Therapy Landscape in Patients with Metastatic HER2-Positive Breast Cancer: Data from the PRAEGNANT Real-World Breast Cancer Registry

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. The PRAEGNANT Research Network
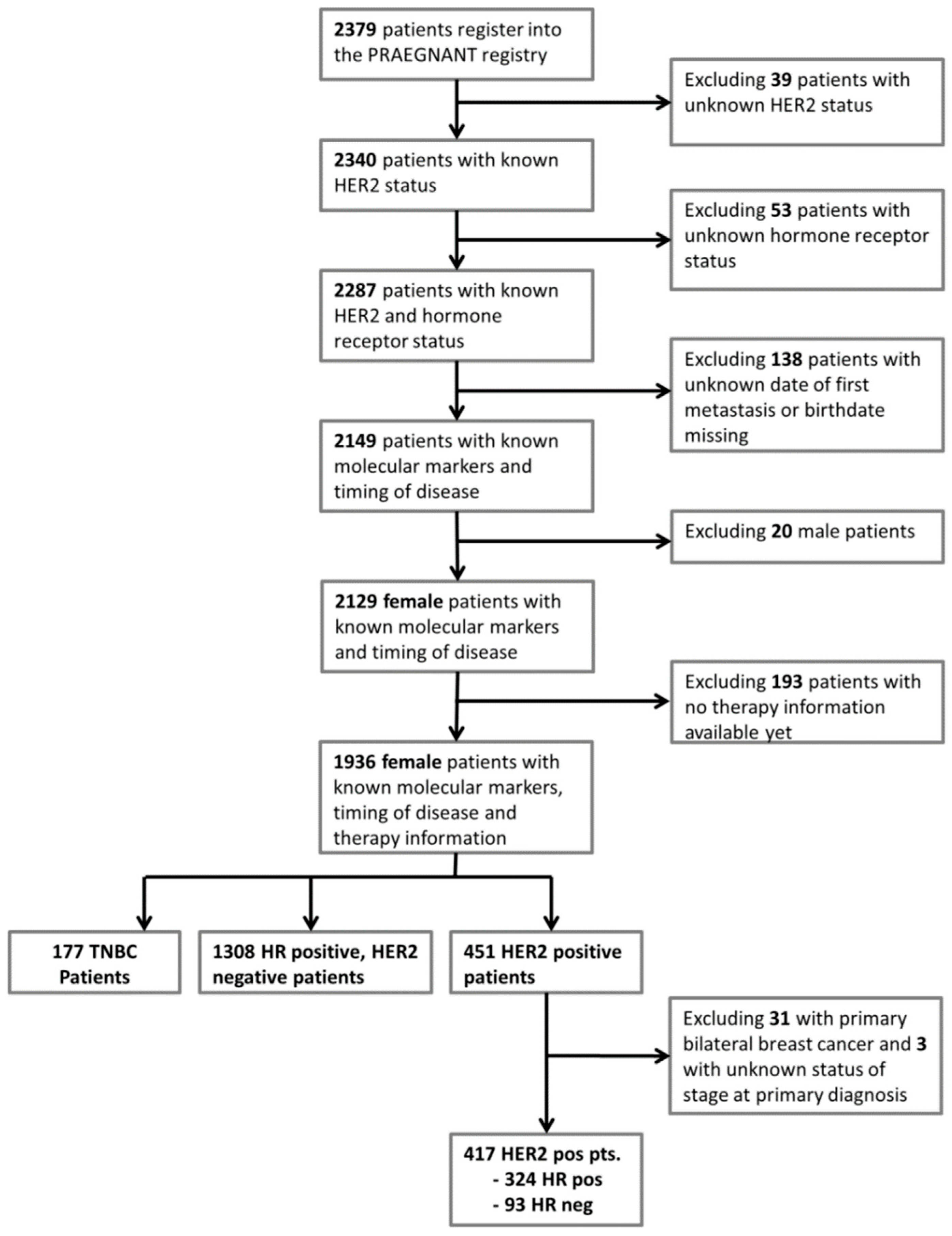
2.2. Patients
2.3. Data Collection
2.4. Definition of Hormone Receptors, HER2 Status and Grading
2.5. Statistical Considerations
3. Results
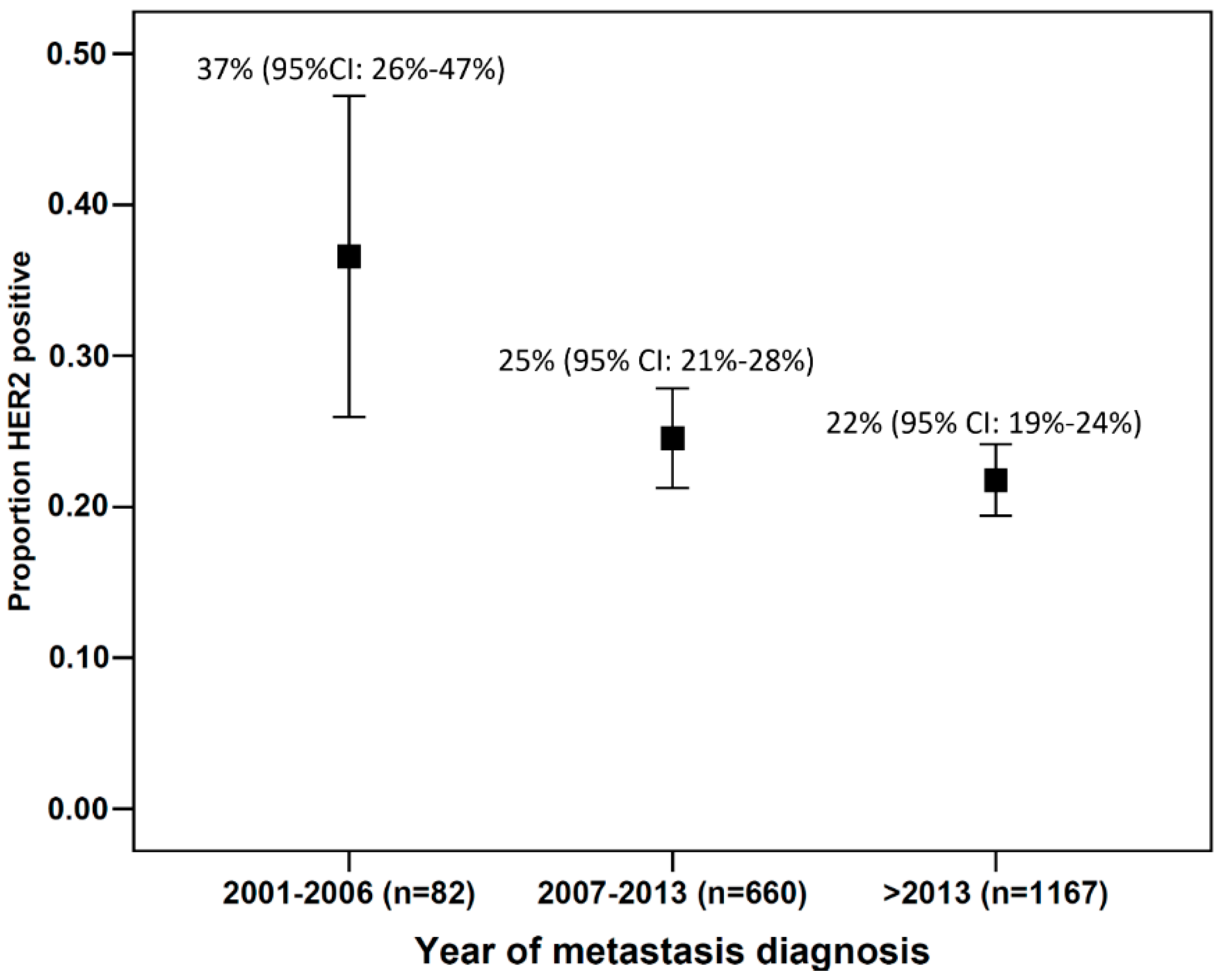
3.1. Patient and Disease Characteristics
3.2. Therapies
3.3. Predictors of the Use of a Therapy Sequence of PH Followed by T-DM1
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, A.; Lux, M.P.; Janni, W.; Hartkopf, A.D.; Nabieva, N.; Taran, F.A.; Overkamp, F.; Kolberg, H.C.; Hadji, P.; Tesch, H.; et al. Update Breast Cancer 2018 (Part 2)—Advanced Breast Cancer, Quality of Life and Prevention. Geburtshilfe Frauenheilkd 2018, 78, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Taran, F.A.; Schneeweiss, A.; Lux, M.P.; Janni, W.; Hartkopf, A.D.; Nabieva, N.; Overkamp, F.; Kolberg, H.C.; Hadji, P.; Tesch, H.; et al. Update Breast Cancer 2018 (Part 1)—Primary Breast Cancer and Biomarkers. Geburtshilfe Frauenheilkd 2018, 78, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Lux, M.P.; Janni, W.; Hartkopf, A.D.; Nabieva, N.; Taran, F.A.; Overkamp, F.; Kolberg, H.C.; Hadji, P.; Tesch, H.; Ettl, J.; et al. Update Breast Cancer 2017—Implementation of Novel Therapies. Geburtshilfe Frauenheilkd 2017, 77, 1281–1290. [Google Scholar] [CrossRef] [PubMed]
- Untch, M.; Huober, J.; Jackisch, C.; Schneeweiss, A.; Brucker, S.Y.; Dall, P.; Denkert, C.; Fasching, P.A.; Fehm, T.; Gerber, B.; et al. Initial Treatment of Patients with Primary Breast Cancer: Evidence, Controversies, Consensus: Spectrum of Opinion of German Specialists at the 15th International St. Gallen Breast Cancer Conference (Vienna 2017). Geburtshilfe Frauenheilkd 2017, 77, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef]
- Geyer, C.E.; Forster, J.; Lindquist, D.; Chan, S.; Romieu, C.G.; Pienkowski, T.; Jagiello-Gruszfeld, A.; Crown, J.; Chan, A.; Kaufman, B.; et al. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N. Engl. J. Med. 2006, 355, 2733–2743. [Google Scholar] [CrossRef]
- Cameron, D.; Casey, M.; Press, M.; Lindquist, D.; Pienkowski, T.; Romieu, C.G.; Chan, S.; Jagiello-Gruszfeld, A.; Kaufman, B.; Crown, J.; et al. A phase III randomized comparison of lapatinib plus capecitabine versus capecitabine alone in women with advanced breast cancer that has progressed on trastuzumab: Updated efficacy and biomarker analyses. Breast Cancer Res. Treat. 2008, 112, 533–543. [Google Scholar] [CrossRef]
- Swain, S.M.; Kim, S.B.; Cortés, J.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.M.; Schneeweiss, A.; Knott, A.; et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA study): Overall survival results from a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. 2013, 14, 461–471. [Google Scholar] [CrossRef]
- Swain, S.M.; Baselga, J.; Kim, S.B.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.M.; Schneeweiss, A.; Heeson, S.; et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N. Engl. J. Med. 2015, 372, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Barrios, C.; Eiermann, W.; Toi, M.; Im, Y.H.; Conte, P.; Martin, M.; Pienkowski, T.; Pivot, X.; Burris, H., III; et al. Trastuzumab Emtansine With or Without Pertuzumab Versus Trastuzumab Plus Taxane for Human Epidermal Growth Factor Receptor 2-Positive, Advanced Breast Cancer: Primary Results From the Phase III MARIANNE Study. J. Clin. Oncol. 2017, 35, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Gianni, L. HER2-positive breast cancer. Lancet 2017, 389, 2415–2429. [Google Scholar] [CrossRef]
- Deeks, E.D. Neratinib: First Global Approval. Drugs 2017, 77, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Huang, C.S.; Hurvitz, S.; Yeh, D.C.; Shao, Z.; Im, S.A.; Jung, K.H.; Shen, K.; Ro, J.; Jassem, J.; et al. Afatinib plus vinorelbine versus trastuzumab plus vinorelbine in patients with HER2-overexpressing metastatic breast cancer who had progressed on one previous trastuzumab treatment (LUX-Breast 1): An open-label, randomised, phase 3 trial. Lancet Oncol. 2016, 17, 357–366. [Google Scholar] [CrossRef]
- Bang, Y.J.; Giaccone, G.; Im, S.A.; Oh, D.Y.; Bauer, T.M.; Nordstrom, J.L.; Li, H.; Chichili, G.R.; Moore, P.A.; Hong, S.; et al. First-in-human phase 1 study of margetuximab (MGAH22), an Fc-modified chimeric monoclonal antibody, in patients with HER2-positive advanced solid tumors. Ann. Oncol. 2017, 28, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Fasching, P.A.; Brucker, S.Y.; Fehm, T.N.; Overkamp, F.; Janni, W.; Wallwiener, M.; Hadji, P.; Belleville, E.; Häberle, L.; Taran, F.A.; et al. Biomarkers in Patients with Metastatic Breast Cancer and the PRAEGNANT Study Network. Geburtshilfe Frauenheilkd 2015, 75, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Hartkopf, A.D.; Huober, J.; Volz, B.; Nabieva, N.; Taran, F.A.; Schwitulla, J.; Overkamp, F.; Kolberg, H.C.; Hadji, P.; Tesch, H.; et al. Treatment landscape of advanced breast cancer patients with hormone receptor positive HER2 negative tumors - Data from the German PRAEGNANT breast cancer registry. Breast 2018, 37, 42–51. [Google Scholar] [CrossRef]
- Müller, V.; Nabieva, N.; Häberle, L.; Taran, F.A.; Hartkopf, A.D.; Volz, B.; Overkamp, F.; Brandl, A.L.; Kolberg, H.C.; Hadji, P.; et al. Impact of disease progression on health-related quality of life in patients with metastatic breast cancer in the PRAEGNANT breast cancer registry. Breast 2018, 37, 154–160. [Google Scholar] [CrossRef]
- Hein, A.; Gass, P.; Walter, C.B.; Taran, F.A.; Hartkopf, A.; Overkamp, F.; Kolberg, H.C.; Hadji, P.; Tesch, H.; Ettl, J.; et al. Computerized patient identification for the EMBRACA clinical trial using real-time data from the PRAEGNANT network for metastatic breast cancer patients. Breast Cancer Res. Treat. 2016, 158, 59–65. [Google Scholar] [CrossRef]
- Slamon, D.J.; Godolphin, W.; Jones, L.A.; Holt, J.A.; Wong, S.G.; Keith, D.E.; Levin, W.J.; Stuart, S.G.; Udove, J.; Ullrich, A.; et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science 1989, 244, 707–712. [Google Scholar] [CrossRef]
- Perez, E.A.; Romond, E.H.; Suman, V.J.; Jeong, J.H.; Sledge, G.; Geyer, C.E., Jr.; Martino, S.; Rastogi, P.; Gralow, J.; Swain, S.M.; et al. Trastuzumab plus adjuvant chemotherapy for human epidermal growth factor receptor 2-positive breast cancer: Planned joint analysis of overall survival from NSABP B-31 and NCCTG N9831. J. Clin. Oncol. 2014, 32, 3744–3752. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [PubMed]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef]
- AGO Commission Breast. Diagnosis and Therapy of patients with primary and metastatic breast cancer. Available online: http://www.ago-online.de/fileadmin/downloads/leitlinien/mamma/2017-03/AGO_deutsch/PDF_Gesamtdatei_deutsch/Alle%20aktuellen%20Empfehlungen_2017.pdf (accessed on 20 March 2017).
- Vici, P.; Pizzuti, L.; Michelotti, A.; Sperduti, I.; Natoli, C.; Mentuccia, L.; Di Lauro, L.; Sergi, D.; Marchetti, P.; Santini, D.; et al. A retrospective multicentric observational study of trastuzumab emtansine in HER2 positive metastatic breast cancer: A real-world experience. Oncotarget 2017, 8, 56921–56931. [Google Scholar] [CrossRef]
- Pobiruchin, M.; Bochum, S.; Martens, U.M.; Schramm, W. Clinical Cancer Registries—Are They Up for Health Services Research? Stud. Health Technol. Inform. 2016, 228, 242–246. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristic | n or Mean | % or SD |
|---|---|---|
| Age at study entry | 57.9 | 13.0 |
| BMI | 26.0 | 5.3 |
| Time from diagnosis to metastasis (days) | 1177.8 | 1743.0 |
| Therapy situation at study entry | ||
| First-line | 223 | 53.5 |
| Second-line | 70 | 16.8 |
| Third-line | 53 | 12.7 |
| Fourth-line | 26 | 6.2 |
| Fifth-line and higher | 34 | 8.2 |
| Therapy situation at database closure | ||
| First-line | 171 | 41.0 |
| Second-line | 82 | 19.7 |
| Third-line | 47 | 11.3 |
| Fourth-line | 17 | 4.1 |
| Fifth-line and higher | 59 | 14.1 |
| Hormone receptor status | ||
| Negative | 93 | 22.3 |
| Positive | 324 | 77.7 |
| ECOG | ||
| 0 | 196 | 47.0 |
| 1 | 155 | 37.2 |
| 2 | 35 | 8.4 |
| 3 | 12 | 2.9 |
| 4 | 2 | 0. 4 |
| Metastasis site at study entry | ||
| Brain a | 79 | 18.9 |
| Visceral b | 222 | 53.2 |
| Bone only | 58 | 13.9 |
| Other c | 50 | 12.0 |
| Metastatic at time of diagnosis | ||
| No | 244 | 58.5 |
| Yes | 173 | 41.5 |
| Therapy | Patients Treated Before 2012 | Patients Treated Crossing 2013 | Patients Treated After 2013 | |||
|---|---|---|---|---|---|---|
| Not Treated | Treated | Not Treated | Treated | Not Treated | Treated | |
| Trastuzumab (H) | ||||||
| treatments in patient group 1 a | 4 (19) | 17 (80.9) | 0 (0) | 6 (100) | 28 (20.4) | 109 (79.5) |
| treatments in patient group 2 b | 0 (0) | 6 (100) | 2 (13.3) | 13 (86.6) | 11 (15) | 62 (84.9) |
| treatments in patient group 3 c | 0 (0) | 4 (100) | 3 (15.7) | 16 (84.2) | 6 (15.3) | 33 (84.6) |
| treatments in patient group 4 d | 3 (20) | 12 (80) | 8 (18.1) | 36 (81.8) | 7 (18.4) | 31 (81.5) |
| Trastuzumab + pertuzumab (PH) | ||||||
| treatments in patient group 1 a | 19 (90.4) | 2 (9.5) | 3 (50) | 3 (50) | 51 (37.2) | 86 (62.7) |
| treatments in patient group 2 b | 6 (100) | 0 (0) | 11 (73.3) | 4 (26.6) | 21 (28.7) | 52 (71.2) |
| treatments in patient group 3 c | 4 (100) | 0 (0) | 13 (68.4) | 6 (31.5) | 12 (30.7) | 27 (69.2) |
| treatments in patient group 4 d | 15 (100) | 0 (0) | 28 (63.6) | 16 (36.3) | 14 (36.8) | 24 (63.1) |
| Lapatinib (L) | ||||||
| treatments in patient group 1 a | 20 (95.2) | 1 (4.7) | 5 (83.3) | 1 (16.6) | 134 (97.8) | 3 (2.1) |
| treatments in patient group 2 b | 6 (100) | 0 (0) | 12 (80) | 3 (20) | 65 (89) | 8 (10.9) |
| treatments in patient group 3 c | 3 (75) | 1 (25) | 15 (78.9) | 4 (21) | 30 (76.9) | 9 (23) |
| treatments in patient group 4 d | 8 (53.3) | 7 (46.6) | 22 (50) | 22 (50) | 18 (47.3) | 20 (52.6) |
| Trastuzumab emtansine (T-DM1) | ||||||
| treatments in patient group 1 a | 21 (100) | 0 (0) | 6 (100) | 0 (0) | 131 (95.6) | 6 (4.3) |
| treatments in patient group 2 b | 6 (100) | 0 (0) | 10 (66.6) | 5 (33.3) | 49 (67.1) | 24 (32.8) |
| treatments in patient group 3 c | 4 (100) | 0 (0) | 8 (42.1) | 11 (57.8) | 21 (53.8) | 18 (46.1) |
| treatments in patient group 4 d | 14 (93.3) | 1 (6.6) | 21 (47.7) | 23 (52.2) | 18 (47.3) | 20 (52.6) |
| Therapy | Patients Treated Before 2012 | Patients Treated Crossing 2012 | Patients Treated After 2012 | |||
|---|---|---|---|---|---|---|
| Not Treated | Treated | Not Treated | Treated | Not Treated | Treated | |
| Pertuzumab/trastuzumab → trastuzumab emtansine (PH → T-DM1) | ||||||
| treatments in patient group 1 a | 21 (100) | 0 (0) | 6 (100) | 0 (0) | 137 (100) | 0 (0) |
| treatments in patient group 2 b | 6 (100) | 0 (0) | 14 (93.3) | 1 (6.6) | 59 (80.8) | 14 (19.1) |
| treatments in patient group 3 c | 4 (100) | 0 (0) | 17 (89.4) | 2 (10.5) | 27 (69.2) | 12 (30.7) |
| treatments in patient group 4 d | 15 (100) | 0 (0) | 39 (88.6) | 5 (11.3) | 22 (57.8) | 16 (42.1) |
| Trastuzumab emtansine → pertuzumab/trastuzumab (T-DM1 → PH) | ||||||
| treatments in patient group 1 a | 21 (100) | 0 (0) | 6 (100) | 0 (0) | 136 (99.2) | 1 (0.7) |
| treatments in patient group 2 b | 6 (100) | 0 (0) | 15 (100) | 0 (0) | 73 (100) | 0 (0) |
| treatments in patient group 3 c | 4 (100) | 0 (0) | 18 (94.7) | 1 (5.2) | 38 (97.4) | 1 (2.5) |
| treatments in patient group 4 d | 15 (100) | 0 (0) | 41 (93.1) | 3 (6.8) | 36 (94.7) | 2 (5.2) |
| Characteristic | PH → T-DM1 | |
|---|---|---|
| No | Yes | |
| Age | ||
| <50 | 28 (65.1) | 15 (34.9) |
| 50–65 | 53 (72.6) | 20 (27.4) |
| >65 | 27 (79.4) | 7 (20.6) |
| Eastern Cooperative Oncology Group (ECOG) score | ||
| 0 | 59 (79.7) | 15 (20.3) |
| 1 | 34 (63.0) | 20 (37.0) |
| 2 | 6 (60.0) | 4 (40.0) |
| 3 | 5 (100) | 0 (0) |
| Metastasis site at study entry | ||
| Brain a | 14 (58.3) | 10 (41.7) |
| Visceral b | 56 (68.3) | 23 (31.7) |
| Bone only c | 16 (94.1) | 1 (5.9) |
| Other d | 19 (82.6) | 4 (14.7) |
| Hormone receptor status | ||
| Negative | 18 (56.3) | 14 (43.8) |
| Positive | 90 (76.3) | 28 (23.7) |
| Grade | ||
| 1 | 2 (100) | 0 (0) |
| 2 | 45 (78.9) | 12 (21.1) |
| 3 | 50 (64.1) | 28 (35.9) |
| Primary metastatic | ||
| No | 68 (73.9) | 24 (26.1) |
| Yes | 40 (69.0) | 42 (28.0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lux, M.P.; Nabieva, N.; Hartkopf, A.D.; Huober, J.; Volz, B.; Taran, F.-A.; Overkamp, F.; Kolberg, H.-C.; Hadji, P.; Tesch, H.; et al. Therapy Landscape in Patients with Metastatic HER2-Positive Breast Cancer: Data from the PRAEGNANT Real-World Breast Cancer Registry. Cancers 2019, 11, 10. https://doi.org/10.3390/cancers11010010
Lux MP, Nabieva N, Hartkopf AD, Huober J, Volz B, Taran F-A, Overkamp F, Kolberg H-C, Hadji P, Tesch H, et al. Therapy Landscape in Patients with Metastatic HER2-Positive Breast Cancer: Data from the PRAEGNANT Real-World Breast Cancer Registry. Cancers. 2019; 11(1):10. https://doi.org/10.3390/cancers11010010
Chicago/Turabian StyleLux, Michael P., Naiba Nabieva, Andreas D. Hartkopf, Jens Huober, Bernhard Volz, Florin-Andrei Taran, Friedrich Overkamp, Hans-Christian Kolberg, Peyman Hadji, Hans Tesch, and et al. 2019. "Therapy Landscape in Patients with Metastatic HER2-Positive Breast Cancer: Data from the PRAEGNANT Real-World Breast Cancer Registry" Cancers 11, no. 1: 10. https://doi.org/10.3390/cancers11010010