Clinical Routine TERT Promoter Mutational Screening of Follicular Thyroid Tumors of Uncertain Malignant Potential (FT-UMPs): A Useful Predictor of Metastatic Disease

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics and TERT Promoter Mutational Status of the Study Cohort
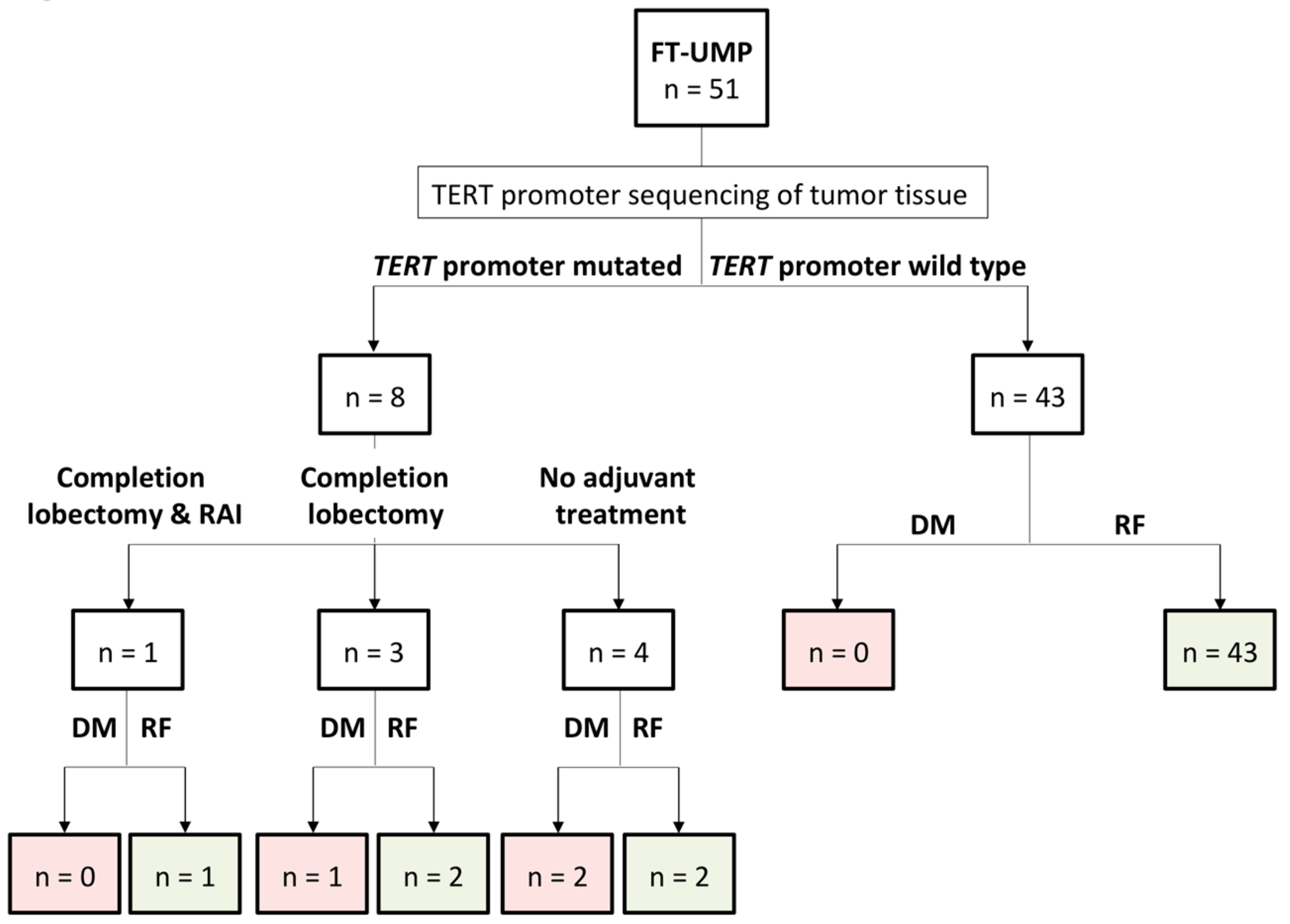
2.2. Individual Treatments for the FT-UMPs
2.3. Clinical Outcome in TERT-Promoter-Mutated FT-UMP
2.4. Correlation to Clinicopathological Parameters in TERT-Promoter-Mutated FT-UMPs
3. Discussion
4. Materials and Methods
4.1. Tumor Cohorts
4.2. Histopathological Criteria
4.3. TERT Promoter Mutation Analysis
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization classification of tumours, 4th ed.; Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J.; Weltgesundheitsorganisation; International Agency for Research on Cancer (Eds.) International Agency for Research on Cancer: Lyon, France, 2017; ISBN 978-92-832-4493-6. [Google Scholar]
- Duggal, R.; Rajwanshi, A.; Gupta, N.; Vasishta, R.K. Interobserver variability amongst cytopathologists and histopathologists in the diagnosis of neoplastic follicular patterned lesions of thyroid. Diagn. Cytopathol. 2011, 39, 235–241. [Google Scholar] [CrossRef]
- Glomski, K.; Nosé, V.; Faquin, W.C.; Sadow, P.M. Metastatic Follicular Thyroid Carcinoma and the Primary Thyroid Gross Examination: Institutional Review of Cases from 1990 to 2015. Endocr. Pathol. 2017, 28, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Hysek, M.; Paulsson, J.O.; Wang, N.; Jatta, K.; Lindh, C.; Fuentes-Martinez, N.; Shabo, I.; Zedenius, J.; Juhlin, C.C. TERT promoter mutational screening as a tool to predict malignant behaviour in follicular thyroid tumours-three examples from the clinical routine. Virchows Arch. 2018, 473, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Wojtas, B.; Pfeifer, A.; Oczko-Wojciechowska, M.; Krajewska, J.; Czarniecka, A.; Kukulska, A.; Eszlinger, M.; Musholt, T.; Stokowy, T.; Swierniak, M.; et al. Gene Expression (mRNA) Markers for Differentiating between Malignant and Benign Follicular Thyroid Tumours. Int. J. Mol. Sci. 2017, 18, 1184. [Google Scholar] [CrossRef] [PubMed]
- Dettmer, M.; Vogetseder, A.; Durso, M.B.; Moch, H.; Komminoth, P.; Perren, A.; Nikiforov, Y.E.; Nikiforova, M.N. MicroRNA expression array identifies novel diagnostic markers for conventional and oncocytic follicular thyroid carcinomas. J. Clin. Endocrinol. Metab. 2013, 98, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Jacques, C.; Guillotin, D.; Fontaine, J.-F.; Franc, B.; Mirebeau-Prunier, D.; Fleury, A.; Malthiery, Y.; Savagner, F. DNA microarray and miRNA analyses reinforce the classification of follicular thyroid tumors. J. Clin. Endocrinol. Metab. 2013, 98, E981–E989. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Aguilar, J.; Clifton-Bligh, R.; Molloy, M.P. Proteomics of thyroid tumours provides new insights into their molecular composition and changes associated with malignancy. Sci. Rep. 2016, 6, 23660. [Google Scholar] [CrossRef]
- Nicolson, N.G.; Murtha, T.D.; Dong, W.; Paulsson, J.O.; Choi, J.; Barbieri, A.L.; Brown, T.C.; Kunstman, J.W.; Larsson, C.; Prasad, M.L.; et al. Comprehensive Genetic Analysis of Follicular Thyroid Carcinoma Predicts Prognosis Independent of Histology. J. Clin. Endocrinol. Metab. 2018, 103, 2640–2650. [Google Scholar] [CrossRef] [Green Version]
- Calabrese, G.; Dolcimascolo, A.; Torrisi, F.; Zappalà, A.; Gulino, R.; Parenti, R. MiR-19a Overexpression in FTC-133 Cell Line Induces a More De-Differentiated and Aggressive Phenotype. Int. J. Mol. Sci. 2018, 19, E3944. [Google Scholar] [CrossRef]
- Horn, S.; Figl, A.; Rachakonda, P.S.; Fischer, C.; Sucker, A.; Gast, A.; Kadel, S.; Moll, I.; Nagore, E.; Hemminki, K.; et al. TERT promoter mutations in familial and sporadic melanoma. Science 2013, 339, 959–961. [Google Scholar] [CrossRef]
- Huang, F.W.; Hodis, E.; Xu, M.J.; Kryukov, G.V.; Chin, L.; Garraway, L.A. Highly recurrent TERT promoter mutations in human melanoma. Science 2013, 339, 957–959. [Google Scholar] [CrossRef]
- Akincilar, S.C.; Unal, B.; Tergaonkar, V. Reactivation of telomerase in cancer. Cell. Mol. Life Sci. 2016, 73, 1659–1670. [Google Scholar] [CrossRef] [Green Version]
- Colebatch, A.J.; Dobrovic, A.; Cooper, W.A. TERT gene: Its function and dysregulation in cancer. J. Clin. Pathol. 2019, 72, 281–284. [Google Scholar] [CrossRef]
- Liu, X.; Bishop, J.; Shan, Y.; Pai, S.; Liu, D.; Murugan, A.K.; Sun, H.; El-Naggar, A.K.; Xing, M. Highly prevalent TERT promoter mutations in aggressive thyroid cancers. Endocr. Relat. Cancer 2013, 20, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Qu, S.; Liu, R.; Sheng, C.; Shi, X.; Zhu, G.; Murugan, A.K.; Guan, H.; Yu, H.; Wang, Y.; et al. TERT promoter mutations and their association with BRAF V600E mutation and aggressive clinicopathological characteristics of thyroid cancer. J. Clin. Endocrinol. Metab. 2014, 99, E1130–E1136. [Google Scholar] [CrossRef]
- Liu, R.; Xing, M. Diagnostic and prognostic TERT promoter mutations in thyroid fine-needle aspiration biopsy. Endocr. Relat. Cancer 2014, 21, 825–830. [Google Scholar] [CrossRef] [Green Version]
- Melo, M.; da Rocha, A.G.; Vinagre, J.; Batista, R.; Peixoto, J.; Tavares, C.; Celestino, R.; Almeida, A.; Salgado, C.; Eloy, C.; et al. TERT promoter mutations are a major indicator of poor outcome in differentiated thyroid carcinomas. J. Clin. Endocrinol. Metab. 2014, 99, E754–E765. [Google Scholar] [CrossRef]
- Paulsson, J.O.; Mu, N.; Shabo, I.; Wang, N.; Zedenius, J.; Larsson, C.; Juhlin, C.C. TERT aberrancies: A screening tool for malignancy in follicular thyroid tumours. Endocr. Relat. Cancer 2018, 25, 723–733. [Google Scholar] [CrossRef]
- Bournaud, C.; Descotes, F.; Decaussin-Petrucci, M.; Berthiller, J.; de la Fouchardière, C.; Giraudet, A.-L.; Bertholon-Gregoire, M.; Robinson, P.; Lifante, J.-C.; Lopez, J.; et al. TERT promoter mutations identify a high-risk group in metastasis-free advanced thyroid carcinoma. Eur. J. Cancer 2019, 108, 41–49. [Google Scholar] [CrossRef]
- Jin, A.; Xu, J.; Wang, Y. The role of TERT promoter mutations in postoperative and preoperative diagnosis and prognosis in thyroid cancer. Medicine 2018, 97, e11548. [Google Scholar] [CrossRef]
- Oishi, N.; Kondo, T.; Ebina, A.; Sato, Y.; Akaishi, J.; Hino, R.; Yamamoto, N.; Mochizuki, K.; Nakazawa, T.; Yokomichi, H.; et al. Molecular alterations of coexisting thyroid papillary carcinoma and anaplastic carcinoma: Identification of TERT mutation as an independent risk factor for transformation. Mod. Pathol. 2017, 30, 1527–1537. [Google Scholar] [CrossRef]
- Liu, T.; Wang, N.; Cao, J.; Sofiadis, A.; Dinets, A.; Zedenius, J.; Larsson, C.; Xu, D. The age- and shorter telomere-dependent TERT promoter mutation in follicular thyroid cell-derived carcinomas. Oncogene 2014, 33, 4978–4984. [Google Scholar] [CrossRef]
- Pathology and Genetics of Tumours of Endocrine Organs; DeLellis, R.A. (Ed.) World Health Organization classification of tumours; IARC Press: Lyon, France, 2004; ISBN 978-92-832-2416-7. [Google Scholar]
- Wang, N.; Liu, T.; Sofiadis, A.; Juhlin, C.C.; Zedenius, J.; Höög, A.; Larsson, C.; Xu, D. TERT promoter mutation as an early genetic event activating telomerase in follicular thyroid adenoma (FTA) and atypical FTA. Cancer 2014, 120, 2965–2979. [Google Scholar] [CrossRef]
- Juhlin, C.C. A Clinical Overview of Telomerase-Associated Aberrancies in Follicular Thyroid Tumors as Diagnostic and Prognostic Markers: Tert Alert! Scand. J. Surg. 2019, 1457496919850434. [Google Scholar] [CrossRef]
- Steward, D.L.; Carty, S.E.; Sippel, R.S.; Yang, S.P.; Sosa, J.A.; Sipos, J.A.; Figge, J.J.; Mandel, S.; Haugen, B.R.; Burman, K.D.; et al. Performance of a Multigene Genomic Classifier in Thyroid Nodules With Indeterminate Cytology: A Prospective Blinded Multicenter Study. JAMA Oncol. 2018. [Google Scholar] [CrossRef]
- Duan, H.; Liu, X.; Ren, X.; Zhang, H.; Wu, H.; Liang, Z. Mutation profiles of follicular thyroid tumors by targeted sequencing. Diagn. Pathol. 2019, 14, 39. [Google Scholar] [CrossRef]
- Juhlin, C.C.; Bränström, R.; Shabo, I.; Höög, A. Clear Cell Variant of a Follicular Thyroid Tumor with Uncertain Malignant Potential: A Case Report. Int. J. Surg. Pathol. 2018, 1066896918809490. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | FT-UMP (n = 51) | miFTC (n = 40) | ||
|---|---|---|---|---|
| Observation | Informative Cases | Observation | Informative Cases | |
| Mean age at diagnosis, years | 52 | 51 | 53 | 40 |
| Female patients, n | 39 | 51 | 28 | 40 |
| Mean tumor diameter, mm | 37 | 50 | 37 | 38 |
| T category *, n | 40 | |||
| pT1 | n/a | 12 | ||
| pT2 | n/a | 15 | ||
| pT3 | n/a | 13 | ||
| pT4 | n/a | 0 | ||
| Extrathyroidal growth, n | n/a | 1 | 40 | |
| Mean follow-up time, months | 26 | 49 | 135 | 40 |
| Outcome, n | 49 | 40 | ||
| Metastatic disease/recurrence | 3 | 4 | ||
| Disease-free | 46 | 36 | ||
| TERT promoter mutated, n | 8 | 51 | 7 | 40 |
| Case No. | Age at Diagnosis | Gender | Type of Surgery | RAI Treatment | Tumor Diameter (mm) | Ki-67 Index | TERTp Mutation | Follow-Up Time (months) | Alive | Metastatic Disease | Site of Metastasis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 71 | F | HT | No | 50 | 7% | C250T | 59 | Yes | No | |
| 2 | 75 | F | HT + CL | No | 70 | 6% | C228T | 37 | Yes | Yes | Bone |
| 3 | 33 | M | HT + CL | No | 50 | 8% | C228T | 49 | Yes | No | |
| 4 | 71 | F | HT + CL | No | 18 | 5% | C228T | 22 | Yes | No | |
| 5 | 75 | F | HT + CL | Yes | 100 | 9% | C228T | 15 | Yes | No | |
| 6 | 56 | M | HT | No | 40 | 5% | C228T | 76 | Yes | Yes | Bone |
| 7 | 79 | M | HT | No | No data | 5% | C228T | 19 | Yes | Yes | Bone, lungs |
| 8 | 58 | F | HT | No | 50 | 4% | C228T | 1 | Yes | No |
| Parameter | TERTp-Mutated FT-UMP (n = 8) | TERTp wt FT-UMP (n = 43) | p-Value |
|---|---|---|---|
| Observation | Observation | ||
| Mean age at diagnosis (years) | 65 | 50 | p = 0.016 |
| Age ≥55 years | 7 | 17 | p = 0.019 |
| Female patients | 5 | 34 | p = 0.372 |
| Mean tumor diameter (mm) | 54 | 34 | p = 0.045 |
| Equivocal capsular invasion # | 8 | 38 | p = 0.580 |
| Equivocal vascular invasion # | 3 | 3 | p = 0.042 |
| Hypercellularity * | 6 | 25 | p = 0.456 |
| Mitotic figures (≥1 per 10 HPFs) | 1 | 6 | p = 1.000 |
| Degenerative changes | 3 | 7 | p = 0.179 |
| Mean Ki-67 index (%) | 6% | 6% | p = 0.468 |
| Outcome | |||
| Metastatic disease/recurrence | 3 | 0 | p = 0.003 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hysek, M.; Paulsson, J.O.; Jatta, K.; Shabo, I.; Stenman, A.; Höög, A.; Larsson, C.; Zedenius, J.; Juhlin, C.C. Clinical Routine TERT Promoter Mutational Screening of Follicular Thyroid Tumors of Uncertain Malignant Potential (FT-UMPs): A Useful Predictor of Metastatic Disease. Cancers 2019, 11, 1443. https://doi.org/10.3390/cancers11101443
Hysek M, Paulsson JO, Jatta K, Shabo I, Stenman A, Höög A, Larsson C, Zedenius J, Juhlin CC. Clinical Routine TERT Promoter Mutational Screening of Follicular Thyroid Tumors of Uncertain Malignant Potential (FT-UMPs): A Useful Predictor of Metastatic Disease. Cancers. 2019; 11(10):1443. https://doi.org/10.3390/cancers11101443
Chicago/Turabian StyleHysek, Martin, Johan O. Paulsson, Kenbugul Jatta, Ivan Shabo, Adam Stenman, Anders Höög, Catharina Larsson, Jan Zedenius, and Carl Christofer Juhlin. 2019. "Clinical Routine TERT Promoter Mutational Screening of Follicular Thyroid Tumors of Uncertain Malignant Potential (FT-UMPs): A Useful Predictor of Metastatic Disease" Cancers 11, no. 10: 1443. https://doi.org/10.3390/cancers11101443