Clinical Evaluation of Effects of Chronic Resveratrol Supplementation on Cerebrovascular Function, Cognition, Mood, Physical Function and General Well-Being in Postmenopausal Women—Rationale and Study Design



Abstract
:1. Introduction
1.1. Estrogen, Menopause and Dementia
1.2. How Could Resveratrol Benefit Postmenopausal Women?
2. Materials and Methods
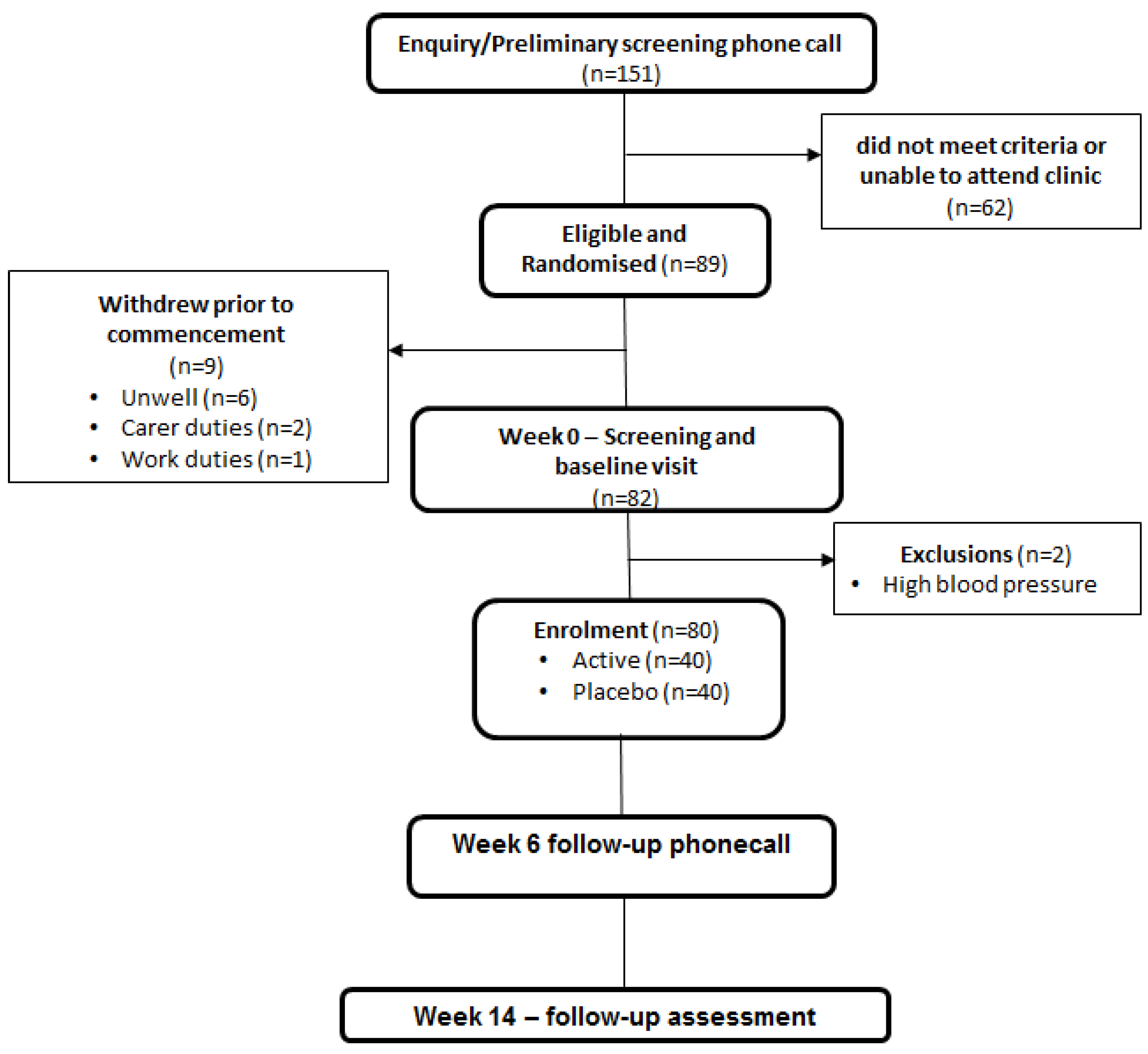
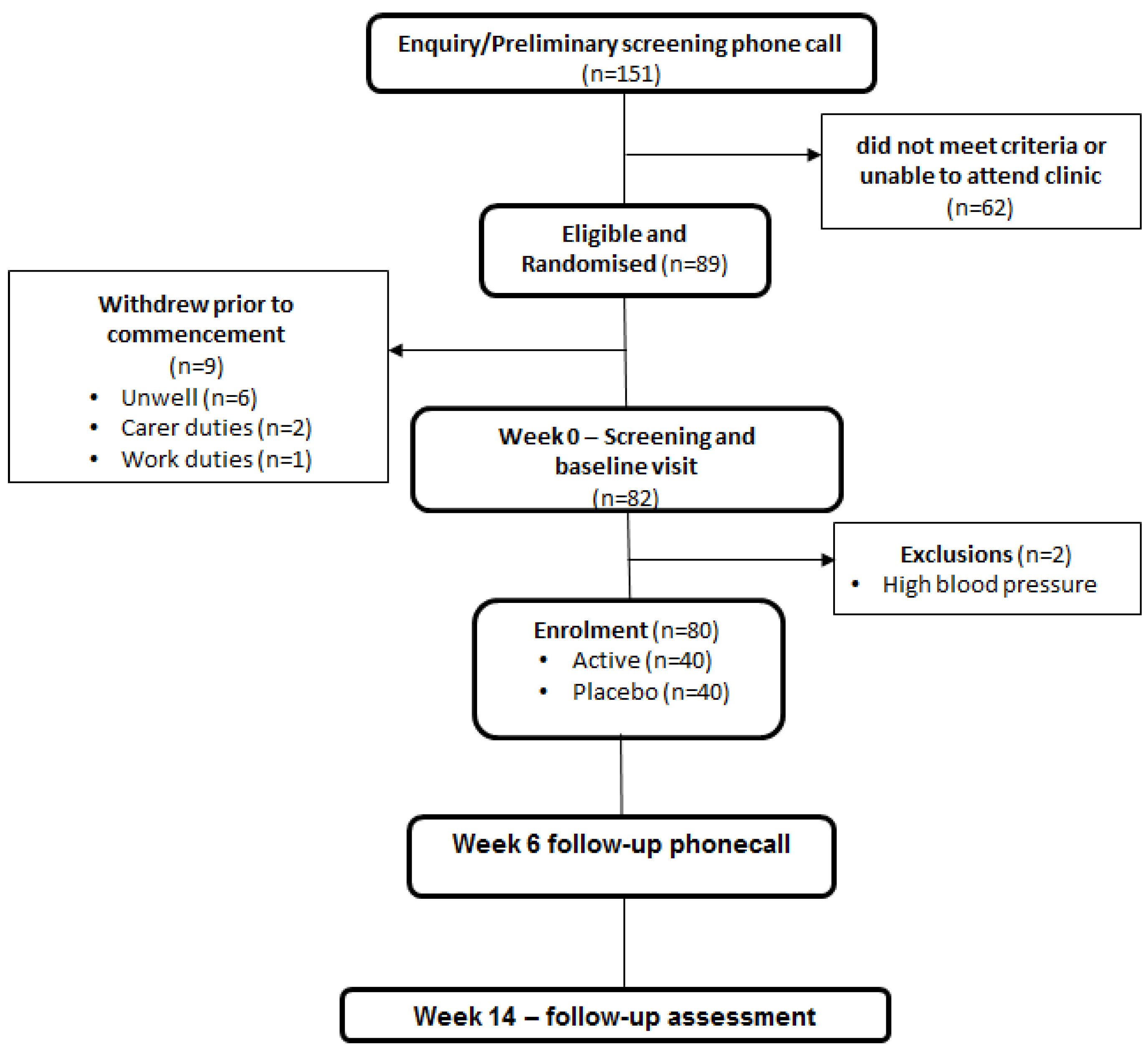
2.1. Study Design
2.2. Study Population
2.3. Investigational Product and Allocation
2.4. Screening/Baseline Visit (Week 0)
2.5. Intervention and Follow-up (Week 0–14)
2.6. End of Intervention Visit (Week 14)
2.7. Outcome Assessments
Clinic Blood Pressure
2.8. Transcranial Doppler Ultrasound Assessements
Basal Cerebral Haemodynamics
2.9. Cerebrovascular Responsiveness
2.10. Cognitive Performance
2.11. Assessment of Mood
2.12. Physical Function Assessment
2.13. Assessment of Overall Well-Being
2.14. Statistical Analysis
3. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ER | estrogen receptors |
| eNOS | endothelial nitric oxide synthase |
| NO | nitric oxide |
| HRT | hormone replacement therapy |
| CVR | cerebrovascular responsiveness |
| BP | blood pressure |
| 3MS | Mini Modified Mental State Examination |
| TCD | transcranial Doppler |
| MCA | middle cerebral artery |
| PCA | posterior cerebral artery |
| PI | pulsatility index |
| RAVLT | Rey Auditory Verbal Learning Test |
| TMT | Trail Making Task |
| POMS | Profile of Mood States |
| CES-D | Center for Epidemiological Studies Depression Scale |
| MRS | menopausal rating scale |
| SF-36 | Short-form 36 |
| ANOVA | analysis of variance |
| ANCOVA | analysis of covariance |
References
- Australian Institute of Health and Welfare. Dementia in Australia; Australian Institute of Health and Welfare: Canberra, Australia, 2012. [Google Scholar]
- Speechly, C.M.; Bridges-Webb, C.; Passmore, E. The pathway to dementia diagnosis. Med. J. Aust. 2008, 189, 487–489. [Google Scholar] [PubMed]
- Hsu, C.L.; Nagamatsu, L.S.; Davis, J.C.; Liu-Ambrose, T. Examining the relationship between specific cognitive processes and falls risk in older adults: A systematic review. Osteoporosis Int. 2012, 23, 2409–2424. [Google Scholar] [CrossRef] [PubMed]
- Genazzani, A.R.; Bernardi, F.; Pluchino, N.; Begliuomini, S.; Lenzi, E.; Casarosa, E.; Luisi, M. Endocrinology of menopausal transition and its brain implications. CNS Spectrums 2005, 10, 449–457. [Google Scholar] [PubMed]
- Genazzani, A.R.; Pluchino, N.; Luisi, S.; Luisi, M. Estrogen, cognition and female ageing. Hum. Reprod. Update 2007, 13, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Jurado, M.B.; Rosselli, M. The elusive nature of executive functions: A review of our current understanding. Neuropsychol. Rev. 2007, 17, 213–233. [Google Scholar] [CrossRef] [PubMed]
- Hogervorst, E.; Williams, J.; Budge, M.; Riedel, W.; Jolles, J. The nature of the effect of female gonadal hormone replacement therapy on cognitive function in post-menopausal women: A meta-analysis. Neuroscience 2000, 101, 485–512. [Google Scholar] [CrossRef]
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; LaCroix, A.Z.; Kooperberg, C.; Stefanick, M.L.; Jackson, R.D.; Beresford, S.A.; Howard, B.V.; Johnson, K.C.; et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the women’s health initiative randomized controlled trial. JAMA 2002, 288, 321–333. [Google Scholar] [PubMed]
- Bagger, Y.Z.; Tanko, L.B.; Alexandersen, P.; Qin, G.R.; Christiansen, C.; Grp, P.S. Early postmenopausal hormone therapy may prevent cognitive impairment later in life. Menopause 2005, 12, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Silvestrini, M.; Pasqualetti, P.; Baruffaldi, R.; Bartolini, M.; Handouk, Y.; Matteis, M.; Moffa, F.; Provinciali, L.; Vernieri, F. Cerebrovascular reactivity and cognitive decline in patients with alzheimer disease. Stroke 2006, 37, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- Kastrup, A.; Dichgans, J.; Niemeier, M.; Schabet, M. Changes of cerebrovascular co2 reactivity during normal aging. Stroke 1998, 29, 1311–1314. [Google Scholar] [CrossRef] [PubMed]
- Greene, R.A. Estrogen and cerebral blood flow: A mechanism to explain the impact of estrogen on the incidence and treatment of alzheimer’s disease. Int. J. Fertil. Women Med. 2000, 45, 253–257. [Google Scholar]
- Maki, P.M.; Resnick, S.M. Longitudinal effects of estrogen replacement therapy on pet cerebral blood flow and cognition. Neurobiol. Aging 2000, 21, 373–383. [Google Scholar] [CrossRef]
- Best, J.R.; Davis, J.C.; Liu-Ambrose, T. Longitudinal analysis of physical performance, functional status, physical activity, and mood in relation to executive function in older adults who fall. J. Am. Geriatr. Soc. 2015, 63, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Sorond, F.A.; Galica, A.; Serrador, J.M.; Kiely, D.K.; Iloputaife, I.; Cupples, L.A.; Lipsitz, L.A. Cerebrovascular hemodynamics, gait, and falls in an elderly population mobilize boston study. Neurology 2010, 74, 1627–1633. [Google Scholar] [CrossRef] [PubMed]
- Sorond, F.A.; Kiely, D.K.; Galica, A.; Moscufo, N.; Serrador, J.M.; Iloputaife, I.; Egorova, S.; Dell’Oglio, E.; Meier, D.S.; Newton, E.; et al. Neurovascular coupling is impaired in slow walkers: The mobilize boston study. Ann. Neurol. 2011, 70, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, F.; Altavilla, D.; Morabito, N.; Crisafulli, A.; D’Anna, R.; Corrado, F.; Ruggeri, P.; Campo, G.M.; Calapai, G.; Caputi, A.P.; et al. The effect of the phytoestrogen genistein on plasma nitric oxide concentrations, endothelin-1 levels and endothelium dependent vasodilation in postmenopausal women. Atherosclerosis 2002, 163, 339–347. [Google Scholar] [CrossRef]
- Beavers, D.P.; Beavers, K.M.; Miller, M.; Stamey, J.; Messina, M.J. Exposure to isoflavone-containing soy products and endothelial function: A bayesian meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Sinn, N.; Buckley, J.D.; Coates, A.M.; Howe, P.R. Soya isoflavone supplementation enhances spatial working memory in men. Br. J. Nutr. 2009, 102, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Utian, W.H.; Jones, M.; Setchell, K.D.R. S-equol: A potential nonhormonal agent for menopause-related symptom relief. J. Womens Health 2015, 24, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.; Elliott, J.G.; Sharma, P.; Berman, R.; Guthrie, N. The effect of synthetic genistein on menopause symptom management in healthy postmenopausal women: A multi-center, randomized, placebo-controlled study. Maturitas 2011, 68, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Nguyen, M.D.; Dobbin, M.M.; Fischer, A.; Sananbenesi, F.; Rodgers, J.T.; Delalle, I.; Baur, J.A.; Sui, G.; Armour, S.M.; et al. Sirt1 deacetylase protects against neurodegeneration in models for alzheimer’s disease and amyotrophic lateral sclerosis. EMBO J. 2007, 26, 3169–3179. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xia, N.; Förstermann, U. Cardiovascular effects and molecular targets of resveratrol. Nitric Oxide 2012, 26, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Klinge, C.M.; Blankenship, K.A.; Risinger, K.E.; Bhatnagar, S.; Noisin, E.L.; Sumanasekera, W.K.; Zhao, L.; Brey, D.M.; Keynton, R.S. Resveratrol and estradiol rapidly activate mapk signaling through estrogen receptors α and β in endothelial cells. J. Biol. Chem. 2005, 280, 7460–7468. [Google Scholar] [CrossRef] [PubMed]
- Bowers, J.L.; Tyulmenkov, V.V.; Jernigan, S.C.; Klinge, C.M. Resveratrol acts as a mixed agonist/antagonist for estrogen receptors α and β. Endocrinology 2000, 141, 3657–3667. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.X.; Berry, N.M.; Coates, A.M.; Buckley, J.D.; Bryan, J.; Kunz, I.; Howe, P.R.C. Chronic resveratrol consumption improves brachial flow-mediated dilatation in healthy obese adults. J. Hypertens. 2013, 31, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.X.; Howe, P.R.C.; Buckley, J.D.; Coates, A.M.; Kunz, I.; Berry, N.M. Acute resveratrol supplementation improves flow-mediated dilatation in overweight/obese individuals with mildly elevated blood pressure. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Witte, A.V.; Kerti, L.; Margulies, D.S.; Floel, A. Effects of resveratrol on memory performance, hippocampal functional connectivity, and glucose metabolism in healthy older adults. J. Neurosci. 2014, 34, 7862–7870. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. Treatment allocation by minimisation. Br. Med. J. 2005, 330, 843–843. [Google Scholar] [CrossRef] [PubMed]
- Bravo, G.; Hebert, R. Age- and education-specific reference values for the mini-mental and modified mini-mental state examinations derived from a non-demented elderly population. Int. J. Geriatr. Psychiatry 1997, 12, 1008–1018. [Google Scholar] [CrossRef]
- Nunes, T.; Almeida, L.; Rocha, J.F.; Falcao, A.; Fernandes-Lopes, C.; Loureiro, A.I.; Wright, L.; Vaz-da-Silva, M.; Soares-da-Silva, P. Pharmacokinetics of trans-resveratrol following repeated administration in healthy elderly and young subjects. J. Clin. Pharmacol. 2009, 49, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed]
- Tegeler, C.H.; Crutchfield, K.; Katsnelson, M.; Kim, J.; Tang, R.; Passmore Griffin, L.; Rundek, T.; Evans, G. Transcranial doppler velocities in a large, healthy population. J. Neuroimaging 2013, 23, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Willie, C.K.; Colino, F.L.; Bailey, D.M.; Tzeng, Y.C.; Binsted, G.; Jones, L.W.; Haykowsky, M.J.; Bellapart, J.; Ogoh, S.; Smith, K.J.; et al. Utility of transcranial doppler ultrasound for the integrative assessment of cerebrovascular function. J. Neurosci. Methods 2011, 196, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary, 3rd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Adlam, A.L.; Patterson, K.; Bozeat, S.; Hodges, J.R. The cambridge semantic memory test battery: Detection of semantic deficits in semantic dementia and alzheimer’s disease. Neurocase 2010, 16, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Lovato, N.; Lack, L.; Wright, H.; Kemps, E.; Cant, M.; Humphreys, J. A preliminary assessment of the reliability and validity of a computerized working memory task. Percept. Mot. Skills 2013, 116, 368–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Cubillo, I.; Perianez, J.A.; Adrover-Roig, D.; Rodriguez-Sanchez, J.M.; Rios-Lago, M.; Tirapu, J.; Barcelo, F. Construct validity of the trail making test: Role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J. Int. Neuropsychol. Soc. 2009, 15, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.; Stanczyk, F.Z.; Dennerstein, L.; Mack, W.J.; Clark, M.S.; Szoeke, C.; Henderson, V.W. Executive functions in recently postmenopausal women: Absence of strong association with serum gonadal steroids. Brain Res. 2011, 1379, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Cui, J.; Shen, Y. Brain sex matters: Estrogen in cognition and alzheimer’s disease. Mol. Cell. Endocrinol. 2014, 389, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Joffe, H.; Hall, J.E.; Gruber, S.; Sarmiento, I.A.; Cohen, L.S.; Yurgelun-Todd, D.; Martin, K.A. Estrogen therapy selectively enhances prefrontal cognitive processes: A randomized, double-blind, placebo-controlled study with functional magnetic resonance imaging in perimenopausal and recently postmenopausal women. Menopause 2006, 13, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Craig, M.C.; Brammer, M.; Maki, P.M.; Fletcher, P.C.; Daly, E.M.; Rymer, J.; Giampietro, V.; Picchioni, M.; Stahl, D.; Murphy, D.G. The interactive effect of acute ovarian suppression and the cholinergic system on visuospatial working memory in young women. Psychoneuroendocrinology 2010, 35, 987–1000. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.; Scholey, A.; Howe, P.R. Assessing premorbid cognitive ability in adults with type 2 diabetes mellitus-a review with implications for future intervention studies. Curr. Diabetes Rep. 2014, 14, 547. [Google Scholar] [CrossRef] [PubMed]
- Wyrwich, K.W.; Yu, H. Validation of poms questionnaire in postmenopausal women. Qual. Life Res. 2011, 20, 1111–1121. [Google Scholar] [CrossRef] [PubMed]
- McCallum, J.; Mackinnon, A.; Simons, L.; Simons, J. Measurement properties of the center for epidemiological studies depression scale: An australian community study of aged persons. J. Gerontol. B Psychol. Sci. Soc. Sci. 1995, 50, S182–S189. [Google Scholar] [CrossRef] [PubMed]
- Avis, N.E.; Brambilla, D.; McKinlay, S.M.; Vass, K. A longitudinal analysis of the association between menopause and depression results from the massachusetts women’s health study. Ann. Epidemiol. 1994, 4, 214–220. [Google Scholar] [CrossRef]
- Reuben, D.B.; Siu, A.L. An objective measure of physical function of elderly outpatients. The physical performance test. J. Am. Geriatr. Soc. 1990, 38, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Revicki, D.A.; Harding, G.; Coyne, K.S.; Peirce-Sandner, S.; Bhagwat, D.; Everton, D.; Burke, L.B.; Cowan, P.; et al. Development and initial validation of an expanded and revised version of the short-form mcgill pain questionnaire (sf-mpq-2). Pain 2009, 144, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Heinemann, K.; Ruebig, A.; Potthoff, P.; Schneider, H.P.; Strelow, F.; Heinemann, L.A.; Do, M.T. The menopause rating scale (mrs) scale: A methodological review. Health Qual. Life Outcomes 2004, 2, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, G.; Schofield, M.J. Norms for the physical and mental health component summary scores of the sf-36 for young, middle-aged and older australian women. Qual. Life Res. 1998, 7, 215–220. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Inclusion Criteria |
|---|
|
| Exclusion criteria |
|
| Cognitive Test & Domains | Procedure | Scoring |
|---|---|---|
| RAVLT (immediate and long-term verbal memory) | Immediate: The participants were required to listen to an electronic audio containing 15 nouns (list A) presented at a rate of 1 word/2 s. After the audio was played, participants were required to verbally recall the words irrespective of order (trial A1). The list was presented a further four times (trial A2-A5). A second interference list (list B) was presented in the same manner (trial B6). Immediately afterward trial B6 participants were instructed to recall all the words from list A without prompt (trial A7). | Scaled scores = raw scores − errors |
| Learning = scaled total (Trials A1-A5). | ||
| Proactive memory = scaled Trial B6. | ||
| Delayed: participants performed other tasks for 20 min before being required to recall all 15 words from list A (trial A8). Participants were then provided with a sheet containing all 15 words from both list A and B as well as 20 words similar in either phonology or semantic terms (total 50 words) and required to correctly identify words from both list A and list B. | ||
| Retroactive interference = scaled trial A7-scaled trial A5. | ||
| For each trial, number of errors was also recorded. | ||
| Delayed recall = scaled trial A8. | ||
| Recognition = Z-score list A + Z-score list B + Z-score Errors | ||
| Cambridge Semantic Memory Battery (semantic memory) | Category fluency: Participants were given 1 min to give as many items within a given category as they could. 8 categories were used, separated into living (animals, fruits, Birds, breed of dogs) and non-living (household items, tools, vehicles, types of boats) | Number of correct responses overall. |
| As per category fluency. | ||
| Letter fluency: Participants were given 1 min to give as many words as they could starting with a given letter. Letters used were F, A and S. Proper nouns were excluded. | ||
| Naming: participants were required to correctly name 64 images of common living and non-living items, presented one by one. | ||
| As per category fluency. | ||
| Category Comprehension: Participants were read the names of 64 items and required to correctly identify each from groups of images closely related to the stimuli. | ||
| Semantic Association (camel and cactus): Participants were shown an item and must correctly identify, from a separate group of 4 items, the item that is best associated with the first. | ||
| As per category fluency. | ||
| As per category fluency. | ||
| Double Span Task (visuospatial working memory) | 14 different objects were used in this task. For each task, a random number of objects (max = 5) displayed in random positions on 4 × 4 grid. Participants were prompted to either recall positions (point to position of each object in the order they were presented) or positions and names (point to the position of each object in the order they were presented saying the name of each object verbally) in an empty grid after a 5 s delay. | “Positions” = number of each correct position in order. |
| “Position and names” as per “positions” with an additional mark for each correct name in order. | ||
| Marks were then tallied for an overall score. | ||
| Trail Making Task (executive function and processing speed) | Trial A: Participants were required to draw a continuous line connecting 25 numbers spread randomly across the page in ascending order. | Trial A and B = Time taken, errors |
| Trial B: Participants were required to draw a continuous line alternating between numbers and letters (1,a,2,b,3,c, etc.) spread randomly across the page | Interference = time taken (trial B/Trial A) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, H.M.; Howe, P.R.C.; Wong, R.H.X. Clinical Evaluation of Effects of Chronic Resveratrol Supplementation on Cerebrovascular Function, Cognition, Mood, Physical Function and General Well-Being in Postmenopausal Women—Rationale and Study Design. Nutrients 2016, 8, 150. https://doi.org/10.3390/nu8030150
Evans HM, Howe PRC, Wong RHX. Clinical Evaluation of Effects of Chronic Resveratrol Supplementation on Cerebrovascular Function, Cognition, Mood, Physical Function and General Well-Being in Postmenopausal Women—Rationale and Study Design. Nutrients. 2016; 8(3):150. https://doi.org/10.3390/nu8030150
Chicago/Turabian StyleEvans, Hamish Michael, Peter Ranald Charles Howe, and Rachel Heloise Xiwen Wong. 2016. "Clinical Evaluation of Effects of Chronic Resveratrol Supplementation on Cerebrovascular Function, Cognition, Mood, Physical Function and General Well-Being in Postmenopausal Women—Rationale and Study Design" Nutrients 8, no. 3: 150. https://doi.org/10.3390/nu8030150