Liquid Biopsy Testing Can Improve Selection of Advanced Non-Small-Cell Lung Cancer Patients to Rechallenge with Gefitinib

 ,
, 
 , , ,
, , , 
Abstract
:1. Introduction
2. Results
2.1. Patients
2.2. Serum Analysis for EGFR Mutations
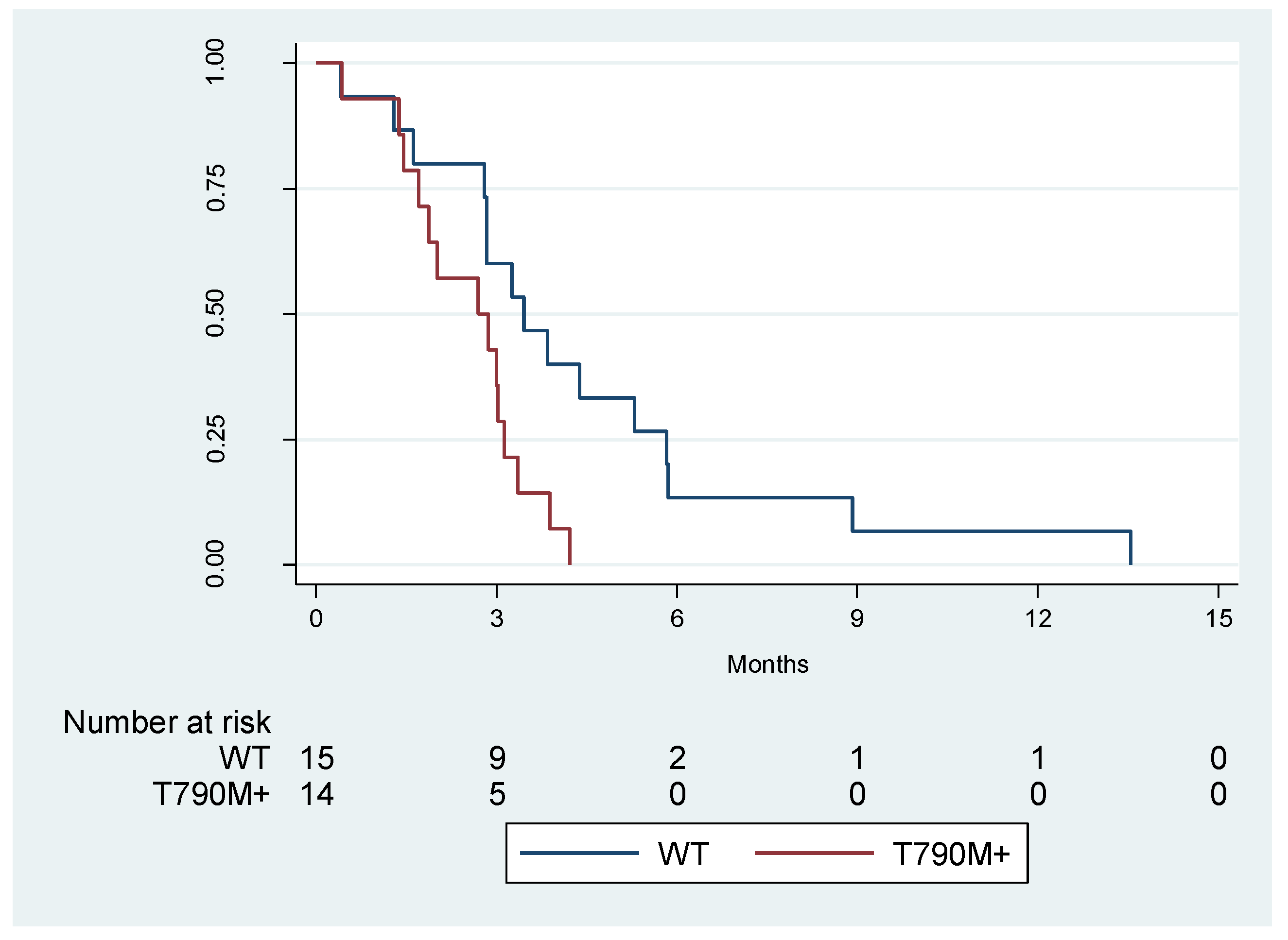
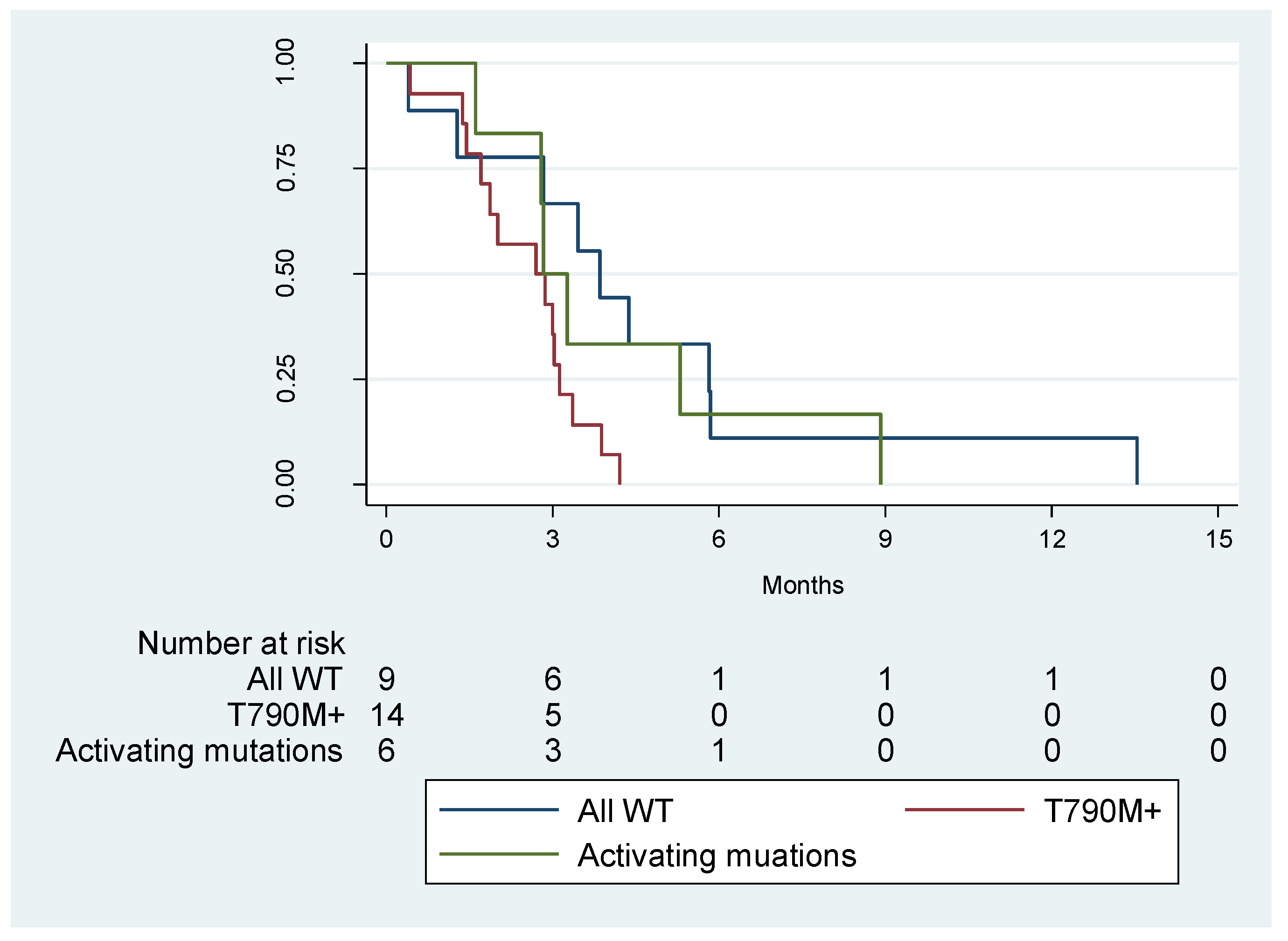
2.3. PFS Analysis According to EGFR p.T790M Status in cfDNA
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Population
4.2. Serum-Derived cfDNA
4.3. Therascreen Plasma EGFR RGQ PCR Kit
4.4. Droplet Digital PCR Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- Schrank, Z.; Chhabra, G.; Lin, L.; Iderzorig, T.; Osude, C.; Khan, N.; Kuckovic, A.; Singh, S.; Miller, R.J.; Puri, N. Current Molecular-Targeted Therapies in NSCLC and Their Mechanism of Resistance. Cancers 2018, 10, 224. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Naci, H.; Gurpinar, E.; Poplavska, E.; Pinto, A.; Aggarwal, A. Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: Retrospective cohort study of drug approvals 2009–13. BMJ 2017, 359, j4530. [Google Scholar] [CrossRef] [PubMed]
- Vyse, S.; Huang, P.H. Targeting EGFR exon 20 insertion mutations in non-small cell lung cancer. Signal Transduct. Target Ther. 2019, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Ke, E.E.; Wu, Y.L. EGFR as a Pharmacological Target in EGFR-Mutant Non-Small-Cell Lung Cancer: Where Do We Stand Now? Trends Pharmacol. Sci. 2016, 37, 887–903. [Google Scholar] [CrossRef] [PubMed]
- Fenizia, F.; De Luca, A.; Pasquale, R.; Sacco, A.; Forgione, L.; Lambiase, M.; Iannaccone, A.; Chicchinelli, N.; Franco, R.; Rossi, A.; et al. EGFR mutations in lung cancer: From tissue testing to liquid biopsy. Future Oncol. 2015, 11, 1611–1623. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.K.; Kim, S.W.; Wu, Y.L.; Nakagawa, K.; Yang, J.J.; Ahn, M.J.; Wang, J.; Yang, J.C.; Lu, Y.; Atagi, S.; et al. Gefitinib Plus Chemotherapy Versus Chemotherapy in Epidermal Growth Factor Receptor Mutation-Positive Non-Small-Cell Lung Cancer Resistant to First-Line Gefitinib (IMPRESS): Overall Survival and Biomarker Analyses. J. Clin. Oncol. 2017, 35, 4027–4034. [Google Scholar] [CrossRef]
- Cappuzzo, F.; Morabito, A.; Normanno, N.; Bidoli, P.; Del Conte, A.; Giannetta, L.; Montanino, A.; Mazzoni, F.; Buosi, R.; Burgio, M.A.; et al. Efficacy and safety of rechallenge treatment with gefitinib in patients with advanced non-small cell lung cancer. Lung Cancer 2016, 99, 31–37. [Google Scholar] [CrossRef]
- Sequist, L.V.; Waltman, B.A.; Dias-Santagata, D.; Digumarthy, S.; Turke, A.B.; Fidias, P.; Bergethon, K.; Shaw, A.T.; Gettinger, S.; Cosper, A.K.; et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci. Transl. Med. 2011, 3, 75ra26. [Google Scholar] [CrossRef]
- Kuiper, J.L.; Heideman, D.A.; Wurdinger, T.; Grunberg, K.; Groen, H.J.; Smit, E.F. Rationale and study design of the IRENE-trial (NVALT-16): A phase II trial to evaluate iressa rechallenge in advanced NSCLC patients with an activating EGFR mutation who responded to an EGFR-TKI used as first-line or previous treatment. Clin. Lung Cancer 2015, 16, 60–66. [Google Scholar] [CrossRef]
- Asahina, H.; Oizumi, S.; Inoue, A.; Kinoshita, I.; Ishida, T.; Fujita, Y.; Sukoh, N.; Harada, M.; Maemondo, M.; Saijo, Y.; et al. Phase II study of gefitinib readministration in patients with advanced non-small cell lung cancer and previous response to gefitinib. Oncology 2010, 79, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, T.; Agatsuma, T.; Ikegami, K.; Suzuki, T.; Kobayashi, T.; Kanda, S.; Yoshikawa, S.; Kubo, K.; Shiina, T.; Takasuna, K.; et al. Prospective study of gefitinib readministration after chemotherapy in patients with advanced non-small-cell lung cancer who previously responded to gefitinib. Clin. Lung Cancer 2012, 13, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Esposito Abate, R.; Pasquale, R.; Fenizia, F.; Rachiglio, A.M.; Roma, C.; Bergantino, F.; Forgione, L.; Lambiase, M.; Sacco, A.; Piccirillo, M.C.; et al. The role of circulating free DNA in the management of NSCLC. Expert Rev. Anticancer Ther. 2019, 19, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Normanno, N.; Denis, M.G.; Thress, K.S.; Ratcliffe, M.; Reck, M. Guide to detecting epidermal growth factor receptor (EGFR) mutations in ctDNA of patients with advanced non-small-cell lung cancer. Oncotarget 2017, 8, 12501–12516. [Google Scholar] [CrossRef] [PubMed]
- Oxnard, G.R.; Thress, K.S.; Alden, R.S.; Lawrance, R.; Paweletz, C.P.; Cantarini, M.; Yang, J.C.; Barrett, J.C.; Janne, P.A. Association Between Plasma Genotyping and Outcomes of Treatment With Osimertinib (AZD9291) in Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 3375–3382. [Google Scholar] [CrossRef]
- Zhang, Q.; Ke, E.; Niu, F.; Deng, W.; Chen, Z.; Xu, C.; Zhang, X.; Zhao, N.; Su, J.; Yang, J.; et al. The role of T790M mutation in EGFR-TKI re-challenge for patients with EGFR-mutant advanced lung adenocarcinoma. Oncotarget 2017, 8, 4994–5002. [Google Scholar] [CrossRef] [PubMed]
- Normanno, N.; Fenizia, F.; Castiglione, F.; Barberis, M.; Taddei, G.L.; Truini, M.; De Rosa, G.; Pinto, C.; Marchetti, A. External quality assessment for EGFR mutations in Italy: Improvements in performances over the time. ESMO Open 2017, 2, e000160. [Google Scholar] [CrossRef] [PubMed]
- Normanno, N.; Maiello, M.R.; Chicchinelli, N.; Iannaccone, A.; Esposito, C.; De Cecio, R.; D’Alessio, A.; De Luca, A. Targeting the EGFR T790M mutation in non-small-cell lung cancer. Expert Opin. Ther. Targets 2017, 21, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Hata, A.; Katakami, N.; Yoshioka, H.; Takeshita, J.; Tanaka, K.; Nanjo, S.; Fujita, S.; Kaji, R.; Imai, Y.; Monden, K.; et al. Rebiopsy of non-small cell lung cancer patients with acquired resistance to epidermal growth factor receptor-tyrosine kinase inhibitor: Comparison between T790M mutation-positive and mutation-negative populations. Cancer 2013, 119, 4325–4332. [Google Scholar] [CrossRef]
- Santoni-Rugiu, E.; Melchior, L.C.; Urbanska, E.M.; Jakobsen, J.N.; Stricker, K.; Grauslund, M.; Sorensen, J.B. Intrinsic resistance to EGFR-Tyrosine Kinase Inhibitors in EGFR-Mutant Non-Small Cell Lung Cancer: Differences and Similarities with Acquired Resistance. Cancers 2019, 11, 923. [Google Scholar] [CrossRef]
- Gaut, D.; Sim, M.S.; Yue, Y.; Wolf, B.R.; Abarca, P.A.; Carroll, J.M.; Goldman, J.W.; Garon, E.B. Clinical Implications of the T790M Mutation in Disease Characteristics and Treatment Response in Patients With Epidermal Growth Factor Receptor (EGFR)-Mutated Non-Small-Cell Lung Cancer (NSCLC). Clin. Lung Cancer 2018, 19, e19–e28. [Google Scholar] [CrossRef] [PubMed]
- Rachiglio, A.M.; Esposito Abate, R.; Sacco, A.; Pasquale, R.; Fenizia, F.; Lambiase, M.; Morabito, A.; Montanino, A.; Rocco, G.; Romano, C.; et al. Limits and potential of targeted sequencing analysis of liquid biopsy in patients with lung and colon carcinoma. Oncotarget 2016, 7, 66595–66605. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics | N = 61 | N = 29 | |||
|---|---|---|---|---|---|
| Gender | Male | 16 | (26.2%) | 9 | (30.1%) |
| Female | 45 | (73.8%) | 20 | (69.9%) | |
| Age | Mean | 67 years | 68 years | ||
| Range | 40–86 years | 40–86 years | |||
| WHO-PS | 0 | 20 | (32.8%) | 11 | (37.9%) |
| 1 | 30 | (49.2%) | 11 | (37.9%) | |
| 2 | 10 | (16.4%) | 6 | (22.6% | |
| n.a. | 1 | (1.6%) | 1 | (1.6%) | |
| Stage at study entry | IIIB | 2 | (3.3%) | 2 | (6.9%) |
| IV | 59 | (96.7%) | 27 | (93.1%) | |
| Smoking status | Never | 41 | (67.2%) | 18 | (62%) |
| Current | 3 | (4.9%) | 2 | (6.9%) | |
| Former | 16 | (26.2%) | 8 | (27.6%) | |
| Missing | 1 | (1.6%) | 1 | (3.5%) | |
| Chemotherapy response | CR | 1 | (1.6%) | 0 | (0%) |
| PR | 13 | (21.3%) | 10 | (34.5%) | |
| SD | 26 | (42.6%) | 10 | (34.5%) | |
| PD | 21 | (34.3%) | 9 | (21%) | |
| Tumor EGFR Mutational Status at Baseline, n | Serum-Derived cfDNA EGFR Mutational Status at Enrolment in the ICARUS Trial, n | ||||
|---|---|---|---|---|---|
| Therascreen | droplet digital PCR (ddPCR) | ||||
| Positive | Negative | Positive | Negative | ||
| p.L858R | 13 | 6 | 7 | 9 | 4 |
| Del Exon 19 | 16 | 7 | 9 | 11 | 5 |
| p.T790M | - | 2 | 27 | 14 | 15 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esposito Abate, R.; Pasquale, R.; Sacco, A.; Piccirillo, M.C.; Morabito, A.; Bidoli, P.; Finocchiaro, G.; Chiari, R.; Foltran, L.; Buosi, R.; et al. Liquid Biopsy Testing Can Improve Selection of Advanced Non-Small-Cell Lung Cancer Patients to Rechallenge with Gefitinib. Cancers 2019, 11, 1431. https://doi.org/10.3390/cancers11101431
Esposito Abate R, Pasquale R, Sacco A, Piccirillo MC, Morabito A, Bidoli P, Finocchiaro G, Chiari R, Foltran L, Buosi R, et al. Liquid Biopsy Testing Can Improve Selection of Advanced Non-Small-Cell Lung Cancer Patients to Rechallenge with Gefitinib. Cancers. 2019; 11(10):1431. https://doi.org/10.3390/cancers11101431
Chicago/Turabian StyleEsposito Abate, Riziero, Raffaella Pasquale, Alessandra Sacco, Maria Carmela Piccirillo, Alessandro Morabito, Paolo Bidoli, Giovanna Finocchiaro, Rita Chiari, Luisa Foltran, Roberta Buosi, and et al. 2019. "Liquid Biopsy Testing Can Improve Selection of Advanced Non-Small-Cell Lung Cancer Patients to Rechallenge with Gefitinib" Cancers 11, no. 10: 1431. https://doi.org/10.3390/cancers11101431
APA StyleEsposito Abate, R., Pasquale, R., Sacco, A., Piccirillo, M. C., Morabito, A., Bidoli, P., Finocchiaro, G., Chiari, R., Foltran, L., Buosi, R., Tiseo, M., Giannetta, L., Battiloro, C., Fasola, G., Romano, G., Ciuffreda, L., Frassoldati, A., de Marinis, F., Cappuzzo, F., & Normanno, N. (2019). Liquid Biopsy Testing Can Improve Selection of Advanced Non-Small-Cell Lung Cancer Patients to Rechallenge with Gefitinib. Cancers, 11(10), 1431. https://doi.org/10.3390/cancers11101431