoid muscle; the tumor involves or invades the arytenoid but not the cricoid (that can present signs of sclerosis anyway), and there is the strong doubt about CAJ involvement, even if in part.
- –
- The eventual infraglottic extension, evaluated exactly at the free edge of the TVC midline, is ≤10 mm.
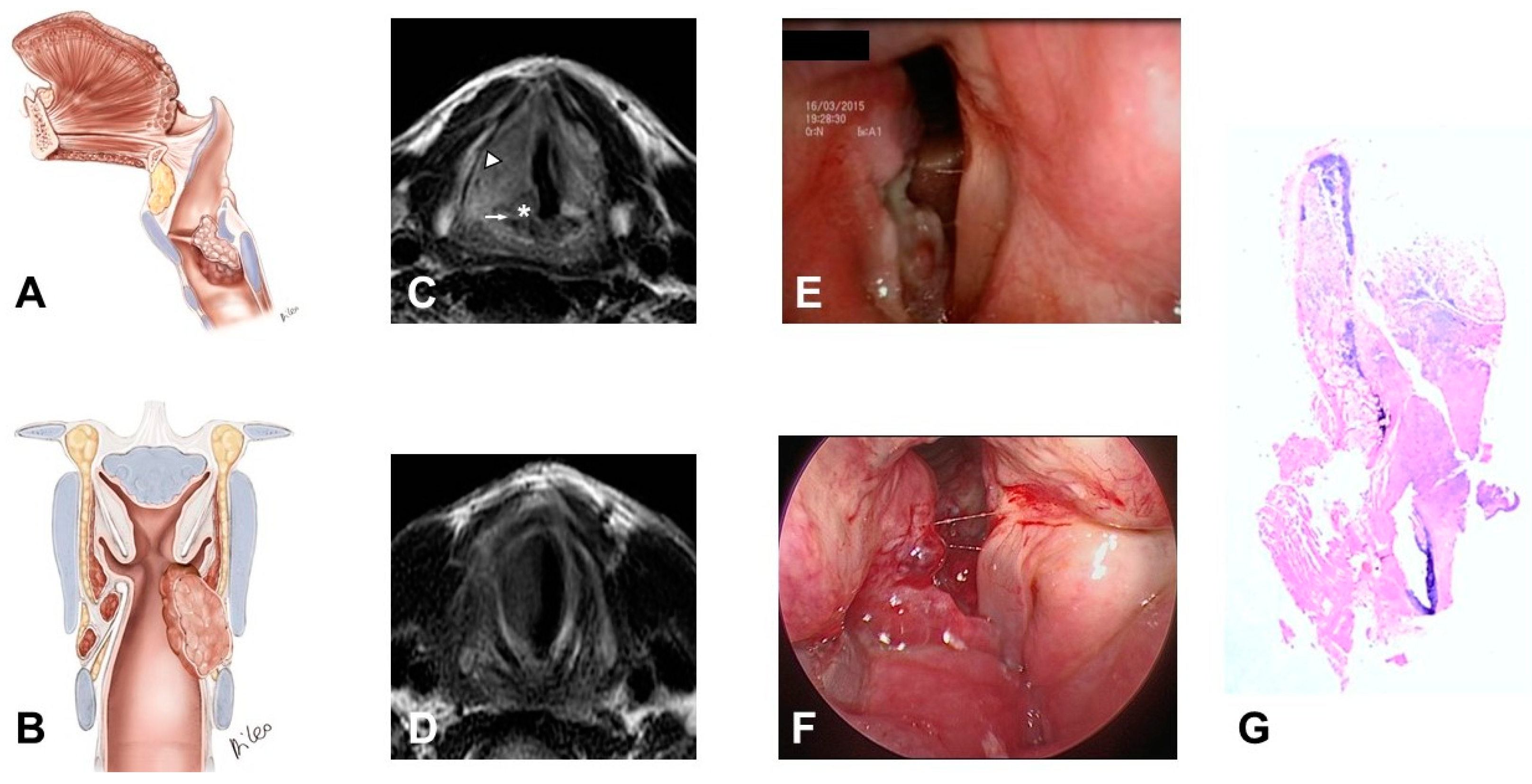
- 3)
- Glottic-subglottic carcinoma invading the CAJ, and wrapping around it, because the tumor can have type II progression together with CAJ invasion through the conus elasticus with medial to lateral progression (Figure 4):
- –
- The tumor massively involves the IPGS, the thyro-arytenoid space and/or posterior crico-thyroid space and blocks the arytenoid laterally corresponding to the lateral crico-arytenoid muscle, it involves or invades the arytenoid and often the cricoid. Cricoid and CAJ involvement are frequent, through the conus elasticus.
- –
- Infraglottic extension >10 mm, evaluated exactly at the free edge of the TVC midline, with progression toward the posterior commissure.
- –
- It tends to minimally extend upwards toward the SPGS.
- 4)
- Transglottic and infraglottic carcinoma with massive involvement of the CAU and of the posterior crico-arytenoid muscle, reaching the hypopharyngeal submucosa (Figure 5):
- –
- The tumor massively infiltrates the SPGS and IPGS, the thyro-arytenoid space and/or posterior crico-thyroid space, it blocks the arytenoid laterally corresponding to the lateral crico-arytenoid muscle, extending downwards medially into the infraglottic site and puncturing the conus elasticus.
- –
- Infraglottic extension >10 mm, evaluated exactly at the free edge of the TVC midline, with progression toward the posterior commissure.
- –
- The tumor invades the arytenoid and, very often, the cricoid, involving the posterior crico-arytenoid and the interarytenoid musculature, reaching the hypopharyngeal submucosa.
- –
- Possible involvement of the contralateral CAU.
2.4. Pathologic Assessment
2.5. Treatments
2.6. Adjuvant Treatments
2.7. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kirchner, J.A.; Som, M.L. Clinical significance of fixed vocal cord. Laryngoscope 1971, 81, 1029–1044. [Google Scholar] [CrossRef]
- Kirchner, J.A. Pathways and Pitfalls in Partial Laryngectomy. Ann. Otol. Rhinol. Laryngol. 1984, 93, 301–305. [Google Scholar] [CrossRef]
- Brasnu, D.; Laccourreye, H.; Dulmet, E.; Jaubert, F. Mobility of the vocal cord and arytenoid in squamous cell carcinoma of the larynx and hypopharynx: An anatomical and clinical comparative study. Ear Nose Throat J. 1990, 69, 324–330. [Google Scholar] [PubMed]
- Katilmiş, H.; Oztürkcan, S.; Ozdemir, I.; Adadan, I.; Tunç, A.; Akder, A.; Başoğlu, S. A clinico-pathological study of laryngeal and hypopharyngeal carcinoma: Correlation of cord-arytenoid mobility with histopathologic involvement. Otolaryngol. Head Neck Surg. 2007, 136, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Prades, J.M.; Dumollard, J.M.; Timoshenko, A.P.; Durand, M.; Martin, C. Descriptive anatomy of the cricoarytenoid articulation: Application to articular dynamics in carcinology. Surg. Radiol. Anat. 2000, 22, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Leroux-Robert, J. La chirurgie conservative dans le cancer du larynx. Ann. Oto-Laryngol. 1957, 74, 40–74. [Google Scholar]
- Olofsson, J.; Lord, I.J.; van Nostrand, A.W. Vocal cord fixation in laryngeal carcinoma. Acta Otolaryngol. 1973, 75, 496–510. [Google Scholar] [CrossRef]
- Kirchner, J.A.; Carter, D. Intralaryngeal barriers to the spread of cancer. Acta Otolaryngol. 1987, 103, 503–513. [Google Scholar]
- Hirano, M.; Kurita, S.; Matsuoka, H.; Tateishi, M. Vocal fold fixation in laryngeal carcinomas. Acta Otolaryngol. 1991, 111, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Som, M.L. Cordal cancer with extension to vocal process. Laryngoscope 1975, 85, 1298–1307. [Google Scholar] [CrossRef]
- Kirchner, J.A. What Have Whole Organ Sections Contributed to the Treatment of Laryngeal Cancer? Ann. Otol. Rhinol. Laryngol. 1989, 98, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Sparano, A.; Chernock, R.; Feldman, M.; Laccourreye, O.; Brasnu, D.; Weinstein, G. Extending the inferior limits of supracricoid partial laryngectomy: A clinicopathological correlation. Laryngoscope 2005, 115, 297–300. [Google Scholar] [CrossRef]
- Succo, G.; Crosetti, E.; Bertolin, A.; Piazza, C.; Molteni, G.; Cirillo, S.; Petracchini, M.; Tascone, M.; Sprio, A.E.; Berta, G.N.; et al. Treatment of T3 to T4a laryngeal cancer by open partial horizontal laryngectomies: Prognostic impact of different pT subcategories. Head Neck 2018, 40, 1897–1908. [Google Scholar] [CrossRef] [PubMed]
- Alterio, D.; Bacigalupo, A.; Cantù, G.; Cerrotta, A.; De Sanctis, V.; Grandi, C.; Gatta, G.; Calareso, G.; Locati, L.; Presutti, L.; et al. Linee Guida—Tumori della testa e del collo, 2016 ed.; Aiom: Milan, Italy, 2016; pp. 57–79. [Google Scholar]
- Karnofsky, D.; Burchenal, J. The Clinical Evaluation of Chemoterapeutic Agents in Cancer; Columbia University Press: New York, NY, USA, 1949; pp. 191–205. [Google Scholar]
- Nakayama, M.; Holsinger, C.; Okamoto, M.; Seino, Y.; Miyamoto, S.; Takeda, M.; Yokobori, S.; Masaki, T.; Hayashi, S. Clinicopathological analyses of fifty supracricoid laryngectomized specimens: Evidence base supporting minimal margins. ORL J. Otorhinolaryngol. Relat. Spec. 2009, 71, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Succo, G.; Peretti, G.; Piazza, C.; Remacle, M.; Eckel, H.E.; Chevalier, D.; Simo, R.; Hantzakos, A.G.; Rizzotto, G.; Lucioni, M.; et al. Open partial horizontal laryngectomies: A proposal for classification by the working committee on nomenclature of the European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2014, 271, 2489–2496. [Google Scholar] [CrossRef]
- Robbins, K.T.; Clayman, G.; Levine, P.A.; Medina, J.; Sessions, R.; Shaha, A.; Som, P.; Wolf, G.T. Neck dissection classification update: Revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef]
- Ang, K.K. Larynx Preservation Clinical Trial Design: Summary of Key Recommendations of a Consensus Panel. Oncologist 2010, 15 (Suppl. 3), 25–29. [Google Scholar] [CrossRef] [Green Version]
- Succo, G.; Crosetti, E.; Bertolin, A.; Lucioni, M.; Arrigoni, G.; Panetta, V.; Sprio, A.E.; Berta, G.N.; Rizzotto, G. Benefits and drawbacks of open partial horizontal laryngectomies, Part B: Intermediate and selected advanced stage laryngeal carcinoma. Head Neck 2016, 38 (Suppl. 1), E649–E657. [Google Scholar] [CrossRef]
- Succo, G.; Crosetti, E.; Bertolin, A.; Lucioni, M.; Caracciolo, A.; Panetta, V.; Sprio, A.E.; Berta, G.N.; Rizzotto, G. Benefits and drawbacks of open partial horizontal laryngectomies, Part A: Early- to intermediate-stage glottic carcinoma. Head Neck 2016, 38, E333–E340. [Google Scholar] [CrossRef]
- Rizzotto, G.; Succo, G.; Lucioni, M.; Pazzaia, T. Subtotal laryngectomy with tracheohyoidopexy: A possible alternative to total laryngectomy. Laryngoscope 2006, 116, 1907–1917. [Google Scholar] [CrossRef] [PubMed]
- Laccourreye, O.; Salzer, S.J.; Brasnu, D.; Shen, W.; Laccourreye, H.; Weinstein, G.S. Glottic carcinoma with a fixed true vocal cord: Outcomes after neoadjuvant chemotherapy and supracricoid partial laryngectomy with cricohyoidoepiglottopexy. Otolaryngol. Head Neck Surg. 1996, 114, 400–406. [Google Scholar] [CrossRef]
- Maroldi, R.; Ravanelli, M.; Farina, D. Magnetic resonance for laryngeal cancer. Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Biller, H.F.; Lawson, W. Partial laryngectomy for vocal cord cancer with marked limitation or fixation of the vocal cord. Laryngoscope 1986, 96, 61–64. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | N of Patients (%) | ||
|---|---|---|---|
| Age | Mean ± standard deviation | 65.4 ± 9.4 | |
| Range | 50–90 | ||
| Gender | Male | 23 (79.3%) | |
| Female | 6 (20.7%) | ||
| Karnofsky | 100 | 24 (82.8%) | |
| 90 | 1 (3.4%) | ||
| 80 | 4 (13.8%) | ||
| Arytenoid mobility | Fixed | 29 (100%) | |
| cTN | Glottic | Supraglottic | |
| cT3 | N0 | 8 (27.6%) | 2 (6.9%) |
| N1 | 2 (6.9%) | 0 (0.0%) | |
| N2 | 0 (0.0%) | 0 (0.0%) | |
| cT4a | N0 | 8 (27.6%) | 1(3.5%) |
| N1 | 2 (6.9%) | 2 (6.9%) | |
| N2 | 4 (13.8%) | 0 (0.0%) | |
| Total | 24 (82.8%) | 5 (17.2%) | |
| Type of Treatment | Pattern 1 (N = 3) | Pattern 2 (N = 5) | Pattern 3 (N = 17) | Pattern 4 (N = 4) | Total | |
|---|---|---|---|---|---|---|
| TL | 1 (33.3%) | 0 (0.0%) | 14 (82.4%) | 3 (75.0%) | 18 (62.0%) | |
| OPHL | IIa + ARY, n (%) | 0 (0.0%) | 3 (60.0%) | 0 (0.0%) | 0 (0.0%) | 3 (10.3%) |
| IIb + ARY, n (%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| IIIa + CAU, n (%) | 0 (0.0%) | 1 (20.0%) | 3 (17.6%) | 1 * (25.0%) | 5 (17.2%) | |
| IIIb + CAU, n (%) | 0 (0.0%) | 1 (20.0%) | 0 (0.0%) | 0 (0.0%) | 1 (3.5%) | |
| IC + RT | 2 (66.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (7.0%) | |
| Invaded Structures | Pattern 2 (N = 5) | Pattern 3 (N = 17) | Pattern 4 (N = 4) | |||
|---|---|---|---|---|---|---|
| Imaging | Pathology | Imaging | Pathology | Imaging | Pathology | |
| SPGS | 3 | 2 | 17 | 13 | 3 | 2 |
| IPGS | 5 | 5 | 17 | 17 | 4 | 4 |
| ARY | 4 | 4 | 16 | 13 | 4 | 4 |
| CAJ | 2 | 2 | 12 | 13 | 4 | 4 |
| Cricoid plate | 0 | 0 | 4 | 2 | 3 | 1 |
| Subglottic extension >10mm | 0 | 1 | 17 | 14 | 4 | 3 |
| Contralateral CAU | 0 | 0 | 0 | 0 | 1 | 1 |
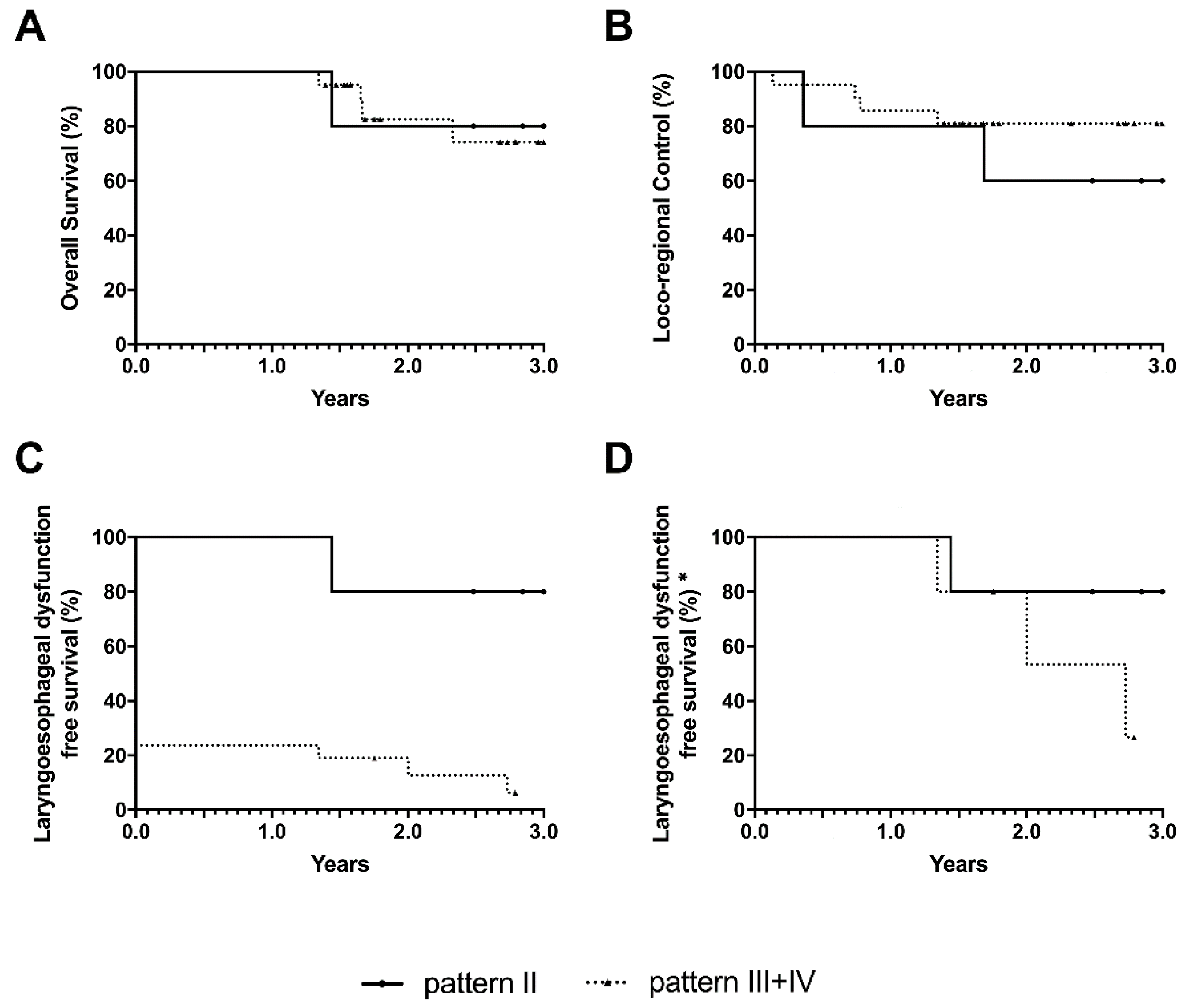
| End point | Pattern | |||
|---|---|---|---|---|
| 2 | 3 | 4 | 3 + 4 | |
| OS | 80.0% | 75.2% | 75.0% | 74.3% |
| LRC | 60.0% | 88.2% | 50.0% | 81.0% |
| LEDFS | 80.0% | 33.3% | 0.0% | 6.3% |
| LEDFS * | 80.0% | 33.3% | 0.0% | 26.7% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Succo, G.; Cirillo, S.; Bertotto, I.; Maldi, E.; Balmativola, D.; Petracchini, M.; Gned, D.; Fornari, A.; Motatto, G.M.; Sprio, A.E.; et al. Arytenoid Fixation in Laryngeal Cancer: Radiological Pictures and Clinical Correlations with Respect to Conservative Treatments. Cancers 2019, 11, 360. https://doi.org/10.3390/cancers11030360
Succo G, Cirillo S, Bertotto I, Maldi E, Balmativola D, Petracchini M, Gned D, Fornari A, Motatto GM, Sprio AE, et al. Arytenoid Fixation in Laryngeal Cancer: Radiological Pictures and Clinical Correlations with Respect to Conservative Treatments. Cancers. 2019; 11(3):360. https://doi.org/10.3390/cancers11030360
Chicago/Turabian StyleSucco, Giovanni, Stefano Cirillo, Ilaria Bertotto, Elena Maldi, Davide Balmativola, Massimo Petracchini, Dario Gned, Alessandro Fornari, Gian Marco Motatto, Andrea E. Sprio, and et al. 2019. "Arytenoid Fixation in Laryngeal Cancer: Radiological Pictures and Clinical Correlations with Respect to Conservative Treatments" Cancers 11, no. 3: 360. https://doi.org/10.3390/cancers11030360