1. Introduction
The role of dietary sugars has become an increasing and controversial active public health issue in recent years. The high consumption of added sugars has been ultimately associated with various conditions, such as obesity, risk factors for coronary heart disease (CHD), diabetes, and metabolic syndrome [
1]. However, at first, the terminology used to describe sugars has resulted in difficulties with respect to providing comparisons between countries and it also impacts the ability to compare intakes with recommendations, risk factors, or disease endpoints, and with the results of intervention studies. The term ‘total sugars’ includes all mono- and disaccharides, namely glucose, fructose, galactose, lactose, sucrose, and maltose. Added and free sugars differ in the quantity of natural sugars included in their definitions. Therefore, free sugars include sugars naturally present in honey, syrups, fruit juices, nectar juices, and fruit juice concentrates, whereas added sugars only refer to those added during processing. No universally accepted definition for added sugars exists [
2]. In addition to various definitions for the term “added sugars”, the World Health Organization (WHO) utilizes the term “free sugars”. Free sugars, as defined by the WHO, refer to monosaccharides and disaccharides added to foods and drinks by the manufacturer, cook, or consumer, and sugars naturally present in honey, syrups, fruit juices, and nectar juices. Intrinsic sugars are defined by the WHO as the sugars incorporated in the structure of intact fruit and vegetables. Free sugars are similar to added sugars, as the term includes all sugars and syrups added to foods; however, free sugars also include sugars naturally present in fruit juices, nectar juices, and fruit juice concentrates. As a consequence, the assessment of added/free sugar intake and compliance with recommendations seems to be extremely difficult. Added sugars are chemically identical to sugar that naturally occurs in food products, and the body cannot distinguish the source of the nutrient and processes the sugar in the same way [
3]. Sugar may be added to food products for many reasons, most commonly to add sweetness and enhance the palatability of foods. Another function of sugar within food products is texture enhancement. Finally, sugar may also play a role in food safety by inhibiting the growth of microorganisms at high concentrations [
4]. It is also well recognized that excess calorie consumption can lead to weight gain and increased risk of obesity and obesity-related comorbidities. The so-called “empty” calories from solid fats and added sugars play a role in this when consumed in excess and unbalanced in terms of energy expenditure [
5]. As a consequence, there is an increasing concern that excessive consumption of added sugars may also contribute to the obesity epidemic worldwide [
1,
6,
7].
In 2010, the European Food Safety Authority (EFSA) published its scientific opinion on dietary reference values for carbohydrates and dietary fiber and was unable to set an upper level for sugar intake as a result of insufficient evidence in relation to body weight, cardiovascular risk factors, type 2 diabetes, and nutrient density of the diet or dental caries [
8]. The latter was mainly due to an association with frequency, but not to quantity. The WHO published its updated guideline on free sugars intake for adults and children in relation to body weight and oral health [
2]. The recommendations were: (i) a reduced intake of free sugars throughout the life-course (strong recommendation); (ii) the reduction of the intake of free sugars to <10% of the total energy (TE) intake in both adults and children (strong recommendation); and (iii) a further reduction of free sugars to below 5% of the total energy intake (conditional recommendation).
It has also been well stated that to design and implement effective measures to reduce added sugars, their dietary sources must be clearly identified [
9,
10]. In fact, most food composition tables do not include information on the added and free sugars content of foods, and few countries have reported on individual sugar intakes. Recently, Newens and Walton [
11] reviewed current intakes of dietary sugars from national representative dietary surveys across the world. Surprisingly, the so-called added sugars intake in adults was only reported in nine countries and ranged from 7.2% TE in Brazilians aged 10 years and older in 2008–2009 to 16.3% TE in US adults aged 18–34 years in 2007–2008. National dietary surveillance, while having inherent limitations (misreporting, accurate updating of food composition tables at the national level, etc.), provides a way to examine eating patterns and their impact on calorie and nutrient intakes across different populations. The use of newly available methodologies (e.g., real-time recording of eating and drinking events) has been urgently claimed to avoid these difficulties if possible [
12,
13]. Different dietary surveys have been previously conducted in Spain [
14,
15,
16]. However, no one has approached, to date, energy and nutrient intake using new, more accurate technologies. As a consequence, the ANIBES Study (Anthropometry, Intake and Energy Balance in Spain) was recently completed in a representative sample of all individuals living in Spain (excluding the autonomous cities of Melilla and Ceuta) aged 9 to 75 years, living in municipalities >2000 inhabitants [
17,
18]. The present study focuses on sugar intake (free and intrinsic) in the Spanish diet for the first time, as well as analyzes food and beverage sources that currently contribute to sugar intake, according to sex and age groups. The latter aim is of particular interest, to provide, firstly, more detailed and accurate information on how the different food and beverage groups and subgroups represent the current market in Spain, but also to drive, in the near future, an adequate labeling of added sugars.
4. Discussion
In this representative sample of the Spanish population, the total sugar consumption comprised 17% TE (median: 71.5 g/day). The free sugar consumption was 7.3% TE (median: 28.8 g/day) and the intrinsic sugar consumption was 9.6% TE (median: 38.3 g/day). The total sugar intake (free and intrinsic) was higher in men than in women for all age groups, although in terms of the contribution to the total energy intake, the opposite was observed. Differences with age were observed for free sugar and intrinsic sugar consumption when considering the percent of TE: it was much higher for free sugar in children and adolescents compared to intrinsic sugar in the elderly population. One in four Spaniards usually exceed the WHO recommendation that free sugar contribute less than 10% of the total energy intake, according to the present data [
2]. Moreover, 25% of the entire population would be within the limits (5% TE) proposed by the SCAN (
Scientific Advisory Committee on Nutrition, United Kingdom).
In the United Kingdom [
20] or the conditional recommendation of the WHO [
2]. The groups most likely to exceed the WHO recommendation were, however, children and young people aged 9 to 12 and 13–17 years, which clearly deserves further attention in terms of effort to improve their diet quality. This adherence pattern to the recommendations for the majority of the population from the ANIBES Study is much higher than that found for the Dutch population (29%–33% of the adults 19–69 years) [
21] or in the last Australian Health Survey: Consumption of Added Sugars (2011–2012) [
22], where one in two Australians (52%) usually exceeded the WHO recommendation. Recently, in a representative national survey in the Netherlands [
21], the consumption of total, intrinsic, and added/free sugars was 22% TE, 14% TE, and 12% TE, respectively, much higher than the results obtained in the Spanish ANIBES Study. These results in the Netherlands are also comparable to the recent intake data from the USA and Canada: in 31,305 children and adults aged six years and older from the National Health and Nutrition Examination Survey (NHANES) 2003–2010, added (“free”) sugars provided approximately 14% TE [
23,
24]; in 35,107 Canadians of all ages from the 2004 Canadian Community Health Survey, the total sugar intake was estimated at 21%TE and added sugar intake at 10%–14% TE [
25]. Approximately 13% of adults’ total caloric intakes in the USA came from added sugars between 2005 and 2010 according to National Health and Nutrition Examination Survey (NHANES), which was higher in comparison to the Dietary Guidelines for Americans [
24]. Interestingly, Wittekind and Walton [
9] have published the trends in sugar intakes reported between 1971 and 2012 in different national nutrition surveys from 10 European countries, but also for Australia, New Zealand, and the United States: In 44 possible comparisons within 13 countries, seven age- and gender-specific or combined groups, and four categories of sugars, the mean population intakes of energy from sugars decreased or remained stable in most comparisons. These findings are also comparable to trends occurring in Spain, according to the Food Consumption Survey evolution in the last decades [
16]. In fact, the percentage contribution of the total carbohydrates has steadily decreased since the 1960s in Spain. Moreover, in that decade, the energy profile was in line with the recommendations [
16]. In Spain, unfortunately, scarce data or outdated methodology for individual sugars result in a very scarce number of studies to compare with the present results from the ANIBES Study. Of interest, from the ENRICA (Nutrition and Cardiovascular Risk in Spain) study carried out in 2008–2010 (>18 years), it was published that the daily sugar intake per capita was 111.2 g/day, but data on individual sugars were not available [
26]. Unfortunately, in the more recent ENIDE (National Dietary Survey in Spain) carried out in 2011 (18–64 years), no data on total and individual sugars were provided [
15].
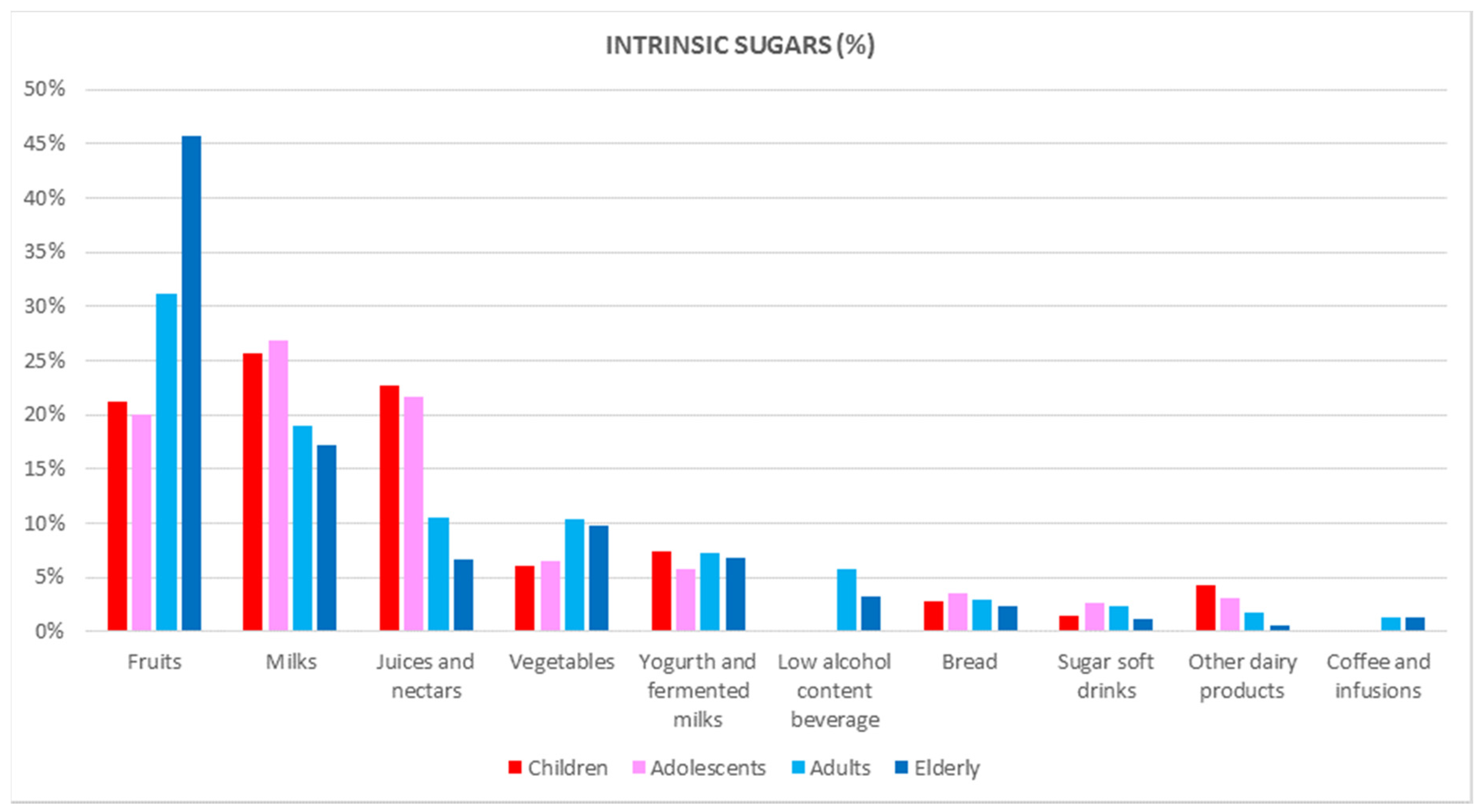
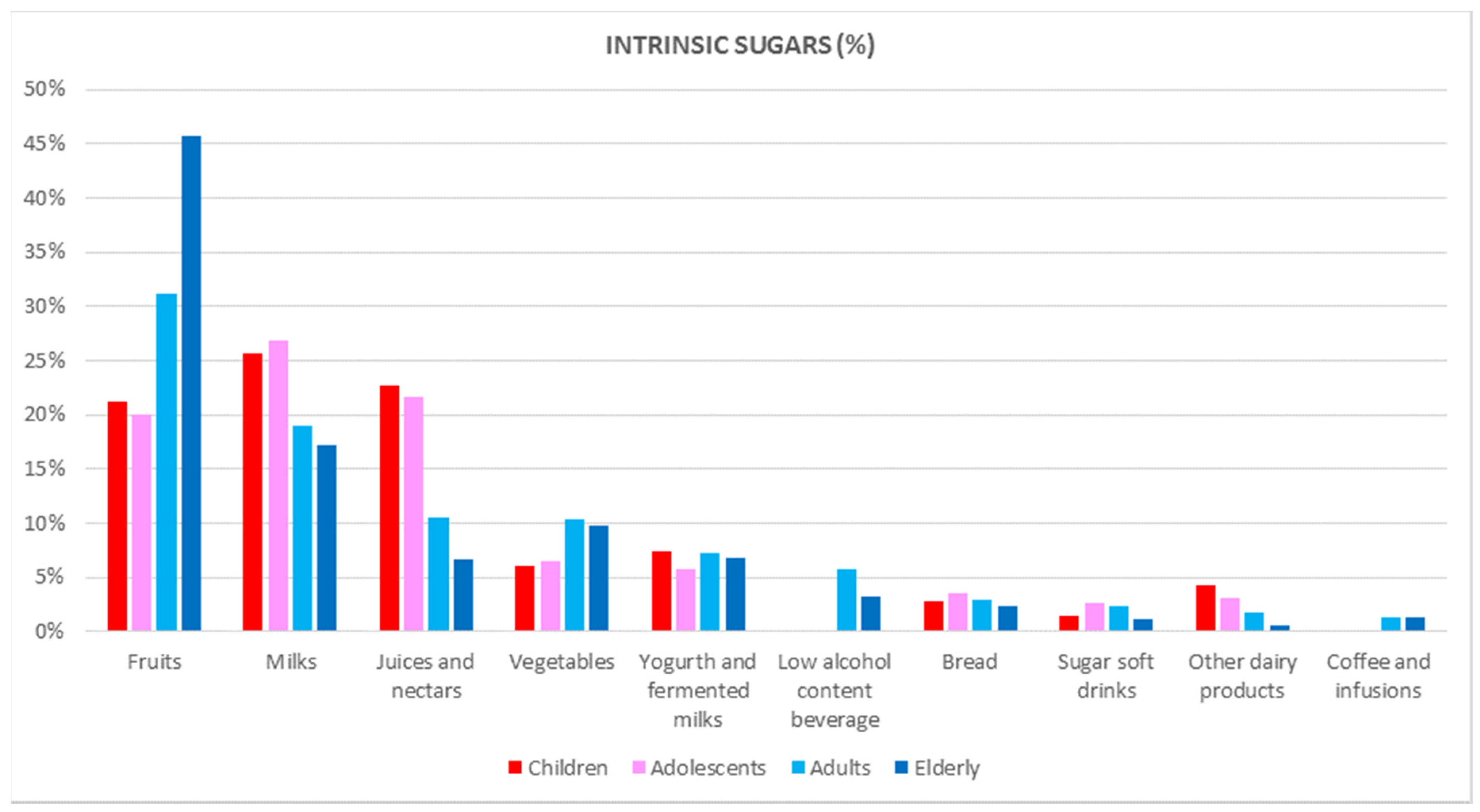
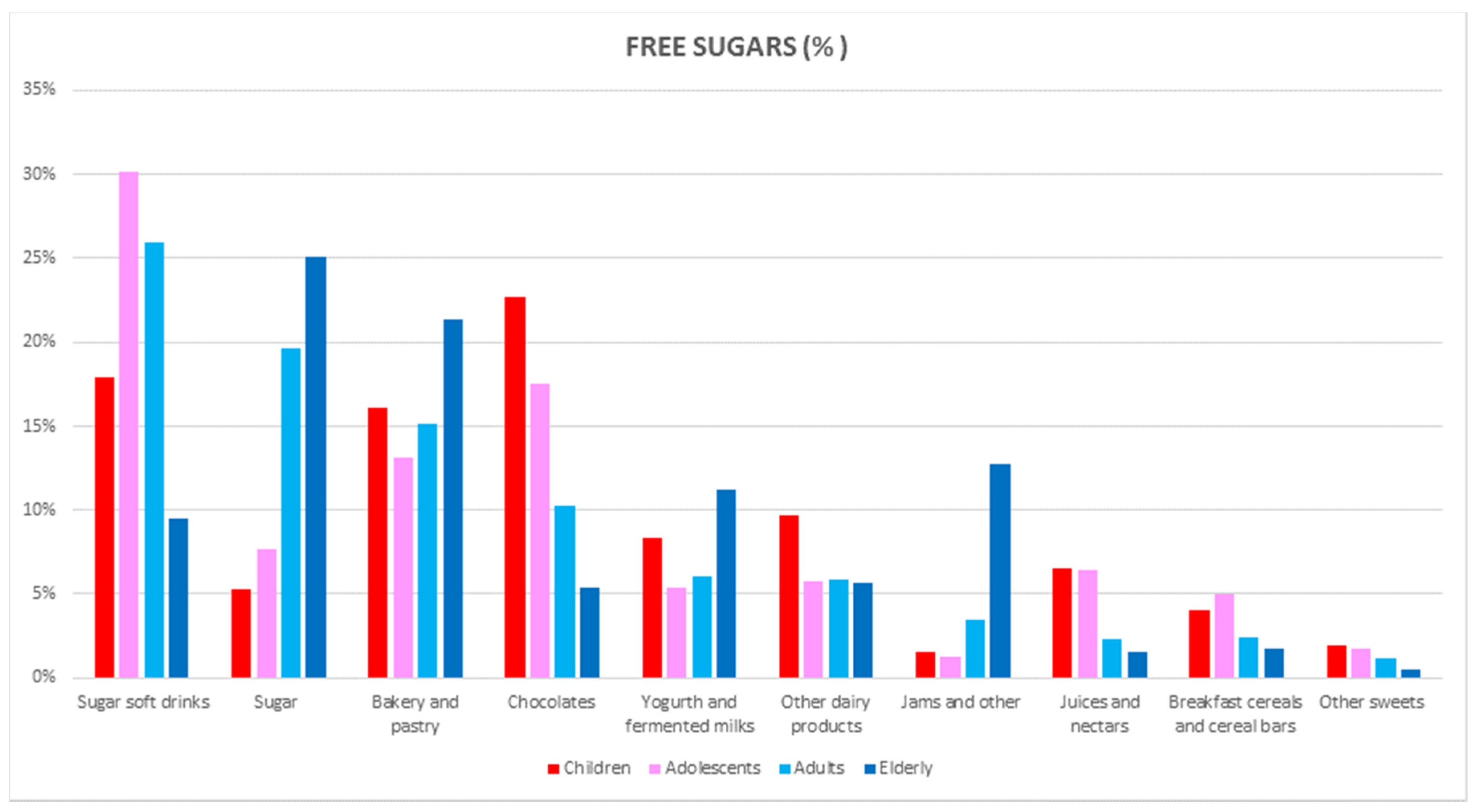
This is the first time that detailed information on the dietary intake of individual sugars and food and beverage sources has been provided in our country. Foods that contributed most to the free sugar intake in the ANIBES Spanish population were sugar soft drinks, sugar, bakery and pastry items, chocolates, yogurt and fermented milk, other dairy products, jams, juices and nectars, and breakfast cereals and cereal bars, accounting for >90% of the contribution. The major sources of intrinsic sugars (%) were fruits, milks, fruit juices and nectar juices, vegetables, yogurt and fermented milks, low-alcohol-content beverages, bread, and sugar soft drinks, summing up to more than 90% of the diet contribution. Nearly 70% of the free sugars were consumed in the total ANIBES Spanish population from usually energy-dense, nutrient-poor foods and beverages, such as sugar soft drinks, sugar, bakery and pastry items, and chocolates. However, marked differences were observed between the age groups for free sugar consumption: in children, the chocolates group ranked first, and sugar was the main contributor in the oldest group (65–75 years), while sugar soft drinks were the first contributor for both adolescents and adults.
Interestingly, summing up the usually perceived healthy foods (fruits, milks, juices/nectars, vegetables, and yogurt and fermented milk) accounted for 80% of the total intrinsic sugars, which was higher in women versus men. For the youngest groups (9 to 17 years), milks ranked first, whereas in adults and the elderly, fruits were the main contributor of intrinsic sugars. Concerning the micronutrient dilution (e.g., vitamins) phenomenon that may occur when the diet model is more based on energy-dense and nutrient-poor foods and beverages, it was found that the sum of the fruits and vegetables contribution (55.4%) to the total intrinsic sugars in the elderly was remarkably higher when compared to the children (27.3%) or adolescents (26.6%).
As published by NHANES [
23,
24], the top sources of added sugars in Americans are sugar-sweetened beverages, desserts, sugary fruit and candy. Within NHANES, the added sugar intake has already decreased between 1999–2000 and 2007–2008 from 100 g/day (18% TE) to 77 g/day (15% TE), which was primarily due to a reduction in sugar-sweetened beverage consumption. In the already-mentioned national survey in the Netherlands [
21], fruit juices and sugar-sweetened beverages, including soft drinks, lemonades, and energy drinks, contributed most to the intake of free sugars, especially in children. In Australian children, sugar soft drinks, cakes, biscuits, pastries, butter-based products, and sugar and sweet spreads were the main contributors to the added sugars intake [
22].
Few issues in nutrition generate more scientific controversy than the potential associations between added or free sugars and health. In fact, recently, various scientific and health organizations have recommended upper limits of sugar consumption. The WHO [
2], the Scientific Advisory Committee on Nutrition in the United Kingdom (SACN) [
20], and the American Heart Association (AHA) [
27] have proposed dramatically reducing the upper limits of sugar consumption to levels of 10% of calories consumed or less. The 2015 Dietary Guidelines Advisory Committee [
28] also recommended a reduction of the upper limit to no more than 10% of calories from added sugars. This latter recommendation derived also that the Food and Drug Administration (FDA) in the USA recommended a similar upper limit of added sugars consumption (10% TE) and proposed to include such information in the nutrition facts panel [
29]. Moreover, a further reduction to below 5% has been suggested by WHO to provide additional health benefits [
2]. In contrast, the European Food Safety Administration (EFSA) found no harm, and even some benefit, in fructose consumption comprising up to 25% of total energy [
8].
A limitation of the present study is that despite our efforts and innovative methodology, the free sugar content in food products could be under- or over-estimated. Food processes, and consequently the food products available on the market, are continuously changing in content and ingredients. The strengths of the present study include the use of a three-day dietary record using precise and innovative technology to collect food and beverage information at the individual level. As already stated, most food composition tables do not include information on the intrinsic and free sugar content of foods, leading to the use of incomplete food composition tables or supply data. Hence, the development of a food composition table/database for the ANIBES Study including not only the total sugar content, but also intrinsic and free sugars, represents the main strength of the present study. Furthermore, the ANIBES Study was conducted among a representative sample of the Spanish population.
In conclusion, with a mean intake of 17% TE total sugar, 9.6% TE intrinsic sugar, and 7.3% TE added/free sugar, only a moderate percentage of the Spanish population under study adhered to the updated WHO recommendations. However, the results obtained show a remarkably better pattern when compared to other countries. The present findings for the main dietary sources of individual sugars also show a higher variety of foods and beverages contributing, in comparison with non-Mediterranean countries, although urgent efforts are needed to improve diet quality in the youngest populations where patterns and trends are of concern. Future studies are warranted on the associations between the intake of total and individual sugars and health outcomes and chronic diseases in Spain to better clarify nutritional policy.

 ,
, 





{kind=link}
{kind=link}