A Systematic Review and Meta-Analysis Comparing Liver Resection with the Rf-Based Device Habib™-4X with the Clamp-Crush Technique

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
2.5. Surgical Technique
3. Results
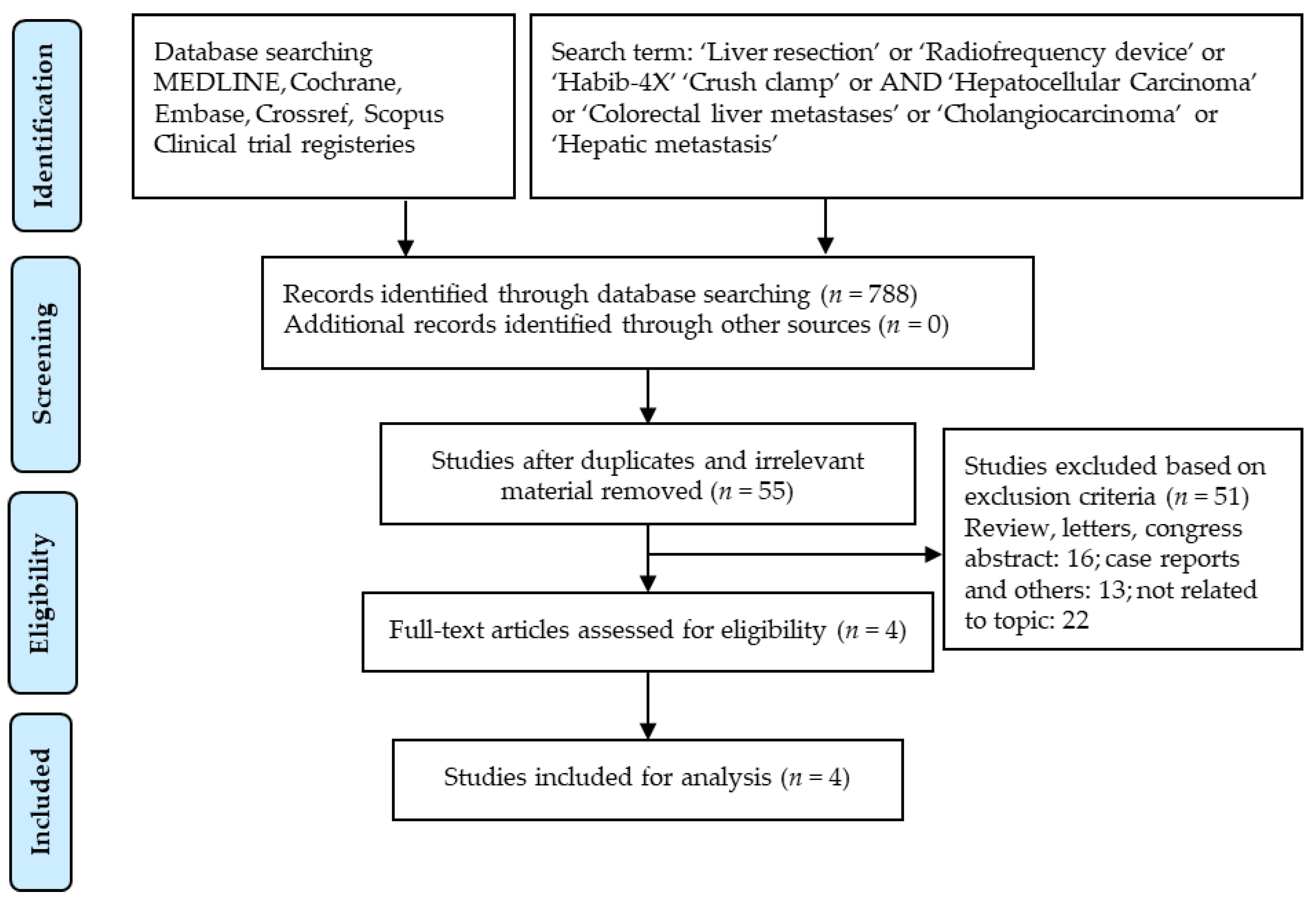
3.1. Search Results
3.2. Blood Loss and Quantity of Blood Transfused
3.3. Operative Time
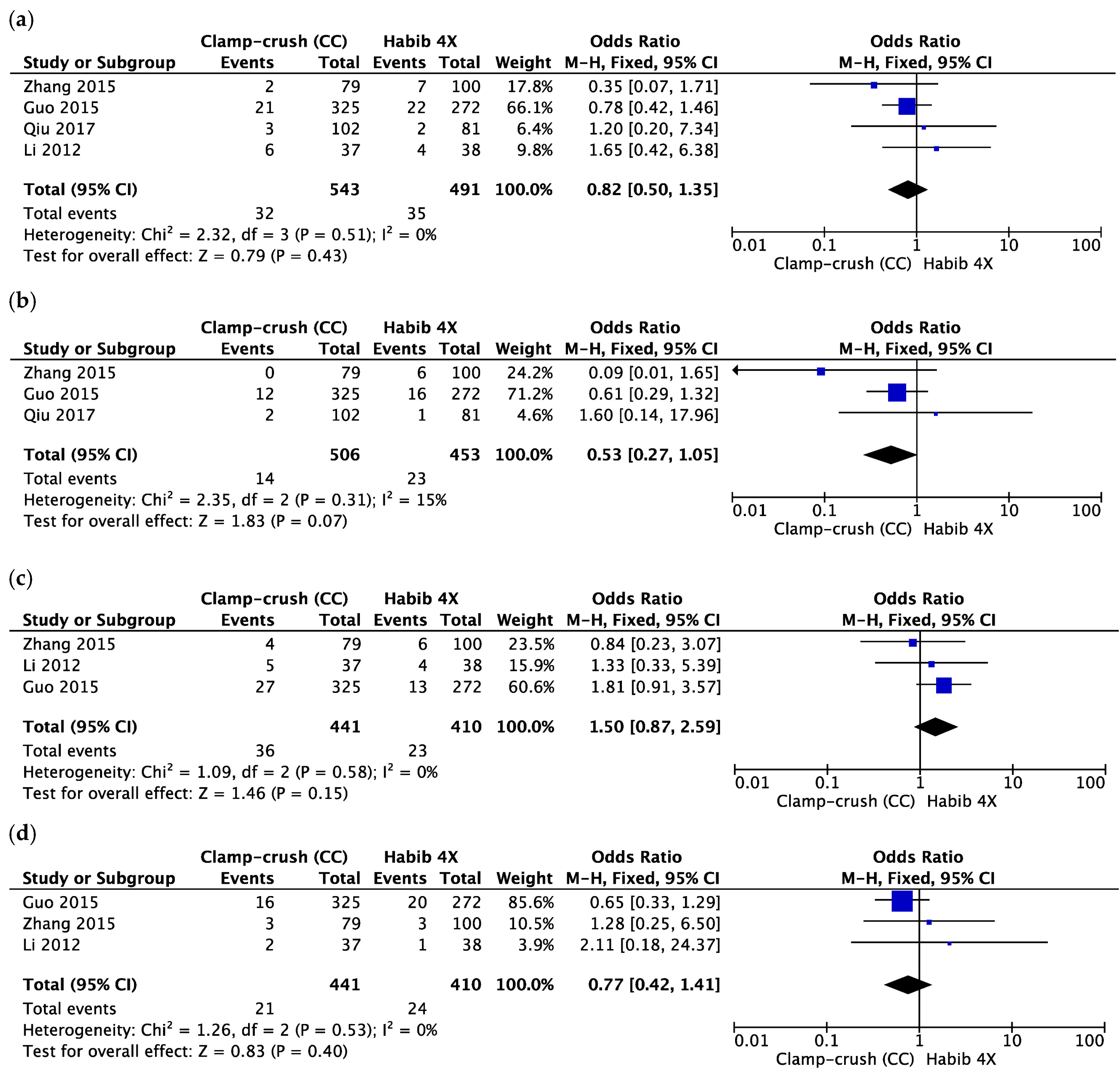
3.4. Serious Adverse Events
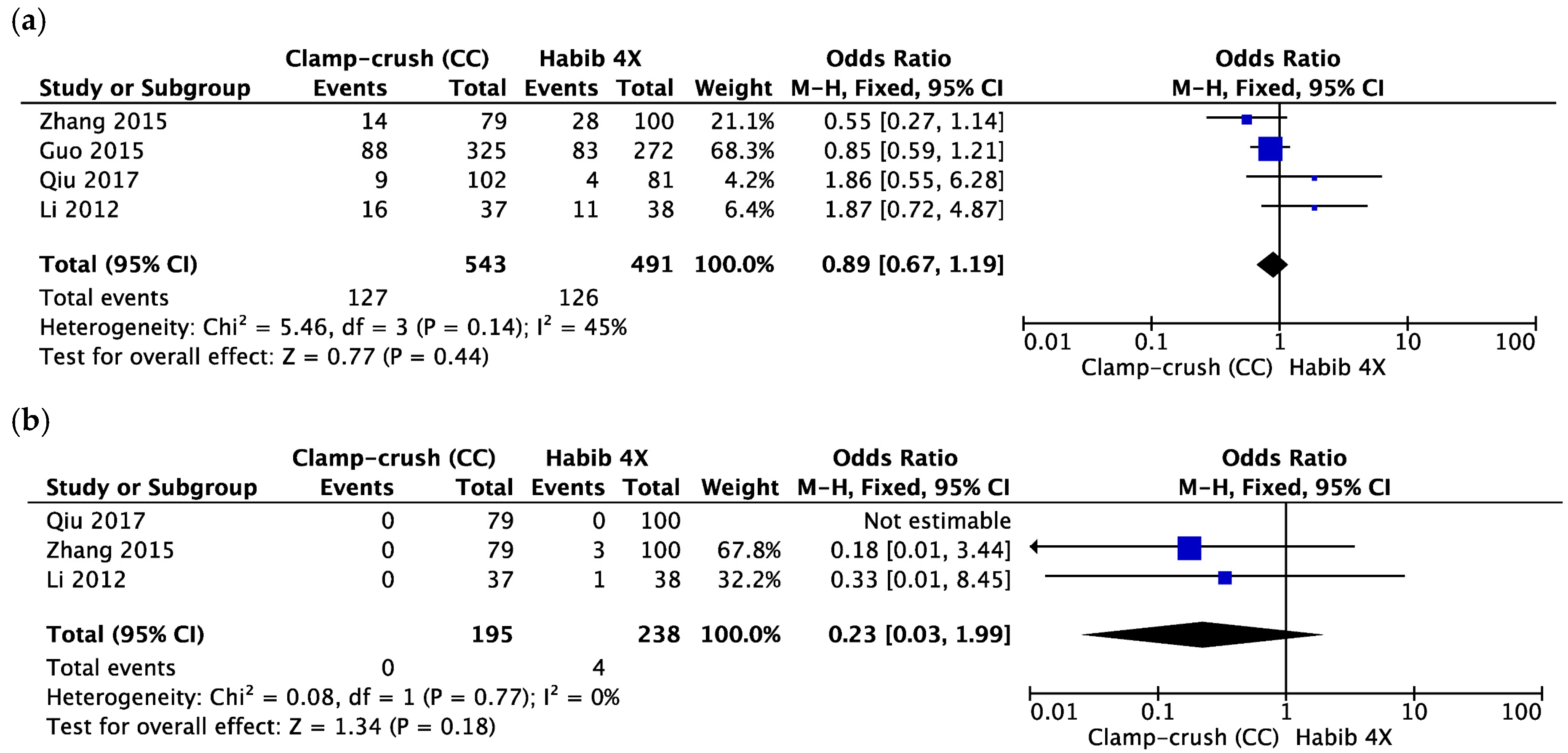
3.5. Length of Hospital Stay, Total Morbidity and 30-Day Mortality
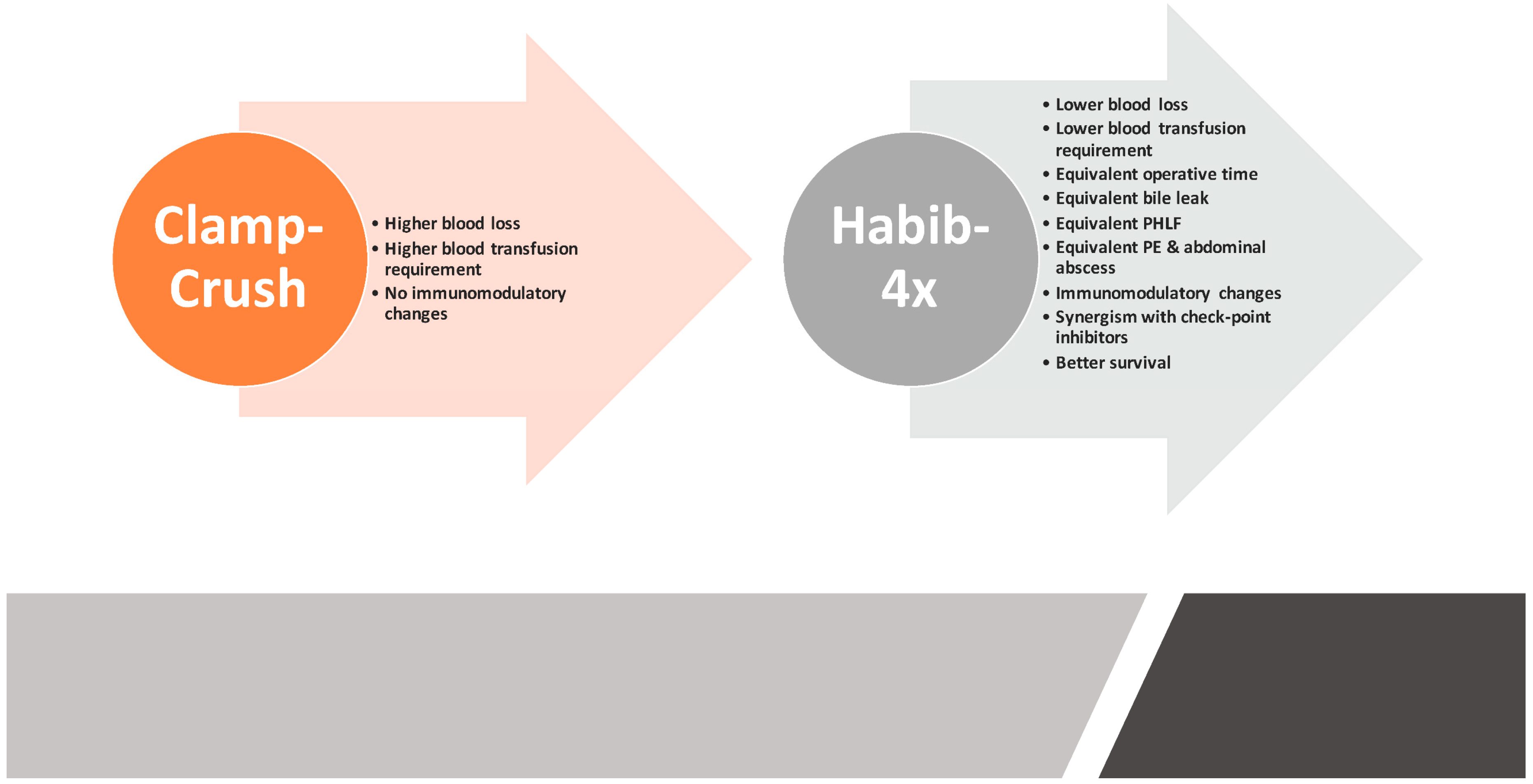
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Hughes, M.J.; Wigmore, S.J. Principles of liver surgery. Surgery 2014, 32, 643–647. [Google Scholar] [CrossRef]
- Ladurner, R.; Königsrainer, A. Liver surgery: What is feasible? ZBL CHIR 2007, 132, 274–280. [Google Scholar] [PubMed]
- Aragon, R.J.; Solomon, N.L. Techniques of hepatic resection. J. Gastrointest. Oncol. 2012, 3, 28–40. [Google Scholar] [PubMed]
- Celinski, S.A.; Gamblin, T.C. Hepatic Resection Nomenclature and Techniques. Surg. Clin. N. Am. 2010, 90, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Reissfelder, C.; Rahbari, N.N.; Koch, M.; Kofler, B.; Sutedja, N.; Elbers, H.; Büchler, M.W.; Weitz, J. Postoperative course and clinical significance of biochemical blood tests following hepatic resection. Br. J. Surg. 2011, 98, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Delis, S.G.; Bakoyiannis, A.; Tassopoulos, N.; Athanassiou, K.; Kechagias, A.; Kelekis, D.; Madariaga, J.; Dervenis, C. Hepatic resection for large hepatocellular carcinoma in the era of UCSF criteria. HPB 2009, 11, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, P.; Primrose, J.; Colquitt, J.; Garden, O.; Poston, G.; Rees, M. Surgical resection of hepatic metastases from colorectal cancer: A systematic review of published studies. Br. J. Cancer 2006, 94, 982–999. [Google Scholar] [CrossRef] [PubMed]
- Khatri, V.P.; Petrelli, N.J.; Belghiti, J. Extending the frontiers of surgical therapy for hepatic colorectal metastases: Is there a limit? J. Clin. Oncol. 2005, 23, 8490–8499. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, M.; Makuuchi, M.; Torzilli, G.; Takayama, T.; Kawasaki, S.; Kosuge, T.; Yamamoto, J.; Imamura, H. Extension of the Frontiers of Surgical Indications in the Treatment of Liver Metastases from Colorectal Cancer. Ann. Surg. 2000, 231, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- Balogh, J.; David Victor, E.H.A., III; Burroughs, S.G.; Boktour, M.; Saharia, A.; Li, X.; Ghobrial, R.M.; Monsour, H.P., Jr. Hepatocellular carcinoma: A review. J. Hepatocell. Carcinoma 2016, 5, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Nimura, Y.; Kamiya, J.; Kondo, S.; Nagino, M.; Uesaka, K.; Oda, K.; Sano, T.; Yamamoto, H.; Hayakawa, N. Aggressive preoperative management and extended surgery for hilar cholangiocarcinoma: Nagoya experience. J. Hepatobiliary Pancreat. Surg. 2000, 7, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Van Gulik, T.; Kloek, J.; Ruys, A.; Busch, O.; Van Tienhoven, G.; Lameris, J.; Rauws, E.; Gouma, D. Multidisciplinary management of hilar cholangiocarcinoma (Klatskin tumor, Extended resection is associated with improved survival. Eur. J. Surg. Oncol. 2011, 37, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Kingham, T.P.; Correa-Gallego, C.; D’Angelica, M.I.; Gönen, M.; DeMatteo, R.P.; Fong, Y.; Allen, P.J.; Blumgart, L.H.; Jarnagin, W.R. Hepatic parenchymal preservation surgery: Decreasing morbidity and mortality rates in 4152 resections for malignancy. J. Am. Coll. Surg. 2015, 220, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Petruzzi, P.; Crocetti, L. Chemoembolization of hepatocellular carcinoma. Semin. Intervent. Radiol. 2013, 30, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Iñarrairaegui, M.; Bilbao, J.I. Radioembolization for hepatocellular carcinoma. J. Hepatol. 2012, 56, 464–473. [Google Scholar] [CrossRef] [PubMed]
- McDermott, S.; Gervais, D.A. Radiofrequency ablation of liver tumors. Semin. Intervent. Radiol. 2013, 30, 49–55. [Google Scholar] [PubMed]
- hiina, S.; Tateishi, R.; Arano, T.; Uchino, K.; Enooku, K.; Nakagawa, H.; Asaoka, Y.; Sato, T.; Masuzaki, R.; Kondo, Y. Radiofrequency Ablation for Hepatocellular Carcinoma: 10-Year Outcome and Prognostic Factors. Am. J. Gastroenterol. 2012, 107, 569–577. [Google Scholar]
- Crissien, A.M.; Frenette, C. Current management of hepatocellular carcinoma. Gastroenterol. Hepatol. 2014, 10, 153–161. [Google Scholar]
- Liu, Y.; Zheng, Y.; Li, S.; Li, B.; Zhang, Y.; Yuan, Y. Percutaneous microwave ablation of larger hepatocellular carcinoma. Clin. Radiol. 2013, 68, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Roberts, L.R. Hepatocellular carcinoma: A global view. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Gores, G.J.; Mazzaferro, V. Hepatocellular carcinoma: Clinical frontiers and perspectives. Gut 2014, 63, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Huntington, J.T.; Royall, N.A.; Schmidt, C.R. Minimizing blood loss during hepatectomy: A literature review. J. Surg. Oncol. 2014, 109, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.Y. A simplified technique for hepatic resection: The crush method. Ann. Surg. 1974, 180, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Ronnie, T. Current techniques of liver transection. HPB 2007, 9, 166–173. [Google Scholar] [Green Version]
- Lesurtel, M.; Selzner, M.; Petrowsky, H.; McCormack, L.; Clavien, P.-A. How should transection of the liver be performed? A prospective randomized study in 100 consecutive patients: Comparing four different transection strategies. Ann. Surg. 2005, 242, 814–822. [Google Scholar] [CrossRef] [PubMed]
- De Boer, M.T.; Molenaar, I.Q.; Porte, R.J. Impact of blood loss on outcome after liver resection. Dig. Surg. 2007, 24, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Schiergens, T.S.; Rentsch, M.; Kasparek, M.S.; Frenes, K.; Jauch, K.-W.; Thasler, W.E. Impact of perioperative allogeneic red blood cell transfusion on recurrence and overall survival after resection of colorectal liver metastases. Dis. Colon Rectum. 2015, 58, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, J.; Kosuge, T.; Takayama, T.; Shimada, K.; Yamasaki, S.; Ozaki, H.; Yamaguchi, N.; Mizuno, S.; Makuuchi, M. Perioperative blood transfusion promotes recurrence of hepatocellular carcinoma after hepatectomy. Surgery 1994, 115, 303–309. [Google Scholar] [PubMed]
- Yamamoto, J.; Kosuge, T.; Takayama, T.; Shimada, K.; Yamasaki, S.; Ozaki, H.; Yamaguchi, N.; Mizuno, S.; Makuuchi, M. Modulation of coagulation and fibrinolysis in hepatic resection: A randomized prospective control study using antithrombin III concentrates. Thromb. Res. 1994, 74, 105–114. [Google Scholar]
- Yoshimura, Y.; Kubo, S.; Shirata, K.; Hirohashi, K.; Tanaka, H.; Shuto, T.; Takemura, S.; Kinoshita, H. Risk factors for postoperative delirium after liver resection for hepatocellular carcinoma. World J. Surg. 2004, 28, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Kaibori, M.; Saito, T.; Matsui, Y.; Uchida, Y.; Ishizaki, M.; Kamiyama, Y. A review of the prognostic factors in patients with recurrence after liver resection for hepatocellular carcinoma. Am. J. Surg. 2007, 193, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.S.; Cho, S.S.; Ha, T.Y.; Hwang, S.; Lee, S.G.; Kim, Y.K. Intraoperative factors associated with delayed recovery of liver function after hepatectomy: Analysis of 1969 living donors. Acta Anaesthesiol. Scand. 2016, 60, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; Chen, C.L.; Lin, C.C.; Yang, C.H.; Wang, C.C.; Wang, S.H.; Liu, Y.W.; Yong, C.C.; Concejero, A.; Jawan, B. Intraoperative blood loss is a risk factor for complications in donors after living donor hepatectomy. Liver Transplant. 2006, 12, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poon, R.T.; Fan, S.T.; Lo, C.M.; Liu, C.L.; Lam, C.M.; Yuen, W.K.; Yeung, C.; Wong, J. Improving perioperative outcome expands the role of hepatectomy in management of benign and malignant hepatobiliary diseases: Analysis of 1222 consecutive patients from a prospective database. Ann. Surg. 2004, 240, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Zhang, J.; Lu, J.-H.; Yang, G.-S.; Wu, M.-C.; Yu, W.-F. Risk Factors Influencing Postoperative Outcomes of Major Hepatic Resection of Hepatocellular Carcinoma for Patients with Underlying Liver Diseases. World J. Surg. 2011, 35, 2073–2082. [Google Scholar] [CrossRef] [PubMed]
- Kooby, D.A.; Stockman, J.; Ben-Porat, L.; Gonen, M.; Jarnagin, W.R.; Dematteo, R.P.; Tuorto, S.; Wuest, D.; Blumgart, L.H.; Fong, Y. Influence of transfusions on perioperative and long-term outcome in patients following hepatic resection for colorectal metastases. Ann. Surg. 2003, 237, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Van Gulik, T.M.; de Graaf, W.; Dinant, S.; Busch, O.R.; Gouma, D.J. Vascular occlusion techniques during liver resection. Dig. Surg. 2007, 24, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-I. Ischemia-reperfusion injury of the human liver during hepatic resection. J. Hepatobiliary Pancreat. Surg. 2003, 10, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, Y.; Ishizaki, Y.; Imamura, H.; Sugo, H.; Yoshimoto, J.; Kawasaki, S. Effects of intermittent Pringle’s manoeuvre on cirrhotic compared with normal liver. Br. J. Surg. 2010, 97, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.-C.; Navarra, G.; Jiao, L.R.; Nicholls, J.P.; Jensen, S.L.; Habib, N.A. New technique for liver resection using heat coagulative necrosis. Ann. Surg. 2002, 236, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Curro, G.; Bartolotta, M.; Barbera, A.; Jiao, L.; Habib, N.; Navarra, G. Ultrasound-guided radiofrequency-assisted segmental liver resection: A. new technique. Ann. Surg. 2009, 250, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Delis, S.G.; Madariaga, J.; Bakoyiannis, A.; Dervenis, C. Current role of bloodless liver resection. WJG 2007, 14, 826–829. [Google Scholar] [CrossRef]
- Pai, M.; Navarra, G.; Ayav, A.; Sommerville, C.; Khorsandi, S.; Damrah, O.; Jiao, L.; Habib, N. Laparoscopic Habib™-4X: A bipolar radiofrequency device for bloodless laparoscopic liver resection. HPB 2008, 10, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Jiao, L.R.; Ayav, A.; Navarra, G.; Sommerville, C.; Pai, M.; Damrah, O.; Khorsandi, S.; Habib, N.A. Laparoscopic liver resection assisted by the laparoscopic Habib Sealer. Surgery 2008, 144, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Jiao, L.R.; Khorsandi, S.; Canelo, R.; Spalding, D.R.; Habib, N.A. Liver resection with bipolar radiofrequency device: Habib™-4X. HPB 2008, 144, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Frampton, A.; Mikhail, S.; Resende, V.; Kornasiewicz, O.; Spalding, D.; Jiao, L.; Habib, N. Radiofrequency assisted liver resection: Analysis of 604 consecutive cases. Eur. J. Surg. Oncol. 2012, 38, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Lu, W.; Yu, N.; Yang, G.; Li, Y.; Huang, Z.; Li, J.; Li, K.; Xu, H.; Chen, S. Habib 4X-assisted resection versus clamp-crush resection for hepatocellular carcinoma: A propensity-matching study. Oncotarget 2017, 8, 4218–4227. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Spalding, D.; Jiao, L.; Habib, N. Use of bipolar radiofrequency in parenchymal transection of the liver, pancreas and kidney. Dig. Surg. 2012, 29, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Yan, J.; Feng, X.-B.; Xia, F.; Li, X.-W.; Ma, K.-S.; Bie, P. Efficiency and safety of radiofrequency-assisted hepatectomy for hepatocellular carcinoma with cirrhosis: A single-center retrospective cohort study. WJG 2015, 21, 10159–10165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Zhang, W.; Li, Y.; Li, P.; Li, J.; Gong, J.; Chen, Y. Radiofrequency-assisted versus clamp-crushing parenchyma transection in cirrhotic patients with hepatocellular carcinoma: A randomized clinical trial. Dig. Dis. Sci. 2013, 58, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Feng, X.; Xiao, S.; Yan, J.; Xia, F.; Ma, K.; Li, X. Short-and long-term outcomes of hepatectomy with or without radiofrequency-assist for the treatment of hepatocellular carcinomas: A retrospective comparative cohort study. Biosci. Trends 2015, 9, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G. MOOSE Guidelines for Meta-Analyses and Systematic Reviews of Observational Studies. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011] [Internet]. Cochrane Handb. Syst. Rev. Interv. 2011. Available online: http://handbook-5-1.cochrane.org/ (accessed on 8 November 2018).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chootrakool, H.; Shi, J.Q.; Yue, R. Meta-analysis and sensitivity analysis for multi-arm trials with selection bias. Stat. Med. 2011, 30, 1183–1198. [Google Scholar] [CrossRef] [PubMed]
- Mavridis, D.; Welton, N.J.; Sutton, A.; Salanti, G. A selection model for accounting for publication bias in a full network meta-analysis. Stat. Med. 2014, 33, 5399–5412. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing Data and Undertaking Meta-Analyses. Cochrane Handb. Syst. Rev. Interv. Cochrane B Ser. 2008, 243–296. [Google Scholar] [CrossRef]
- Reccia, I.; Kumar, J.; Kusano, T.; Giakoustidis, A.; Zanellato, A.; Retsas, P.; Habib, N.; Jiao, L.; Spalding, D.; Pai, M. Radiofrequency-assisted liver resection: Technique and results. Surg. Oncol. 2018, 27, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Makuuchi, M.; Inoue, K. The vascular control in liver resection: Revisitation of a controversial issue. Hepatogastroenterology 2002, 49, 28–31. [Google Scholar] [PubMed]
- Alkozai, E.M.; Lisman, T.; Porte, R.J. Bleeding in Liver Surgery: Prevention and Treatment. Clin. Liver Dis. 2009, 13, 145–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoekstra, L.T.; Van Trigt, J.D.; Reiniers, M.J.; Busch, O.R.; Gouma, D.J.; Van Gulik, T.M. Vascular occlusion or not during liver resection: The continuing story. Dig. Surg. 2012, 29, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.N.; Koch, M.; Mehrabi, A.; Weidmann, K.; Motschall, E.; Kahlert, C.; Büchler, M.W.; Weitz, J. Portal triad clamping versus vascular exclusion for vascular control during hepatic resection: A systematic review and meta-analysis. J. Gastrointest. Surg. 2009, 13, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Chouillard, E.K.; Gumbs, A.A.; Cherqui, D. Vascular clamping in liver surgery: Physiology, indications and techniques. Ann. Surg. Innov. Res. 2010, 4, 2. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, E.K.; Noun, R.; Belghiti, J. Hepatic vascular occlusion: Which technique? Surg. Clin. N. Am. 2004, 84, 563–585. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Koch, M.; Schmidt, T.; Motschall, E.; Bruckner, T.; Weidmann, K.; Mehrabi, A.; Büchler, M.W.; Weitz, J. Meta-analysis of the clamp-crushing technique for transection of the parenchyma in elective hepatic resection: Back to where we started? Ann. Surg. Oncol. 2009, 16, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Moggia, E.; Rouse, B.; Simillis, C.; Li, T.; Vaughan, J.; Davidson, B.R.; Gurusamy, K.S. Methods to decrease blood loss during liver resection: A network meta-analysis. Cochrane Database Syst. Rev. 2016, 10, CD010683. [Google Scholar] [CrossRef] [PubMed]
- Pringle, J.H.V. Notes on the Arrest of Hepatic Hemorrhage Due to Trauma. Ann. Surg. 1908, 48, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Dixon, E.; Vollmer, C.M., Jr.; Bathe, O.F.; Sutherland, F. Vascular occlusion to decrease blood loss during hepatic resection. Am. J. Surg. 2005, 190, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Gurusamy, K.S.; Sheth, H.; Kumar, Y.; Sharma, D.; Davidson, B.R. Methods of vascular occlusion for elective liver resections. Cochrane Database Syst. Rev. 2009, CD007632. [Google Scholar] [CrossRef]
- Lau, W.Y.; Lai, E.C.H.; Lau, S.H.Y. Methods of vascular control technique during liver resection: A comprehensive review. Hepatobiliary Pancreat. Dis. Int. 2010, 9, 473–481. [Google Scholar] [PubMed]
- Serracino-Inglott, F.; Habib, N.A.; Mathie, R.T. Hepatic ischemia-reperfusion injury. Am. J. Surg. 2001, 181, 160–166. [Google Scholar] [CrossRef]
- Belghiti, J.; Noun, R.; Malafosse, R.; Jagot, P.; Sauvanet, A.; Pierangeli, F.; Marty, J.; Farges, O. Continuous versus intermittent portal triad clamping for liver resection: A. controlled study. Ann. Surg. 1999, 229, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Capussotti, L.; Nuzzo, G.; Polastri, R.; Giuliante, F.; Muratore, A.; Giovannini, I. Continuous versus intermittent portal triad clamping during hepatectomy in cirrhosis. Results of a prospective, randomized clinical trial. Hepatogastroenterology 2003, 50, 1073–1077. [Google Scholar] [PubMed]
- Wang, C.-C.; Yap, A.Q.; Chen, C.-L.; Concejero, A.M.; Lin, Y.-H. Comparison of major hepatectomy performed under intermittent pringle maneuver versus continuous pringle maneuver coupled with in situ hypothermic perfusion. World J. Surg. 2011, 35, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.; Wente, M.; Schemmer, P.; Diener, M.; Hoffmann, K.; Motschall, E.; Schmidt, J.; Weitz, J.; Büchler, M. Systematic review and meta-analysis of the effect of portal triad clamping on outcome after hepatic resection. Br. J. Surg. 2008, 95, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Doklestic, K.; Karamarkovic, A.; Stefanovic, B.; Milic, N.; Gregoric, P.; Djukic, V.; Bajec, D. The efficacy of three transection techniques of liver resection: A randomized clinical trial. Hepatogastroenterology 2012, 59, 1501–1506. [Google Scholar] [CrossRef] [PubMed]
- Veteläinen, R.; van Vliet, A.; Gouma, D.J.; van Gulik, T.M. Steatosis as a risk factor in liver surgery. Ann. Surg. 2007, 245, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, H.; Kuroda, S.; Mikuriya, Y.; Ohdan, H. Ischemia-reperfusion injury in patients with fatty liver and the clinical impact of steatotic liver on hepatic surgery. Surg. Today 2014, 44, 1611–1625. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Nimura, Y.; Nagino, M.; Bland, K.I.; Chaudry, I.H. Role of thromboxane in producing hepatic injury during hepatic stress. Arch. Surg. 2005, 140, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Yao, P.; Morris, D.L. Radiofrequency ablation-assisted liver resection: Review of the literature and our experience. HPB 2006, 8, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.-W.; Lee, P.-H.; Kusano, T.; Reccia, I.; Jayant, K.; Habib, N. Impact of cavitron ultrasonic surgical aspirator (CUSA) and bipolar radiofrequency device (Habib-4X) based hepatectomy for hepatocellular carcinoma on tumour recurrence and disease-free survival. Oncotarget 2017, 55, 93644–93654. [Google Scholar] [CrossRef] [PubMed]
- Mazmishvili, K.; Jayant, K.; Janikashvili, N.; Kikodze, N.; Mizandari, M.; Pantsulaia, I.; Paksashvili, N.; Sodergren, M.H.; Reccia, I.; Pai, M. Study to evaluate the immunomodulatory effects of radiofrequency ablation compared to surgical resection for liver cancer. J. Cancer 2018, 9, 3187. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Srivastava, R.M.; López-Albaitero, A.; Ferrone, S.; Ferris, R.L. Natural killer (NK): Dendritic cell (DC) cross talk induced by therapeutic monoclonal antibody triggers tumor antigen-specific T cell immunity. Immunol. Res. 2011, 50, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Widenmeyer, M.; Shebzukhov, Y.; Haen, S.P.; Schmidt, D.; Clasen, S.; Boss, A.; Kuprash, D.V.; Nedospasov, S.A.; Stenzl, A.; Aebert, H. Analysis of tumor antigen-specific T cells and antibodies in cancer patients treated with radiofrequency ablation. Int. J. Cancer 2011, 128, 2653–2662. [Google Scholar] [CrossRef] [PubMed]
- Pedroza-Gonzalez, A.; Verhoef, C.; Ijzermans, J.N.; Peppelenbosch, M.P.; Kwekkeboom, J.; Verheij, J.; Janssen, H.L.; Sprengers, D. Activated tumor-infiltrating CD4+ regulatory T cells restrain antitumor immunity in patients with primary or metastatic liver cancer. Hepatology 2013, 57, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Napoletano, C.; Taurino, F.; Biffoni, M.; De Majo, A.; Coscarella, G.; Bellati, F.; Rahimi, H.; Pauselli, S.; Pellicciotta, I.; Burchell, J.M. RFA strongly modulates the immune system and anti-tumor immune responses in metastatic liver patients. Int. J. Oncol. 2008, 32, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Gibney, G.T.; Weiner, L.M.; Atkins, M.B. Predictive biomarkers for checkpoint inhibitor-based immunotherapy. Lancet Oncol. 2016, 17, e542–e551. [Google Scholar] [CrossRef] [Green Version]
- Houot, R.; Schultz, L.M.; Marabelle, A.; Kohrt, H. T-cell-based Immunotherapy: Adoptive Cell Transfer and Checkpoint Inhibition. Cancer Immunol. Res. 2015, 3, 1115–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, A.G.; Ulahannan, S.V.; Makorova-Rusher, O.; Rahma, O.; Wedemeyer, H.; Pratt, D.; Davis, J.L.; Hughes, M.S.; Heller, T.; ElGindi, M. Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma. J. Hepatol. 2017, 6, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Gomez-Martin, C.; de la Mata, M.; Iñarrairaegui, M.; Garralda, E.; Barrera, P.; Riezu-Boj, J.I.; Larrea, E.; Alfaro, C.; Sarobe, P. A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J. Hepatol. 2013, 59, 81–88. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Design | Retrospective, Prospective, Randomized or Non-Randomized |
|---|---|
| Study group | Liver resection |
| Study size | Any |
| Length of follow-up | Any |
| Source | Peer-reviewed journals |
| Language | Any |
| Outcome measure | Primary: blood loss, blood transfusion, operative time; secondary: bile leak, post-hepatectomy liver failure, abdominal abscess, pleural effusion, overall hospital stay, morbidity and 30-day mortality |
| Study | Publication Year | Study Design | (Clamp-Crush) (CC) Group | Habib™-4X Group | Liver Disease | Operative Time (Minutes) (CC vs. Habib™-4X) |
|---|---|---|---|---|---|---|
| Li et al. [51] | 2012 | Randomized (Prospective) | 37 | 38 | HCC | 188.7 ± 62.1 vs. 193.7 ± 50.5 (p = 0.28) |
| Guo et al. [52] | 2015 | Retrospective | 325 | 272 | HCC | 295.9 ± 107.3 vs. 211.2 ± 63.2 (p = 0.00) |
| Zhang et al. [50] | 2015 | Retrospective | 79 | 100 | HCC | 245.6 ± 75.5 vs. 230.5 ± 77.9 (p = 0.19) |
| Qiu et al. [48] | 2017 | Retrospective | 102 | 81 | HCC | 196.0 ± 54.0 vs. 160 ± 61.0 (p = 0.00) |
| Study | Blood Loss (mL) (CC vs. Habib™-4X) | Blood Transfusion (CC vs. Habib™-4X) | Bile Leak (CC vs. Habib™-4X) | PHLF (CC vs. Habib™-4X) | Pleural Effusion (CC vs. Habib™-4X) | Abdominal Abscess (CC vs. Habib™-4X) | Total Morbidity (CC vs. Habib™-4X) | Mortality 30 Days’ (CC vs. Habib™-4X) |
|---|---|---|---|---|---|---|---|---|
| Li et al. [51] | 863.0 ± 610.5 vs. 618.7 ± 446.0 (p = 0.001) | 10 vs. 6 (p = 0.23) | 6 vs. 4 (p = 0.46) | NA | 5 vs. 4 (p = 0.69) | 2 vs. 1 (p = 0.54) | 16 vs. 11 (p < 0.001) | 0 vs. 1 (p = 0.321) |
| Guo et al. [52] | 763.2 ± 1154.8 vs. 485.54 ± 465.8 (p = 0.003) | 103 vs. 52 (p = 0.000) | 21 vs. 22 (p = 0.44) | 12 vs. 16 (p = 0.44) | 27 vs. 13 (p = 0.40) | 16 vs. 20 (p = 0.21) | 88 vs. 83 (p = 0.35) | NA |
| Zhang et al. [50] | 587.0 ± 418.6 vs. 525.0 ± 375.3 (p = 0.01) | 19 vs. 17 (p = 0.24) | 2 vs. 7 (p = 0.31) | 0 vs. 6 (p = 0.04) | 4 vs. 6 (p = 1.0) | 3 vs. 3 (p = 1.0) | 14 vs. 28 (p = 0.11) | 0 vs. 3 (p = 0.23) |
| Qiu et al. [48] | 250.0 ± 6 74.0 vs. 150.0 ± 572.0 (p = 0.005) | 25 vs. 10 (p = 0.03) | 3 vs. 2 (p = 0.89) | 2 vs. 1 (p = 1.0) | NA | NA | 9 vs. 4 (p = 0.39) | 0 vs. 0 (p = 0.99) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jayant, K.; Sodergren, M.H.; Reccia, I.; Kusano, T.; Zacharoulis, D.; Spalding, D.; Pai, M.; Jiao, L.R.; Huang, K.W. A Systematic Review and Meta-Analysis Comparing Liver Resection with the Rf-Based Device Habib™-4X with the Clamp-Crush Technique. Cancers 2018, 10, 428. https://doi.org/10.3390/cancers10110428
Jayant K, Sodergren MH, Reccia I, Kusano T, Zacharoulis D, Spalding D, Pai M, Jiao LR, Huang KW. A Systematic Review and Meta-Analysis Comparing Liver Resection with the Rf-Based Device Habib™-4X with the Clamp-Crush Technique. Cancers. 2018; 10(11):428. https://doi.org/10.3390/cancers10110428
Chicago/Turabian StyleJayant, Kumar, Mikael H. Sodergren, Isabella Reccia, Tomokazu Kusano, Dimitris Zacharoulis, Duncan Spalding, Madhava Pai, Long R. Jiao, and Kai Wen Huang. 2018. "A Systematic Review and Meta-Analysis Comparing Liver Resection with the Rf-Based Device Habib™-4X with the Clamp-Crush Technique" Cancers 10, no. 11: 428. https://doi.org/10.3390/cancers10110428