Development of a Semi-Quantitative Food Frequency Questionnaire to Assess the Dietary Intake of a Multi-Ethnic Urban Asian Population


Abstract
:1. Introduction
2. Materials and Methods
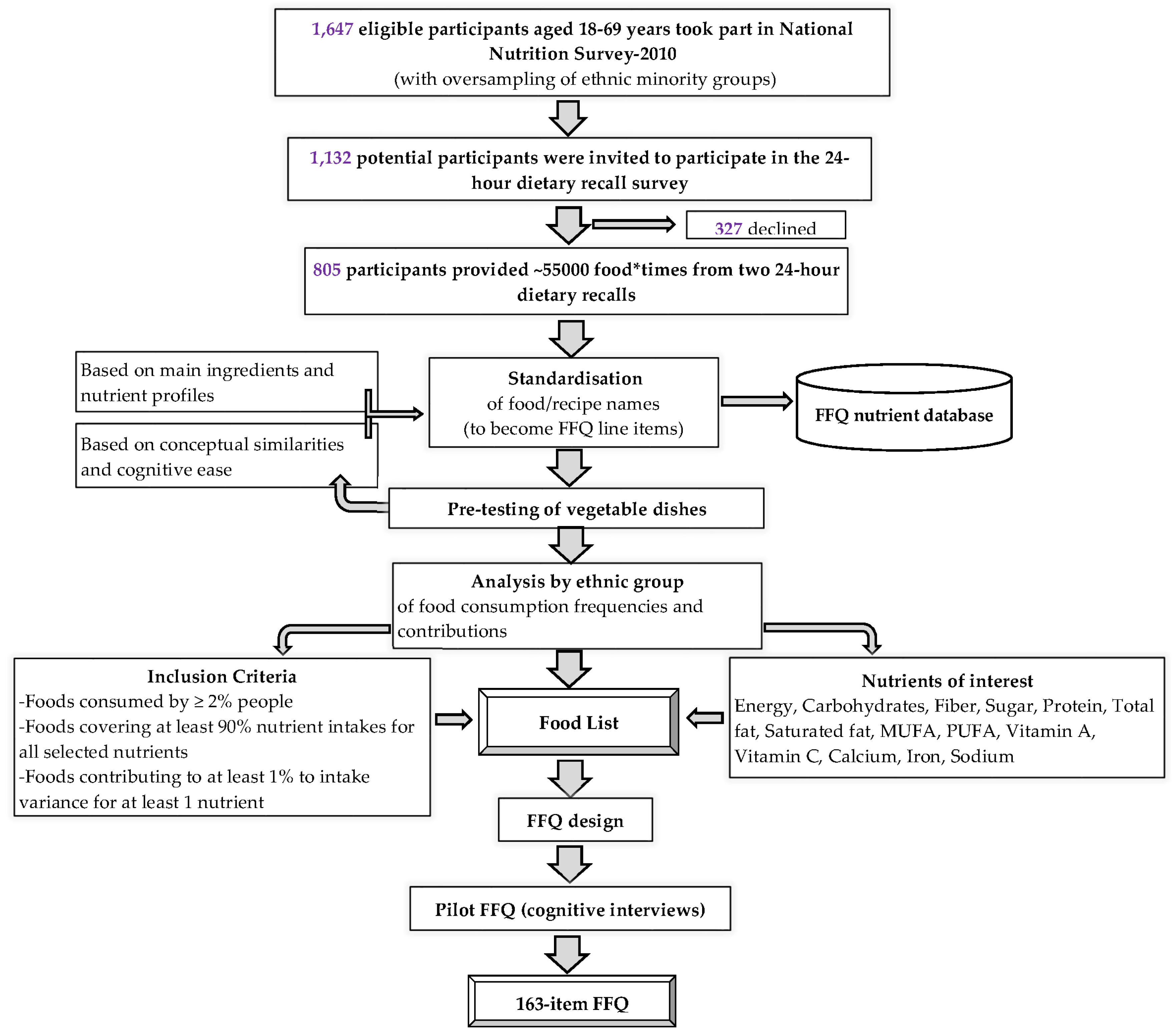
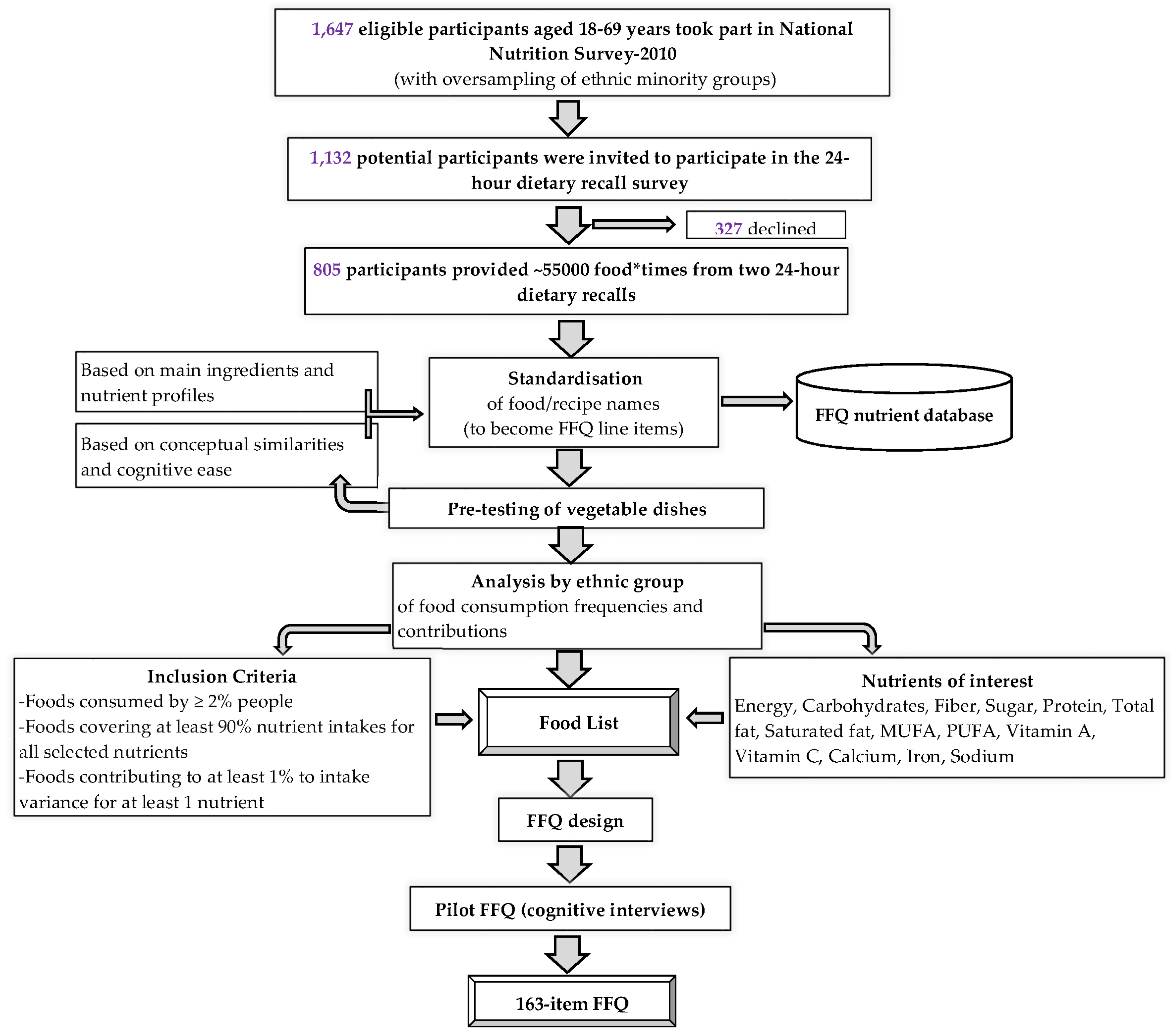
2.1. 24-h Dietary Recall Data Collection
2.2. Development of the FFQ
2.2.1. Standardization
2.2.2. Pre-Testing of Vegetables Dish Questions
2.2.3. Food List of the FFQ
2.2.4. FFQ Design
2.2.4.1. Layout of the FFQ
2.2.4.2. Sub-Type Questions
2.2.4.3. Frequency of Food Consumption
2.2.4.4. FFQ Portion Size
2.3. Pre-Testing and Pilot Testing of the FFQ
2.3.1. Feedback from Local Food Experts and Stakeholders
2.3.2. Cognitive Interviews
2.4. Nutrient Database
2.5. Statistical Analysis
3. Results
3.1. FFQ Development Phase
3.2. FFQ Testing Phase: Cognitive Interview Results
3.3. Final FFQ
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| F | female |
| FFQ | food frequency questionnaire |
| FIND | food information and nutrient database |
| M | male |
| MUFA | mono-unsaturated fatty acid |
| NHS | national health survey |
| PUFA | poly-unsaturated fatty acid |
| SD | standard deviation |
| SFA | saturated fatty acid |
| y | years |
References
- World Health Organisation. Noncommunicable Disease Report-Chapter 1; Burden: Mortality, Morbidity and Risk Factors. Available online: http://www.who.int/nmh/publications/ncd_report_chapter1.pdf?ua=1 (accessed on 5 July 2016).
- Thompson, F.E.; Subar, A.F. Nutrition in the Prevention and Treatment of Disease: Dietary Assessment Methodology, 3rd ed.Elsevier Inc.: Oxford, UK, 2013. Available online: http://appliedresearch.cancer.gov/diet/adi/thompson_subar_dietary_assessment_methodology.pdf (accessed on 11 August 2016).
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013; Volume 40. [Google Scholar]
- Mayer-Davis, E.J.; Vitolins, M.Z.; Carmichael, S.L.; Hemphill, S.; Tsaroucha, G.; Rushing, J.; Levin, S. Validity and reproducibility of a food frequency interview in a multi-cultural epidemiology study. Ann. Epidemiol. 1999, 9, 314–324. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Rock, C.L.; Wang, Y.; Jenny, N.S.; Jacobs, D.R. Associations between dietary macronutrient intake and plasma lipids demonstrate criterion performance of the multi-ethnic study of atherosclerosis (mesa) food-frequency questionnaire. Br. J. Nutr. 2009, 102, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Beukers, M.H.; Dekker, L.H.; de Boer, E.J.; Perenboom, C.W.; Meijboom, S.; Nicolaou, M.; de Vries, J.H.; Brants, H.A. Development of the helius food frequency questionnaires: Ethnic-specific questionnaires to assess the diet of a multiethnic population in the netherlands. Eur. J. Clin. Nutr. 2015, 69, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Ireland, P.; Jolley, D.; Giles, G.; O'Dea, K.; Powles, J.; Rutishauser, I.; Wahlqvist, M.L.; Williams, J. Development of the melbourne ffq: A food frequency questionnaire for use in an australian prospective study involving an ethnically diverse cohort. Asia Pac. J. Clin. Nutr. 1994, 3, 19–31. [Google Scholar] [PubMed]
- Stram, D.O.; Hankin, J.H.; Wilkens, L.R.; Pike, M.C.; Monroe, K.R.; Park, S.; Henderson, B.E.; Nomura, A.M.; Earle, M.E.; Nagamine, F.S.; et al. Calibration of the dietary questionnaire for a multiethnic cohort in hawaii and los angeles. Am. J. Epidemiol. 2000, 151, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Shahar, D.; Shai, I.; Vardi, H.; Brener-Azrad, A.; Fraser, D. Development of a semi-quantitative food frequency questionnaire (ffq) to assess dietary intake of multiethnic populations. Eur. J. Epidemiol. 2003, 18, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Department of Statistics. Singapore in Figures 2016. Available online: https://www.singstat.gov.sg/docs/default-source/default-document-library/publications/publications_and_papers/reference/sif2016.pdf (accessed on 4 August 2016).
- Deurenberg-Yap, M.; Li, T.; Tan, W.L.; van Staveren, W.A.; Deurenberg, P. Validation of a semiquantitative food frequency questionnaire for estimation of intakes of energy, fats and cholesterol among singaporeans. Asia Pac. J. Clin. Nutr. 2000, 9, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Epidemiology and Disease Control Division. Report of the National Health Survey 2010. 2011. Available online: https://www.moh.gov.sg/content/dam/moh_web/Publications/Reports/2011/NHS2010%20-%20low%20res.pdf (accessed on 4 August 2016). [Google Scholar]
- Jayawardena, R.; Swaminathan, S.; Byrne, N.M.; Soares, M.J.; Katulanda, P.; Hills, A.P. Development of a food frequency questionnaire for sri lankan adults. Nutr. J. 2012, 11, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Promotion Board, Research and Strategic Plannind Division. Report of the National Nutrition Survey 2010. Available online: http://www.hpb.gov.sg/HOPPortal/content/conn/HOPUCM/path/Contribution%20Folders/uploadedFiles/HPB_Online/Publications/NNS-2010.pdf (accessed on 8 March 2016).
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the us department of agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin Nutr. 2003, 77, 1171–1178. [Google Scholar] [PubMed]
- Health Promotion Board. Energy and Nutrient Composition of Food. 2011. Available online: http://focos.hpb.gov.sg/eservices/ENCF/ (accessed on 4 August 2016). [Google Scholar]
- Block, G.; Hartman, A.M.; Dresser, C.M.; Carroll, M.D.; Gannon, J.; Gardner, L. A data-based approach to diet questionnaire design and testing. Am. J. Epidemiol. 1986, 124, 453–469. [Google Scholar] [PubMed]
- Kobayashi, T.; Tanaka, S.; Toji, C.; Shinohara, H.; Kamimura, M.; Okamoto, N.; Imai, S.; Fukui, M.; Date, C. Development of a food frequency questionnaire to estimate habitual dietary intake in japanese children. Nutr. J. 2010, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Willis, G.B. Cognitive Interviewing: A “How to” Guide; Research Triangle Institute: Research Triangle Park, NC, USA, 1999. [Google Scholar]
- Department of Statistics. Census of Population 2010 Statistical Release 1: Demographic Characteristics, Education, Language and Religion. 2010. Available online: http://www.singstat.gov.sg/publications/publications-and-papers/cop2010/census10_stat_release1#sthash.dawylkhf.dpuf (accessed on 26 April 2016). [Google Scholar]
- Subar, A.F.; Thompson, F.E.; Smith, A.F.; Jobe, J.B.; Ziegler, R.G.; Potischman, N.; Schatzkin, A.; Hartman, A.; Swanson, C.; Kruse, L.; et al. Improving food frequency questionnaires: A qualitative approach using cognitive interviewing. J. Am. Diet. Assoc. 1995, 95, 781–788. [Google Scholar] [CrossRef]
- Wakai, K.; Egami, I.; Kato, K.; Lin, Y.; Kawamura, T.; Tamakoshi, A.; Aoki, R.; Kojima, M.; Nakayama, T.; Wada, M.; et al. A simple food frequency questionnaire for japanese diet--Part i. Development of the questionnaire, and reproducibility and validity for food groups. J. Epidemiol. 1999, 9, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Bautista, L.E.; Herran, O.F.; Pryer, J.A. Development and simulated validation of a food-frequency questionnaire for the colombian population. Public Health Nutr. 2005, 8, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Byers, T.; Marshall, J.; Fiedler, R.; Zielezny, M.; Graham, S. Assessing nutrient intake with an abbreviated dietary interview. Am. J. Epidemiol. 1985, 122, 41–50. [Google Scholar] [PubMed]
- Hamdan, M.; Monteagudo, C.; Lorenzo-Tovar, M.L.; Tur, J.A.; Olea-Serrano, F.; Mariscal-Arcas, M. Development and validation of a nutritional questionnaire for the palestine population. Public Health Nutr. 2014, 17, 2512–2518. [Google Scholar] [CrossRef] [PubMed]
- Decarli, A.; Ferraroni, M.; Palli, D. A reduced questionnaire to investigate the mediterranean diet in epidemiologic studies. Epidemiology 1994, 5, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Overvad, K.; Tjonneland, A.; Haraldsdottir, J.; Ewertz, M.; Jensen, O.M. Development of a semiquantitative food frequency questionnaire to assess food, energy and nutrient intake in denmark. Int. J. Epidemiol. 1991, 20, 900–905. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Total Sample | Chinese | Malay | Indian | p-Value |
|---|---|---|---|---|---|
| (n = 805) | (n = 318) | (n = 244) | (n = 243) | ||
| Age (years) | 44.5 ± 16.0 | 44.5 ± 16.4 | 43.9 ± 16.1 | 45.0 ± 15.5 | 0.72 |
| Females, n (%) | 398 (49.4) | 161 (50.6) | 122 (50.0) | 115 (47.3) | 0.72 |
| Educational status, n (%) | |||||
| Primary education or less | 161 (20.0) | 56 (17.6) | 54 (22.1) | 51 (21.1) | |
| Secondary school | 309 (38.4) | 109 (34.3) | 124 (50.8) | 76 (31.4) | <0.001 |
| Higher education including vocational | 198 (24.6) | 79 (24.8) | 59 (24.2) | 60 (24.8) | |
| University | 135 (16.8) | 74 (23.3) | 6 (2.5) | 55 (22.7) | |
| Marital status, n (%) | |||||
| Single | 173 (21.5) | 80 (25.2) | 51 (20.9) | 42 (17.4) | |
| Married | 555 (69.0) | 213 (67.0) | 172 (70.5) | 170 (70.2) | 0.11 |
| Others † | 76 (9.5) | 25 (7.9) | 21 (8.6) | 30 (12.4) | |
| Working status, n (%) | |||||
| Employed | 519 (64.6) | 207 (65.1) | 155 (63.5) | 157 (64.9) | |
| Homemaker | 144 (17.9) | 49 (15.4) | 44 (18.0) | 51 (21.1) | |
| Retired | 64 (8.0) | 26 (8.2) | 24 (9.8) | 14 (5.8) | 0.002 |
| Unemployed | 17 (2.1) | 1 (0.3) | 6 (2.5) | 10 (4.1) | |
| Student/National service | 60 (7.5) | 35 (11.0) | 15 (6.1) | 10 (4.1) | |
| Family income (S$ per month), n (%) | |||||
| <2000 | 174 (21.6) | 47 (14.8) | 75 (30.7) | 52 (21.5) | |
| 2000–3999 | 222 (27.6) | 67 (21.1) | 78 (32.0) | 77 (31.8) | |
| 4000–5999 | 157 (19.5) | 67 (21.1) | 43 (17.6) | 47 (19.4) | <0.001 |
| ≥6000 | 138 (17.1) | 79 (24.8) | 17 (6.9) | 42 (17.4) | |
| Don’t know/refused | 113 (14.1) | 58 (18.2) | 31 (12.7) | 24 (9.9) | |
| Body mass index (kg/m2) | 25.2 ± 4.9 | 23.6 ± 3.9 | 26.6 ± 5.6 | 26.1 ± 4.6 | <0.001 |
| Chinese (n = 318) | Malay (n = 244) | Indian (n = 243) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Rank | Food items | Energy (%) | % consumers | Food items | Energy (%) | % consumers | Food items | Energy (%) | % consumers |
| 1 | White rice | 12.7 | 81.1 | White rice | 15.9 | 88.1 | White rice | 16.0 | 85.6 |
| 2 | Fried noodles | 6.8 | 42.1 | Chicken dishes | 7.3 | 64.3 | White bread | 4.9 | 52.7 |
| 3 | Noodles in soup | 6.3 | 37.1 | White bread | 4.7 | 54.5 | Fried noodles | 4.4 | 30.0 |
| 4 | Chicken dishes | 4.6 | 60.1 | Fried noodles | 4.3 | 30.3 | Chicken dishes | 3.8 | 43.6 |
| 5 | Pork dishes | 3.9 | 50.3 | White fish dishes | 3.9 | 44.3 | Coffee | 3.5 | 62.1 |
| 6 | Dry noodles | 3.2 | 22.0 | Flavored rice | 3.4 | 33.6 | Thosai 3 | 2.7 | 25.1 |
| 7 | White fish dishes | 3.0 | 46.5 | Oily fish dishes | 3.0 | 43.0 | Flavored rice | 2.7 | 23.5 |
| 8 | White bread | 2.7 | 42.5 | Coffee | 2.9 | 57.4 | Dhal 4 | 2.3 | 46.5 |
| 9 | Coffee | 2.4 | 56.9 | Puffs and pies | 2.8 | 20.9 | Chapati 5 | 2.3 | 17.3 |
| 10 | Flavored rice | 2.3 | 22.6 | Tea | 2.0 | 58.6 | White fish dishes | 2.0 | 26.3 |
| 11 | Fried rice | 1.6 | 11.0 | Beef dishes | 2.0 | 24.6 | Noodles in soup | 1.9 | 11.5 |
| 12 | Oily fish dishes | 1.5 | 28.6 | Non-carbonated sweetened drinks 1 | 1.9 | 31.1 | Wholemeal bread | 1.8 | 23.0 |
| 13 | Nuts | 1.4 | 4.7 | Noodles in soup | 1.6 | 15.2 | Tea | 1.8 | 51.0 |
| 14 | Filled buns, savory | 1.2 | 12.6 | Roti prata 2 | 1.5 | 19.7 | Oily fish dishes | 1.6 | 23.9 |
| 15 | Dumplings | 1.2 | 13.5 | Fried rice | 1.5 | 10.2 | Mutton and lamb dishes | 1.4 | 11.9 |
| 16 | Non-carbonated sweetened drinks 1 | 1.1 | 29.2 | Malted drinks | 1.5 | 29.9 | Potato dishes | 1.4 | 37.9 |
| 17 | Tea | 1.1 | 44.0 | Noodles in gravy | 1.3 | 10.2 | Roti prata | 1.4 | 16.5 |
| 18 | Soybean curd dishes | 1.1 | 28.3 | Fried chips and crackers, savory | 1.2 | 20.5 | Malted drinks | 1.3 | 23.9 |
| 19 | Flavored white rice porridge | 1.1 | 12.9 | Processed chicken products | 1.2 | 15.6 | Soybean curd dishes | 1.3 | 18.1 |
| 20 | Red/brown rice | 1.1 | 7.5 | Mutton and lamb dishes | 1.2 | 11.5 | Non-carbonated sweetened drinks | 1.3 | 18.5 |
| Chinese (n = 318) | Malay (n = 244) | Indian (n = 243) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Rank | Food items | Cum R2 † | % of fiber intake ‡ | Food items | Cum R2 † | % of fiber intake ‡ | Food items | Cum R2 † | % of fiber intake ‡ |
| 1 | Pears | 0.11 | 2.78 | Lontong dishes 5 | 0.09 | 1.30 | Dhal | 0.26 | 9.22 |
| 2 | Chocolate | 0.16 | 0.55 | Chicken dishes | 0.16 | 6.04 | Innards | 0.39 | 0.00 |
| 3 | Fried noodles | 0.20 | 7.05 | Puffs and pies | 0.22 | 2.77 | Chapati 7 | 0.46 | 3.25 |
| 4 | Ice cream 1 | 0.24 | 0.49 | Roti prata 6 | 0.26 | 1.76 | Other grains 8 | 0.54 | 0.43 |
| 5 | Sweet desserts in soup | 0.26 | 1.32 | Dumplings | 0.30 | 0.58 | Idli 9 | 0.61 | 1.62 |
| 6 | Egg, fried/scrambled/braised | 0.29 | 0.02 | Egg, fried/scrambled/braised | 0.33 | 0.03 | Red/brown rice | 0.64 | 0.69 |
| 7 | French fries | 0.32 | 1.17 | Flavored rice | 0.36 | 3.69 | Pasta with meat/fish/vegetables | 0.67 | 0.45 |
| 8 | Red/brown rice | 0.35 | 1.30 | Pancake/hotcake/waffle | 0.38 | 0.88 | Flavored wholegrain breakfast cereal | 0.70 | 0.02 |
| 9 | Nuts | 0.37 | 1.58 | Oranges | 0.40 | 0.63 | Nuts | 0.72 | 1.11 |
| 10 | Olives | 0.38 | 0.01 | Fried chips and crackers, savory | 0.43 | 1.20 | Papaya | 0.74 | 1.69 |
| 11 | Papaya | 0.40 | 1.72 | Beef dishes | 0.45 | 1.93 | Soya milk, low sugar | 0.75 | 0.20 |
| 12 | Lettuce | 0.42 | 0.12 | Bean dishes | 0.47 | 1.33 | Bean dishes | 0.77 | 1.58 |
| 13 | Fried rice with vegetables | 0.44 | 0.39 | Milkshake | 0.49 | 0.20 | Ice cream 1 | 0.78 | 0.27 |
| 14 | Noodles in soup | 0.45 | 5.29 | Cauliflower dishes | 0.50 | 0.22 | Savory fried snack | 0.79 | 0.79 |
| 15 | 100% fruit or vegetable juice | 0.47 | 0.44 | Fried noodles | 0.52 | 4.25 | Chicken dishes | 0.79 | 2.12 |
| 16 | Flavored rice | 0.48 | 3.09 | Wholemeal bread | 0.53 | 2.25 | Filled buns, sweet | 0.80 | 0.71 |
| 17 | Oranges | 0.49 | 1.07 | Sweet desserts in soup (with coconut) | 0.55 | 0.61 | Guava | 0.81 | 0.73 |
| 18 | Potato dishes | 0.51 | 1.38 | Powdered nutrition drink | 0.57 | 0.00 | Wholemeal bread | 0.81 | 4.10 |
| 19 | Dragon fruit | 0.52 | 0.57 | White fish dishes | 0.58 | 3.29 | Fried noodles | 0.82 | 4.18 |
| 20 | Pasta with meat/fish/vegetables | 0.53 | 0.90 | Fried rice, plain or with meat/fish | 0.59 | 0.85 | Avocado | 0.83 | 0.40 |
| 21 | Non-carbonated sweetened drinks 2 | 0.54 | 0.28 | Mutton and lamb dishes | 0.60 | 0.89 | Noodles in soup | 0.83 | 1.25 |
| 22 | Filled buns, savory | 0.55 | 1.63 | Peanut butter | 0.61 | 0.49 | Plain wholegrain breakfast cereal | 0.84 | 0.16 |
| 23 | Lotus root dishes | 0.57 | 0.13 | Pears | 0.62 | 0.93 | Sweet desserts in soup | 0.84 | 1.00 |
| 24 | Kaya 3 | 0.58 | 0.06 | Whole milk | 0.63 | 0.01 | Apples | 0.85 | 2.69 |
| 25 | Dhal 4 | 0.58 | 0.21 | Soya milk, low sugar | 0.64 | 0.29 | Dry noodles | 0.85 | 0.38 |
| 26 | Gourd dishes | 0.59 | 0.53 | Preserved vegetables | 0.64 | 0.05 | Cured pork products | 0.86 | 0.05 |
| 27 | Canned meat | 0.60 | 0.03 | Cabbage dishes | 0.65 | 1.50 | Banana flower | 0.86 | 0.00 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neelakantan, N.; Whitton, C.; Seah, S.; Koh, H.; Rebello, S.A.; Lim, J.Y.; Chen, S.; Chan, M.F.; Chew, L.; Van Dam, R.M. Development of a Semi-Quantitative Food Frequency Questionnaire to Assess the Dietary Intake of a Multi-Ethnic Urban Asian Population. Nutrients 2016, 8, 528. https://doi.org/10.3390/nu8090528
Neelakantan N, Whitton C, Seah S, Koh H, Rebello SA, Lim JY, Chen S, Chan MF, Chew L, Van Dam RM. Development of a Semi-Quantitative Food Frequency Questionnaire to Assess the Dietary Intake of a Multi-Ethnic Urban Asian Population. Nutrients. 2016; 8(9):528. https://doi.org/10.3390/nu8090528
Chicago/Turabian StyleNeelakantan, Nithya, Clare Whitton, Sharna Seah, Hiromi Koh, Salome A. Rebello, Jia Yi Lim, Shiqi Chen, Mei Fen Chan, Ling Chew, and Rob M. Van Dam. 2016. "Development of a Semi-Quantitative Food Frequency Questionnaire to Assess the Dietary Intake of a Multi-Ethnic Urban Asian Population" Nutrients 8, no. 9: 528. https://doi.org/10.3390/nu8090528