Macronutrient Balance and Dietary Glycemic Index in Pregnancy Predict Neonatal Body Composition

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
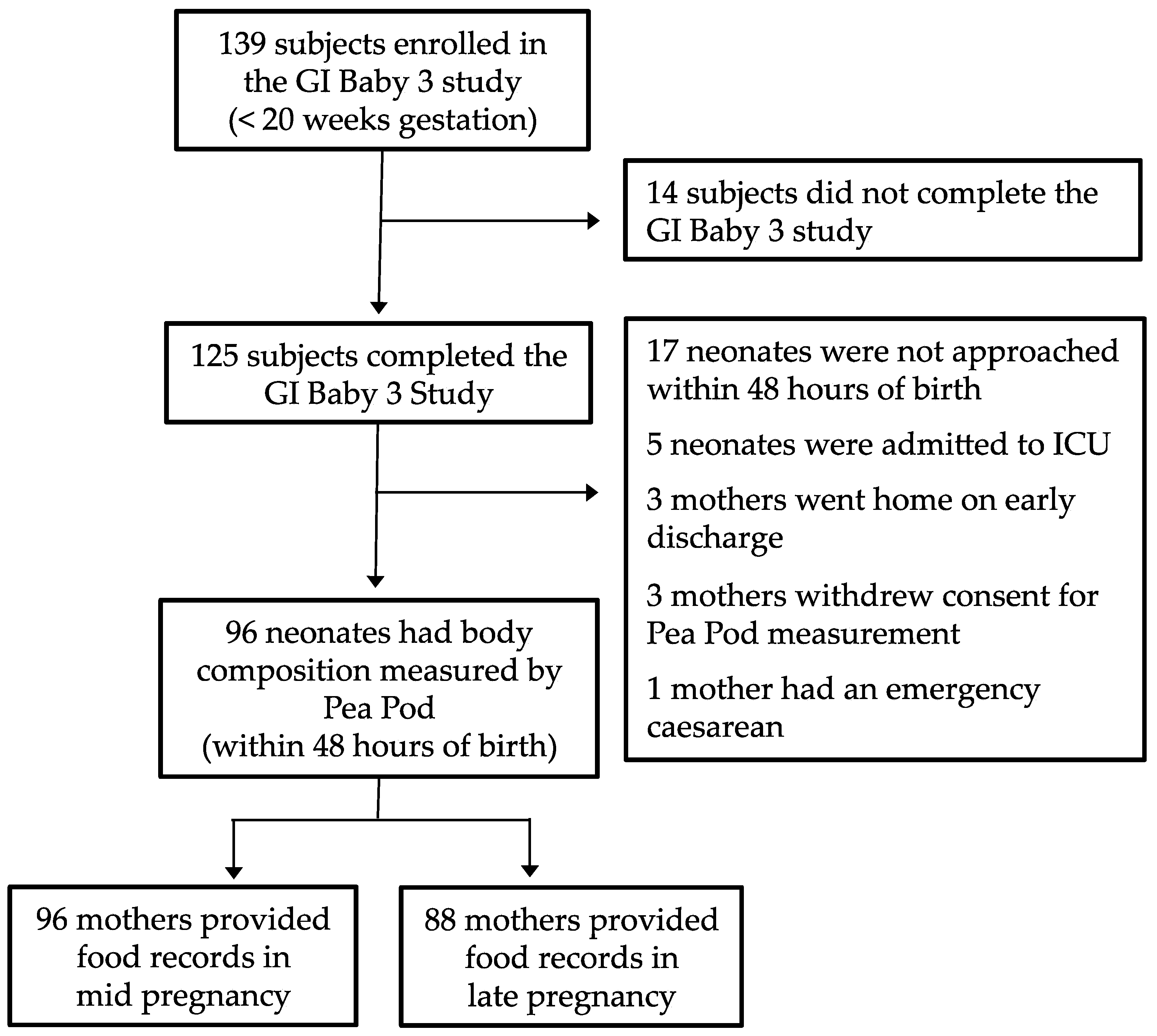
2.1. Sample
2.2. Data Collection
2.3. Statistics
3. Results
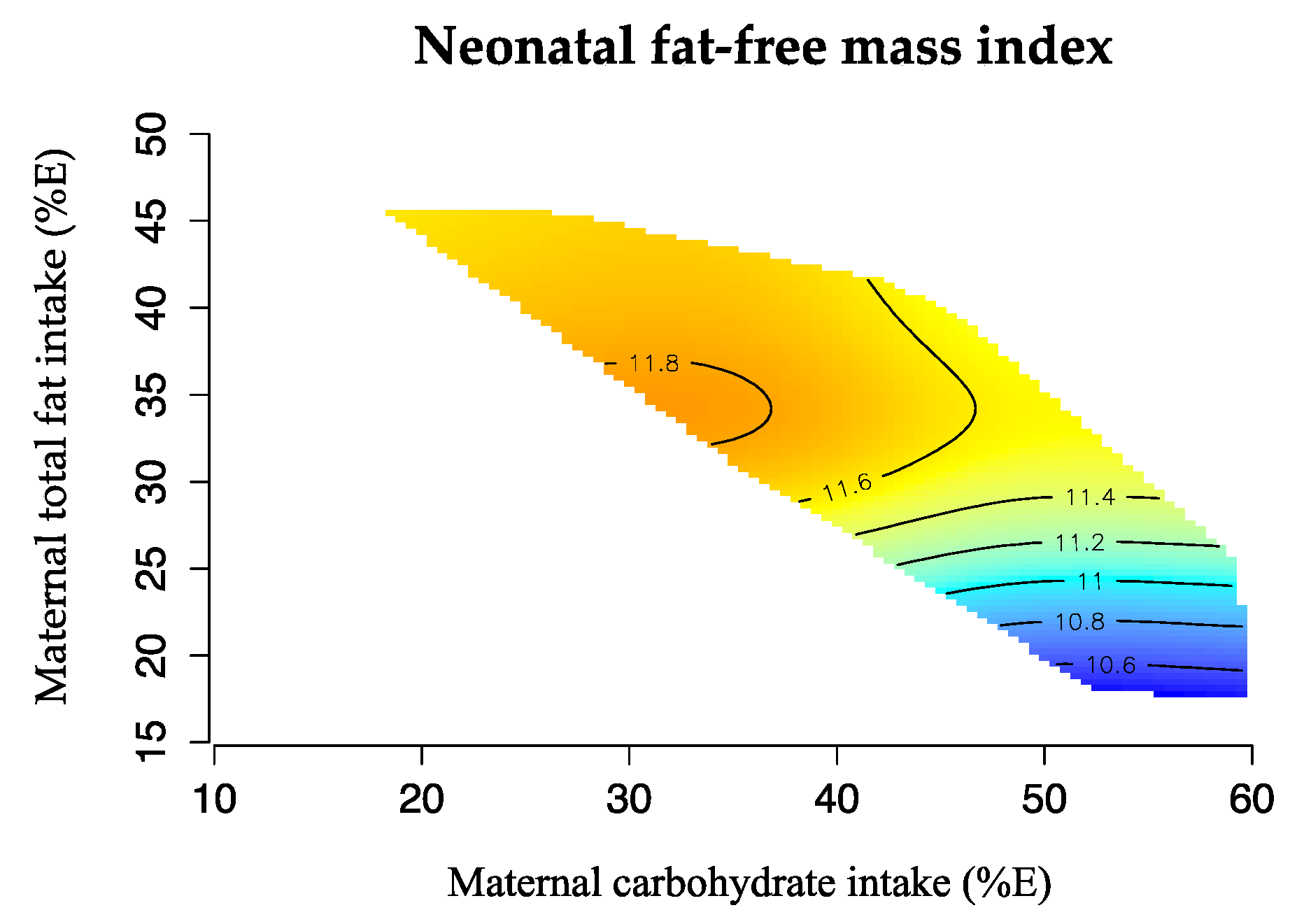
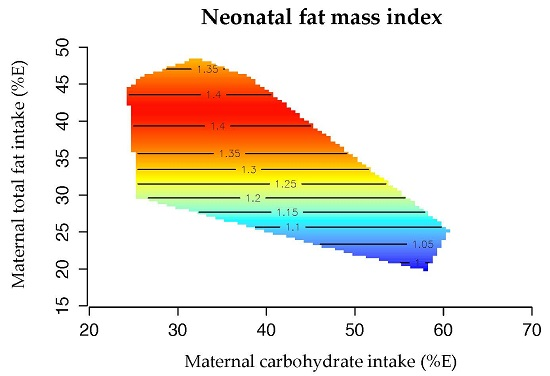
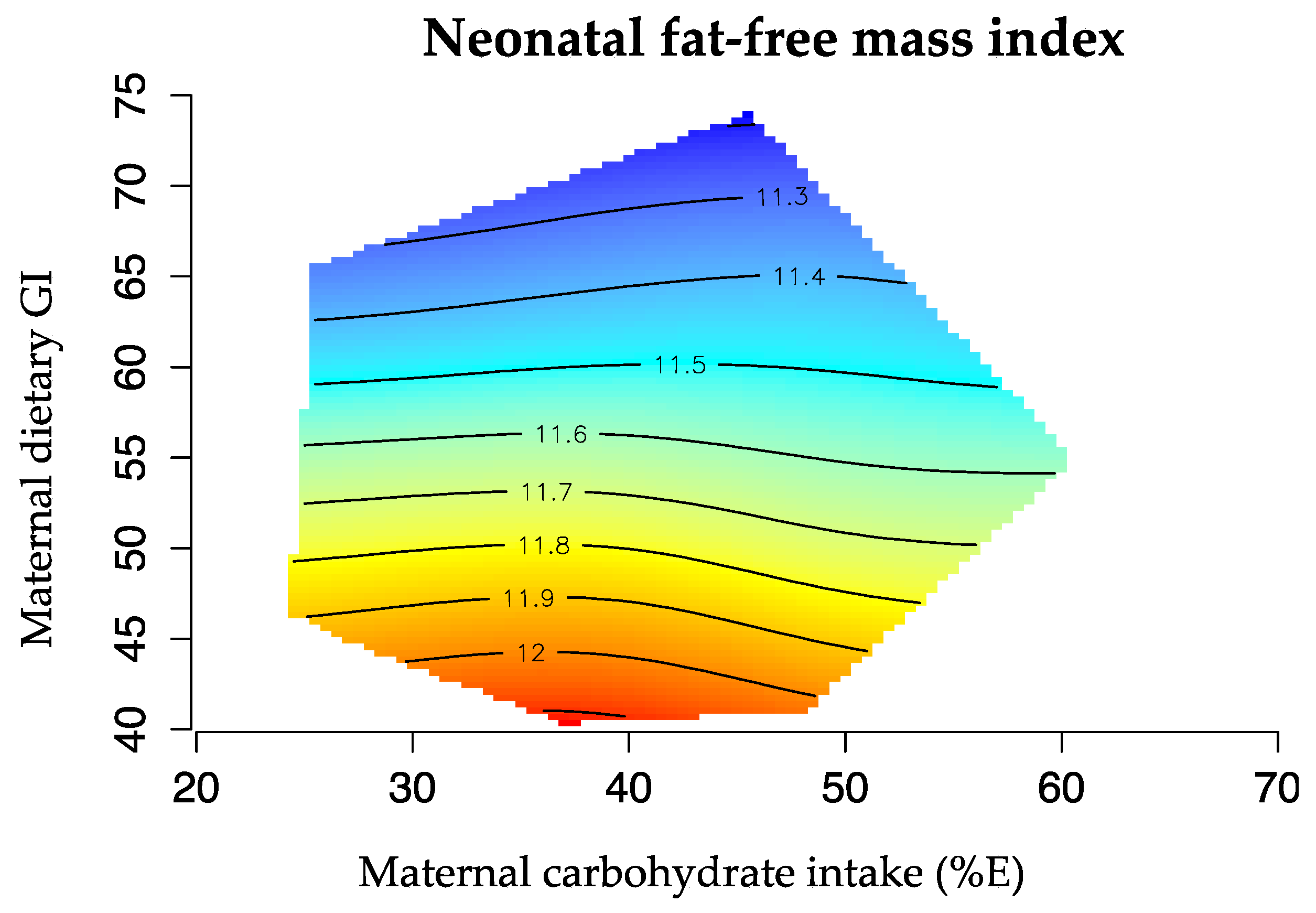
Maternal Macronutrient Balance and Neonatal Body Composition
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- McMillen, I.C.; Robinson, J.S. Developmental origins of the metabolic syndrome: Prediction, plasticity, and programming. Physiol. Rev. 2005, 85, 571–633. [Google Scholar] [CrossRef] [PubMed]
- Gresham, E.; Byles, J.E.; Bisquera, A.; Hure, A.J. Effects of dietary interventions on neonatal and infant outcomes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 1298–1321. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, A.C.; van Der Meulen, J.H.; Osmond, C.; Barker, D.J.; Bleker, O.P. Obesity at the age of 50 years in men and women exposed to famine prenatally. Am. J. Clin. Nutr. 1999, 70, 811–816. [Google Scholar] [PubMed]
- Roseboom, T.; de Rooij, S.; Painter, R. The Dutch famine and its long-term consequences for adult health. Early Hum. Dev. 2006, 82, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Salas, P.; Moore, S.E.; Baker, M.S.; Bergen, A.W.; Cox, S.E.; Dyer, R.A.; Fulford, A.J.; Guan, Y.; Laritsky, E.; Silver, M.J.; et al. Maternal nutrition at conception modulates DNA methylation of human metastable epialleles. Nat. Commun. 2014, 5, 3746. [Google Scholar] [CrossRef] [PubMed]
- Heijmans, B.T.; Tobi, E.W.; Stein, A.D.; Putter, H.; Blauw, G.J.; Susser, E.S.; Slagboom, P.E.; Lumey, L.H. Persistent epigenetic differences associated with prenatal exposure to famine in humans. Proc. Natl. Acad. Sci. USA 2008, 105, 17046–17049. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Eriksson, J.G.; Forsen, T.; Osmond, C. Fetal origins of adult disease: strength of effects and biological basis. Int. J. Epidemiol. 2002, 31, 1235–1239. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A. Maternal constraint of fetal growth and its consequences. Semin. Fetal Neonatal Med. 2004, 9, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Sewell, M.F.; Huston-Presley, L.; Super, D.M.; Catalano, P. Increased neonatal fat mass, not lean body mass, is associated with maternal obesity. Am. J. Obstet. Gynecol. 2006, 195, 1100–1103. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Thomas, A.; Huston-Presley, L.; Amini, S.B. Increased fetal adiposity: A very sensitive marker of abnormal in utero development. Am. J. Obstet. Gynecol. 2003, 189, 1698–1704. [Google Scholar] [CrossRef]
- Shields, B.M.; Knight, B.A.; Powell, R.J.; Hattersley, A.T.; Wright, D.E. Assessing newborn body composition using principal components analysis: Differences in the determinants of fat and skeletal size. BMC Pediatr. 2006, 6, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalano, P.M.; Farrell, K.; Thomas, A.; Huston-Presley, L.; Mencin, P.; de Mouzon, S.H.; Amini, S.B. Perinatal risk factors for childhood obesity and metabolic dysregulation. Am. J. Clin. Nutr. 2009, 90, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Chomtho, S.; Fewtrell, M.S. Programming of body composition by early growth and nutrition. Proc. Nutr. Soc. 2007, 66, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.J.; Le Couteur, D.G.; Raubenheimer, D. Putting the balance back in diet. Cell 2015, 161, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Solon-Biet, S.M.; McMahon, A.C.; Ballard, J.W.; Ruohonen, K.; Wu, L.E.; Cogger, V.C.; Warren, A.; Huang, X.; Pichaud, N.; Melvin, R.G. The ratio of macronutrients, not caloric intake, dictates cardiometabolic health, aging, and longevity in ad libitum-fed mice. Cell Metab. 2014, 19, 418–430. [Google Scholar] [CrossRef] [PubMed]
- Solon-Biet, S.M.; Walters, K.A.; Simanainen, U.K.; McMahon, A.C.; Ruohonen, K.; Ballard, J.W.; Raubenheimer, D.; Handelsman, D.J.; Le Couteur, D.G.; Simpson, S.J. Macronutrient balance, reproductive function, and lifespan in aging mice. Proc. Natl. Acad. Sci. USA 2015, 112, 3481–3486. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.L.; Hure, A.J.; MacDonald-Wicks, L.K.; Smith, R.; Simpson, S.J.; Giles, W.B.; Raubenheimer, D.; Collins, C.E. Dietary balance during pregnancy is associated with fetal adiposity and fat distribution. Am. J. Clin. Nutr. 2012, 96, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.M.; Sheppard, A.; Gluckman, P.D.; Lillycrop, K.A.; Burdge, G.C.; McLean, C.; Rodford, J.; Slater-Jefferies, J.L.; Garratt, E.; Crozier, S.R.; et al. Epigenetic gene promoter methylation at birth is associated with child’s later adiposity. Diabetes 2011, 60, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- Markovic, T.P.; Muirhead, R.; Overs, S.; Ross, G.P.; Louie, J.C.; Kizirian, N.; Denyer, G.; Petocz, P.; Hyett, J.; Brand-Miller, J.C.; et al. Randomized controlled trial investigating the effects of a Low-Glycemic Index Diet on Pregnancy Outcomes in Women at High Risk of Gestational Diabetes Mellitus: The GI Baby 3 Study. Diabetes Care 2015, 39, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, L.; Nolan, C.; Wilson, J.D.; Oats, J.J.; Simmons, D. Gestational diabetes mellitus—Management guidelines. The Australasian Diabetes in Pregnancy Society. Med. J. Aust. 1998, 169, 93–97. [Google Scholar] [PubMed]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M. Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; Institute of Medicine and National Research Council: Washington, DC, USA, 2009. [Google Scholar]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar] [PubMed]
- World Health Organization. WHO Anthro for Personal Computers Software. Available online: http://www.who.int/childgrowth/software/en/ (accessed on 1 July 2013).
- Ellis, K.J.; Yao, M.; Shypailo, R.J.; Urlando, A.; Wong, W.W.; Heird, W.C. Body-composition assessment in infancy: Air-displacement plethysmography compared with a reference 4-compartment model. Am. J. Clin. Nutr. 2007, 85, 90–95. [Google Scholar] [PubMed]
- Wells, J.C. A critique of the expression of paediatric body composition data. Arch. Dis. Child. 2001, 85, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C. Toward body composition reference data for infants, children, and adolescents. Adv. Nutr. 2014, 5, 320S–329S. [Google Scholar] [CrossRef] [PubMed]
- Raubenheimer, D.; Simpson, S.J.; Mayntz, D. Nutrition, ecology and nutritional ecology: toward an integrated framework. Funct. Ecol. 2009, 23, 4–16. [Google Scholar] [CrossRef]
- Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; McIntyre, H.D.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.A.; Gerard, L.; Jensen, D.R.; Kealey, E.H.; Hernandez, T.L.; Reece, M.S.; Barbour, L.A.; Bessesen, D.H. Continuous glucose profiles in obese and Normal-Weight Pregnant Women on a Controlled Diet: Metabolic determinants of fetal growth. Diabetes Care 2011, 34, 2198–2204. [Google Scholar] [CrossRef] [PubMed]
- Carberry, A.E.; Raynes-Greenow, C.H.; Turner, R.M.; Askie, L.M.; Jeffery, H.E. Is body fat percentage a better measure of undernutrition in newborns than birth weight percentiles? Pediatr. Res. 2013, 74, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Barker, M.; Robinson, S.; Osmond, C.; Barker, D.J. Birth weight and body fat distribution in adolescent girls. Arch. Dis. Child. 1997, 77, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.B.; Han, S.P.; Zhu, G.Z.; Zhu, C.; Wang, X.J.; Cao, X.G.; Guo, X.R. Birth weight and subsequent risk of obesity: A systematic review and meta-analysis. Obes. Rev. 2011, 12, 525–542. [Google Scholar] [CrossRef] [PubMed]
- Horan, M.K.; McGowan, C.A.; Gibney, E.R.; Donnelly, J.M.; McAuliffe, F.M. Maternal low glycaemic index diet, fat intake and postprandial glucose influences neonatal adiposity—Secondary analysis from the ROLO study. Nutr. J. 2014, 13, 78. [Google Scholar] [CrossRef] [PubMed]
- Ainge, H.; Thompson, C.; Ozanne, S.E.; Rooney, K.B. A systematic review on animal models of maternal high fat feeding and offspring glycaemic control. Int. J. Obes. 2011, 35, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.L.; Hure, A.J.; Macdonald-Wicks, L.; Smith, R.; Collins, C.E. Systematic review and meta-analysis of energy and macronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2012, 70, 322–336. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Yao, M.; Liu, Y.; Lin, A.; Zou, H.; Urlando, A.; Wong, W.W.; Nommsen-Rivers, L.; Dewey, K.G. Validation of a new pediatric air-displacement plethysmograph for assessing body composition in infants. Am. J. Clin. Nutr. 2004, 79, 653–660. [Google Scholar] [PubMed]
- Lof, M. Physical activity pattern and activity energy expenditure in healthy pregnant and non-pregnant Swedish women. Eur. J. Clin. Nutr. 2011, 65, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.M.; Spaaij, C.J.; Goldberg, G.R.; Poppitt, S.D.; van Raaij, J.M.; Totton, M.; Swann, D.; Black, A.E. Energy requirements of pregnant and lactating women. Eur. J. Clin. Nutr. 1996, 50, S82–S110, discussion S10–S11. [Google Scholar] [PubMed]
- Crume, T.L.; Shapiro, A.L.; Brinton, J.T.; Glueck, D.H.; Martinez, M.; Kohn, M.; Harrod, C.; Friedman, J.E.; Dabelea, D. Maternal fuels and metabolic measures during pregnancy and neonatal body composition: The healthy start study. J. Clin. Endocrinol. Metab. 2015, 100, 1672–1680. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age (year) | 34.8 ± 4.3 |
| Pre-pregnancy BMI (kg/m2) | 25.2 ± 5.3 |
| BMI ≥ 25 kg/m2 | 45 (36.0) |
| Ethnicity | |
| Caucasian | 72 (57.6) |
| Asian | 33 (26.4) |
| Others | 20 (16.0) |
| Tertiary education | 95 (76.0) |
| Nulliparous | 59 (47.2) |
| GWG (kg) | 10.9 ± 5.5 |
| IOM weight gain range | |
| Below | 44 (35.8) |
| Within | 51 (41.5) |
| Above | 28 (22.8) |
| Delivery | |
| Vaginal delivery | 89 (71.2) |
| Elective caesarean | 18 (14.4) |
| Emergency caesarean | 18 (14.4) |
| GDM | 38 (30.4) |
| GDM diagnosed | |
| <20 weeks gestation | 20 (16) |
| 26–28 weeks gestation | 18 (14.4) |
| Insulin use | 23 (18.4) |
| HbA1c (%) 1 | 4.9 (0.3) |
| ISI 2 | 9.9 (4.8) |
| Gestational age 3 | 39.6 (38.7, 40.4) |
| Male | 39.2 (35, 42) |
| Female | 39.8 (35.6, 41.5) |
| Sex (male) | 60 (48) |
| Birth weight (kg) | 3.4 ± 0.4 |
| Male | 3.4 ± 0.5 |
| Female | 3.5 ± 0.4 |
| Birth length (cm) 3 | 50.0 (49, 51) |
| Male | 50 (43.5, 55.0) |
| Female | 50.5 (45.0, 57.0) |
| Weight-for-age z-score | 0.2 ± 0.9 |
| Male | 0.0 ± 1.0 |
| Female | 0.4 ± 0.8 |
| Ponderal Index (kg/m3) | 2.7 ± 0.2 |
| Male | 2.7 ± 0.2 |
| Female | 2.7 ± 0.2 |
| %FM 4 | 10.1 ± 3.8 |
| Male | 8.8 ± 3.3 |
| Female | 11.2 ± 3.9 |
| FMI 3,4 | 1.3 (0.9, 1.6) |
| Male | 1.2 ± 0.5 |
| Female | 1.5 ± 0.6 |
| FFMI 4 | 11.6 ± 0.9 |
| Male | 11.8 ± 1.1 |
| Female | 11.5 ± 0.8 |
| Heading | Mid Pregnancy | Late Pregnancy |
|---|---|---|
| n | 96 | 88 |
| Energy (MJ) | 8.8 ± 1.9 | 8.3 ± 1.6 |
| Protein (g) | 100.0 ± 23 | 97.0 ± 28.2 |
| Total fat (g) | 80.6 ± 22.8 | 77.5 ± 24.3 |
| Total carbohydrates (g) | 233.6 ± 64.3 | 210.3 ± 47.0 |
| Sugars (g) | 95.4 ± 36 | 89.0 ± 27.5 |
| Starch (g) | 136.6 ± 48 | 120.0 ± 31.3 |
| Fiber (g) | 25.8 ± 8.3 | 27.0 ± 8.6 |
| P:C ratio | 0.5 ± 0.2 | 0.5 ± 0.2 |
| GI | 57 ± 5 | 54 ± 6 |
| GL | 125 ± 41 | 106 ± 30 |
| Protein (%E) | 19.5 ± 4.1 | 20.0 ± 4.1 |
| Total fat (%E) | 33.6 ± 5.7 | 34.2 ± 6.0 |
| Saturated fat (%E) | 12.7 ± 3.0 | 12.3 ± 3.0 |
| Carbohydrates (%E) | 43.5 ± 6.5 | 42.1 ± 6.4 |
| R2 | Beta | 95% CI | p | |
|---|---|---|---|---|
| FFMI | ||||
| Energy (MJ) | 0.063 | 0.035 | −0.071, −0.141 | 0.517 |
| Protein (%E) | 0.059 | −0.003 | −0.050, 0.043 | 0.883 |
| Total fat (%E) | 0.123 | 0.041 | 0.009, 0.073 | 0.012 |
| Saturated fat (%E) | 0.126 | 0.079 | 0.019, 0.139 | 0.010 |
| Carbohydrates (%E) | 0.104 | −0.030 | −0.057, −0.002 | 0.037 |
| Fiber (%E) | 0.069 | −0.144 | −0.443, 0.154 | 0.339 |
| P:C ratio | 0.067 | 0.471 | −0.569, 1.512 | 0.371 |
| GI | 0.064 | −0.012 | −0.046, 0.023 | 0.503 |
| GL | 0.070 | −0.002 | −0.007, 0.002 | 0.312 |
| FMI | ||||
| Energy (MJ) | 0.073 | 0.046 | −0.017, 0.108 | 0.151 |
| Protein (%E) | 0.075 | −0.021 | −0.048, 0.007 | 0.134 |
| Total fat (%E) | 0.076 | 0.015 | −0.004, 0.034 | 0.131 |
| Saturated fat (%E) | 0.067 | 0.022 | −0.015, 0.059 | 0.235 |
| Carbohydrates (%E) | 0.055 | −0.004 | −0.021, 0.013 | 0.615 |
| Fiber (%E) | 0.059 | 0.074 | −0.104, 0.252 | 0.413 |
| P:C ratio | 0.056 | −0.205 | −0.826, 0.416 | 0.513 |
| GI | 0.052 | 0.002 | −0.019, 0.022 | 0.875 |
| GL | 0.054 | 0.001 | −0.002, 0.003 | 0.643 |
| R2 | Beta | 95% CI | p | |
|---|---|---|---|---|
| FFMI | ||||
| Energy (MJ) | 0.037 | 0.020 | −0.106, 0.147 | 0.750 |
| Protein (%E) | 0.038 | −0.011 | −0.063, 0.041 | 0.681 |
| Total fat (%E) | 0.045 | 0.015 | −0.018, 0.049 | 0.369 |
| Saturated fat (%E) | 0.040 | 0.020 | −0.045, 0.084 | 0.544 |
| Carbohydrates (%E) | 0.047 | −0.017 | −0.051, 0.017 | 0.330 |
| Fiber (%E) | 0.040 | 0.072 | −0.175, 0.319 | 0.564 |
| P:C ratio | 0.036 | 0.126 | −1.098, 1.349 | 0.839 |
| GI | 0.110 | −0.040 | −0.071, −0.010 | 0.010 |
| GL | 0.064 | −0.006 | −0.013, 0.001 | 0.118 |
| FMI | ||||
| Energy (MJ) | 0.079 | 0.026 | −0.049, 0.100 | 0.495 |
| Protein (%E) | 0.073 | −0.003 | −0.034, 0.027 | 0.835 |
| Total fat (%E) | 0.124 | 0.021 | 0.002, 0.040 | 0.032 |
| Saturated fat (%E) | 0.124 | 0.040 | 0.003, 0.077 | 0.033 |
| Carbohydrates (%E) | 0.123 | −0.021 | −0.042, −0.002 | 0.034 |
| Fiber (%E) | 0.084 | 0.070 | −0.074, 0.214 | 0.336 |
| P:C ratio | 0.090 | 0.437 | −0.272, 1.147 | 0.224 |
| GI | 0.073 | 0.001 | −0.018, 0.020 | 0.927 |
| GL | 0.084 | −0.002 | −0.006, 0.002 | 0.322 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kizirian, N.V.; Markovic, T.P.; Muirhead, R.; Brodie, S.; Garnett, S.P.; Louie, J.C.Y.; Petocz, P.; Ross, G.P.; Brand-Miller, J.C. Macronutrient Balance and Dietary Glycemic Index in Pregnancy Predict Neonatal Body Composition. Nutrients 2016, 8, 270. https://doi.org/10.3390/nu8050270
Kizirian NV, Markovic TP, Muirhead R, Brodie S, Garnett SP, Louie JCY, Petocz P, Ross GP, Brand-Miller JC. Macronutrient Balance and Dietary Glycemic Index in Pregnancy Predict Neonatal Body Composition. Nutrients. 2016; 8(5):270. https://doi.org/10.3390/nu8050270
Chicago/Turabian StyleKizirian, Nathalie V., Tania P. Markovic, Roslyn Muirhead, Shannon Brodie, Sarah P. Garnett, Jimmy C. Y. Louie, Peter Petocz, Glynis P. Ross, and Jennie C. Brand-Miller. 2016. "Macronutrient Balance and Dietary Glycemic Index in Pregnancy Predict Neonatal Body Composition" Nutrients 8, no. 5: 270. https://doi.org/10.3390/nu8050270