Causes, Consequences and Public Health Implications of Low B-Vitamin Status in Ageing


Abstract
:1. Introduction
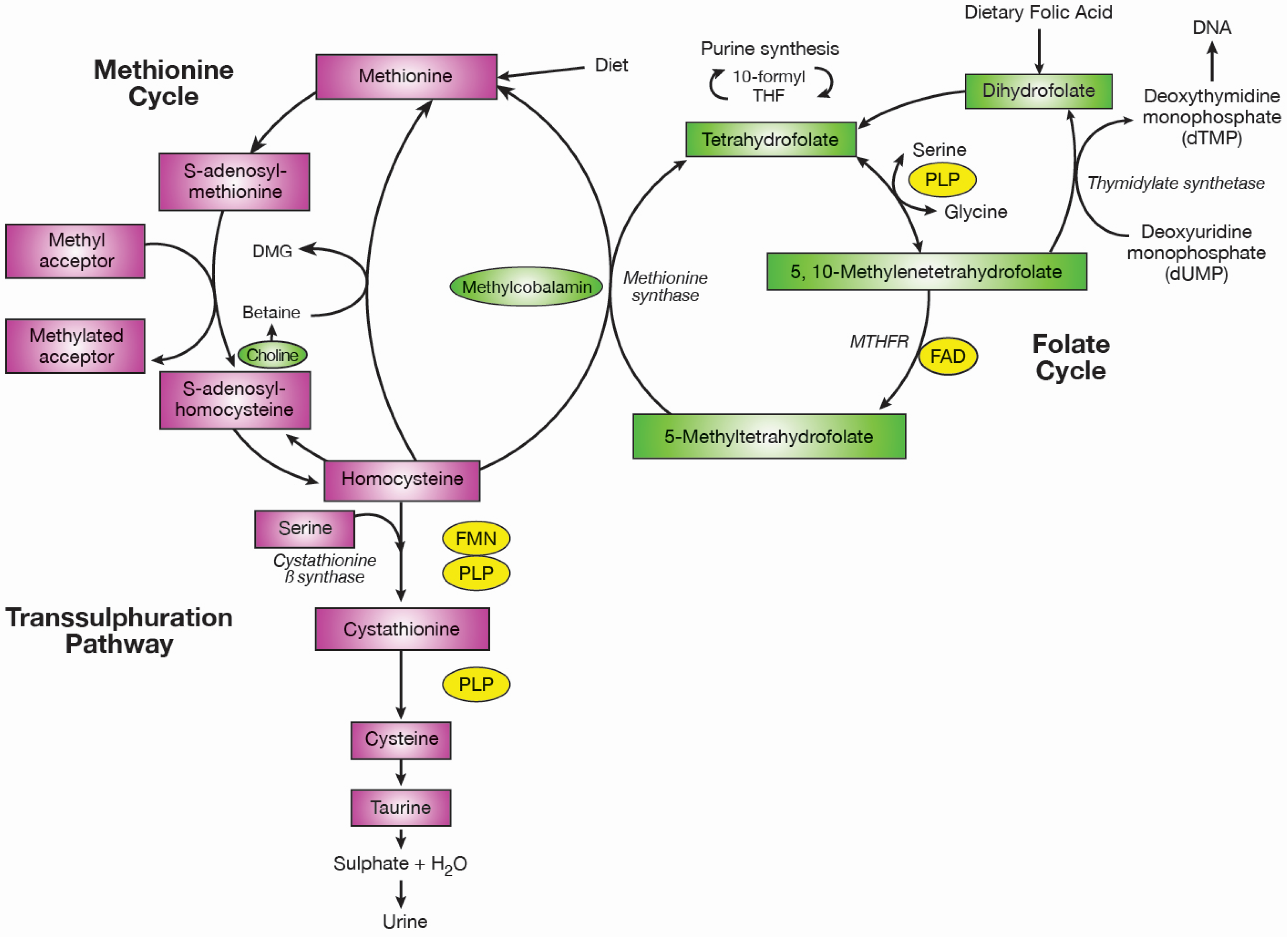
2. Metabolic Role of B-Vitamins in One-Carbon Metabolism
3. Causes of B-Vitamin Deficiency
4. Assessment of B-Vitamin Biomarker Status
5. Consequences of B-Vitamin Deficiency
6. Emerging Roles of B-Vitamin Status in Preventing Diseases of Ageing
6.1. Cardiovascular Health in Ageing
6.2. Bone Health in Ageing
6.3. Brain Health in Ageing
Cognitive Dysfunction
6.4. Future Directions
7. Potential Mechanisms Linking B-Vitamins with Diseases of Ageing
8. Public Health Implications
9. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Beard, J.R.; Bloom, D.E. Towards a comprehensive public health response to population ageing. Lancet 2015, 385, 658–661. [Google Scholar] [CrossRef]
- Prince, M.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- A Global Brief on Hypertension. Available online: http://ish-world.com/news/a/World-Health-Organization-A-Global-Brief-on-Hypertension/ (accessed on 1 August 2016).
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.-T.; Prina, M.; International, A.D. World Alzheimer’s Report—The Global Impact of Dementia; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Selhub, J. Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J. Nutr. Health Aging 2002, 6, 39–42. [Google Scholar] [PubMed]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- McGarel, C.; Pentieva, K.; Strain, J.J.; McNulty, H. Emerging roles for folate and related B-vitamins in brain health across the lifecycle. Proc. Nutr. Soc. 2015, 74, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Molloy, A. Folate-vitamin B12 interrelationships; links to disease risk. In Folate in Health and Disease, 2nd ed.; Bailey, L., Ed.; CRC Press: Boca Raton, FL, USA, 2010; pp. 381–408. [Google Scholar]
- Scott, J.; Weir, D. The methyl folate trap: A physiological response in man to prevent methyl group deficiency in kwashiorkor (methionine deficiency) and an explanation for folic-acid-induced exacerbation of subacute combined degeneration in pernicious anaemia. Lancet 1981, 318, 337–340. [Google Scholar] [CrossRef]
- Brachet, P.; Chanson, A.; Demigne, C.; Batifoulier, F.; Alexandre-Gouabau, M.C.; Tyssandier, V.; Rock, E. Age-associated B vitamin deficiency as a determinant of chronic diseases. Nutr. Res. Rev. 2004, 17, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Araujo, J.R.; Martel, F.; Borges, N.; Araujo, J.M.; Keating, E. Folates and aging: Role in mild cognitive impairment, dementia and depression. Ageing Res. Rev. 2015, 22, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.; Parnell, L.D.; Troen, A.M.; Shen, J.; Caouette, H.; Warodomwichit, D.; Lee, Y.; Crott, J.W.; Qiu, W.Q.; Rosenberg, I.H.; et al. MAT1A variants are associated with hypertension, stroke, and markers of DNA damage and are modulated by plasma vitamin B-6 and folate. Am. J. Clin. Nutr. 2010, 91, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Wilcken, B.; Bamforth, F.; Li, Z.; Zhu, H.; Ritvanen, A.; Redlund, M.; Stoll, C.; Alembik, Y.; Dott, B.; Czeizel, A.E.; et al. Geographical and ethnic variation of the 677C > T allele of 5,10-methylenetetrahydrofolate reductase (MTHFR): Findings from over 7000 newborns from 16 areas Worldwide. J. Med. Genet. 2003, 40, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Reilly, R.; Hopkins, S.; Ward, M.; McNulty, H.; McCann, A.; McNulty, B.; Walton, J.; Molloy, A.; Strain, J.J.; Flynn, A.; et al. MTHFR 677TT genotype and related B-vitamins: Novel determinants of hypertension in healthy Irish adults. J. Inherit. Metab. Dis. 2013, 36, 35. [Google Scholar]
- Clarke, M.; Ward, M.; Dickey, W.; Hoey, L.; Molloy, A.M.; Waldron, L.; Varghese, A.; McCann, A.; Blayney, J.K.; McNulty, H. B-vitamin status in relation to bone mineral density in treated celiac disease patients. Scand. J. Gastroenterol. 2015, 50, 975–984. [Google Scholar] [CrossRef] [PubMed]
- Ter Borg, S.; Verlaan, S.; Hemsworth, J.; Mijnarends, D.M.; Schols, J.M.G.A.; Luiking, Y.C.; De Groot, L.C.P.G.M. Micronutrient intakes and potential inadequacies of community-dwelling older adults: A systematic review. Br. J. Nutr. 2015, 113, 1195–1206. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.; Lennox, A.; Bates, C. National Diet and Nutrition Survey: Results from Years 1–4 (Combined) of the Rolling Programme (2008/2009–2011/12); Public Health England: London, UK, 2014.
- Lindenbaum, J.; Allen, R. Clinical spectrum and diagnosis of folate deficiency. In Folate in Health and Disease, 2nd ed.; Bailey, L., Ed.; CRC Press: London, UK, 2009; pp. 43–67. [Google Scholar]
- Bailey, L.B.; Stover, P.J.; McNulty, H.; Fenech, M.F.; Gregory, J.F., III; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.; Ueland, P.M.; et al. Biomarkers of Nutrition for Development-Folate Review. J. Nutr. 2015, 145, 1636–1680. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R. Assessment status of riboflavin, B6, folate and B12 status. In Principles of Nutritional Assessment, 2nd ed.; Oxford University: New York, NY, USA, 2005; pp. 554–562, 575–640. [Google Scholar]
- Carmel, R.; Jacobsen, D. (Eds.) Homocysteine in Health and Disease; Cambridge University Press: Cambridge, UK, 2001.
- Selhub, J.; Jacques, P.F.; Bostom, A.G.; Wilson, P.W.; Rosenberg, I.H. Relationship between plasma homocysteine and vitamin status in the Framingham study population. Impact of folic acid fortification. Public Health Rev. 2000, 28, 117–145. [Google Scholar] [PubMed]
- McKillop, D.; Pentieva, K.; Daly, D.; McPartlin, J.; Hughes, J.; Strain, J.; Scott, J.; McNulty, H. The effect of different cooking methods on folate retention in various foods that are amongst the major contributors to folate intake in the UK diet. Br. J. Nutr. 2002, 88, 681–688. [Google Scholar] [CrossRef] [PubMed]
- McNulty, H.; Scott, J.M. Intake and status of folate and related B-vitamins: Considerations and challenges in achieving optimal status. Br. J. Nutr. 2008, 99, S48–S54. [Google Scholar] [CrossRef] [PubMed]
- Selhub, J.; Bagley, L.C.; Miller, J.; Rosenberg, I.H. B vitamins, homocysteine, and neurocognitive function in the elderly. Am. J. Clin. Nutr. 2000, 71, 614S–620S. [Google Scholar] [PubMed]
- Powers, H.J. Riboflavin (vitamin B-2) and health. Am. J. Clin. Nutr. 2003, 77, 1352–1360. [Google Scholar] [PubMed]
- Allen, L.H. How common is vitamin B-12 deficiency? Am. J. Clin. Nutr. 2009, 89, 693S–696S. [Google Scholar] [CrossRef] [PubMed]
- Refsum, H.; Yajnik, C.S.; Gadkari, M.; Schneede, J.; Vollset, S.E.; Orning, L.; Guttormsen, A.B.; Joglekar, A.; Sayyad, M.G.; Ulvik, A.; et al. Hyperhomocysteinemia and elevated methylmalonic acid indicate a high prevalence of cobalamin deficiency in Asian Indians. Am. J. Clin. Nutr. 2001, 74, 233–241. [Google Scholar] [PubMed]
- Antony, A.C. Prevalence of cobalamin (vitamin B-12) and folate deficiency in India—Audi alteram partem. Am. J. Clin. Nutr. 2001, 74, 233–241. [Google Scholar]
- Clarke, R.; Refsum, H.; Birks, J.; Evans, J.G.; Johnston, C.; Sherliker, P.; Ueland, P.M.; Schneede, J.; McPartlin, J.; Nexo, E.; et al. Screening for vitamin B-12 and folate deficiency in older persons. Am. J. Clin. Nutr. 2003, 77, 1241–1247. [Google Scholar] [PubMed]
- Clarke, R.; Sherliker, P.; Hin, H.; Nexo, E.; Hvas, A.M.; Schneede, J.; Birks, J.; Ueland, P.M.; Emmens, K.; Scott, J.M.; et al. Detection of vitamin B-12 deficiency in older people by measuring vitamin B-12 or the active fraction of vitamin B-12, holotranscobalamin. Clin. Chem. 2007, 53, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Grimley Evans, J.; Schneede, J.; Nexo, E.; Bates, C.; Fletcher, A.; Prentice, A.; Johnston, C.; Ueland, P.M.; Refsum, H.; et al. Vitamin B12 and folate deficiency in later life. Age Ageing 2004, 33, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.M.; Caudill, S.P.; Gunter, E.W.; Osterloh, J.; Sampson, E.J. Biochemical indicators of B vitamin status in the US population after folic acid fortification: Results from the National Health and Nutrition Examination Survey 1999–2000. Am. J. Clin. Nutr. 2005, 82, 442–450. [Google Scholar] [PubMed]
- Pfeiffer, C.M.; Johnson, C.L.; Jain, R.B.; Yetley, E.A.; Picciano, M.F.; Rader, J.I.; Fisher, K.D.; Mulinare, J.; Osterloh, J.D. Trends in blood folate and vitamin B-12 concentrations in the United States, 1988–2004. Am. J. Clin. Nutr. 2007, 86, 718–727. [Google Scholar] [PubMed]
- MacFarlane, A.J.; Greene-Finestone, L.S.; Shi, Y. Vitamin B-12 and homocysteine status in a folate-replete population: Results from the Canadian Health Measures Survey. Am. J. Clin. Nutr. 2011, 94, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Green, T.J.; Venn, B.J.; Skeaff, C.M.; Williams, S.M. Serum vitamin B-12 concentrations and atrophic gastritis in older New Zealanders. Eur. J. Clin. Nutr. 2005, 59, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Loikas, S.; Koskinen, P.; Irjala, K.; Lopponen, M.; Isoaho, R.; Kivela, S.; Pelliniemi, T. Vitamin B12 deficiency in the aged: A population-based study. Age Ageing 2007, 36, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Carmel, R. Cobalamin, the stomach, and aging. Am. J. Clin. Nutr. 1997, 66, 750–759. [Google Scholar] [PubMed]
- Hughes, C.F.; Ward, M.; Hoey, L.; McNulty, H. Vitamin B-12 and ageing: Current issues and interaction with folate. Ann. Clin. Biochem. 2013, 50, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Van Asselt, D.Z.B.; De Groot, L.C.P.G.M.; Van Staveren, W.A.; Blom, H.J.; Wevers, R.A.; Biemond, I.; Hoefnagels, W.H.L. Role of cobalamin intake and atrophic gastritis in mild cobalamin deficiency in older Dutch subjects. Am. J. Clin. Nutr. 1998, 68, 328–334. [Google Scholar] [PubMed]
- Hannibal, L.; Lysne, V.; Bjørke-Monsen, A.L.; Behringer, S.; Grünert, S.C.; Spiekerkoetter, U.; Jacobsen, D.W.; Blom, H.J. Biomarkers and algorithms for the diagnosis of vitamin B12 deficiency. Front. Mol. Biosci. 2016, 3, 27. [Google Scholar] [CrossRef] [PubMed]
- Valuck, R.J.; Ruscin, J.M. A case-control study on adverse effects: H2 blocker or proton pump inhibitor use and risk of vitamin B-12 deficiency in older adults. J. Clin. Epidemiol. 2004, 57, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Masclee, G.M.C.; Sturkenboom, M.C.J.M.; Kuipers, E.J. A Benefit-Risk Assessment of the Use of Proton Pump Inhibitors in the Elderly. Drugs Aging 2014, 31, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.R.; Schneider, J.L.; Zhao, W.; Corley, D.A. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B-12 deficiency. JAMA 2013, 310, 2435–2442. [Google Scholar] [CrossRef] [PubMed]
- Chapman, L.E.; Darling, A.L.; Brown, J.E. Association between metformin and vitamin B12 deficiency in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aroda, V.R.; Edelstein, S.L.; Goldberg, R.B.; Knowler, W.C.; Marcovina, S.M.; Orchard, T.J.; Bray, G.A.; Schade, D.S.; Temprosa, M.G.; White, N.H.; et al. Long-term metformin use and vitamin B12 deficiency in the diabetes prevention program outcomes study. J. Clin. Endocrinol. Metab. 2016, 101, 1754–1761. [Google Scholar] [CrossRef] [PubMed]
- Haller, J. The vitamin status and its adequacy in the elderly: An international overview. Int. J. Vitam. Nutr. Res. 1999, 69, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.; Pentieva, K.; Prentice, A.; Mansoor, M.; Finch, S. Plasma pyridoxal phosphate and pyridoxic acid and their relationship to plasma homocysteine in a representative sample of British men and women aged 65 years and over. Br. J. Nutr. 1999, 81, 191–201. [Google Scholar] [PubMed]
- Morris, M.S.; Picciano, M.F.; Jacques, P.F.; Selhub, J. Plasma pyridoxal 5′-phosphate in the US population: The National Health and Nutrition Examination Survey, 2003–2004. Am. J. Clin. Nutr. 2008, 87, 1446–1454. [Google Scholar] [PubMed]
- Ribayamercado, J.; Russell, R.; Sahyoun, N.; Morrow, F.; Gershoff, S. Vitamin-B6 requirements of elderly men and women. J. Nutr. 1991, 121, 1062–1074. [Google Scholar]
- Van Den Berg, H. Vitamin B6 status and requirements in older adults. Br. J. Nutr. 1999, 81, 175–176. [Google Scholar] [PubMed]
- Troesch, B.; Hoeft, B.; McBurney, M.; Eggersdorfer, M.; Weber, P. Dietary surveys indicate vitamin intakes below recommendations are common in representative Western countries. Br. J. Nutr. 2012, 108, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.; Cox, L.; Page, S.; Prentice, A.; Steer, T.; Swan, G. National Diet and Nutrition Survey: Results from Years 5 and 6 (Combined) of the Rolling Programme (2012/2013–2013/2014); Public Health England: London, UK, 2016.
- Walton, J.; Flynn, A. NANS: Food and Nutrient Intakes, Physical Measurements, Physical Activity Patterns and Food Choice Motives; Irish Universities Nutrition Alliance: Dublin, Ireland, 2011; pp. 1–40. [Google Scholar]
- Eussen, S.J.P.M.; De Groot, C.P.G.M.; Clarke, R.; Schneede, J.; Ueland, P.M.; Hoefnagels, W.H.L.; Van Staveren, W.A. Oral cyanocobalamin supplementation in older people with vitamin B-12 deficiency—A dose-finding trial. Arch. Intern. Med. 2005, 165, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- McKinley, M.C.; McNulty, H.; McPartlin, J.; Strain, J.J.; Pentieva, K.; Ward, M.; Weir, D.G.; Scott, J.M. Low-dose vitamin B-6 effectively lowers fasting plasma homocysteine in healthy elderly persons who are folate and riboflavin replete. Am. J. Clin. Nutr. 2001, 73, 759–764. [Google Scholar] [PubMed]
- McNulty, H.; Dowey, L.R.C.; Strain, J.J.; Dunne, A.; Ward, M.; Molloy, A.M.; McAnena, L.B.; Hughes, J.P.; Hannon-Fletcher, M.; Scott, J.M. Riboflavin lowers homocysteine in individuals homozygous for the MTHFR 677C → T polymorphism. Circulation 2006, 113, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.; Fazili, Z.; Zhang, M. Folate analytical methodology. In Folate in Health and Disease, 2nd ed.; Bailey, L.B., Ed.; CRC Press: Boca Raton, FL, USA, 2010; pp. 517–574. [Google Scholar]
- Mason, J.B. Biomarkers of nutrient exposure and status in one-carbon (methyl) metabolism. J. Nutr. 2003, 133, 941S–947S. [Google Scholar] [PubMed]
- Clifford, A.J.; Noceti, E.M.; Block-Joy, A.; Block, T.; Block, G. Erythrocyte folate and its response to folic acid supplementation is assay dependent in women. J. Nutr. 2005, 135, 137–143. [Google Scholar] [PubMed]
- Wu, A.; Chanarin, I.; Slavin, G.; Levi, A.J. Folate-Deficiency in alcoholic—Relationship to clinical and hematological abnormalities, liver-disease and folate stores. Br. J. Haematol. 1975, 29, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.E.; Hoey, L.; Hughes, C.F.; Strain, J.J.; Rankin, A.; Souverein, O.W.; Dullemeijer, C.; Collings, R.; Hooper, L.; McNulty, H. Biomarker responses to folic acid intervention in healthy adults: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2014, 99, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Carmel, R. Current concepts in cobalamin deficiency. Annu. Rev. Med. 2000, 51, 357–375. [Google Scholar] [CrossRef] [PubMed]
- Lindenbaum, J.; Rosenberg, I.H.; Wilson, P.W.F.; Stabler, S.P.; Allen, R.H. Prevalence of cobalamin deficiency in the Framingham elderly population. Am. J. Clin. Nutr. 1994, 60, 2–11. [Google Scholar] [PubMed]
- Naurath, H.J.; Joosten, E.; Riezler, R.; Stabler, S.P.; Allen, R.H.; Lindenbaum, J. Effects of vitamin-B12, folate, and vitamin-B6 supplements in elderly people with normal serum vitamin concentrations. Lancet 1995, 346, 85–89. [Google Scholar] [CrossRef]
- Carmel, R.; Green, R.; Jacobsen, D.W.; Rasmussen, K.; Florea, M.; Azen, C. Serum cobalamin, homocysteine, and methylmalonic acid concentrations in a multiethnic elderly population: Ethnic and sex differences in cobalamin and metabolite abnormalities. Am. J. Clin. Nutr. 1999, 70, 904–910. [Google Scholar] [PubMed]
- Riedel, B.M.; Molloy, A.M.; Meyer, K.; Fredriksen, A.; Ulvik, A.; Schneede, J.; Nexo, E.; Hoff, G.; Ueland, P.M. Transcobalamin Polymorphism 67A → G, but Not 776C → G, Affects serum holotranscobalamin in a cohort of healthy middle-aged men and women. J. Nutr. 2011, 141, 1784–1790. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Azar, D.; Yun, Y.; Ghausi, O.; Ix, J.; Fitzgerald, R.L. Serum methylmalonic Acid and holotranscobalamin-II as markers for vitamin b12 deficiency in end-stage renal disease patients. Ann. Clin. Lab. Sci. 2013, 43, 243–249. [Google Scholar] [PubMed]
- Carmel, R. Biomarkers of cobalamin (vitamin B-12) status in the epidemiologic setting: A critical overview of context, applications, and performance characteristics of cobalamin, methylmalonic acid, and holotranscobalamin II. Am. J. Clin. Nutr. 2011, 94, 348S–358S. [Google Scholar] [CrossRef] [PubMed]
- Leklem, J.E. Vitamin-B6—A status-report. J. Nutr. 1990, 120, 1503–1507. [Google Scholar] [PubMed]
- Ueland, P.M.; Ulvik, A.; Rios-Avila, L.; Midttun, O.; Gregory, J.F. Direct and functional biomarkers of vitamin b6 status. Annu. Rev. Nutr. 2015, 35, 33–70. [Google Scholar] [CrossRef] [PubMed]
- Chiang, E.P.; Smith, D.E.; Selhub, J.; Dallal, G.; Wang, Y.C.; Roubenoff, R. Inflammation causes tissue-specific depletion of vitamin B-6. Arthritis Res. Ther. 2005, 7, R1254–R1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoey, L.; McNulty, H.; Strain, J.J. Studies of biomarker responses to intervention with riboflavin: A systematic review. Am. J. Clin. Nutr. 2009, 89, 1960S–1980S. [Google Scholar] [CrossRef] [PubMed]
- Yetley, E.A.; Johnson, C.L. Folate and vitamin B-12 biomarkers in NHANES: History of their measurement and use. Am. J. Clin. Nutr. 2011, 94, 322S–331S. [Google Scholar] [CrossRef] [PubMed]
- Hoey, L.; Strain, J.J.; McNulty, H. Studies of biomarker responses to intervention with vitamin B-12: A systematic review of randomized controlled trials. Am. J. Clin. Nutr. 2009, 89, 1981S–1996S. [Google Scholar] [CrossRef] [PubMed]
- Bisp, M.R.; Bor, M.V.; Heinsvig, E.M.; Kall, M.A.; Nexo, E. Determination of vitamin B6 vitamers and pyridoxic acid in plasma: Development and evaluation of a high-performance liquid chromatographic assay. Anal. Biochem. 2002, 305, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Apeland, T.; Mansoor, M.A.; Pentieva, K.; McNulty, H.; Strandjord, R.E. Fasting and post-methionine loading concentrations of homocysteine, vitamin B2, and vitamin B6 in patients on antiepileptic drugs. Clin. Chem. 2003, 49, 1005–1008. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, E. Vitamin B12, folic acid, and the nervous system. Lancet Neurol. 2006, 5, 949–960. [Google Scholar] [CrossRef]
- Scott, J.; Weir, D. Folate/vitamin B12 inter-relationships. Essays Biochem. 1994, 28, 63–72. [Google Scholar] [PubMed]
- Healton, E.; Brust, J.; Garrett, T.; Lindenbaum, J. Neurologic aspects of coabalmin deficiency. Medicine 1991, 70, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Rampersaud, G.C.; Kauwell, G.P.A.; Bailey, L.B. Folate: A key to optimizing health and reducing disease risk in the elderly. J. Am. Coll. Nutr. 2003, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke: A meta-analysis. JAMA 2002, 288, 2015–2022. [Google Scholar]
- Wald, D.S.; Law, M.; Morris, J.K. Homocysteine and cardiovascular disease: Evidence on causality from a meta-analysis. Br. Med. J. 2002, 325, 1202K–1206K. [Google Scholar] [CrossRef]
- Smith, D.A.; Refsum, H. Homocysteine, B Vitamins, and Cognitive Impairment. Annu. Rev. Nutr. 2016, 36, 211–239. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Morris, J.K.; Wald, N.J. Reconciling the Evidence on Serum Homocysteine and Ischaemic Heart Disease: A Meta-Analysis. PLoS ONE 2011, 6, e16473. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Kasturiratne, A.; Simmonds, M. Serum homocysteine and dementia: Meta-analysis of eight cohort studies including 8669 participants. Alzheimer’s Dement. 2011, 7, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Lee, M.; Hong, K.; Ovbiagele, B.; Saver, J.L. Efficacy of folic acid supplementation in cardiovascular disease prevention: An updated meta-analysis of randomized controlled trials. Eur. J. Intern. Med. 2012, 23, 745–754. [Google Scholar] [CrossRef] [PubMed]
- Enneman, A.W.; Swart, K.M.; Van Wijngaarden, J.P.; Zillikens, M.C.; Dhonukshe-Rutten, R.A.; De Groot, L.C.; Van Schoor, N.M.; Lips, P.; Van Meurs, J.B.; Uitterlinden, A.G.; et al. Association between plasma homocysteine and bone density and quality parameters in the elderly. Bone 2012, 50, S134. [Google Scholar] [CrossRef]
- McNulty, H.; Strain, J.J.; Pentieva, K.; Ward, M. C-1 metabolism and CVD outcomes in older adults. Proc. Nutr. Soc. 2012, 71, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Toole, J.F.; Malinow, M.R.; Chambless, L.E.; Spence, J.D.; Pettigrew, L.C.; Howard, V.J.; Sides, E.G.; Wang, C.; Stampfer, M. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death: The Vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial. JAMA 2004, 291, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Bonaa, K.H.; Njolstad, I.; Ueland, P.M.; Schirmer, H.; Tverdal, A.; Steigen, T.; Wang, H.; Nordrehaug, J.E.; Arnesen, E.; Rasmussen, K. Homocysteine lowering and cardiovascular events after acute myocardial infarction. N. Engl. J. Med. 2006, 354, 1578–1588. [Google Scholar] [CrossRef] [PubMed]
- Lonn, E.; Yusuf, S.; Arnold, M.J.; Sheridan, P.; Pogue, J.; Micks, M.; McQueen, M.J.; Probstfield, J.; Fodor, G.; Held, C.; et al. Homocysteine lowering with folic acid and B vitamins in vascular disease. N. Engl. J. Med. 2006, 354, 1567–1577. [Google Scholar] [PubMed]
- Albert, C.M.; Cook, N.R.; Gaziano, J.M.; Zaharris, E.; MacFadyen, J.; Danielson, E.; Buring, J.E.; Manson, J.E. Effect of folic acid and B vitamins on risk of cardiovascular events and total mortality among women at high risk for cardiovascular disease: A randomized trial. JAMA 2008, 299, 2027–2036. [Google Scholar] [CrossRef] [PubMed]
- Ebbing, M.; Bleie, O.; Ueland, P.M.; Nordrehaug, J.E.; Nilsen, D.W.; Vollset, S.E.; Refsum, H.; Pedersen, E.K.R.; Nygard, O. Mortality and cardiovascular events in patients treated with homocysteine-lowering B vitamins after coronary angiography—A Randomized controlled trial. JAMA 2008, 300, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J.; Eikelboom, J.W.; Baker, R.I.; Gelavis, A.; Hickling, S.C.; Jamrozik, K.; Van Bockxmeer, F.M.; Vasikaran, S.; Hankey, G.J.; Chen, C.; et al. B vitamins in patients with recent transient ischaemic attack or stroke in the VITAmins TO Prevent Stroke (VITATOPS) trial: A randomised, double-blind, parallel, placebo-controlled trial. Lancet Neurol. 2010, 9, 855–865. [Google Scholar]
- Clarke, R.; Bennett, D.A.; Parish, S.; Verhoef, P.; Dotsch-Klerk, M.; Lathrop, M.; Xu, P.; Nordestgaard, B.G.; Holm, H.; Hopewell, J.C.; et al. Homocysteine and Coronary Heart Disease: Meta-analysis of MTHFR Case-Control Studies, Avoiding Publication Bias. PLoS Med. 2012, 9, e1001177. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.H.; Botto, L.D.; Erickson, J.D.; Berry, R.J.; Sambell, C.; Johansen, H.; Friedman, J.M. Improvement in stroke mortality in Canada and the United States, 1990 to 2002. Circulation 2006, 113, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Qin, X.; Demirtas, H.; Li, J.; Mao, G.; Huo, Y.; Sun, N.; Liu, L.; Xu, X. Efficacy of folic acid supplementation in stroke prevention: A meta-analysis. Lancet 2007, 369, 1876–1882. [Google Scholar] [CrossRef]
- Lee, M.; Hong, K.; Chang, S.; Saver, J.L. Efficacy of homocysteine-lowering therapy with folic acid in stroke prevention: A meta-analysis. Stroke 2010, 41, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Huo, Y.; Li, J.; Qin, X.; Huang, Y.; Wang, X.; Gottesman, R.F.; Tang, G.; Wang, B.; Chen, D.; He, M.; et al. Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China the CSPPT Randomized Clinical Trial. JAMA 2015, 313, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Huang, T.; Zheng, Y.; Muka, T.; Troup, J.; Hu, F.B. Folic acid supplementation and the risk of cardiovascular diseases: A meta-Analysis of randomized controlled trials. J. Am. Heart Assoc. 2016, 5, e003768. [Google Scholar] [CrossRef] [PubMed]
- Klerk, M.; Verhoef, P.; Clarke, R.; Blom, H.J.; Kok, F.J.; Schouten, E.G.; MTHFR Studies Collaboration Group. MTHFR 677C → T polymorphism and risk of coronary heart disease—A meta-analysis. JAMA 2002, 288, 2023–2031. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.J.; Ebrahim, S.; Smith, G.D. Meta-analysis of MTHFR 677C → T polymorphism and coronary heart disease: Does totality of evidence support causal role for homocysteine and preventive potential of folate? Br. Med. J. 2005, 331, 1053A–1056A. [Google Scholar] [CrossRef] [PubMed]
- Holmes, M.V.; Newcombe, P.; Hubacek, J.A.; Sofat, R.; Ricketts, S.L.; Cooper, J.; Breteler, M.M.B.; Bautista, L.E.; Sharma, P.; Whittaker, J.C.; et al. Effect modification by population dietary folate on the association between MTHFR genotype, homocysteine, and stroke risk: A meta-analysis of genetic studies and randomised trials. Lancet 2011, 378, 584–594. [Google Scholar] [CrossRef] [Green Version]
- Niu, W.-Q.; You, Y.-G.; Qi, Y. Strong association of methylenetetrahydrofolate reductase gene C677T polymorphism with hypertension and hypertension-in-pregnancy in Chinese: A meta-analysis. J. Hum. Hypertens. 2012, 26, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Jia, J.; Mao, L.; Men, C.; Tang, K.; Li, Y.; Ding, H.; Zhang, Y. Methylenetetrahydrofolate reductase C677T gene polymorphism and essential hypertension: A meta-analysis of 10,415 subjects. Biomed. Rep. 2014, 2, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Horigan, G.; McNulty, H.; Ward, M.; Strain, J.J.; Purvis, J.; Scott, J.M. Riboflavin lowers blood pressure in cardiovascular disease patients homozygous for the 677C → T polymorphism in MTHFR. J. Hypertens. 2010, 28, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.P.; Ward, M.; McNulty, H.; Strain, J.J.; Trouton, T.G.; Horigan, G.; Purvis, J.; Scott, J.M. Riboflavin offers a targeted strategy for managing hypertension in patients with the MTHFR 677TT genotype: A 4-y follow-up. Am. J. Clin. Nutr. 2012, 95, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.P.; McNulty, H.; Ward, M.; Strain, J.J.; Trouton, T.G.; Hoeft, B.A.; Weber, P.; Roos, F.F.; Horigan, G.; McAnena, L.; et al. Blood pressure in treated hypertensive individuals with the MTHFR 677TT genotype is responsive to intervention with riboflavin: Findings of a targeted randomized trial. Hypertension 2013, 61, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Gjesdal, C.G.; Vollset, S.E.; Ueland, P.M.; Refsum, H.; Drevon, C.A.; Gjessing, H.K.; Tell, G.S. Plasma total homocysteine level and bone mineral density: The hordaland homocysteine study. Arch. Intern. Med. 2006, 166, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.S.; Jacques, P.F.; Selhub, J. Relation between homocysteine and B-vitamin status indicators and bone mineral density in older Americans. Bone 2005, 37, 234–242. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R.; Jacques, P.F.; Selhub, J.; Tucker, K.L.; Samelson, E.J.; Broe, K.E.; Hannan, M.T.; Cupples, L.A.; Kiel, D.P. Homocysteine as a predictive factor for hip fracture in older persons. N. Engl. J. Med. 2004, 350, 2042–2049. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hu, X.; Zhang, Q.; Cao, H.; Wang, J.; Liu, B. Homocysteine level and risk of fracture: A meta-analysis and systematic review. Bone 2012, 51, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Van Wijngaarden, J.P.; Doets, E.L.; Szczecinska, A.; Souverein, O.W.; Duffy, M.E.; Dullemeijer, C.; Cavelaars, A.E.J.M.; Pietruszka, B.; Van’t Veer, P.; Brzozowska, A.; et al. Vitamin B12, folate, homocysteine, and bone health in adults and elderly people: A systematic review with meta-analyses. J. Nutr. Metab. 2013, 2013, 486186. [Google Scholar] [CrossRef] [PubMed]
- Cagnacci, A.; Baldassari, F.; Rivolta, G.; Arangino, S.; Volpe, A. Relation of homocysteine, folate, and vitamin B-12 to bone mineral density of postmenopausal women. Bone 2003, 33, 956–959. [Google Scholar] [CrossRef] [PubMed]
- Tucker, K.L.; Hannan, M.T.; Qiao, N.; Jacques, P.F.; Selhub, J.; Cupples, L.A.; Kiel, D.P. Low plasma vitamin B12 is associated with lower BMD: The Framingham Osteoporosis Study. J. Bone Miner. Res. 2005, 20, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Gjesdal, C.G.; Vollset, S.E.; Ueland, P.M.; Refsum, H.; Meyer, H.E.; Tell, G.S. Plasma homocysteine, folate, and vitamin B 12 and the risk of hip fracture: The hordaland homocysteine study. J. Bone Miner. Res. 2007, 22, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, N.; Zillikens, M.C.; Rivadeneira, F.; De Jong, R.; Lindemans, J.; Uitterlinden, A.G.; Pols, H.A.P.; Van Meurs, J.B.J. Effect of dietary B vitamins on BMD and risk of fracture in elderly men and women: The Rotterdam Study. Bone 2007, 41, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Dhonukshe-Rutten, R.A.M.; De Vries, J.H.M.; De Bree, A.; Van Der Put, N.; Van Staveren, W.A.; De Groot, L.C.P.G.M. Dietary intake and status of folate and vitamin B12 and their association with homocysteine and cardiovascular disease in European populations. Eur. J. Clin. Nutr. 2009, 63, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.; Wang, R.; Ang, L.W.; Yuan, J.-M.; Koh, W.-P. Dietary B vitamin intake and risk of hip fracture: The Singapore Chinese Health Study. Osteoporos. Int. 2013, 24, 2049–2059. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R.; Jacques, P.F.; Selhub, J.; Fredman, L.; Tucker, K.L.; Samelson, E.J.; Kiel, D.P.; Cupples, L.A.; Hannan, M.T. Plasma B vitamins, homocysteine, and their relation with bone loss and hip fracture in elderly men and women. J. Clin. Endocrinol. Metab. 2008, 93, 2206–2212. [Google Scholar] [CrossRef] [PubMed]
- Rumbak, I.; Zizic, V.; Sokolic, L.; Cvijetic, S.; Kajfez, R.; Baric, I.C. Bone mineral density is not associated with homocysteine level, folate and vitamin B-12 status. Arch. Gynecol. Obstet. 2012, 285, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Beilby, J.; Dick, I.M.; Devine, A.; Soos, M.; Prince, R.L. The effects of homocysteine and MTHFR genotype on hip bone loss and fracture risk in elderly women. Osteoporos. Int. 2009, 20, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Honda, Y.; Iwamoto, J.; Kanoko, T.; Satoh, K. Effect of folate and mecobalamin on hip fractures in patients with stroke: A randomized controlled trial. JAMA 2005, 293, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Sawka, A.M.; Ray, J.G.; Yi, Q.; Josse, R.G.; Lonn, E. Randomized clinical trial of homocysteine level-lowering therapy and fractures. Arch. Intern. Med. 2007, 167, 2136–2139. [Google Scholar] [CrossRef] [PubMed]
- Gommans, J.; Yi, Q.; Eikelboom, J.W.; Hankey, G.J.; Chen, C.; Rodgers, H.; VITATOPS Trial Study Group. The effect of homocysteine-lowering with B-vitamins on osteoporotic fractures in patients with cerebrovascular disease: Substudy of VITATOPS, a randomised placebo-controlled trial. BMC Geriatr. 2013, 13, 88. [Google Scholar] [CrossRef] [PubMed]
- Enneman, A.W.; Swart, K.M.A.; Van Wijngaarden, J.P.; Van Dijk, S.C.; Ham, A.C.; Brouwer-Brolsma, E.M.; Van Der Zwaluw, N.L.; Dhonukshe-Rutten, R.A.M.; van der Cammen, T.J.M.; De Groot, L.C.P.G.M.; et al. Effect of vitamin b12 and folic acid supplementation on bone mineral density and quantitative ultrasound parameters in older people with an elevated plasma homocysteine level: B-PROOF, a randomized controlled trial. Calcif. Tissue Int. 2015, 96, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Van Wijngaarden, J.P.; Swart, K.M.A.; Enneman, A.W.; Dhonukshe-Rutten, R.A.M.; Van Dijk, S.C.; Ham, A.C.; Brouwer-Brolsma, E.M.; Van der Zwaluw, N.L.; Sohl, E.; Van Meurs, J.B.J.; et al. Effect of daily vitamin B-12 and folic acid supplementation on fracture incidence in elderly individuals with an elevated plasma homocysteine concentration: B-PROOF, a randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Wolffe, A.P.; Matzke, M.A. Epigenetics: Regulation through repression. Science 1999, 286, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.D.; Wolffe, A.P. DNA methylation in health and disease. Nat. Rev. Genet. 2000, 1, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Kass, S.U.; Pruss, D.; Wolffe, A.P. How does DNA methylation repress transcription? Trends Genet. 1997, 13, 444–449. [Google Scholar] [CrossRef]
- Bird, A.P.; Wolffe, A.P. Methylation-induced repression—Belts, braces, and chromatin. Cell 1999, 99, 451–454. [Google Scholar] [CrossRef]
- Jones, P.A.; Takai, D. The role of DNA methylation in mammalian epigenetics. Science 2001, 293, 1068–1070. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsen, B.; Madsen, J.S.; Tofteng, C.L.; Stilgren, L.; Bladbjerg, E.M.; Kristensen, S.R.; Brixen, K.; Mosekilde, L. A common methylenetetrahydrofolate reductase (C677T) polymorphism is associated with low bone mineral density and increased fracture incidence after menopause: Longitudinal data from the Danish osteoporosis prevention study. J. Bone Miner. Res. 2003, 18, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Miyao, M.; Morita, H.; Hosoi, T.; Kurihara, H.; Inoue, S.; Hoshino, S.; Shiraki, M.; Yazaki, Y.; Ouchi, Y. Association of methylenetetrahydrofolate reductase (MTHFR) polymorphism with bone mineral density in postmenopausal Japanese women. Calcif. Tissue Int. 2000, 66, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Hsu, Y.; Terwedow, H.; Tang, G.; Liu, X.; Jiang, S.; Xu, X.; Xu, X. Association of the methylenetetrahydrofolate reductase C677T polymorphism and fracture risk in Chinese postmenopausal women. Bone 2007, 40, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, C. Association of MTHFR C667T polymorphism with bone mineral density and fracture risk: An updated meta-analysis. Osteoporos. Int. 2012, 23, 2625–2634. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; McGuigan, F.E.; Fraser, W.D.; New, S.A.; Ralston, S.H.; Reid, D.M. Methylenetetrahydrofolate reductase polymorphism interacts with riboflavin intake to influence bone mineral density. Bone 2004, 35, 957–964. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R.; Karasik, D.; Selhub, J.; Tucker, K.L.; Ordovas, J.M.; Russo, G.T.; Cupples, L.A.; Jacques, P.F.; Kiel, D.P. Association of a common polymorphism in the methylenetetrahydrofolate reductase (MTHFR) gene with bone phenotypes depends on plasma folate status. J. Bone Miner. Res. 2004, 19, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsen, B.; Madsen, J.S.; Tofteng, C.L.; Stilgren, L.; Bladbjerg, E.M.; Kristensen, S.R.; Brixen, K.; Mosekilde, L. Are effects of MTHFR (C677T) genotype on BMD confined to women with low folate and riboflavin intake? Analysis of food records from the Danish osteoporosis prevention study. Bone 2005, 36, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, N.; Uitterlinden, A.G.; Zillikens, M.C.; Jhamai, M.; Rivadeneira, F.; Hofman, A.; De Jonge, R.; Lindemans, J.; Pols, H.A.; Van Meurs, J.B. Low dietary riboflavin but not folate predicts increased fracture risk in postmenopausal women homozygous for the MTHFR 677 T allele. J. Bone Miner. Res. 2008, 23, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Hedden, T.; Gabrieli, J. Insights into the ageing mind: A view from cognitive neuroscience. Nat. Rev. Neurosci. 2004, 5, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Park, D.C.; Reuter-Lorenz, P. The Adaptive Brain: Aging and Neurocognitive Scaffolding. Annu. Rev. Psychol. 2009, 60, 173–196. [Google Scholar] [CrossRef] [PubMed]
- Busse, A.; Bischkopf, J.; Riedel-Heller, S.G.; Angermeyer, M.C. Mild cognitive impairment: Prevalence and incidence according to different diagnostic criteria. Results of the Leipzig Longitudinal Study of the Aged (LEILA75+). Br. J. Psychiatry 2003, 182, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; et al. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Esiri, M.; Matthews, F.; Brayne, C.; Ince, P.; Matthews, F.; Xuereb, J.; Broome, J.; McKenzie, J.; Rossi, M.; McKeith, I.; et al. Pathological correlates of late-onset dementia in a multicentre, community-based population in England and Wales. Lancet 2001, 357, 169–175. [Google Scholar]
- Stevens, T.; Livingston, G.; Kitchen, G.; Manela, M.; Walker, Z.; Katona, C. Islington study of dementia subtypes in the community. Br. J. Psychiatry 2002, 180, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, P.B.; Scuteri, A.; Black, S.E.; DeCarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L.; Nyenhuis, D.; et al. Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef] [PubMed]
- Van der Flier, W.; Scheltens, P. Epidemiology and risk factors of dementia. J. Neurol. Neurosurg. Psychiatry 2005, 76, V2–V7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, R.; Panikkar, A.; McKeith, I. Dementia with Lewy bodies: Diagnosis and management. Int. J. Geriatr. Psychiatry 2001, 16, S12–S18. [Google Scholar] [CrossRef]
- Querfurth, H.W.; LaFerla, F.M. Alzheimer’s Disease. N. Engl. J. Med. 2010, 362, 329–344. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Paling, S.; Barber, R.; Williams, E.; Ballard, C.; McKeith, I.; Gholkar, A.; Crum, W.; Rossor, M.; Fox, N. Progressive brain atrophy on serial MRI in dementia with Lewy bodies, AD, and vascular dementia. Neurology 2001, 56, 1386–1388. [Google Scholar] [CrossRef] [PubMed]
- De Wilde, M.C.; Kamphuis, P.J.G.H.; Sijben, J.W.C.; Scheltens, P. Utility of imaging for nutritional intervention studies in Alzheimer’s disease. Eur. J. Pharmacol. 2011, 668, S59–S69. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.W.; Green, R.; Mungas, D.M.; Reed, B.R.; Jagust, W.J. Homocysteine, vitamin B6, and vascular disease in AD patients. Neurology 2002, 58, 1471–1475. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D. The worldwide challenge of the dementias: A role for B vitamins and homocysteine? Food Nutr. Bull. 2008, 29, S143–S172. [Google Scholar] [CrossRef] [PubMed]
- Oulhaj, A.; Refsum, H.; Beaumont, H.; Williams, J.; King, E.; Jacoby, R.; Smith, A.D. Homocysteine as a predictor of cognitive decline in Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2010, 25, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Nie, T.; Lu, T.; Xie, L.; Huang, P.; Lu, Y.; Jiang, M. Hyperhomocysteinemia and risk of cognitive decline: A meta-analysis of prospective cohort studies. Eur. Neurol. 2014, 72, 241–248. [Google Scholar] [PubMed]
- Beydoun, M.A.; Beydoun, H.A.; Gamaldo, A.A.; Teel, A.; Zonderman, A.B.; Wang, Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: Systematic review and meta-analysis. BMC Public Health 2014, 14, 643. [Google Scholar] [CrossRef] [PubMed]
- Horvat, P.; Gardiner, J.; Kubinova, R.; Pajak, A.; Tamosiunas, A.; Schoettker, B.; Pikhart, H.; Peasey, A.; Jansen, E.; Bobak, M. Serum folate, vitamin B-12 and cognitive function in middle and older age: The HAPIEE study. Exp. Gerontol. 2016, 76, 33–38. [Google Scholar] [CrossRef] [PubMed]
- De Lau, L.M.L.; Refsum, H.; Smith, A.D.; Johnston, C.; Breteler, M.M.B. Plasma folate concentration and cognitive performance: Rotterdam scan study. Am. J. Clin. Nutr. 2007, 86, 728–734. [Google Scholar] [PubMed]
- Hooshmand, B.; Solomon, A.; Kareholt, I.; Rusanen, M.; Hanninen, T.; Leiviska, J.; Winblad, B.; Laatikainen, T.; Soininen, H.; Kivipelto, M. Associations between serum homocysteine, holotranscobalamin, folate and cognition in the elderly: A longitudinal study. J. Intern. Med. 2012, 271, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.; Huang, M.H.; Karlamangla, A.; Seeman, T.; Kado, D. Do the effects of APOE-epsilon4 on cognitive function and decline depend upon vitamin status? MacArthur Studies of Successful Aging. J. Nutr. Health Aging 2011, 15, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Stewart, R.; Kim, S.; Shin, I.; Yang, S.; Shin, H.; Yoon, J. Changes in folate, vitamin B12 and homocysteine associated with incident dementia. J. Neurol. Neurosurg. Psychiatry 2008, 79, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Suever, B.L.; Prakash, R.S.; Colcombe, S.J.; McAuley, E.; Kramer, A.F. Greater intake of vitamins B6 and B12 spares gray matter in healthy elderly: A voxel-based morphometry study. Brain Res. 2008, 1199, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, D.; Peter, I.; Scott, T.M.; Parnell, L.D.; Lai, C.; Crott, J.W.; Ordovas, J.M.; Selhub, J.; Griffith, J.; Rosenberg, I.H.; et al. Status of vitamins B-12 and B-6 but not of folate, homocysteine, and the methylenetetrahydrofolate reductase C677T polymorphism are associated with impaired cognition and depression in adults. J. Nutr. 2012, 142, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- Mooijaart, S.P.; Gussekloo, J.; Frolich, M.; Jolles, J.; Stott, D.J.; Westendorp, R.G.J.; De Craen, A.J.M. Homocysteine, vitamin B-12, and folic acid and the risk of cognitive decline in old age: The Leiden 85-Plus study. Am. J. Clin. Nutr. 2005, 82, 866–871. [Google Scholar] [PubMed]
- Kang, J.H.; Irizarry, M.C.; Grodstein, F. Prospective study of plasma folate, vitamin B12, and cognitive function and decline. Epidemiology 2006, 17, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Birks, J.; Nexo, E.; Ueland, P.M.; Schneede, J.; Scott, J.; Molloy, A.; Evans, J.G. Low vitamin B-12 status and risk of cognitive decline in older adults. Am. J. Clin. Nutr. 2007, 86, 1384–1391. [Google Scholar] [PubMed]
- Haan, M.N.; Miller, J.W.; Aiello, A.E.; Whitmer, R.A.; Jagust, W.J.; Mungas, D.M.; Allen, L.H.; Green, R. Homocysteine, B vitamins, and the incidence of dementia and cognitive impairment: Results from the Sacramento Area Latino Study on Aging. Am. J. Clin. Nutr. 2007, 85, 511–517. [Google Scholar] [PubMed]
- Lildballe, D.L.; Fedosov, S.; Sherliker, P.; Hin, H.; Clarke, R.; Nexo, E. Association of cognitive impairment with combinations of vitamin B12-related parameters. Clin. Chem. 2011, 57, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Tangney, C.C.; Tang, Y.; Evans, D.A.; Morris, M.C. Biochemical indicators of vitamin B12 and folate insufficiency and cognitive decline. Neurology 2009, 72, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.S.; Selhub, J.; Jacques, P.F. Vitamin B-12 and folate status in relation to decline in scores on the mini-mental state examination in the Framingham heart study. J. Am. Geriatr. Soc. 2012, 60, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, F.; Allman-Farinelli, M.; Samman, S. Vitamin B12 status, cognitive decline and dementia: A systematic review of prospective cohort studies. Br. J. Nutr. 2012, 108, 1948–1961. [Google Scholar] [CrossRef] [PubMed]
- Kado, D.M.; Karlamangla, A.S.; Huang, M.; Troen, A.; Rowe, J.W.; Selhub, J.; Seeman, T.E. Homocysteine versus the vitamins folate, B6, and B12 as predictors of cognitive function and decline in older high-functioning adults: MacArthur Studies of Successful Aging. Am. J. Med. 2005, 118, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Riggs, K.M.; Spiro, A.; Tucker, K.; Rush, D. Relations of vitamin B-12, vitamin B-6, folate, and homocysteine to cognitive performance in the normative aging study. Am. J. Clin. Nutr. 1996, 63, 306–314. [Google Scholar] [PubMed]
- Tucker, K.L.; Qiao, N.; Scott, T.; Rosenberg, I.; Spiro, A. High homocysteine and low B vitamins predict cognitive decline in aging men: The Veterans affairs normative aging study. Am. J. Clin. Nutr. 2005, 82, 627–635. [Google Scholar] [PubMed]
- Corrada, M.M.; Kawas, C.H.; Hallfrisch, J.; Muller, D.; Brookmeyer, R. Reduced risk of Alzheimer’s disease with high folate intake: The Baltimore Longitudinal Study of Aging. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2005, 1, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Xiu, L.; Lee, M.; Wahlqvist, M.L.; Chen, R.C.; Huang, Y.; Chen, K.; Li, D. Low and high homocysteine are associated with mortality independent of B group vitamins but interactive with cognitive status in a free-living elderly cohort. Nutr. Res. 2012, 32, 928–939. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Kasturiratne, A.; Simmonds, M. Effect of folic acid, with or without other B vitamins, on cognitive decline: Meta-analysis of randomized trials. Am. J. Med. 2010, 123, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Bennett, D.; Parish, S.; Lewington, S.; Skeaff, M.; Eussen, S.J.P.M.; Lewerin, C.; Stott, D.J.; Armitage, J.; Hankey, G.J.; et al. Effects of homocysteine lowering with B vitamins on cognitive aging: Meta-analysis of 11 trials with cognitive data on 22,000 individuals. Am. J. Clin. Nutr. 2014, 100, 657–666. [Google Scholar] [CrossRef] [PubMed]
- McCaddon, A.; Miller, J.W. Assessing the association between homocysteine and cognition: Reflections on Bradford Hill, meta-analyses, and causality. Nutr. Rev. 2015, 73, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; de Jager, C.; Refsum, H.; Rosenberg, I.H. B-vitamin trials meta-analysis: Less than meets the eye. Am. J. Clin. Nutr. 2015, 101, 415–416. [Google Scholar] [CrossRef] [PubMed]
- Garrard, P.; Jacoby, R. Homocysteine lowering, B vitamins, and cognitive aging. Am. J. Clin. Nutr. 2015, 101, 414–415. [Google Scholar] [CrossRef] [PubMed]
- Van der Zwaluw, N.L.; Dhonukshe-Rutten, R.A.M.; Van Wijngaarden, J.P.; Brouwer-Brolsma, E.M.; Van De Rest, O.; In’t Veld, P.H.; Enneman, A.W.; Van Dijk, S.C.; Ham, A.C.; Swart, K.M.A.; et al. Results of 2-year vitamin B treatment on cognitive performance: Secondary data from an RCT. Neurology 2014, 83, 2158–2166. [Google Scholar] [CrossRef] [PubMed]
- Durga, J.; Van Boxtel, M.P.J.; Schouten, E.G.; Kok, F.J.; Jolles, J.; Katan, M.B.; Verhoef, P. Effect of 3-year folic acid supplementation on cognitive function in older adults in the FACIT trial: A randomised, double blind, controlled trial. Lancet 2007, 369, 208–216. [Google Scholar] [CrossRef]
- Walker, J.G.; Batterham, P.J.; Mackinnon, A.J.; Jorm, A.F.; Hickie, I.; Fenech, M.; Kljakovic, M.; Crisp, D.; Christensen, H. Oral folic acid and vitamin B-12 supplementation to prevent cognitive decline in community-dwelling older adults with depressive symptoms—The beyond ageing project: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Douaud, G.; Refsum, H.; de Jager, C.A.; Jacoby, R.; Nichols, T.E.; Smith, S.M.; Smith, A.D. Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment. Proc. Natl. Acad. Sci. USA 2013, 110, 9523–9528. [Google Scholar] [CrossRef] [PubMed]
- Kwok, T.; Lee, J.; Law, C.B.; Pan, P.C.; Yung, C.Y.; Choi, K.C.; Lam, L.C. A randomized placebo controlled trial of homocysteine lowering to reduce cognitive decline in older demented people. Clin. Nutr. 2011, 30, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Cook, N.; Manson, J.; Buring, J.E.; Albert, C.M.; Grodstein, F. A trial of B vitamins and cognitive function among women at high risk of cardiovascular disease. Am. J. Clin. Nutr. 2008, 88, 1602–1610. [Google Scholar] [CrossRef] [PubMed]
- McMahon, J.A.; Green, T.J.; Skeaff, C.M.; Knight, R.G.; Mann, J.I.; Williams, S.M. A controlled trial of homocysteine lowering and cognitive performance. N. Engl. J. Med. 2006, 354, 2764–2772. [Google Scholar] [CrossRef] [PubMed]
- Balk, E.M.; Raman, G.; Tatsioni, A.; Chung, M.; Lau, J.; Rosenberg, I.H. Vitamin B-6, B-12, and folic acid supplementation and cognitive function—A systematic review of randomized trials. Arch. Intern. Med. 2007, 167, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Brady, C.B.; Gaziano, J.M.; Cxypoliski, R.A.; Guarino, P.D.; Kaufman, J.S.; Warren, S.R.; Hartigan, P.; Goldfarb, D.S.; Jamison, R.L. Homocysteine lowering and cognition in CKD: The Veterans Affairs homocysteine study. Am. J. Kidney Dis. 2009, 54, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.H.; Flicker, L.; Alfonso, H.; Thomas, J.; Clarnette, R.; Martins, R.; Almeida, O.P. Vitamins B(12), B(6), and folic acid for cognition in older men. Neurology 2010, 75, 1540–1547. [Google Scholar] [CrossRef] [PubMed]
- De Jager, C.A.; Oulhaj, A.; Jacoby, R.; Refsum, H.; Smith, A.D. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: A randomized controlled trial. Int. J. Geriatr. Psychiatry 2012, 27, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Smith, S.M.; de Jager, C.A.; Whitbread, P.; Johnston, C.; Agacinski, G.; Oulhaj, A.; Bradley, K.M.; Jacoby, R.; Refsum, H. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: A randomized controlled trial. PLoS ONE 2010, 5, e1224. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.; Hong, C.; Yeh, H.; Liou, Y.; Yang, A.C.; Liu, M.; Hwang, J. Heterozygote advantage of the MTHFR C677T Polymorphism on specific cognitive performance in elderly Chinese males without dementia. Dement. Geriatr. Cogn. Disord. 2011, 32, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.H.; Flicker, L.; Hankey, G.J.; Norman, P.; van Bockxmeer, F.M.; Almeida, O.P. Homocysteine, methylenetetrahydrofolate reductase C677T polymorphism and cognitive impairment: The health in men study. Mol. Psychiatry 2012, 17, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Rai, V. Methylenetetrahydrofolate Reductase (MTHFR) C677T Polymorphism and Alzheimer Disease Risk: A meta-analysis. Mol. Neurobiol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Yang, M.; Li, G.; Qiu, Y.; Zheng, J.; Du, X.; Wang, J.; Liu, R. The MTHFR C677T polymorphism contributes to an increased risk for vascular dementia: A meta-analysis. J. Neurol. Sci. 2010, 294, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.; Zhao, H.; Kong, Y.; Ye, M. Association between the MTHFR Gene and Alzheimer’s Disease: A meta-analysis. Int. J. Neurosci. 2011, 121, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Hooshmand, B.; Mangialasche, F.; Kalpouzos, G.; Solomon, A.; Kareholt, I.; Smith, A.D.; Refsum, H.; Wang, R.; Muhlmann, M.; Ertl-Wagner, B.; et al. Association of vitamin B12, folate, and sulfur amino acids with brain magnetic resonance imaging measures in older adults: A longitudinal population-based study. JAMA Psychiatry 2016, 73, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Kobe, T.; Witte, A.V.; Schnelle, A.; Grittner, U.; Tesky, V.A.; Pantel, J.; Schuchardt, J.P.; Hahn, A.; Bohlken, J.; Rujescu, D.; et al. Vitamin B-12 concentration, memory performance, and hippocampal structure in patients with mild cognitive impairment. Am. J. Clin. Nutr. 2016, 103, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzoglou, A.; Refsum, H.; Johnston, C.; Smith, S.M.; Bradley, K.M.; De Jager, C.; Budge, M.M.; Smith, A.D. Vitamin B12 status and rate of brain volume loss in community-dwelling elderly. Neurology 2008, 71, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Tangney, C.C.; Aggarwal, N.T.; Li, H.; Wilson, R.S.; Decarli, C.; Evans, D.A.; Morris, M.C. Vitamin B12, cognition, and brain MRI measures: A cross-sectional examination. Neurology 2011, 77, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- De Lau, L.M.L.; Smith, A.D.; Refsum, H.; Johnston, C.; Breteler, M.M.B. Plasma vitamin B12 status and cerebral white-matter lesions. J. Neurol. Neurosurg. Psychiatry 2009, 80, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, M.; Zanardo, A.; Bendini, M.; Di Paola, F.; Boldrini, P.; Grossi, E. Serum folate, homocysteine, brain atrophy, and auto-CM system: The Treviso Dementia (TREDEM) study. J. Alzheimer’s Dis. 2014, 38, 581–587. [Google Scholar]
- Maestu, F.; Campo, P.; Del Rio, D.; Moratti, S.; Gil-Gregorio, P.; Fernandez, A.; Capilla, A.; Ortiz, T. Increased biomagnetic activity in the ventral pathway in mild cognitive impairment. Clin. Neurophysiol. 2008, 119, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- Lipton, S.A.; Kim, W.K.; Choi, Y.B.; Kumar, S.; DEmilia, D.M.; Rayudu, P.V.; Arnelle, D.R.; Stamler, J.S. Neurotoxicity associated with dual actions of homocysteine at the N-methyl-D-aspartate receptor. Proc. Natl. Acad. Sci. USA 1997, 94, 5923–5928. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.P.; Bottiglieri, T.; Arning, E.; Ziegler, M.G.; Hansen, L.A.; Masliah, E. Elevated S-adenosylhomocysteine in Alzheimer brain: Influence on methyltransferases and cognitive function. J. Neural Transm. 2004, 111, 547–567. [Google Scholar] [CrossRef] [PubMed]
- Fuso, A.; Seminara, L.; Cavallaro, R.A.; D’Anselmi, F.; Scarpa, S. S-adenosylmethionine/homocysteine cycle alterations modify DNA methylation status with consequent deregulation of PS1 and BACE and beta-amyloid production. Mol. Cell. Neurosci. 2005, 28, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Duthie, S.J.; Narayanan, S.; Brand, G.M.; Pirie, L.; Grant, G. Impact of folate deficiency on DNA stability. J. Nutr. 2002, 132, 2444S–2449S. [Google Scholar] [PubMed]
- Kruman, I.I.; Kumaravel, T.S.; Lohani, A.; Pedersen, W.A.; Cutler, R.G.; Kruman, Y.; Haughey, N.; Lee, J.; Evans, M.; Mattson, M.P. Folic acid deficiency and homocysteine impair DNA repair in hippocampal neurons and sensitize them to amyloid toxicity in experimental models of Alzheimer’s disease. J. Neurosci. 2002, 22, 1752–1762. [Google Scholar] [PubMed]
- Kruman, I.I.; Culmsee, C.; Chan, S.L.; Mattson, M.P. Folic acid deficiency and homocysteine induce neuronal apoptosis. Soc. Neurosci. 2000, 26, 93. [Google Scholar]
- Selhub, J.; Troen, A.; Rosenberg, I.H. B vitamins and the aging brain. Nutr. Rev. 2010, 68, S112–S118. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.L. Vitamin B6 in clinical neurology. Ann. N. Y. Acad. Sci. 1990, 585, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Tracy, R.P. Emerging relationships of inflammation, cardiovascular disease and chronic diseases of aging. Int. J. Obes. 2003, 27, S29–S34. [Google Scholar] [CrossRef] [PubMed]
- Dik, M.; Ferrucci, L. Chronic inflammation and common geriatric syndromes: The longitudinal aging study Amsterdam. Gerontologist 2005, 45, 654–656. [Google Scholar]
- Van Oijen, M.; de Jong, F.J.; Witteman, J.C.M.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M.B. Atherosclerosis and risk for dementia. Ann. Neurol. 2007, 61, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kim, C.; Park, J.; Lee, K.; Park, C. Effects of vitamin B12 on cell proliferation and cellular alkaline phosphatase activity in human bone marrow stromal osteoprogenitor cells and UMR106 osteoblastic cells. Metabolism 1996, 45, 1443–1446. [Google Scholar] [CrossRef]
- Masse, P.; Delvin, E.; Hauschka, P.; Donovan, S.; Grynpas, M.; Mahuren, J.; Watkins, B.; Howell, D. Perturbations in factors that modulate osteoblast functions in vitamin B6 deficiency. Can. J. Physiol. Pharmacol. 2000, 78, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Holstein, J.H.; Herrmann, M.; Splett, C.; Herrmann, W.; Garcia, P.; Histing, T.; Klein, M.; Kurz, K.; Siebel, T.; Pohlemann, T.; et al. High bone concentrations of homocysteine are associated with altered bone morphology in humans. Br. J. Nutr. 2011, 106, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Wei, I.L.; Huang, Y.H.; Wang, G.S. Vitamin B-6 deficiency decreases the glucose utilization in cognitive brain structures of rats. J. Nutr. Biochem. 1999, 10, 525–531. [Google Scholar] [CrossRef]
- Fuso, A.; Nicolia, V.; Cavallaro, R.A.; Ricceri, L.; D’Anselmi, F.; Coluccia, P.; Calamandrei, G.; Scarpa, S. B-vitamin deprivation induces hyperhomocysteinemia and brain S-adenosylhomocysteine, depletes brain S-adenosylmethionine, and enhances PS1 and BACE expression and amyloid-beta deposition in mice. Mol. Cell. Neurosci. 2008, 37, 731–746. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.B.; Jin, F.; Kan, R.; Ji, S.; Zhang, C.F.; Lu, Z.P.; Zheng, C.G.; Yang, Z.; Wang, L. Association of MTHFR gene polymorphism C677T with susceptibility to late-onset Alzheimer’s disease. J. Mol. Neurosci. 2005, 27, 23–27. [Google Scholar] [CrossRef]
- Bi, X.; Zhao, H.; Zhang, Z.; Zhang, J. Association of RFC1 A80G and MTHFR C677T polymorphisms with Alzheimer’s disease. Neurobiol. Aging 2009, 30, 1601–1607. [Google Scholar] [CrossRef] [PubMed]
- Global Progress. Available online: http://ffinetwork.org/global_progress/index.php (accessed on 1 September 2016).
- Williams, J.; Mai, C.T.; Mulinare, J.; Isenburg, J.; Flood, T.J.; Ethen, M.; Frohnert, B.; Kirby, R.S. Updated estimates of neural tube defects prevented by mandatory folic Acid fortification—United States, 1995–2011. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 1–5. [Google Scholar] [PubMed]
- Jacques, P.F.; Selhub, J.; Bostom, A.G.; Wilson, P.W.F.; Rosenberg, I.H. The effect of folic acid fortification on plasma folate and total homocysteine concentrations. N. Engl. J. Med. 1999, 340, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.S.; Jacques, P.F.; Rosenberg, I.H.; Selhub, J. Folate and vitamin B-12 status in relation to anemia, macrocytosis, and cognitive impairment in older Americans in the age of folic acid fortification. Am. J. Clin. Nutr. 2007, 85, 193–200. [Google Scholar] [PubMed]
- Bailey, R.L.; Looker, A.C.; Lu, Z.; Fan, R.; Eicher-Miller, H.A.; Fakhouri, T.H.; Gahche, J.J.; Weaver, C.M.; Mills, J.L. B-vitamin status and bone mineral density and risk of lumbar osteoporosis in older females in the United States. Am. J. Clin. Nutr. 2015, 102, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Hoey, L.; McNulty, H.; Askin, N.; Dunne, A.; Ward, M.; Pentieva, K.; Strain, J.J.; Molloy, A.M.; Flynn, C.A.; Scott, J.M. Effect of a voluntary food fortification policy on folate, related B vitamin status, and homocysteine in healthy adults. Am. J. Clin. Nutr. 2007, 86, 1405–1413. [Google Scholar] [PubMed]
- Hopkins, S.M.; Gibney, M.J.; Nugent, A.P.; McNulty, H.; Molloy, A.M.; Scott, J.M.; Flynn, A.; Strain, J.J.; Ward, M.; Walton, J.; et al. Impact of voluntary fortification and supplement use on dietary intakes and biomarker status of folate and vitamin B-12 in Irish adults. Am. J. Clin. Nutr. 2015, 101, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Panel. Dietary Reference Intake: Thiamin, Riboflavin, Niacin, Vitamin B6, Vitamin B12, Pantothenic acid, Biotin and Choline; National Academies Press: Washington, DC, USA, 2000; pp. 306–356. [Google Scholar]
- EFSA NDA Panel. Scientific opinion on dietary reference values for cobalamin (Vitamin B12). EFSA J. 2015, 13, 4150. [Google Scholar]
- Carmel, R.; Green, R.; Rosenblatt, D.S.; Watkins, D. Update on cobalamin, folate, and homocysteine. Hematol. Am. Soc. 2003, 1, 62–81. [Google Scholar] [CrossRef]
- Mills, J.L.; Von Kohorn, I.; Conley, M.R.; Zeller, J.A.; Cox, C.; Williamson, R.E.; Dufour, D.R. Low vitamin B-12 concentrations in patients without anemia: The effect of folic acid fortification of grain. Am. J. Clin. Nutr. 2003, 77, 1474–1477. [Google Scholar] [PubMed]
- Mills, J.L.; Carter, T.C.; Scott, J.M.; Troendle, J.F.; Gibney, E.R.; Shane, B.; Kirke, P.N.; Ueland, P.M.; Brody, L.C.; Molloy, A.M. Do high blood folate concentrations exacerbate metabolic abnormalities in people with low vitamin B-12 status? Am. J. Clin. Nutr. 2011, 94, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Hamner, H.; Pfeiffe, C.; Berry, R. The prevalence of low serum vitamin B-12 status in the absence of anemia or macrocytosis did not increase among older U.S. adults after mandatory folic acid fortification. J. Nutr. 2014, 144, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Selhub, J.; Morris, M.S.; Jacques, P.F.; Rosenberg, I.H. Folate-vitamin B-12 interaction in relation to cognitive impairment, anemia, and biochemical indicators of vitamin B-12 deficiency. Am. J. Clin. Nutr. 2009, 89, 702s–706s. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.M.; Ames, D.; Mander, A.G.; Carne, R.P.; Brodaty, H.; Woodward, M.C.; Boundy, K.; Ellis, K.A.; Bush, A.I.; Faux, N.G.; et al. Among vitamin B12 deficient older people, high folate levels are associated with worse cognitive function: Combined data from three cohorts. J. Alzheimer’s Dis. 2014, 39, 661–668. [Google Scholar]
- Clarke, R.; Sherliker, P.; Hin, H.; Molloy, A.M.; Nexo, E.; Ueland, P.M.; Emmens, K.; Scott, J.M.; Evans, J.G. Folate and vitamin B12 status in relation to cognitive impairment and anaemia in the setting of voluntary fortification in the UK. Br. J. Nutr. 2008, 100, 1054–1059. [Google Scholar] [CrossRef] [PubMed]
- Doets, E.L.; Ueland, P.M.; Tell, G.S.; Vollset, S.E.; Nygard, O.K.; Van’t Veer, P.; De Groot, L.C.P.G.M.; Nurk, E.; Refsum, H.; Smith, A.D.; et al. Interactions between plasma concentrations of folate and markers of vitamin B(12) status with cognitive performance in elderly people not exposed to folic acid fortification: The Hordaland Health Study. Br. J. Nutr. 2014, 111, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- National Toxicology Program. Identifying Research Needs for Safe Use of High Intakes of Folic Acid. 2015. Available online: https://ntp.niehs.nih.gov/ntp/ohat/folicacid/ntpfolicacid_approach_508.pdf (accessed on 1 August 2016). [Google Scholar]
- Ebbing, M.; Bonaa, K.H.; Nygard, O.; Arnesen, E.; Ueland, P.M.; Nordrehaug, J.E.; Rasmussen, K.; Njolstad, I.; Refsum, H.; Nilsen, D.W.; et al. Cancer incidence and mortality after treatment with folic acid and vitamin B-12. JAMA 2009, 302, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, J.C.; Grau, M.V.; Haile, R.W.; Sandler, R.S.; Summers, R.W.; Bresalier, R.S.; Burke, C.A.; McKeown-Eyssen, G.E.; Baron, J.A. Folic acid and risk of prostate cancer: Results from a randomized clinical trial. J. Natl. Cancer Inst. 2009, 101, 432–435. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.B. Folate consumption and cancer risk: A confirmation and some reassurance, but we’re not out of the woods quite yet. Am. J. Clin. Nutr. 2011, 94, 965–966. [Google Scholar] [CrossRef] [PubMed]
- Report to CMO on Folic Acid and Colorectal Cancer. Available online: https://www.gov.uk/government/publications/sacn-report-to-cmo-on-folic-acid-and-colorectal-cancer-risk (accessed on 24 August 2016).
- Troen, A.M.; Mitchell, B.; Sorensen, B.; Wener, M.H.; Johnston, A.; Wood, B.; Selhub, J.; McTiernan, A.; Yasui, Y.; Oral, E.; et al. Unmetabolized folic acid in plasma is associated with reduced natural killer cell cytotoxicity among postmenopausal women. J. Nutr. 2006, 136, 189–194. [Google Scholar] [PubMed]


{kind=link}
| B Vitamin | Inadequate Intake | Increased Requirement | Malabsorption | Drug–Nutrient Interactions | Other |
|---|---|---|---|---|---|
| Folate [19,20,21,22,23,24] | Common Poor cooking techniques | Elderly Pathological conditions | Intestinal diseases Coeliac disease Crohn’s disease Ulcerative Colitis | Phenytoin Phenobarbital/Primidone Trimethoprim Methotrexate Sulfasalazine Metformin | Alcohol abuse Genetic disorders Haemolytic anaemia |
| B12 [19,21,22,25,26] | Common Vegan diets | Elderly | Intestinal diseases Coeliac disease Crohn’s disease Gastric/intestinal resection Atrophic gastritis Bacterial overgrowth Helicobacter pylori Pancreatic insufficiency Pernicious anaemia Zollinger–Ellison Syndrome | Proton pump inhibitors H2-receptor antagonists Metformin Nitrous oxide Colchicine | Alcohol abuse Genetic disorders Tropical or non-tropical sprue |
| B6 [21,22,25,26] | Rare Chronic dieters | Elderly | HIV | Isoniazid Anti-Convulsants Steroids | Alcohol abuse Genetic disorders Liver disease Renal dialysis Rheumatoid arthritis |
| B2 [21,25,26,27] | Common Chronic dieters | Elderly | Diabetes Liver disease Thyroid and renal insufficiency GI and biliary obstruction | Phenothiazines, e.g., chlorpromazine Theophylline | Alcohol abuse Genetic disorders Hypochromic anaemia Metals such as zinc, copper and iron |
| Biomarker | Strengths | Limitations | ||
|---|---|---|---|---|
| Homocysteine [20] | Functional | Plasma homocysteine | Sensitive functional biomarker Highly responsive to intervention with B-vitamins Responds within 3–4 weeks of B-vitamin depletion and subsequent repletion Very stable analyte Can be stored frozen for extended periods of time | Lacks specificity as affected by other B-vitamins Requires separation from RBCs within one hour of blood collection, or <8 h if whole blood is kept on ice Influenced by other factors such as lifestyle, genetics, renal insufficiency, age and medications |
| Folate [20,21,60,63,75] | Direct | Serum/Plasma folate | Earliest indicator of altered folate exposure Reflects recent dietary folate intake Requires less time processing at time of blood collection vs. RBC folate Can be measured in the field | Inconsistent use of cut off values makes comparisons across different methods and labs difficult Fasting blood samples are recommended |
| Red cell folate | Sensitive indicator of long-term folate status Reflects folate status over half-life of RBCs Reflects tissue folate stores as parallels liver concentrations Highly correlated with habitual intake when expressed as DFEs | Affected by vitamin B12 deficiency Inconsistent use of cut off values makes comparisons across different methods and labs difficult Cannot be measured in the field | ||
| B12 [21,34,60,70,75,76] | Direct | Serum/Plasma total B12 | Serum standard clinical test Variety of assays available Measures all forms of vitamin B12 | Does not reflect intracellular vitamin B12 Falsely elevated B12 caused by factors including liver disorders, bacterial overgrowth, renal failure Falsely low B12 caused by factors such as iron deficiency, HIV infection and pregnancy Inconsistent use of cut off values makes comparisons across different methods and labs difficult |
| Serum/Plasma Holo-transcobalamin (HoloTC) | Represents metabolically active fraction of B12 Decrease in holoTC can indicate earliest sign of B12 depletion Considered better indicator of B12 status in elderly | Highly sensitive to altered renal function and influenced by factors including genetics | ||
| Functional | Serum/plasma/urine Methylmalonic acid (MMA) | Reflects availability of intracellular B12 Early detection of functional B12 deficiency Not affected by folate deficiency | Lacks sensitivity as can be elevated in those with renal impairment High running costs | |
| B6 [21,60,72,77,78] | Direct | Plasma Pyridoxal-Phosphate (PLP) | Most widely used Good specificity and reflects PLP content in liver Responds quickly within 1–2 weeks of B6 depletion and subsequent repletion Reference ranges available for younger and older adults Fairly stable at low temperatures | Does not represent PLP content in the muscle which is resistant to B6 depletion Influenced by other factors such as age, sex, pregnancy, protein and alcohol intake PLP declines in samples stored at room temperature and exposure to light Fasting blood samples are recommended Plasma PLP concentrations affected by use of certain drugs |
| Erythrocyte PLP | Positively correlated with B6 dietary intake Responds within weeks of B6 depletion and subsequent repletion Appears more responsive than plasma PLP to supplementation May be more reliable marker than plasma PLP under conditions and disease associated with inflammation | Affected by haemoglobin variants Assay is cumbersome, with variable recovery and low precision | ||
| B2 [21,60,74,78] | Direct | Serum/Plasma/Erythrocyte Riboflavin/Flavine Adenine Dinucleotide (FAD)/Flavin Mononucleotide (FMN) | Riboflavin vitamers are stable for several years when plasma samples are stored at −80 ° CSerum/plasma can be used retrospectively in a hospital setting | Influenced by other factors such as age, sex, pregnancy, protein and alcohol intake Serum/plasma riboflavin concentrations affected by use of certain drugs High variability within and between-subjects compared to the cofactor forms of riboflavin (plasma/erythrocyte) |
| Functional | Erythrocyte glutathione reductase activation (EGRac) assay | Most widely used marker of status Measures tissue saturation and long term status Enzyme is stable for several years when erythrocyte lysates are stored at −80 °C | Poor index of optimum riboflavin status Assay is not linear against status Difficult make comparisons across different methods and labs |
| Clinical Deficiency Signs [19,20,21,22] | |
|---|---|
| Folate | Megaloblastic anaemia, clinical features characterised by megaloblasts in the bone marrow macrocytes in the peripheral blood gigantism in the morphology of proliferating cells |
| B12 | Megaloblastic anaemia indistinguishable from folate-related megaloblastic anaemia Irreversible nerve damage/neuropathy Sub-acute combined degeneration of the spinal cord (SCD) |
| B6 | Notable symptoms include: Microcytic anaemia Inflammation of the tongue Sores or ulcers of the mouth Dermatitis Nervous/muscular signs Irritability, fatigue, numbness Headache, muscle twitching Difficulty walking, convulsions Depression and confusion |
| B2 | Classic signs arbioflavinosis, rarely encountered in isolation Anaemia Cheliosis, Angular stomatitis Glossitis Redness and swelling of the lining of the mouth and throat Seborrheic dermatitis particularly affecting the nose, cheeks and forehead Eyes burning and itching Sensitivity to light Loss of visual acuity Gritty sensation under the eyelids |
| Health Consequences of Low Status of Folate and/or Other B-Vitamins [83,84,85,86,87,88,89] | |
| Elevated homocysteine CVD and stroke Cognitive decline/dementia/Alzheimer’s Osteoporosis and risk of fractures |
| Author/Year/Trial | Country | Sample Size (n) | Age (Years) | Population Studied Plasma tHcy (µmol/L) | Treatment (mg/day) | Duration | Cognitive Outcomes |
|---|---|---|---|---|---|---|---|
| Questionnaire based assessment | |||||||
| McMahon 2006 [191] | New Zealand | 276 | ≥65 | Healthy tHcy > 13 | 1.0 FA, 0.5 B12, 10 B6 | 2 years | No significant effect on cognition |
| FACIT Durga 2007 [186] | The Netherlands | 818 | 50–70 | Healthy tHcy 13–26 | 0.8 FA or placebo | 3 years | Improvement in domains including memory, information-processing and sensorimotor speed No improvement in global cognition or domains of complex speed or word fluency |
| WAFACS Kang 2008 [190] | USA | 2009 | ≥65 | CVD/high risk women tHcy not provided | 2.5 FA, 1.0 B12, 50 B6 or placebo | 6.6 years | Reduced risk of cognitive decline among women with low baseline dietary intake of B-vitamins Overall no significant effect on rate of cognitive decline |
| Brady 2009 [193] | USA | 659 | Mean 67.3 | Advanced renal disease tHcy ≥ 15 | 40 FA, 2.0 B12, 100 B6 or placebo | 5 years | No significant effect on cognition |
| Health in Men Study: sub set Ford 2010 [194] | Australia | 299 | ≥75 | Hypertensive men Mean tHcy 13.1–14 | 2.0 FA, 0.4 B12, 25 B6 or placebo | 2 years | No significant effect on cognition |
| Kwok 2011 [189] | Hong Kong | 140 | ≥60 | Dementia diagnosis Mean tHcy 14.1 | 5.0 FA, 1.0 B12 or placebo | 2 years | Improvement in domain of construction No change in global cognitive decline, attention, memory or conceptualisation |
| Beyond ageing project Walker 2012 [187] | Australia | 900 | 60–74 | Elevated psychological distress Mean tHcy 9.7 | 0.4 FA, 0.1 B12 or placebo | 2 years | Improvement in overall global cognition and in domains of immediate and delayed recall scores No significant change in other cognitive domains |
| VITACOG De Jager 2012 [195] | UK | 168 | ≥70 | MCI Mean tHcy 11.3 | 0.8 FA, 0.5 B12, 20 B6 or placebo | 2 years | Slower decline in global cognition and in domains of semantic and episodic memory Clinical benefit in global clinical dementia rating score |
| BPROOF Van Der Zwaluw 2014 [185] | The Netherlands | 2919 | ≥65 | Healthy tHcy 12–50 | 0.4 FA, 0.5 B12, 0.15 D3 or placebo + D3 | 2 years | Slower rate of decline in global cognition No change in domains of memory |
| Brain-imaging assessment | |||||||
| VITACOG Smith 2010 Douaud 2013 [188,196] | UK | 168 | ≥70 | MCI Mean tHcy 11.3 | 0.8 FA, 0.5 B12, 20 B6 or placebo | 2 years | Slowed shrinkage of brain Marked reduction in cerebral atrophy in grey matter regions |
| BPROOF Van Der Zwaluw 2014 [185] | The Netherlands | 2919 | ≥65 | Healthy tHcy 12–50 | 0.4 FA, 0.5 B12, 0.15 D3 or placebo + D3 | 2 years | Awaiting MRI scan results |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porter, K.; Hoey, L.; Hughes, C.F.; Ward, M.; McNulty, H. Causes, Consequences and Public Health Implications of Low B-Vitamin Status in Ageing. Nutrients 2016, 8, 725. https://doi.org/10.3390/nu8110725
Porter K, Hoey L, Hughes CF, Ward M, McNulty H. Causes, Consequences and Public Health Implications of Low B-Vitamin Status in Ageing. Nutrients. 2016; 8(11):725. https://doi.org/10.3390/nu8110725
Chicago/Turabian StylePorter, Kirsty, Leane Hoey, Catherine F. Hughes, Mary Ward, and Helene McNulty. 2016. "Causes, Consequences and Public Health Implications of Low B-Vitamin Status in Ageing" Nutrients 8, no. 11: 725. https://doi.org/10.3390/nu8110725